Embed Size (px)
Citation preview

TARGETING KIDNEY INFLAMMATION IN A MURINE MODEL OF ALPORT SYNDROME
by
Kyoungheon Ahn
A thesis submitted in conformity with the requirements for the degree of Master of Science
Department of Physiology University of Toronto
© Copyright by Kyoungheon Ahn 2018

ii
Targeting kidney inflammation in a murine model of Alport Syndrome
Kyoungheon Ahn
Master of Science
Department of Physiology University of Toronto
2018
Abstract
Alport Syndrome is a rare inherited kidney disease that is due to genetic mutations of
type IV collagen. The mutations interfere with normal assembly of the glomerular basement
membrane and this structural abnormality leads to a progressive rise in urinary protein excretion
and eventually to end stage renal failure. Preliminary studies in our laboratory suggest that
inflammation may play an early role in the pathogenesis of glomerular injury.
Thus, the relationship between inflammatory pathways and AS disease progression was
examined in this study by inhibiting NF-κB activation in glomerular cells using MS417. I
hypothesized that the early activation of NF-κB plays a key role in the initiation and progression
of kidney injury in AS and the blockade of NF-κB-mediated gene expression can attenuate
kidney injury in experimental AS. The findings from the analysis of gene expression in a murine
model of AS identified NF-κB as an important target for treatment.

iii
Acknowledgements
I would like to thank my supervisor, Dr. James Scholey, for providing me with this
opportunity. I am truly grateful for the time and effort you have invested in me and the
experiences I have gained in your lab has helped me grow not only as a scholar but as a human
being. Thank you!
I would also like to thank my committee members, Dr. York Pei and Dr. Scott Heximer,
for their invaluable input and guidance. Their support throughout my degree have challenged and
pushed me to become a more critical and attentive scientist.
A special thanks to my examination committee members, Dr. Zhong-Ping Feng and Dr.
Tianru Jin, for providing me with indispensable input to my thesis work. I am also extremely
grateful for Dr. Feng’s unflagging patience, understanding, and support as the departmental
graduate coordinator.
I must also extend my gratitude to the members of the Pei lab, in particular, Dr. Xuewen
Song, who has lent her expertise to my research work, as well as members of the Scholey lab.
A very special thank you to Veronica Talunay for her unrelenting kindness and patience.
Thank you for all the laughter and chats, I will forever be grateful to you!
I also would like to thank Dr. John He for providing me with the NF-κB inhibiting
compound, MS417, which provided the foundation for my research.
This thesis could not have been completed without the funding provided by the
Department of Physiology, the Alport Syndrome Foundation, and the Kidney Foundation of
Canada.

iv
Table of Contents
Acknowledgements ...................................................................................................................... iii
Table of Contents ......................................................................................................................... iv
List of Figures ............................................................................................................................... vi
List of Tables .............................................................................................................................. viii
List of Abbreviations ................................................................................................................... ix
Chapter 1 Introduction ................................................................................................................ 1
1.1 Clinical features of Alport Syndrome ....................................................................... 1
1.2 Genotype-phenotype correlation ............................................................................... 4
1.3 Glomerular basement membrane .............................................................................. 6
1.3.1 Laminin ............................................................................................................ 6
1.3.2 Type IV collagen .............................................................................................. 8
1.3.3 Nidogen ............................................................................................................ 9
1.3.4 Heparan sulfate proteoglycans ....................................................................... 10
1.3.5 Glomerular basement memebrane in Alport Syndrome ................................ 11
1.4 Current clinical management options ..................................................................... 12
1.5 Renal inflammation blockade via BRD4 inhibition ................................................ 18
1.6 Experimental design and hypothesis ....................................................................... 23
Chapter 2 Materials and Methods ............................................................................................. 24
2.1 Animals ................................................................................................................... 24
2.2 MS417 treatment ..................................................................................................... 24
2.3 Blood biochemistry ................................................................................................. 25
2.4 Urinary albumin excretion ...................................................................................... 25

v
2.5 Isolation of mice glomeruli ..................................................................................... 26
2.6 Microarray data and bioinformatics analysis .......................................................... 30
2.7 Cell culture and NF-κB activity assay .................................................................... 31
2.8 Real-time RT-PCR .................................................................................................. 32
2.9 Statistical analysis ................................................................................................... 32
Chapter 3 Results ........................................................................................................................ 33
3.1 Characterization and breeding of murine model of Alport Syndrome ................... 33
3.2 Early microarray studies in glomeruli ..................................................................... 39
3.3 Targeting NF-κB in vitro ........................................................................................ 47
3.4 Analysis of NF-κB inhibition in vivo using whole kidney samples ....................... 49
3.4.1 Whole animal kidney examination ................................................................ 49
3.4.2 Proinflammatory cytokine expression ........................................................... 54
3.5 Analysis of NF-κB inhibition in vivo via microarray studies ................................. 56
Chapter 4 Discussion .................................................................................................................. 65
4.1 Major changes in gene expression are observed in the glomeruli prior to a decline in GFR in experimental AS ........................................................................................................... 65 4.2 Pathway analysis of the differential gene expressions established that pathways converged on NF-κB ..................................................................................................................... 72 4.3 A novel approach to inhibiting NF-κB-mediated gene expression: BRD4 antagonism .................................................................................................................................... 76 4.4 BRD4 inhibitor treatment led to a decrease in cytokine gene expression and a trend towards improved creatinine levels and albuminuria ................................................................... 78 4.5 Conclusions ............................................................................................................. 80
4.6 Pitfalls and future directions ................................................................................... 81
References .................................................................................................................................... 82

vi
List of Figures
Figure 1. Molecular mechanism of BRD4-regulated inflammation and the inhibition of inflammatory gene transcription with MS417 .............................................................................. 22 Figure 2. Flow chart of glomeruli isolation from Col4a3-/- mice .................................................. 28
Figure 3. RT-PCR of podocyte and distal tubular markers for microarray sample selections ..... 29
Figure 4. Col4a3 KO mice breeding scheme and PCR genotyping ............................................. 35
Figure 5. Heat map of collagen IV α1-α5 expression levels in Col4a3-/- kidneys ....................... 36
Figure 6. Histopathologic injury in Col4a3-/- and WT kidneys .................................................... 37
Figure 7. Functional manifestations of renal pathology of Col4a3-/- mice ................................... 38
Figure 8. Levels of differential gene expression in kidney tissues in WT and KO mice ............. 41
Figure 9. Schematic summary of aberrant activation of signnaling pathways in AS mice .......... 43
Figure 10. Levels of differentially expressed IL-1β target genes ................................................. 44
Figure 11. Levels of differentially expressed TLR4 and MYD88 target genes ............................ 45
Figure 12. Levels of differentially expressed NF-κB target genes in kidney tissues of WT and KO mice ........................................................................................................................................ 46 Figure 13. MS417-inhibited Ang II-induced NF-κB activation HK-2 cells ................................. 48
Figure 14. Body weight change measurements in WT and KO mice ........................................... 50
Figure 15. Blood urea nitrogen (BUN) levels in 7-week-old WT and KO mice following vehicle or MS417 treatment ...................................................................................................................... 51 Figure 16. Serum creatinine levels assessed in 7-week-old animals following vehicle or MS417 treatment ....................................................................................................................................... 52 Figure 17. Urinary albumin excretion (UAE) assessed in 7-week-old animals ........................... 53
Figure 18. Proinflammatory cytokine levels in kidney tissue in WT and Col4a3 KO mice after sham or MS417 treatment ............................................................................................................. 55 Figure 19. Levels of differential gene expression in glomeruli in WT and KO mice after 10-day treatment with sham or MS417 ..................................................................................................... 61

vii
Figure 20. Marked differential gene expression levels of IL-1β target genes in glomeruli of WT and KO mice ................................................................................................................................. 62 Figure 21. Levels of marked differential gene expression levels of TLR4 and MYD88 target genes in glomeruli of WT and KO mice ....................................................................................... 63 Figure 22. Marked differential gene expression levels of NF-κB target genes in glomeruli of WT and KO mice ................................................................................................................................. 64

viii
List of Tables
Table 1. 55 Ingenuity Pathway Analysis predicted activated upstream regulators in 4-week-old KO glomeruli ................................................................................................................................ 42 Table 2. Summary of glomerular isolation perfusion performed and RNA yield qualities for analyses ......................................................................................................................................... 58 Table 3. RNA quality of glomeruli samples selected for microarray study .................................. 59 Table 4. Reassignment of experimental groups for microarray study .......................................... 60

ix
List of Abbreviations
αSMA Alpha-smooth muscle actin
ACE Angiotensin-converting enzyme
ADAS Autosomal dominant Alport Syndrome
ADM Adrenomedullin
AKI Acute kidney injury
Ang II Angiotensin II
ARAS Autosomal recessive Alport Syndrome
ARB Angiotensin receptor blocker
AS Alport Syndrome
AT1R Angiotensin II type 1 receptor
AT2R Angiotensin II type 2 receptor
BET Bromodomain and extra-terminal domain
BM Bone marrow
BMP-7 Bone morphogenic protein-7
BRD4 Bromodomain-containing protein 4
BUN Blood urea nitrogen
CCP-1 Chemokine receptor 1
CD45 Cluster of differentiation 45
CDK9 Cyclin-dependent kinase 9
CKD Chronic kidney disease
COL Collagen
CXCL10 C-X-C motif chemokine 10
CXCR3 C-X-C motif chemokine receptor 3
CYP1B1 Cytochrome P450 family 1 subfamily B member 1
DAMP Damage-associated molecular pattern
DOX Doxycycline
DMSO Dimethyl sulfoxide
EAST Epilepsy, ataxia, sensorineural deafness, and tubulopathy
ECM Extracellular matrix

x
ESCAPE Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness
ESRD End-stage renal disease
ESRF End-stage renal failure
GAPDH Glyceraldehyde 3-phosphate dehydrogenase
GBM Glomerular basement membrane
GFR Glomerular filtration rate
HBSS Hank’s balanced salt solution
HIV Human immunodeficiency virus
HIVAN HIV-associated nephropathy
HK-2 Human kidney-2
HMG-CoA 3-hydroxy-3-methylglutaryl-CoA
HSPG Heparan sulfate proteoglycan
IFN-γ Interferon gamma
IgA Immunoglobulin A
IκB Inhibitor kappa B
IKK IκB kinase
IL Interleukin
IPA Ingenuity Pathway Analysis
KCNJ1 Potassium voltage-gated channel subfamily J member 1; renal outer medullary potassium channel
KCNJ16 Potassium voltage-gated channel subfamily J member 16; inward rectifier potassium channel 16
KLK1 Kallikrein 1
KO Knockout
LCC Laminin coiled-coil
LG Laminin globular
LM-521 Laminin-521
LincRNA Long intergenic non-coding ribonucleic acid
LPS Lipopolysaccharide
MCP-1 Monocyte chemoattractant protein-1
MMP Matrix metalloproteinase

xi
MSC Mesenchymal stem cell
MT Masson’s trichrome
MYD88 Myeloid differentiation primary response 88
NADPH Nicotinamide adenine dinucleotide phosphate
NC Negative control
NF-κB Nuclear factor-kappa-light-chain-enhancer of activated B cells
NLR Nucleotide-binding oligomerization domain-like receptor
PAMP Pattern-associated molecular pattern
PAS Periodic acid-Schiff
PBS Phosphate-buffered saline
PDGF Platelet-derived growth factor
PI3K Phosphoinositide 3-kinase
PRR Pattern recognition receptor
P-TEFb Positive transcription elongation factor b
RANTES Regulated on activation, normal T cell expressed and secreted
RAS Renin-angiotensin system
RC Renal cortex
RCC Renal cell carcinoma
RHD Rel homology domain
RIN Ribonucleic acid integrity number
ROS Reactive oxygen species
RT-PCR Reverse transcription polymerase chain reaction
SFRP1 Secreted frizzled related protein 1
SM22α Smooth muscle protein 22-alpha
TAGLN Transgelin
TGF-β Transforming growth factor beta
TLR Toll-like receptor
TNF Tumour necrosis factor
TNF-α Tumour necrosis factor alpha
TNFRSF12A Tumour necrosis factor receptor superfamily member 12A
TNFSF12 Tumour necrosis factor superfamily member 12

xii
TRIF Toll-interleukin-1 receptor domain-containing adapter-inducing interferon-beta
TWEAK TNF-related weak inducer of apoptosis
UAE Urinary albumin excretion
UUO Unilateral ureteral obstruction
Wnt Wingless-related mouse mammary tumour virus
WT Wildtype
XLAS X-linked Alport Syndrome

1
Chapter 1
Introduction
1.1 Clinical features of Alport Syndrome
Alport Syndrome (AS) is a rare inherited form of chronic kidney disease (CKD)
characterized by progressive nephropathy, sensorineural loss, ocular defects, and the
development of end stage renal disease (ESRD)1–3. It affects at least one in 50,000 individuals
and it is caused by mutations in genes that encode α3-α4-α5(IV) chains of type IV collagen
(Col4α3, Col4α4, and Col4α5, respectively), which interfere with the normal assembly of the
glomerular basement membrane (GBM)2,4–6. Mutations of the COL4A5 gene on chromosome
Xq22 cause X-linked AS (XLAS), which accounts for approximately 85% of cases, whereas
recessive mutations of COL4A3 or COL4A4 genes on chromosome 2q36 constitute the remaining
cases (autosomal recessive AS; ARAS)7–9. In rare instances (<1%), COL4A3 or COL4A4
mutations may follow an autosomal dominant pattern (autosomal dominant AS; ADAS)10.
Clinically, XLAS and ARAS have similar disease characteristics and prognosis, and are
indistinguishable on clinical grounds or standard assessments of renal biopsy tissue, despite the
very distinct patterns of inheritance6.
Such genetic mutations in the type IV collagen give rise to microhematuria as the first
renal manifestation of AS in childhood, which then gradually progress to proteinuria,
hypertension, and eventually to kidney failure in all males with XLAS and in both sexes with
ARAS4,11. Males with X-linked inheritance may be affected with an early onset of the disease,
generally accompanied by extrarenal features, and develop ESRD before the age of 30, or
experience a late onset with renal failure after 30 years of age, commonly accompanied solely by
hearing loss12,13. High-tone sensorineural hearing loss occurs in 70% of affected males and

2
lenticonus in approximately 30% of males with XLAS by age 40, when renal failure, hearing
loss, and retinopathy are already present14. In contrast, the disease characteristics tend to be
predominantly milder in females with XLAS compared to males as they are heterozygous
carriers of the disease. Generally, XLAS female patients have minimal clinical manifestations
such as asymptomatic hematuria by age of 30-40 years, proteinuria (75%), ESRD (15% by age
of 60), hearing loss (40%), or peripheral retinopathy (40%). Lenticonus may not occur and
central retinopathy is rare15. As well, X chromosome inactivation, the process by which the
unmutated copy of one X chromosome counters the effect of the mutation, contributes to
variability among female carriers of XLAS, lending to mosaic disease symptoms16.
Autosomal recessive AS is suspected where the disease is found in only a single
generation or a consanguineous family, where males and females in a family are affected with
equal frequency and severity1,17. In autosomal recessive AS, patients exhibit an early onset of
renal failure, including persistent microhematuria that progresses to significant proteinuria and
ultimately to ESRD, before 30 years of age in both sexes. Individuals with ARAS typically also
exhibit juvenile onset of hearing loss with no gender differences in the incidence of hearing
deficit. Ocular lesions stemming from ARAS are present in 30-40% of individuals with more
frequent occurrences in affected males than females18. Contrastingly, in individuals with
autosomal dominant AS, ESRD is frequently delayed until later adulthood than in those with
XLAS or ARAS, with late onset of cochlear manifestations and rare occurrence of ocular
complicity19,20.
In addition to nephropathy, cochlear and ocular abnormalities observed in AS result from
an absence of the collagen IV networks in the ear and eye14. Hearing loss in AS is never
congenital with defective adhesion of the organ of Corti to the basilar membrane possibly

3
underlying the hearing deficit observed in AS patients21,22. Pathognomonic ocular feature of AS
is bilateral anterior lenticonus in which the anterior surface of the lens assumes abnormal conical
shapes and protrude into the anterior chambers of the eyes, bringing about progressive distortion
of the lens accompanied by increasing myopia and astigmatism23. Other typical ocular
abnormalities include dot-and-fleck retinopathy, consisting of whitish or yellowish flecks or
granulations in the retina, corneal disorders, such as recurrent corneal erosion and posterior
polymorphous corneal dystrophy, which can cause severe ocular pain24–27.
Atypical clinical features of AS include gastroesophageal leiomyomatosis, a condition
characterized by visceral smooth muscle overgrowth leading to benign tumours within the
respiratory, gastrointestinal, and female reproductive tracts28,29. Leiomyomas are rarely
associated with AS; however, when present, it is pathognomonic for AS and affected patients
carry a large deletion in the 5’ ends of the COL4A5 and COL4A6 genes, which is normally
expressed in smooth muscle cells of the gastroesophageal tract30. The pathogenetic correlation
between the deletions of the COL4A5 and COL4A6 genes and the incidence of leiomyomas has
not been elucidated. One study by Dahan et al. (1995) suggests that cell proliferation in
leiomyomatosis could be due to the misalignment that results from the occurrence of repeated
sequences in the large COL4A5 and COL4A6 introns31. Arterial abnormalities, such as aneurysms
in adolescence, have also been reported in patients with AS, pronouncing the importance of
Col4α5 and Col4α6 chains in the maintenance of vascular integrity32–34.
The pathologic lesions for renal biopsies from AS patients are variable when examined
by electron microscopy; however, typically renal biopsies exhibit podocyte hypertrophy and
stiffness of the capillary wall, periodically associated with the presence of tubular red blood cell
casts20. Thereafter, gradual glomerular basement membrane thickening and splitting with

4
progressive enlargement of mesangial stalks can be observed20,35. This development of
longitudinal splitting of the lamina densa of GBM bestowing a lamellated appearance is
diagnostic of AS36. The GBM lesion can be intermittent, alternating between segments of thick
or abnormally thin GBM, which is particularly prevalent in children with AS or XLAS females37.
GBM lamellation is also accompanied by fragmentary podocyte foot process effacement,
exhibiting progressive podocyte depletion, a common mechanism in glomerular diseases that
further drives progression38–41. Furthermore, there is segmental or diffuse glomerulosclerosis,
tubular atrophy, and interstitial fibrosis present, along with interstitial infiltration with
lymphocytes and macrophages, correlated with progressive renal failure42,43.
1.2 Genotype-phenotype correlation
The correlation between clinical presentations and the underlying mutations that bring
about AS has been extensively studied and reviewed in order to not only better understand the
mechanisms of disease, but also to potentiate the prognostic value of efficient and noninvasive
screening methods, such as genetic testing44. Extensive studies have been performed globally to
characterize the natural history of AS and it has been established that there is a strong association
between the genetic variants and the renal disease severity45–47. Specifically, patients with large
deletions and nonsense mutations demonstrate more severe manifestations of the disease with
earlier progression to ESRD compared to those with missense mutations, while those with splice
site mutations present with an intermediate disease progression48. Thus, the risk of ESRD by 30
years of age for male XLAS patients with missense mutations, splice site mutations, and large
deletions and nonsense mutations are 50%, 70%, and 90%, respectively, with the average age of
ESRD being 37, 28, and 25 years, respectively12. Correspondingly, large deletions, splice site, or

5
truncating mutations confer a significantly higher risk of developing hearing loss and ocular
lesions in patients than among those with missense mutations12,44,48. Furthermore, Bekheirnia et
al. (2010) demonstrated that there was an association between the mutation position and the
disease outcome, with an earlier onset of ESRD related to pathogenic mutations at the 5’ end of
the gene; the development of hearing impairment and ocular changes showed a similar
association with the mutation location. Though the genotype-phenotype correlation has only
been established in XLAS males, clinical courses of XLAS and ARAS are similar47. In contrast,
no correlation between the degree of the disease progression and the type of underlying mutation
could be substantiated in female carriers of XLAS15,49.
Currently several animal models of Alport Syndrome have been developed and published
in the literature50,51. Such experimental models have yielded significant insight into the
molecular basis of AS as well as the structure and biosynthesis of type IV collagen, thus making
animal models invaluable in the study of pathogenesis and treatment of disease52. So far, these
models are limited to spontaneous AS in dogs and transgenic models of AS generated in mice51.
XLAS models include COL4A5-mutant Samoyed dogs and Navasota dogs, with English cocker
spaniel modelling ARAS, and Bull terrier for ADAS53–57. Murine models are comprised of
COL4A3 knockouts and tg/tg mice58–60. These animal models offer opportunities for
investigation of the molecular pathophysiology of the disease, the roles of type IV collagen
chains in the pathobiology, as well as the applicability of the model in the treatment of AS51.
Understanding the source and extent of the genetic variation underlying AS is crucial in
the management of the disease as clinical care and treatments rely on prognosticating phenotypes
from genetic polymorphisms. Knowledge about the type and location of the mutations adds
significant information about the progress of the renal and extrarenal manifestations of the

6
disease, which could potentially aid in clinical counselling and evaluation of therapeutic
approaches.
1.3 Glomerular basement membrane
The glomerular basement membrane (GBM) is a non-cellular meshwork of extracelluar
matrix (ECM) proteins that plays a central role in the glomerular filtration barrier, separating the
vasculature from the urinary space61. It is situated between the interdigitated podocytes (visceral
epithelial cells) and fenestrated endothelial cells, formed during glomerulogenesis by the fusion
of these two cellular membranes62. It provides not only selective permeability across the
glomerular filtration barrier, but also contributes integral structural support for the glomerular
capillaries62. Moreover, it imparts morphogenic cues that determine the polarization of
subcellular constituents and harbours ligands for cell receptors and transporters on the surface of
adjacent endothelial cells, podocytes, and mesangial cells62. As with all basement membranes,
the four major components of the GBM are type IV collagen, laminin, nidogens, and heparan
sulfate proteoglycans (HSPG), which conjunctively assemble an interwoven meshwork that
imparts size and charge-selective properties63. However, the GBM is unusually thicker than most
other basement membranes and consists of ECM macromolecule isoforms that vary from other
basement membranes (laminin-521, collagen α3α4α5(IV), and agrin), presumably due to its
unique functional properties in establishing and maintaining the glomerular filtration barrier64.
1.3.1 Laminin
Laminin is a ubiquitous basement membrane component that is secreted as heterotrimers
of alpha, beta, and gamma chains65. There are five α chains, four β chains, and three γ chains that

7
assemble to form 15 different heterotrimeric macromolecules. Each distinct laminin trimers are
named based on the specific αβγ chain composition; for instance, laminin α5β2γ1 is referred to
as laminin-521 (LM-521)66. The laminin heterotrimeric glycoprotein is structurally cross-shaped
with the lower long arm of the cruciform assembled by the association of all three α, β, and γ
chains intertwining with one another via coiled-coil interactions and disulfide bonding, forming
laminin coiled-coil (LCC) domains67. The laminin globular (LG) domain is situated at the distal
end of the long arm, consisting exclusively of carboxyl-termini of α chains. The LG domains
mediate interactions between laminin trimers and neighbouring cells by serving as ligands to cell
surface receptors, such as integrins and dystroglycan68. The three other short arms are formed by
alternating globular and rod-like domains, including the amino-terminal globular domain, called
LN domain, which mediates the trimer-trimer interactions in the extracellular space that bring
about laminin polymerization and the initiation of basement membrane assembly64,65,69.
The major laminin trimer found in the mature GBM is LM-521, which is secreted by both
podocytes and endothelial cells69. In the early stages of glomerulogenesis, LM-111 and LM-511
are the major laminin components in the nascent GBM; however, as the GBM matures, major
transitions in the laminin trimer deposition occurs in which LM-111 is initially replaced by LM-
511 and then eventually by LM-521 in the mature glomeruli, the composition of which persists
in the GBM throughout life70. The molecular mechanisms responsible for these developmental
laminin isoform substitutions have yet to be elucidated, but this composition transition is crucial
for glomerulogenesis71. The importance of these laminin transitions is particularly highlighted by
the effects of mutations that prevent them from occurring. For example, a null mutation of
laminin α5 in mice prevents the developmental switch in laminin α chain deposition in which α5
replaces α1 in the GBM during glomerular morphogenesis70. Thus, this gives rise to an aberrant

8
GBM and the subsequent failure of glomerular vascularization. The GBM breakdown most likely
occurs due to the lack of a sufficient concentration of polymerized laminin trimers, as the
laminin network is required to maintain basement membrane integrity. Furthermore, Lama5-/-
mice were shown to exhibit either renal agenesis in one or both kidneys or if both present, the
kidneys were much diminished in size in comparison to those of the littermate controls70,72. The
absence of laminin α5 leads to progressively atypical metanephrogenesis and eventually result in
embryonic lethality.
1.3.2 Type IV collagen
Type IV collagen is the most abundant protein found in the GBM, composed of six
distinct alpha chains 1 through 6, designated Col4α1-Col4α67. The encoded proteins, α1(IV)-
α6(IV) assemble to form three different heterotrimers referred to as protomers: α1α1α2;
α3α4α5; and α5α5α673. Collagen α1α1α2(IV) is synthesized by endothelial cells, mesangial
cells, as well as podocytes of immature glomeruli, while collagen α3α4α5(IV) originates solely
from podocytes74. Like all collagen chains, type IV collagen chains are characterized by a long
collagenous domain of Gly-X-Y amino acid triplet repeats, with glycine being the only residue
small enough to fit inside the collagen helix75. However, unlike other collagen types, type IV
chains consist of multiple noncollagenous interruptions, which impart flexibility to the protomers
and the overall interwoven network they form in the GBM65. The small noncollagenous amino-
terminal domain of all collagen IV α chains is termed 7S and the larger carboxyl-terminal
noncollagenous domain is called NC1, with both domains involved in promoter interactions and
promoting collagen IV network assembly64. The compositions of the protomers are

9
predetermined by the sequence and structure embedded in the NC1, ensuring that only the three
types of heterotrimers form76.
During embryonic development, the α1α1α2(IV) network is the most abundant collagen
IV network in the GBM, and it is gradually replaced by the α3α4α5(IV) heterotrimer in the
glomerulus, cochlea, and eye77. This transition in the composition of collagen IV chains occurs
concurrently with the transition of trimeric laminin chains, which switches from laminin-511 to
laminin-521, as well as the formation of the capillary loops within the maturing glomeruli76. The
molecular mechanisms for the laminin and collagen IV isoform substitutions in the GBM are
unknown. However, the mature α3α4α5(IV) network is more heavily crosslinked with disulfide
linkages and resistant to proteolytic degradation than the immature α1α1α2(IV) network, which
consists of more proteolytic cleavage sites than the α3α4α5(IV) network24. This isoform switch
may be critical for the establishment and maintenance of the permselective barrier properties in
the glomerulus, especially when accommodating the increased blood pressure in the adult74. In
AS, mutations in type IV collagen genes COL4A3, COL4A4, and COL4A5, which encode the
α3α4α5(IV) chains, interfere with the assembly of the α3α4α5(IV) collagen network in the
GBM and hinder the developmental switch from α1α1α2(IV) to α3α4α5(IV) network77. This
persistence of the nascent GBM results in abnormal membranes and clinical features
characteristic of AS, illustrating the importance of the α3α4α5 type IV collagen network in the
GBM.
1.3.3 Nidogen
Nidogens are two homologous basement membrane glycoproteins, designated nidogen-1
and nidogen-2, that are able to bind to the short arms of laminin γ1 chain as well as to type IV

10
collagen62. Thus, they are thought to act as a molecular bridge between the laminin and collagen
IV networks in the basement membrane78. However, the loss of either or both isoforms of
nidogen have no effect on the basement membrane formation, suggesting that nidogens may
provide extra stability to basement membranes under increased stress, but are not required for
their initial development79. Both nidogen-1 and -2 are present in the GBM, but not much is
known about their developmental expression patterns78.
1.3.4 Heparan sulfate proteoglycans
Heparan sulfate proteoglycans (HSPGs) are glycoproteins with a protein core to which
heparan sulfate side chains are covalently linked62. These sulfated glycosaminoglycan side
chains can impart a highly negative charge, which corresponds to the anionic sites within the
GBM that are detectable by cationic probes78. Whilst perlecan is the most prominent HSPG in
most basement membranes and in the mesangial matrix, agrin is the major HSPG in the mature
GBM. During glomerulogenesis, perlecan and agrin are uniformly distributed; thereafter,
perlecan is substituted by agrin and confined to the subendothelial side of the GBM78.
Perlecan, produced primarily by glomerular endothelial cells, is anchored in the basement
membranes by interactions with other constituents, binding to nidogen via its core protein, and to
laminin and collagen IV via its heparan sulfate side chains80. On the other hand, agrin is derived
mainly from podocytes and its N-terminal domain binds to the laminin γ1 subunit, while the C-
terminal LG domain binds to cell surface receptors, such as dystroglycans and integrins63. Thus,
agrin may play a role in cell-matrix adhesion through the affinity of its domain for laminin,
dystroglycan, and integrin.

11
HSPGs in GBM were originally thought to confer charge selectivity in the glomerular
filtration barrier; however, this concept has been recently challenged81. Mice with podocyte-
derived agrin knockout did not lead to any structural or functional defects in the glomerulus,
despite the loss of GBM negativity76. Furthermore, deletions of both agrin and heparan sulfate
side chains on perlecan had little, if any, effects on permselectivity with no signs of proteinuria82.
Hence, no critical role for HSPGs, agrin and perlecan, in the GBM has been proven thus far.
1.3.5 Glomerular basement membrane in Alport Syndrome
Mutations of COL4A3, COL4A4, or COL4A5 interfere with the assembly of the
α3α4α5(IV) network in the GBM, resulting in the impediment of the collagen switch from
α1α1α2(IV) to α3α4α5(IV) network during development4. This persistent distribution of the
primordial α1α1α2(IV) network in the Alport GBM produces abnormal membranes that are less
structurally sound due to fewer intra- and interheterotrimer crosslinks and more proteolytic
cleavage sites than the α3α4α5(IV) network24,83. Thus, the α1α1α2(IV) isoform is more
susceptible to biomechanical strain caused by intraglomerular hypertension and ultrafiltration,
endogenous proteolysis, and eventually results in the characteristic degenerative GBM
splitting84,85. This disposition to proteolytic degradation at the site of glomerular filtration is
augmented by ectopic deposition of laminin chains, α1 and α5, resulting in an overall disruption
of the GBM architecture86. LM-511 increases in regions of focally thickened GBM, which are
more permeable to protein71. Furthermore, the lack of collagen IV and laminin isoform
substitutions in the GBM bring about altered podocyte orientation, podocyte foot process
effacement, and disruption of slit diaphragms. Affected podocytes can transmit this pathology
and injury to adjacent healthy podocytes, giving rise to glomerulosclersosis with an

12
accumulation of ECM, as well as kidney fibrosis due to fibroblast formation by epithelial-
mesenchymal transition, a physiological repair response to injury87,88. Dysregulation of matrix
metalloproteinases (MMPs) in glomerular mesangial cells has also been evidenced in AS, with
their induction shown to contribute to the mechanism of pathobiology, while the blockade of
specific MMP activities has been shown to ameliorate the disease progression89,90. In particular,
MMP-2, MMP-3, MMP-9, MMP-12, and MMP-14 have been most frequently associated with
inflammatory diseases and fibrosis in the literature89–93. Furthermore, a study by Zeisberg et al.
(2006) identified a dichotomous role for MMPs in the progression of AS in Col4α3-/- mice, in
which an MMP upregulation was significantly correlated to deterioration of glomerular function;
however, after the induction of proteinuria and the emergence of fibrosis, MMPs were found to
be renoprotective against disease progression91. Thus, changes in the integrity of the GBM,
brought about by the mutations in the genes encoding collagen type IV α chains, affect cell
signalling mechanisms, and further the pathogenesis of Alport glomerulopathy.
1.4 Current clinical management options
Currently the mechanisms responsible for kidney injury in AS have not been fully
elucidated and the standard of care is limited to nonspecific therapeutic approaches that reduce
renal fibrosis and delay the onset of ESRD94. To date, several treatment options have been
demonstrated to improve outcomes in animal models of AS, including renin-angiotensin system
(RAS) blockade, such as angiotensin-converting enzyme inhibitors (ACE inhibitors) and
angiotensin receptor blockers (ARBs), cyclosporine A, matrix metalloproteinase (MMP)
inhibitors, transforming growth factor beta 1 (TGF-β1) inhibitors, HMG-CoA reductase
inhibition, chemokine receptor 1 (CCP-1) blockade, bone morphogenic protein-7 (BMP-7), stem

13
cell transplantation, and bone marrow irradiation90,91,95–104. Such studies have not only shed light
on an array of potentially effective therapies for AS, but have also contributed significantly in the
understanding of the mechanistic pathways mediating the progression of AS towards ESRD.
Despite the lack of definite treatment for AS, ACE inhibitors are the recommended first
line of treatment for non-immunological therapy of proteinuric glomerular disease105. ACE
inhibitors work by preventing the conversion of angiotensin I to angiotensin II, a growth factor
involved in activating fibroblasts, leading to increased synthesis of matrix proteins, as well as
functioning as a profibrotic cytokine, activating mononuclear cells and increasing
proinflammatory mediators98. The downstream proinflammatory effects of angiotensin II are
mediated via the angiotensin type 2 receptor (AT2R) and the TGF-β pathway, which has been
shown to be important in the renal fibrosis in AS98. Thus, ACE inhibition has been shown to have
antiproteinuric and antifibrotic nephroprotective effects in AS in a time-dependent manner, with
earlier introduction of therapy yielding delayed onset of ESRD and prolonged life
expectancy97,106. Extensive clinical data on the efficacy and safety of ACE inhibitors in patients
with progressive nephropathies are available; for instance, the Evaluation Study of Congestive
Heart Failure and Pulmonary Artery Catheterization Effectiveness (ESCAPE) trial showed that
ACE inhibition with ramipril resulted in low incidence of adverse effects in children with
chronic kidney disease107. However, in the case of patients experiencing adverse reactions to
ACE inhibitors, such as coughs, angioedema, hyperkalemia, as well as decreased glomerular
filtration rate (GFR), ARBs may be used108,109. ARBs inhibit angiotensin II activity specifically
by antagonizing its action on the angiotensin II type 1 receptor (AT1R)110. Long-term treatment
with losartan was found to confer sustained antihypertensive and renoprotective effects with high
tolerance in children with nephropathies111,112. Thus, angiotensin antagonism has been shown to

14
be effective in preserving renal function via its capacity to reduce glomerular hypertrophy and
sclerosis, as well as tubulointerstitial inflammation and fibrosis. This recommended approach to
treatment is well-tolerated and is widely used in patients with AS; however, it does not prevent
ESRD105. Its efficacy is limited and most pronounced when administered at early stages of the
disease, before the onset of microalbuminuria, thus making it a partially effective treatment
option with limitations.
Calcineurin inhibitor, cyclosporine A, has also been experimentally and clinically studied
as a potential treatment option of AS94. Originally introduced into clinical practice as an
immunosuppressant medication, it has been found to have beneficial effects on proteinuria and
renal function when applied in the therapeutic management of AS. A study in a canine model of
XLAS by Chen et al. (2003) showed that cyclosporine induced a significant delay in the onset
and rate of progression of glomerulosclerosis as well as in the deterioration of renal function,
although treatment did not affect the amount of interstitial fibrosis nor yield any beneficial
effects on proteinuria99. In contrast, the examination of the therapeutic efficacy of cyclosporine
in small clinical trials have demonstrated a substantial reduction in proteinuria in Alport patients.
However, cyclosporine usage was also associated with decreased GFR and significant renal
lesions related to cyclosporine nephrotoxicity, thus precluding long-term administration113–115.
Though the mechanisms of actions of cyclosporine in AS have yet to be elucidated, its
antiproteinuric effect seems to stem from its ability to stabilize the podocyte actin cytoskeleton,
independent of its immunosuppressive action116. This discovery sheds further light on the role of
calcineurin signalling in the biology of proteinuric kidney diseases and provides novel
calcineurin substrates, such as synaptopodin, as auspicious starting points for the identification of
antiproteinuric drugs that evade the chronic adverse effects of long-term cyclosporine treatment.

15
Other experimental pharmacological therapies that have been studied with limited clinical
experience include broad spectrum MMP inhibition, TGF-β1 blockade, inhibition of HMG-CoA
reductase, CCP-1 antagonist, and BMP-7. These therapeutic interventions start to give insight
into the pathophysiology of AS and highlight the importance of understanding the underlying
molecular mechanisms of disease before initiating treatment. For instance, the pharmacologic
ablation of MMP-2, MMP-3, MMP-9, and MMP-12, which are responsible for the proteolytic
degradation of GBM, before the onset of proteinuria in Col4α3-/- mice have led to a significant
attenuation in disease progression, marked by delayed proteinuria and prolonged survival91,92.
Likewise, a significant elevation in MMP expression levels were observed in a canine model of
XLAS, implicating their induction with ECM dysregulation and interstitial fibrosis in Alport
kidneys117,118. Thus, MMPs have a contributory role in the pathobiology of Alport renal disease
and their inhibition ameliorate GBM damage, restoring its ultrastructure and function119. TGF-β1
has also been shown to have a potential role in Alport renal disease pathogenesis. A study by
Sayers et al. (1999) observed an induction of TGF-β1 mRNA and proteins in both human and
murine podocytes following the establishment of proteinuria120. Similarly, HMG-CoA reductase
inhibitors, also referred to as statins, which are potent inhibitors of cholesterol synthesis, have
been recognized to have nephroprotective effects in Col4α3-/- mice1. Beyond its role on lipid
reduction, HMG-CoA reductase inhibitor’s pleiotropic effects have been recognized, in which,
for instance in the kidney, it is able to inhibit mesangial cell proliferation, mesangial matrix
deposition, as well as moderate monocyte infiltration and production of TGF-β1101. Thus, the
administration of HMG-CoA reductase inhibitor brought about an attenuation in the expression
of TGF-β, as well as concomitant decreases in proteinuria, renal fibrosis, and inflammatory cell
infiltration, in addition to a prolongation of the lifespan of the KO mice. Other Col4a3-/- mice

16
studies have further illustrated CCP-1 antagonist and the upregulation of BMP-7 as potential new
therapies for use in AS. The usage of BX471, a small molecule CCR-1 inhibitor, was associated
with improved survival of KO mice, as well as decreased interstitial macrophages, tubular
atrophy, and interstitial fibrosis100. Treatment of KO mice with exogenous recombinant human
BMP-7 led to significant decrease in the expression of profibrotic molecules, improved renal
function, histology, and survival in mice, illuminating an overall renal protective effect of BMP-
7102.
Biological interventions, including cell-based therapies and bone marrow irradiation, are
emerging techniques that have been extensively evaluated as a prospective therapeutic options in
AS patients. Cell-based regenerative therapy aims to repair the underlying defect; in the case of
AS, the defective assembly of the α3-α4-α5(IV) chains of collagen in the GBM121. Thus far,
replacement of the mutated genes via gene therapy have not been successful in humans122. In
Alport mice, however, it has been reported that stem cell therapy has yielded therapeutic
benefits, promoting its application for clinical trials. For instance, Ninichuk et al. (2006)
presented that injections of primary bone marrow (BM)-derived multipotent mesenchymal stem
cells (MSCs) into Col4a3 KO mice reduced interstitial fibrosis compared to saline-injected mice,
though marks of renal function, including blood urea nitrogen (BUN), creatinine levels,
proteinuria, and survival were not affected by MSC administration96. Interestingly, MSC was
found to localize to kidneys of the KO mice after injection, but their differentiation into renal
cells was not detected. Similarly, studies by Prodromidi et al. (2006) and Sugimoto et al. (2006)
have independently illustrated that whole BM transplantation is able to ameliorate the chronic
renal injury caused by Col4α3 deficiency in KO mice via differentiation of stem cells into
podocytes that then secrete the missing collagen α3-α4-α5(IV) chains103,104. This is paralleled by

17
decreased serum urea and creatinine levels, reduced interstitial fibrosis, and improved renal
histology. Nonetheless, the extent of podocyte cell engraftment by BM cells was low, suggesting
that some other effect of BM transplantation may be contributing to the functional disease
recovery122. Furthermore, despite reported improvements in renal function as well as glomerular
architecture defects in treated Alport mice compared to control groups, the age at ESRF, a
meaningful endpoint of the disease, was not tested in either studies94,122–124. Contrastingly,
Katayama et al. (2006) reported that BM transplant after lethal irradiation with either WT or KO
BM prolonged the lifespan with similar efficiencies, denoting that the amelioration of disease
observed is conferred most significantly by the irradiation. A positive correlation between the
irradiation dosage and survival time was noted. The work by Katayama et al. challenges the
observations published by Prodromidi and Sugimoto groups and these differences may be
derived from the dissimilar age at the time of BM transplant as well as the varying genetic
backgrounds of the experimental Alport mice, in which Katayama’s study was performed in AS
mice on the 129 SvJ background, while Prodromidi and Sugimoto’s studies were generated in
C57BL/6J strain of Col4a3 KO mice95,103,104. Thus, the different backgrounds and age at which
BM transplantations were completed could have imparted different outcomes, attributable to the
varied severity of GBM defects. Our current knowledge about gene- and cell-based therapies and
their possible efficacies in the treatment of AS is yet insufficient and many experimental
questions need to be addressed before clinical studies are considered in Alport patients125.
Nonetheless, biological interventions, such as regenerative medicine, provide new hope for a
means to restore structural and functional integrity of the diseased kidney in the treatment of AS
and other inherited renal glomerular diseases.

18
Currently there is a lack of therapies that can effectually change the course of disease
progression in patients with AS94. Promising experimental treatments have been developed and
studied that promote the elucidation of the renal pathology of AS. However, despite a variety of
treatment options available, none of these are causal therapeutic strategies that have been as
effective in prolonging survival as ACE inhibition; they merely attenuate and do not prevent the
progression to ESRD1. Hence, for patients with AS who have progressed to renal failure, dialysis
or renal transplantation are the only therapeutic options104. There remains a gap in our
understanding of the early mechanisms that lead to progressive kidney injury in AS which limits
efficacious treatment. Accordingly, the Alport Foundation has issued a call for new studies in the
development of novel treatment approaches to AS.
1.5 Renal inflammation blockade via BRD4 inhibition
The role of inflammation as a major driver in the pathophysiology of CKD has been
widely and compellingly recognized in recent years126. Inflammation contributes to progressive
kidney damage by inducing the release of proinflammatory cytokines and adhesion molecules,
which eventually brings about a loss of glomeruli, tubular atrophy and fibrosis, accompanied by
a decrease in glomerular filtration rate127. Therefore, an understanding of the molecular pathways
driving renal inflammation is indispensable in the elucidation of the pathogenesis of chronic
renal diseases as well as for the development of novel, targeted therapeutics in hopes of
preventing ESRD in renal pathology128.
During the initial stages of renal disease, inflammatory changes are detected with the
concomitant involvements of several inflammatory cytokines, such as tumour necrosis factor-
alpha (TNF-α) and various interleukins (IL-1, IL-6, IL-18), which then activate a number of

19
signalling pathways129,130. The expression of such inflammatory mediators is regulated by the
transcription factor, nuclear factor-kappaB (NF-κB), which has been shown to activate a number
of proinflammatory genes in both human and experimental models of progressive
nephropathies126. The mammalian NF-κB family consists of five members, RelA (p65), RelB, c-
Rel, NF-κB1 (p50; precursor p105), and NF-κB2 (p52; precursor p100), which all share a highly
conserved DNA-binding domain in the N-terminal region called the Rel homology domain
(RHD)131. Through the association of the RHD, the NF-κB proteins are able to form various
homo- and heterodimers with each other, with the most common and best characterized dimer
being the p65/p50 heterodimer132. In addition, the RHD also binds with the inhibitory κB
proteins (IκB), through which the NF-κB heterodimer is sequestered as an inactive complex in
the cytoplasm. In response to a stimulus, such as cytokines, oxidative stress, or bacterial
endotoxin (LPS), the IκB subunit is rapidly phosphorylated by IκB kinase (IKK) and ultimately
degraded133. The resulting release of the NF-κB dimers and their subsequent translocation to the
nucleus promotes the transcription of target proinflammatory genes, such as RANTES, IL-1, IL-
2, IL-6, MCP-1, TNF-α, as well as adhesion molecules, thereby promoting downstream renal
inflammation126.
Recently, it has come to light that the acetylation of the RelA subunit of NF-κB at lysine-
310 is crucial for the transcriptional activation of NF-κB and the succeeding expression of
inflammatory genes (Figure 1)134. Stimulus-coupled acetylation of RelA by p300/CBP at lysine-
310 promotes a direct interaction with bromodomain-containing protein 4 (BRD4) via its two
bromodomains, which then recruits the acetylated NF-κB to the promoter regions of its target
genes134,135. The binding of the BRD4 to acetylated lysine-310 also promotes the kinases within
the positive transcription elongation factor b (P-TEFb) complex, such as cyclin-dependent kinase

20
9 (CDK9), to phosphorylate RNA polymerase II for the transcriptional activation of NF-κB
target genes, thus driving transcription of proinflammatory genes136,137. This masterly epigenetic
regulator, BRD4, belongs to the bromodomain and extra-terminal domain (BET) family,
consisting of BRD2, BRD3, BRD4, and BRDT. A family of transcriptional coactivators and
elongation factors, BET proteins are characterized by the presence of two conserved tandem
bromodomains and an extra-terminal domain138. The N-terminal bromodomains of BET proteins
are able to recognize and bind to acetylated lysine residues on histones and other nuclear proteins
in the regulation of gene transcriptional activity of cellular proliferation and differentiation
processes, while the extra-terminal domain interacts with histone modifiers to bring about
changes in the chromatin structure, thus effecting epigenetic modulations via chromatic dynamic
and nucleosome assembly modifications139.
Of all the mammalian BET proteins, BRD4 is the most extensively studied isoform and is
broadly implicated in the regulation of renal inflammation140. Given its role in the regulation of
the innate and adaptive immune responses, however, a selective and temporal inhibition of NF-
κB’s proinflammatory activity has been explored as of late, as a complete suppression of NF-κB
may lead to adverse effects141. Recent studies have demonstrated that targeted inhibition of NF-
κB transcriptional activity brings about an attenuation of inflammation in experimental models
of kidney injury. For instance, Zhang et al. (2012) have shown that BET-specific bromodomain
inhibitor, MS417, designed to block BRD4 from binding to the acetylated NF-κB, significantly
downregulates the expression of proinflammatory cytokine and chemokine genes in human renal
tubular epithelial cells, as well as reducing proteinuria, improving renal function, and effectively
ameliorating NF-κB acetylation and in parallel, the expression of its target genes in Tg26 mice,
an established animal model for HIV-associated nephropathy (HIVAN)140. Likewise,

21
administration of the same NF-κB inhibitor, MS417, in db/db mice was shown to attenuate
proteinuria and podocyte injury in diabetic kidney disease142. Hence, these findings strongly
suggest that the selective inhibition of NF-κB activity via BET bromodomain blockade,
represents a new therapeutic approach for treating NF-κB-mediated inflammation and kidney
injury.
Currently the specific effects of NF-κB signalling in experimental AS have not been
extensively studied in the literature. However, recent findings involving the usage of this
aforementioned novel compound, MS417, in the blockade of NF-κB activation in other renal
disease models seem to be promising140,142. The inhibition of BRD4 not only illustrates the
pathophysiologic functions of NF-κB, but it also highlights the significant role of inflammation
in mediating renal disease progression. Thus, these data motivate a pivotal need to investigate the
collaborative roles of NF-kB and BRD4 in the regulation of proinflammatory activation in the
pathogenesis of AS in hopes that targeting epigenetic regulators such as BET proteins may
contribute in the elucidation of the etiology and progression of AS.

22
Figure 1. Molecular mechanism of BRD4-regulated inflammation and the inhibition of inflammatory gene transcription with MS417. Inflammatory stimulus consisting of the binding of ligand to a cell surface receptor, such as Toll-like receptor 4 (TLR4), leads to the recruitment of I kappa B kinase (IKK) complex, which in turn leads to the phosphorylation and degradation of the IκB inhibitor. This frees and activates the NF-κB dimers, p65 and p50. Active NF-κB is translocated to the nucleus, where it binds to consensus sequences in the regulatory elements of gene promoters. The transcription factor recruits BRD4 and together NF-κB and BRD4 control the transcription of inflammatory response genes. BRD4 also helps recruit RNA polymerase II to initiate gene transcription. However, MS417, a BRD4 inhibitor, prevents BRD4 from binding to NF-κB, limiting the recruitment of RNA polymerase II to the transcriptional complex140,142. Thus, the blockade of BRD4 binding to the acetylated NF-κB using MS417 can effectively attenuate NF-κB transcriptional activation of proinflammatory genes.

23
1.6 Experimental design and hypothesis
Sterile inflammation is an innate immune response that is vital for tissue and wound
repair in response to trauma or ischemia-reperfusion injury in the absence of any
microorganisms143. Similar to pathogen-induced inflammation, sterile inflammation is marked by
the recruitment of neutrophils and macrophages, bringing about the production of
proinflammatory cytokines and chemokines, such as TNF and IL-1144. Although inflammation is
important in the resolution of the initial insult, chronic inflammation may lead to emergence of
disease, contributing to the pathophysiology127. Therefore, this study sought to examine the
pathways that result in sterile inflammation in experimental AS, in particular the impact of NF-
κB inhibition via the administration of a BRD4 antagonist.
In order to discern the changes in the patterns of gene expression in the Alport kidney, a
microarray was performed using 4-week-old KO and WT glomeruli as described in Chapter 2.
IPA approach was subsequently used to analyze the differential expression data in hopes of
better understanding the biological changes that occur with the onset of the disease, as well as to
predict the upstream transcriptional regulators to uncover potential therapeutic targets. Once the
molecular alterations of the disease were determined, pharmacologic inhibitor of BRD4 was
administered in HK-2 cells and in KO mice to better define the role of NF-κB in the
pathogenesis of AS.
In summary, I hypothesize that NF-κB will attenuate kidney injury in mice with AS.

24
Chapter 2
Materials and Methods
2.1 Animals
Col4a3+/+ (wildtype; WT) and Col4a3-/- (KO) mice of 129/SvJ background were
purchased from The Jackson Laboratory (Bar Harbor, ME, USA)58. All animals were housed at
the Division of Comparative Medicine at the University of Toronto, and fed standard chow diet
with free access to food and water. Only male mice were used for experiments to avoid the
potential confounding effects of female sex hormones. All experiments were conducted under the
guidelines of the University of Toronto Animal Care Committee.
Male mice were followed from 4 weeks of age until sacrifice and tissue harvest at 7
weeks of age. 24-hour urine samples were obtained at 7 weeks of age by placing animals
individually in metabolic cages in order to perform urinary albumin measurements. At sacrifice,
mice were anesthetized with inhaled isoflurane and their body weights and kidney weights were
recorded. Blood samples were collected from the carotid artery and both kidneys were dissected
out. The kidneys were cross-sectioned into 3 parts, with two polar sections snap-frozen in liquid
nitrogen and stored at -80°C until use. Middle sections of kidneys were fixed in buffered
formalin and embedded in paraffin for histological analysis. The genotypes of study mice were
verified by tail clip genotyping PCR via the usage of the following primers: common, 5’-
CCAGGCTTAAAGGGAAATCC-3’; WT reverse, 5’-TGCTCTCTCAAATGCACCAG-3’; and
mutant reverse, 5’-GCTATCAGGACATAGCGTTGG-3’.
2.2 MS417 treatment
Male WT and KO mice were administered with either a control vehicle (0.1% DMSO in

25
PBS) or MS417 by daily oral gavage at a dosage of 0.0016 mg/kg. MS417 was provided by Dr.
John Cijiang He (Mount Sinai School of Medicine, New York, NY, USA)140,142. The mice were
fed this compound daily from the age of 4 weeks to sacrifice at 7 weeks of age. The mice were
euthanized at 7 weeks of age for blood, urine, and kidney collection. Body weight was recorded
daily from the start of the experiment till sacrifice for all experimental groups.
For the glomerular microarray study, male WT and KO mice were administered with
either a control vehicle (0.1% DMSO in PBS) or MS417 by daily oral gavage at a dosage of
0.0016 mg/kg. The mice were fed this compound daily from the age of 4 weeks till they were
sacrificed 10 days later.
2.3 Blood biochemistry
Blood samples were collected from carotid artery with Microvette (Sarstedt Inc.,
Montreal, QC, Canada) according to the manufacturers’ protocol at the time of sacrifice. Serum
was isolated by centrifuging blood samples at 2000 x g for 5 minutes at room temperature and
was then stored at -80°C until use. Levels of blood biochemical parameters, including blood urea
nitrogen, creatinine, sodium, potassium, chloride, phosphorus, calcium, and total proteins, were
measured at the Toronto Centre for Phenogenomics (Toronto, ON, Canada).
2.4 Urinary albumin excretion
24-hour urine samples were obtained by placing experimental animals individually in
metabolic cages (Nalgene, Nalge Nunc International, Rochester, NY, USA). Urine samples were
centrifuged at 8000 x g for 5 min at room temperature and the supernatants were collected and
stored at -80°C until use. Albumin levels were determined with Albuwell M Kit (Exocell,

26
Philadelphia, PA, USA) following the manufacturers’ guide. Urinary albumin levels were used to
calculate the 24h urinary albumin excretion (UAE) rate.
2.5 Isolation of mice glomerli
The glomerular isolation procedure was adapted from a magnetic bead-based isolation
method described by Takemoto et al. (2002) and Schwarz et al. (2013). An illustrated flow chart
of the protocol is shown in Figure 2145,146.
M-450 tosylactivated, 4.5 µm diameter Dynabeads (Invitrogen, Carlsbad, CA, USA)
were inactivated according to manufacturer’s instructions. Congenic male WT and KO mice at 4
weeks of age were used. At the time of kidney glomeruli harvest, mice were anesthetized and
perfused with 10mL of Hank’s balanced salt solution (HBSS; Invitrogen, Carlsbad, CA, USA)
and then 10mL of 8 x 107 magnetic Dynabeads diluted in HBSS through the left ventricle of the
heart at a constant perfusion speed of 2.3ml/min using Syringe Infusion Pump (Harvard
Apparatus, Holliston, MA, USA). Once the perfusion was completed, kidneys were removed,
minced into 1mm3 pieces, and digested with 1mg/ml collagenase A (Roche Diagnostics,
Indianapolis, IN, USA) in 3ml of HBSS at 37°C for 30 minutes with gentile agitation. The
digested tissue was passed through a 100 µm cell strainer (Thermo Fisher Scientific, Waltham,
MA, USA) using a flattened syringe pestle and the cell strainer was then washed 3 times with 1
ml of PBS. The cell suspension containing intact glomeruli with trapped paramagnetic
Dynabeads was placed into a magnetic particle concentrator (Invitrogen, Carlsbad, CA, USA) for
7 minutes. The glomeruli containing Dynabeads were gathered on the wall of tubes; the
supernatant (containing smaller tubular fragments, single tubular cells, a variety of polymorphic
interstitial cells, and blood cells) and pellets (containing larger tubular fragments) were then

27
carefully pipetted into separate tubes and stored on ice. The glomeruli and larger tubular
fragments were washed for at least three times with PBS. All procedures were performed on ice
except the collagenase digestion. The purity of the glomerular and tubular isolates was verified
under light microscopy. To prove the glomerular and tubulointerstitial origin of separated tissue
fractions, the mRNA expression levels of glomerular (Nphs1 for podocyte) and tubular (Fxyd2
for distal tubules) markers were also examined (Figure 3). Isolated glomeruli samples were
resuspended in QIAzol Lysis Reagent and stored in -80°C.

28
Figure 2. Flow chart of glomeruli isolation from Col4a3-/- mice. Anesthetized mice are perfused with Dynabeads (depicted by blue circles) diluted in HBSS through the left ventricle of the heart. The kidneys are removed, minced into 1mm3 pieces, and then chemically digested in collagenase for 15min at 37°C. The collagenase-digested tissue is then gently filtered through a 100µm cell strainer. The supernatant is discarded and the cell pellet resuspended in HBSS. The glomeruli containing Dynabeads are then collected by a magnetic particle concentrator145,146.

29
Figure 3. RT-PCR of podocyte and distal tubular markers for microarray sample selections. Representative gels illustrating whether glomeruli RNA samples isolated from WT and KO mice had tubular contamination was evaluated via RT-PCR using podocyte (Nphs1) and tubular (Fxyd2) markers. The first column shows an isolated glomeruli sample along with cDNA controls from glomeruli, tubules, renal cortex (RC) sample from a 7-week-old mouse, and RC sample from a 4-week-old mouse, along with a negative control (NC).

30
2.6 Microarray data and bioinformatics analysis
By using Affymetrix Mouse Gene 2.0 ST Arrays (Affyetrix, Santa Clara, CA, USA), the
global gene profiling of glomerular samples from male WT and KO mice at 4 weeks of age (n =
8 per group) was performed. Then in order to test whether the early genetic changes observed in
the disease model could be reversed by the anti-inflammatory drug, MS417, the global gene
profiling of glomerular samples from male vehicle-treated WT mice (n = 5), vehicle-treated KO
mice (n = 9), and MS417-treated KO mice (n = 2) was performed. For all microarray studies, the
total RNA containing small RNA was extracted using RNeasy Mini Kit (Qiagen Inc.,
Mississauga, ON, Canada) following the manufacturer’s protocol with an on-column DNA
digestion step to minimize genomic DNA contamination. The sample integrity of the RNA was
assessed using the RNA 6000 Nano Assay on 2100 Bioanalyzer (Agilent Technologies, Inc.,
Santa Clara, CA, USA) to ensure that RNA integrity number (RIN) was greater than 7.
Microarray experiments were performed at the Microarray Analysis and Gene Expression
Facility at The Hospital for Sick Children (Toronto, Ontario, Canada). Following the
manufacturer’s protocol, 125 ng of total RNA was labelled using the GeneChip WT PLUS
Reagent Kit (Affymetrix, Santa Clara, CA, USA). Fragmented and biotin-labelled ss-cDNAs
were then hybridized to GeneChip Mouse Gene 2.0 ST Arrays for 16 hours at 45°C. GeneChip
Mouse Gene 2.0 ST Arrays feature probe sets for 28,137 coding transcripts, 7,103 non-coding
transcripts, 2,000 long intergenic non-coding transcripts (lincRNA), with an average of 21
unique probes across each gene. Hybridized arrays were then stained and washed in the
Affymetrix Fluidics Station 450. Thereafter, the arrays were scanned on an Affymetrix GeneChip
Scanner 3000 and the image (.DAT) files were preprocessed using the Affymetrix GeneChip
Command Console (AGCC) software v.4.3 to generate cell intensity (.CEL) files. After image

31
processing, the array data was uploaded to the Affymetrix Expression Console software v1.4.1
for further processing and quality control. All quality assessment metrics, including spike-in
controls during target preparation and hydrization, were found within the boundaries. The probe
set signal intensities were then extracted and normalized using the robust multi-array average
(RMA) algorithm embedded in the Expression Console software, which consists of convolution
background correction, quantile normalization, and median polish summarization. Downstream
supervised statistical analysis was carried out via Partek Genomics Suite 6.6 (Partek Inc.,
Chesterfield, MO, USA) to determine differentially expressed genes affected by the genotype
and treatment using a one-way ANOVA and a false discovery rate (FDR) equal to or less than
10%. Ingenuity Pathway Analysis (IPA; Qiagen Silicon Valley, Redwood City, CA, USA) was
used to determine enriched biological processes, disease or toxicological functions, signalling
and metabolic canonical pathways, upstream regulators, and gene pathways and networks in the
context of the gene expression changes in experimental Alport Syndrome.
2.7 Cell culture and NF-κB activity assay
Human kidney-2 cells were sub-cultured in 6-well plates for 24 hours and co-transfected
with 0.4 ug/well of pNF-κB-Luc plasmid (Stratagene, Agilent Technologies, Inc., Santa Clara,
CA, USA) and 3 ug/well of pRL-TK reporter vector (Promega Corp., Madison, WI, USA) using
the Effectene Transfection Reagent Kit (Qiagen, GmbH, Hilden, Germany) according to the
manufacturers’ guides. Cells were incubated for 17 hours then subjected to Angiotensin II (10-7
mol/L) treatment with or without MS417 (1 uM) for 24 hours. Luciferase activity was
determined with the Dual-Luciferase Reporter Assay System (Promega Corp., Madison, WI,
USA) and the light emission was read by FB12 Luminometer (Titertek-Berthold, Berthold

32
Detection System GmbH, Pforzheim, Germany). Total protein measured with Bradford Assay
(Bio-Rad, Hercules, CA, USA) was used to normalize the activity results.
2.8 Real-time RT-PCR
Total RNAs from cortical and glomerular samples were isolated using RNeasy Mini Kit
and reverse transcribed into cDNA with the QuantiTect Reverse Transcription Kit (Qiagen Inc.,
Misssissauga, ON, Canada). For the cortical samples, the mRNA expression levels for TNF-α,
TGF-β1, IL-6, and IL-1β were quantified by real-time PCR (TaqMan; Thermo Fisher Scientific,
Waltham, MA, USA) by using a sequence detection system (ABI Prism 7900; Applied
Biosystems, Foster City, CA). GAPDH was used as internal control. For the glomerular samples,
the mRNA expression levels for Fxyd2 and Nphs1 were quantified by semi-quantitative PCR.
2.9 Statistical analysis
All results are shown as mean ± S.E. Statistical analyses were performed using GraphPad
Prism 5 (GraphPad Software, Inc. La Jolla, CA, USA). For multiple group comparisons, one-
way ANOVAs with Tukey’s range test were performed, and for two-group comparisons,
unpaired t-tests were performed. Statistical significance was set at a p-value of less than 0.05.

33
Chapter 3
Results
3.1 Characterization and breeding of murine model of Alport Syndrome
In order to better understand the molecular pathways associated with renal disease
progression and address the call for new therapeutic options, a well-characterized experimental
murine model of AS with a Col4a3 knockout raised on a 129/SvJ genetic background was
employed for the study. To produce a cohort of mice for experiments, two heterozygous mutant
mice were bred together and succeeding heterozygous progenies were used for further breeding.
The genotypes of study mice were verified by PCR and only male Col4a3-/- mice and wildtype
(WT) littermate control mice were used for the study (Figure 4). The developmental collagen IV
switch has been demonstrated in the Col4a3-/- mice between 4 to 7 weeks of age (Figure 5). It is
evident that by 7 weeks of age, the kidneys of Col4a3-/- mice fail to undergo the normal collagen
IV network switch; Figure 5 illustrates the markedly decreased expression levels of collagen IV
α3, α4, and α5 genes in the Col4a3-/- kidneys, while the expressions of both α1 and α2 genes
were increased compared to that of the age-matched WT controls.
The structural and functional manifestations of the renal pathology of Col4a3-/- mice have
been comprehensively reviewed in the literature, establishing the experimental disease model
extensively and solidly58,147–154. Histopathologic kidney injury was pronounced in the 7-week-old
Col4a3-/- mice on Periodic acid-Schiff- and Masson’s trichrome-stained sections, along with
tubular dilatation, tubulointerstitial scarring, and fibrosis compared with the WT mice (Figure 6).
Furthermore, Col4a3-/- mice exhibited albuminuria with a significant increase in urinary albumin
excretion (UAE) as early as 4 weeks of age compared to WT mice (Figure 7A). Serum creatinine
levels were progressing in an increasing trend in the 7-week-old Col4a3-/- mice, however, the

34
difference did not reach statistical significance (Figure 7B, p = 0.18). Thus, the macroscopic and
microscopic renal examinations illustrated how this Col4a3 knockout model mirrors that of the
human AS.

35
Figure 4. Col4a3 KO mice breeding scheme and PCR genotyping. The breeding scheme for generating experimental groups as well as the maintenance of the mice colonies were effectuated via pairing of two heterozygous mutants (A). Only Col4a3+/+ and Col4a3-/- mice were utilized as experimental groups for the study. Panel B then shows the representative PCR blot of the genotypes of mice used for the study as well as in generation of the Col4a3-/- mouse line verified by PCR (B). The first loaded sample is of Col4a3 KO sample with WT sample loaded next. The third column is of the heterozygous sample152.
309 Bp
230 Bp
Col+/- Col-/- Col+/+
A
B

36
Figure 5. Heat map of collagen IV α1-α5 expression levels in Col4a3-/- kidneys. The gene expression levels for collagen IV α1-α5 in kidney tissue derived from the microarray analysis of 4- and 7-week-old WT and Col4a3-/- mice (latter 7-week-old dataset highlighted with a green box). It is evident that there is an impaired collagen IV network switch in the KO mice between 4 to 7 weeks of age. In the 7-week-old KO kidney, there is an absence of Col4a3, Col4a4, and Col4a5, indicated by the blue squares, as well as a persistence of Col4a1 and Col4a2, indicated by the red squares, compared to the age-matched WT kidney. Each column represents an individual mouse sample and each row represents an individual collagen gene. Red colour indicates upregulation and blue represents downregulation152.

37
Figure 6. Histopathologic injury in Col4a3-/- and WT kidneys. The renal phenotypes of Col4a3-/- (KO) and WT mice at 4 and 7 weeks of age presented in Periodic acid-Schiff-stained and Masson’s trichrome-stained sections. The KO mice display minimal glomerular abnormalities and normal tubulointerstitium compared to WT mice at 4 weeks of age. However, by 7 weeks of age, moderately severe glomerular and tubulointerstitial scarring was evident in the KO but not WT mice. Similarly, there was very little fibrosis evident in 4-week-old KO kidneys compared to the age-matched WT kidneys. By 7 weeks of age, the KO kidneys exemplify extensive tubulointerstitial fibrosis compared to WT mice evidenced by the green protein casts in MT-stained samples152. Insets in PAS-stained sections show the glomerulus. Original magnification: 100x, insets 200x.

38
Figure 7. Functional manifestations of renal pathology of Col4a3-/- mice. Urinary albumin excretion (A) and serum creatinine levels (B) in WT and KO mice at 4 and 7 weeks of age. At 4 weeks of age, a slight increase in urinary albumin excretion, but normal serum creatinine levels in the KO mice as compared to control WT mice. However, by 7 weeks of age, there was a marked increase in albuminuria excretion measure in KO mice, as well as an increase trend in plasma creatinine level, although it was not statistically significant (p = 0.18) Data are expressed as means ± SEM. *p < 0.05 versus WT152.
A B

39
3.2 Early microarray studies in glomeruli
To elucidate the molecular pathways associated with renal disease progression, total RNA
was extracted from glomeruli of 4-week-old male wildtype (WT) and Col4a3-/- (KO) mice
(n=8/group) and a microarray performed using Affymetrix GeneChip Mouse Gene 2.0 ST Array.
The purity of glomeruli samples was evaluated via RT-PCR using podocyte (Nphs1) and tubular
(Fxyd2) markers prior to the microarray analysis (Figure 3). The purity of the RNA glomeruli
samples without any tubular contamination was also quality checked via Bioanalyzer and only
those with RNA of greater 7 were utilized for the microarray study.
Figure 8 shows the heat map highlighting the marked differential expressions of genes in
the glomeruli of 4-week-old WT and KO mice. It presents a very distinct pattern of genes that
are upregulated or downregulated even at 4 weeks of age in the glomeruli of WT and KO mice,
comprising of genes which are involved in a wide variety of biological processes. Table 1 shows
the Ingenuity Pathway Analysis (IPA) predicted activated upstream regulators that may be
responsible for the gene expression changes observed. It identified 55 unique transcription
factors and proteins in the Col4a3 KO glomeruli, with the transcription factor, NF-κB, predicted
by IPA to be the most activated of all upstream regulators. Figures 10, 11, and 12 show the heat
maps of differentially expressed target genes of IL-1β, TLR4 and MYD88, and NF-κB in the
glomeruli of 4-week-old WT and KO mice, respectively. They all highlight the distinct patterns
of gene upregulation and downregulation even at 4 weeks of age. Figure 9 maps the activated
signal transduction pathways in experimental AS as predicted by IPA in 4-week-old KO
glomeruli. It was shown that there are changes in the collagen protein levels in the extracellular
matrix, levels of cytokines, as well as a number of membrane receptors, such as TLR4, TNF-α,

40
and IL-1β receptors, which all converge on the transcription factor, NF-κB. NF-κB, thereafter,
influences a number of inflammatory genes.

41
Figure 8. Levels of differential gene expression in kidney tissues in WT and KO mice. Heat map of marked differential gene expression levels in the glomeruli isolated from 4-week-old WT and KO mice (n = 8 for both groups). Columns represent kidney samples, rows present different genes, and each cell indicates the expression value of the gene in that sample. Red colour indicates increased expression relative to mean (white colour), whereas blue colour indicates decreased expression relative to mean. Courtesy of Dr. Xuewen Song and Dr. York Pei.

42
Table 1. 55 Ingenuity Pathway Analysis predicted activated upstream regulators in 4-week-old KO glomeruli. 55 Ingenuity Pathway Analysis (IPA) predicted activated upstream regulators in Col4a3-/- glomeruli. The upstream regulators are arranged by the z-score, which predicts the activation state of specific upstream regulators using expression patterns of downstream target genes. An upstream regulator is considered activated and significant if equal to or greater than 2. A z-score of equal to or less than -2 is considered an inhibited upstream regulator. Bolded upstream regulators suggest activation of Toll-like receptor (TLR) signalling. Regulators indicated with an asterisk (*) signal downstream of FREM1. Courtesy of Dr. Song and Dr. Pei.

43
Figure 9. Schematic summary of aberrant activation of signalling pathways in AS mice. Map of signalling pathways in AS as predicted by IPA. Upregulated genes are labelled in red and downregulated genes are labelled in green. Genes that were not differentially expressed at the mRNA level are labelled in black. Genes that are predicted to be activated by the IPA upstream regulator analysis is indicated by a red asterisk and genes that are predicted to be inhibited is marked by a green asterisk. Genes highlighted in blue (a-c) are genes whose altered levels of differentially expressed target genes were further examined and visualized via heat maps (presented in subsequent figures). Courtesy of Dr. Xuewen Song and Dr. York Pei.

44
Figure 10. Levels of differentially expressed IL-1β target genes. Heat map of differentially expressed target genes of IL-1β in the glomeruli of 4-week-old KO and WT mice (n = 8 for both groups). Columns represent kidney samples, rows present different genes, and each cell indicates the expression value of the gene in that sample. Upregulated genes are labelled in red and downregulated genes are labelled in blue. Courtesy of Dr. Xuewen Song and Dr. York Pei.

45
Figure 11. Levels of differentially expressed TLR4 and MYD88 target genes. Heat map of differentially expressed target genes of TLR4 and MYD88 in the glomeruli of 4-week-old KO and WT mice (n = 8 for both groups). Columns represent kidney samples, rows present different genes, and each cell indicates the expression value of the gene in that sample. Upregulated genes are labelled in red and downregulated genes are labelled in blue. Courtesy of Dr. Xuewen Song and Dr. York Pei.

46
Figure 12. Levels of differentially expressed NF-κB target genes in kidney tissues of WT and KO mice. Heat map of differentially expressed target genes of NF-κB in the glomeruli of 4-week-old KO and WT mice with red depicting upregulation and blue representing downregulation (n = 8 for both groups). Columns represent kidney samples, rows present different genes. Interestingly, the heat map shows that mRNA levels for several genes regulated by NF-κB actually decreased. The mechanism responsible for these changes were not addressed in this current study. It possibly represents secondary effects downstream of the original stimulus for the activation of NF-κB. Courtesy of Dr. Xuewen Song and Dr. York Pei.

47
3.3 Targeting NF-κB in vitro
In order to determine whether there was any biological effect of MS417 on NF-κB
inactivation, the NF-κB luciferase activity was measured in human kidney-2 (HK-2) cells
cultured in medium containing angiotensin II (Ang II), with or without the NF-κB-blocking
compound, MS417. HK-2 cells were transfected with an NF-κB reporter construct and the NF-
κB activation activity was determined by measuring the luciferase activity. As expected, Ang II
caused a robust increase in NF-κB activity in HK-2 cells transfected with the NF-κB reporter
construct. This effect was attenuated with MS417 treatment, which inhibited activation of Ang
II-induced NF-κB (Figure 13).

48
Figure 14. MS417-inhibited Ang II-induced NF-κB activation in HK-2 cells. Human-kidney 2 cells were transfected with pNF-κB-Luc plasmid as described previously. After 24 hours of incubation with Ang II (10-7 mol/L) with or without MS417 (1 uM), cells were lysed and the lysates were used for luciferase activity assay. Ang II stimulated the luciferase activity and the treatment with MS417 attenuated the Ang II-induced rise in NF-κB activation in the HK-2 cells. n = 3 for all groups. *p < 0.001 vs. transfection control; † p < 0.001 vs. Ang II-treated group.

49
3.4 Analysis of NF-κB inhibition in vivo using whole kidney samples
3.4.1 Whole animal kidney examination
Compared to corresponding sham animals, there was no significant change in body
weights after MS417 treatment in either WT mice or Col4a3 KO mice, indicating no apparent
toxicity observed based on body weight measurements (Figure 14). No mortality in either
untreated and treated groups were observed during the course of the experiment (data not
shown). BUN and creatinine levels were measured to assess kidney function. Plasma BUN was
increased in vehicle-treated WT kidneys (Figure 15). However, compared to control, the plasma
BUN level was not significantly altered with MS417 treatment in the KO kidneys. Plasma
creatinine values were changed to a similar extent in both WT and MS417-treated KO animals
(Figure 16).
To determine if MS417 treatment would help alleviate kidney function impairment, the
urinary albumin excretion rates were measured for all experimental groups (UAE, Figure 17).
The vehicle-treated KO mice had elevated UAE, but despite a trend of a decrease in the change
in albuminuria level, the UAE failed to reach statistical significance when compared to the WT
mice (Figure 17).

50
Figure 14. Body weight change measurements in WT and KO mice. Body weight measurements were recorded from the start of the treatment at 4 weeks of age till sacrifice at 7 weeks of age for all experimental groups. There were no significant differences among the three experimental groups in their body weight measurements at the time of sacrifice. Results are shown as mean ± SE. n = 4 for vehicle-treated WT; n = 3 for vehicle-treated KO; n = 5 for MS417-treated KO.

51
Figure 15. Blood urea nitrogen (BUN) levels in 7-week-old WT and KO mice following vehicle or MS417 treatment. Plasma samples were obtained at sacrifice at 7 weeks of age after 3 weeks of daily treatment. BUN levels were measured with frozen plasma samples. MS417 treatment trended towards a reduction in the BUN levels in the KO kidneys compared to the vehicle-treated KO kidneys, but the difference failed to reach statistical significance. Results are presented as mean ± SE. n = 13 for WT sham; n = 9 in vehicle-treated KO group; n = 9 in MS417-treated KO group. *p < 0.05 compared to WT sham; p = 0.12 for MS417-treated KO group vs vehicle-treated KO group.

52
Figure 16. Serum creatinine levels assessed in 7-week-old animals following vehicle or MS417 treatment. Creatinine levels were measured with frozen plasma samples. There was a clear rise in the serum creatinine level in the vehicle-treated KO kidneys, which was attenuated with the administration of MS417; however, the difference failed to reach statistical significance. Results are presented as mean ± SE. For WT with vehicle treatment, n = 13; n = 9 for KO with vehicle treatment; n = 9 for KO with MS417 treatment. *p < 0.05 compared to WT sham; p = 0.21 for MS417-treated KO kidneys compared to vehicle-treated KO kidneys.

53
Figure 17. Urinary albumin excretion (UAE) assessed in 7-week-old animals. Body weight measurements were recorded from the start of the treatment at 4 weeks of age till sacrifice at 7 weeks of age for all experimental groups. The rise in albuminuria observed in the vehicle-treated KO group is decreased with MS417 treatment, though the difference failed to reach statistical difference. Results are shown as mean ± SE. n = 10 for all groups. *p < 0.05 compared to WT sham; p = 0.07 for MS417-treated KO vs vehicle-treated KO.
*

54
3.4.2 Proinflammatory cytokine expression
Renal inflammation and the accumulation of macrophages play an important role in
kidney injury. Thus, the expression profiles of proinflammatory cytokines, interleukein-6 (IL-6)
and interleukin-1β (IL-1β) were assessed in cortical kidney samples as indicators of
inflammation and disease progression (Figure 18). The measurement of mRNA levels of
proinflammatory cytokines, IL-6 and IL-1β, showed dramatic induction of all genes in vehicle-
treated KO mice compared to the kidneys of WT mice. However, the mean mRNA levels of IL-6
and IL-1β were lowered in the kidneys of the MS417-treated KO mice compared to the kidneys
of WT mice with a statistically significant difference for IL-1β (Figure 18). The differences were
not statistically significance when the proinflammatory mRNA expression levels of MS417-
treated kidneys were compared to vehicle-treated KO kidneys.

55
Figure 18. Proinflammatory cytokine levels in kidney tissue in WT and Col4a3 KO mice after sham or MS417 treatment. mRNA expression levels of IL-6 (A) IL-1β and (B) TNF-α in WT and KO mouse kidney after vehicle or MS417 treatment. GAPDH was used as internal control. Results are normalized to WT sham and presented as mean ± SE. n ≥ 10 in each experimental group for IL-6 and IL-1β. n values are varying per experimental group as during the performance of the experiments, amplifications failed in some of the wells and were omitted for the data analysis. *p < 0.05 compared to WT sham; p = 0.19 for MS417-treated KO vs vehicle-treated KO (A); p = 0.54 for MS417-treated KO kidney vs vehicle-treated KO kidney (B).
A B

56
3.5 Analysis of NF-κB inhibition in vivo via microarray studies of isolated glomeruli
To determine whether there were any changes in the molecular pathways linked to the
disease progression of Alport Syndrome with the administration of MS417, the total RNA was
extracted from the glomeruli of 38-day-old male mice from three experimental groups: WT with
vehicle treatment; KO with vehicle treatment; and KO with MS417 treatment (n = 7 for all
experimental groups). As previously described, the purity of the glomerular RNA samples to
ensure the absence of tubular contamination was evaluated via RT-PCR using podocyte and
tubular markers (Figure 3). Table 2 shows the summary of the glomerular isolation perfusions
performed, the number of glomeruli RNA samples with RIN higher than 6, the number of RNA
samples sent for Bioanalyzer analysis, and the number of RNA samples used for the microarray
analysis. Table 3 lists the RNA glomeruli samples that were selected for the microarray study.
When the microarray analysis was performed, it became evident that the assignment of the
genotypes to the experimental animals was incorrect. Table 4 then lists the newly assigned
genotype and treatment grouping after an inaccuracy in the genotype assignment in the
experimental group was discerned. A total of 21 glomeruli samples were utilized for the study.
A microarray was then performed using Affymetrix GeneChip Mouse Gene 2.0 ST Array
on these samples. Figure 19 shows the heat map of the differential gene expression levels in the
glomeruli of WT and KO mice after 10 days of either sham or MS417 treatment. The initial
changes in gene expression that was previously observed in the glomeruli of 4-week-old mice in
vehicle-treated WT and KO groups were sustained in this experiment. However, there was no
significant marked differential expressions of genes in the MS417-treated KO group when
compared to the vehicle-treated KO group.
Figures 20, 21, and 22 illustrate the heat maps of differentially expressed target genes of

57
IL-1β, TLR4 and MYD88, and NF-κB in the glomeruli of WT and KO mice treated for 10 days
with sham or MS417, respectively. Once again, the distinct patterns of marked differential gene
expression noted in the 4-week-old WT and KO glomeruli are conserved in the glomeruli after
the 10-day treatment with sham or MS417. The 10-day treatment of MS417 in KO mice did not
alter the gene expression patterns of NF-κB, IL-1β, and TLR4 and MYD88 targets compared to
that of the vehicle-treated KO mice.

58
Table 2. Summary of glomerular isolation perfusions performed and RNA yield qualities for analyses. A total of 34 perfusions were completed on three experimental groups of WT vehicle (n = 15), KO vehicle (n = 8), and KO treatment (n = 11) mice, which yielded n = 11, n = 7, and n = 7 of acceptable-quality RNA samples (RIN > 9) for WT vehicle, KO vehicle, and KO treatment groups, respectively. RIN score of greater than or equal to 6 is considered a good quality RNA suitable for analysis155. A total of 25 RNA samples were submitted for Bioanalyzer analysis and a total of 21 RNA samples were utilized for the microarray analysis. Courtesy of Dr. Xuewen Song and Dr. Pei York.

59
Table 3. RNA quality of glomeruli samples selected for microarray study. The RNA concentration and the sample purity levels (260/280 and 260/230) levels are shown for the individual RNA samples that were selected for the microarray study. In total, 21 RNA samples were submitted, which is comprised of n = 7 for each experimental group of WT vehicle, KO vehicle, and KO treatment. A 260/280 ratio of approximately 2.0 or higher is acceptable as pure for RNA and a 260/230 range of 2.0 to 2.2 is considered pure for RNA samples156. Courtesy of Dr. Xuewen Song and Dr. Pei York.

60
Table 4. Reassignment of experimental groups for microarray study. The genotypes of the three experimental groups, WT vehicle, KO vehicle, and KO treatment (n = 7 per group), were reanalyzed. The first column shows the RNA ID of the individual samples. The second column shows the treatment assignment to the WT and KO animals; however, when the microarray analysis was performed, it became evident that the assignment of the genotypes of the animals was incorrect. The corrected genotype and treatment is shown in the third column. The RNA samples were then reassigned experimental grouping as WT vehicle (n = 5), WT treatment (n = 5), KO vehicle (n = 9), and KO treatment (n =2). In total, 21 individual samples of glomeruli were experimented on. Courtesy of Dr. Xuewen Song and Dr. Pei York.

61
Figure 19. Levels of differential gene expression in glomeruli in WT and KO mice after 10-day treatment with sham or MS417. Heat map of marked differential gene expression levels in the glomeruli isolated from 38-day-old WT and KO mice treated with either sham or MS417 for 10 days after which the mice were sacrificed. n = 9 for vehicle-treated KO; n = 2 for MS417-treated KO; n = 5 for vehicle-treated WT; n = 5 for MS417-treated WT. Columns represent kidney samples, rows present different genes, and each cell indicates the expression value of the gene in that sample. Upregulated genes are shown in red and downregulated genes are shown in blue. Courtesy of Dr. Xuewen Song and Dr. York Pei.

62
Figure 20. Marked differential gene expressions of IL-1β target genes in glomeruli of WT and KO mice. Heat map of marked differential gene expression levels of IL-1β targets in the glomeruli isolated from WT and KO mice treated with vehicle or MS417 for 10 days. n = 9 for vehicle-treated KO; n =2 for MS417-treated KO; n = 5 for vehicle-treated WT; n = 5 for MS417-treated WT. Columns represent kidney samples, rows present different genes, and each cell indicates the expression value of the gene in that sample. Upregulated genes are labelled in red and downregulated genes are labelled in blue. Courtesy of Dr. Xuewen Song and Dr. York Pei.
After10-daytreatmentwithMS417

63
Figure 21. Levels of marked differential gene expression of TLR4 and MYD88 targets in glomeruli in WT and KO mice. Heat map of TLR4 and MYD88 target gene expression levels in the glomeruli isolated from WT and KO mice after a 10-day treatment with vehicle or MS417. n = 9 for vehicle-treated KO group; n = 2 for MS417-treated KO; n = 5 for vehicle-treated WT; n = 5 for MS417-treated WT. Upregulated genes are shown in red and downregulated genes are shown in blue. Courtesy of Dr. Xuewen Song and Dr. York Pei.
After10-daytreatmentwithMS417

64
Figure 22. Marked differential gene expression levels of NF-κB target genes in glomeruli of WT and KO mice. Heat map of marked differentially expressed NF-κB target genes in the glomeruli isolated from WT and KO mice treated with vehicle or MS417 for 10 days before sacrificing. n = 9 for vehicle-treated KO; n = 2 for MS417-treated KO; n = 5 for vehicle-treated WT; n = 5 for MS417-treated WT. Columns represent kidney samples, rows present different genes, and each cell indicates the expression value of the gene in that sample. Upregulated genes are labelled in red and downregulated genes are labelled in blue. Courtesy of Dr. Xuewen Song and Dr. York Pei.

65
Chapter 4
Discussion
Alport Syndrome is a progressive nephropathy of the glomerular basement membrane, a
major component of the glomerular filtration barrier87. It is caused by mutations in the genes
encoding the α3/α4/α5 chains of type IV collagen, which is one of the principal constituents of
the GBM93,157. Thus, the dysregulation of the collagen IV alpha chains manifests in a clinical
course present with microscopic hematuria, which progresses to proteinuria, and eventually
culminating in renal failure5,87. Renal biopsies from patients also typically show segmental or
diffuse glomerulosclerosis, tubular atrophy, interstitial fibrosis, as well as interstitial infiltration
of lymphocytes and macrophages, correlating with progressive renal failure8,158. Yet, the exact
molecular mechanisms by which the mutations exert their pathogenic effects on the glomerulus
remain elusive. A greater understanding of the mechanisms behind the gradual degeneration of
the GBM in AS would lead to the discovery of renoprotective methods, which could potentially
prevent glomerulopathies in the future. Therefore, using in vitro and in vivo models, this study
examined the possibility of inflammation as a major driving force behind the glomerular injury
in AS. Furthermore, the impact of NF-κB inhibition via competitive blockade of BRD4 on the
renal disease progression in AS was investigated.
4.1 Major changes in gene expression are observed in the glomeruli prior to a decline in
GFR in experimental AS
The molecular effects of COL4A3/A4/A5 mutations were investigated in the glomeruli of
WT or mutant (Col4a3-/-) mice via microarray analysis. Microarray technology is a powerful tool
that allows the analysis and quantification of thousands of gene expression levels

66
simultaneously159,160. Thus, such high-throughput approach has been utilized in recent years to
discern a global viewpoint of the disease at the molecular level, enabling the evaluation of the
cellular and metabolic derangement associated with the diseased state161. The gene expression
profiles in this study give information with regards to both upregulated and downregulated genes
in the early phase of disease progression in this experimental model. Figure 8 shows the heat
map of differentially expressed genes with twofold greater expression in 4-week-old KO
compared to WT kidneys, showcasing a prominent pattern of pathway activation and inactivation
that is consonant with the COL4A3 mutation. The heat map revealed marked overexpression of
genes involved in inflammation mediated by chemokine and cytokine signalling pathways as
well as PDGF signalling pathway in 4-week-old KO glomeruli compared to the age- and sex-
matched control glomeruli. Genes involved in a variety of non-immune pathways, such as
angiogenesis, blood coagulation, gonadotropin-releasing hormone receptor, integrin signalling,
PI3 kinase, as well as Wnt signalling, were downregulated in the early timepoint of COL4A3
deletion.
Inflammation has been well-established as an important driver of pathophysiology across
a broad range of diseases in the literature, including in nephropathies162,163. The expression levels
of proinflammatory mediators, such as cytokines and chemokines, are upregulated in the
diseased state in comparison to healthy controls, conveying their crucial role in the pathogenesis
of CKD. For instance, TNFRSF12A (tumour necrosis factor receptor superfamily member 12A)
is a receptor for tumour necrosis factor ligand superfamily member 12 (TNFSF12; also called
TNF-related weak inducer of apoptosis (TWEAK)), a cytokine that is widely expressed with
overlapping signalling function with tumour necrosis factor (TNF)164,165. Excessive activation of

67
the TNF/TWEAK pathway has been observed in kidney injury to promote NF-κB-dependent
inflammatory response, fibrosis, angiogenesis, as well as apoptosis165,166.
Likewise, C-X-C motif chemokine 10 (CXCL10) is a cytokine belonging to the CXC
chemokine family that has been implicated in inflammatory diseases, which is seen to be
strongly expressed in 4-week-old KO mice167. It was seen in the study by Petrovic-Djergovic et
al. (2015) that stimulation of cultured podocytes with IFN-γ and TNF-α markedly induced the
expression of Cxcl10 mRNA and CXCL10 secretion, illustrating its role in the propagation of
innate and adaptive immunity, as well as inflammation168. Kaffe et al. (2018) also investigated
the pathogenetic role of CXCL10 in disease progression in vivo by blocking the CXCR3-
CXCL10 axis, inhibiting macrophage recruitment in congenital hepatic fibrosis in the presence
of polycystic kidney disease169. It was found that CXCL10 inhibition slowed the progression of
the disease by reducing CD45+ immune cell infiltration, collagen deposition, the total number of
macrophages, as well as proinflammatory T cells.
Adrenomedullin (ADM) is a vasodilatory peptide abundantly expressed in the kidney
with antiproliferative effects on glomerular mesangial cells170. Its production has been seen to be
activated in several pathophysiological states, including cardiac, hepatic, respiratory, renal
failure, tumour growth, as well as during inflammatory states171,172. A body of evidence indicates
that inflammatory cytokines, such as TNF-α and IL-1β, upregulates ADM mRNA expression,
suggesting that inflammatory cytokines may trigger ADM gene expression during
inflammation171. A rise in ADM level was observed to significantly ameliorate proteinuria,
glomerular and tubular injury, as well as renal dysfunction in salt-related renal hypertension173.
Thus the increase in delivery of ADM gene in the kidney suggests a renoprotective role,

68
producing a wide spectrum of beneficial effects in compensation for the impaired renal function
in the diseased state174.
Another gene that was overexpressed in the KO glomeruli is CYP1B1, which is a
member of the cytochrome P450 enzyme family I, subfamily B, polypeptide 1175,176. It is
expressed in cardiovascular and renal tissues, with a major role in the mediation of Ang II-
induced activation of NADPH oxidase, generation of reactive oxygen species (ROS),
proliferation, hypertrophy and/or deactivation of a wide range of xenobiotics176–178. CYP1B1
expression has been implicated in pathophysiology, particularly in tumours as well as
cardiovascular and renal abnormalities179. For instance, Zordoky and group reported that acute
doxorubicin (DOX) toxicity, a chemotherapy drug that causes oxidative damage and induces
inflammatory changes in the heart, kidney, and liver tissues, caused an induction of CYP1B1
expression in both the kidneys and liver in rats in a mechanism which has yet to be fully
elucidated177. Similarly, the deleterious pathophysiological effects of Ang II infusion in the
kidneys were observed to be minimized by the inhibition of CYP1B1 activity by treatment with a
selective CYP1B1 inhibitor, TMS, in rats, and by Cyp1b1 gene disruption in the mice175,180,181.
Transgelin (TAGLN), also designated SM22α, is a cytoskeletal protein whose expression
has been known to be induced in kidney injury182,183. A differentiation marker of smooth muscle
cells during embryogenesis, TAGLN is present transiently in the glomeruli during development
and later absent in normal adult glomeruli184. However, the reappearance of TAGLN within
injured glomeruli is a major finding that links its expression to the initiation and/or progression
of renal diseases characterized by podocyte injury and proteinuria, corresponding to the
overexpression seen in the KO glomeruli in the microarray analysis185. The literature has
documented marked TAGLN upregulation in experimental models of nephropathies, as well as in

69
renal tissue of patients with proteinuric diseases, such as diabetic nephropathy and IgA
nephropathy186. Furthermore, microarray and proteomic analyses in obstructive nephropathy
model suggest TAGLN is upregulated during fibrosis development, an important pathological
feature that eventually leads to renal failure187.
Genes downregulated in diseased animals compared to controls were mainly required for
cell structure and localization, cell cycle, metabolic processes, and developmental processes
(Figure 8). Among the 16 genes belonging to this group were, for example, secreted frizzled
related protein 1 (SFRP1), kallikrein 1 (KLK1), and klotho. SFRP1, a secreted antagonist of Wnt
signalling, is a known tumour suppressor that is involved in cell growth188. Though the role of
SFRP1 in CKD has not yet been elucidated, the loss of its expression and the contribution its
absence has on pathological events have been documented in a variety of cancers, including
renal cell carcinomas (RCC), in which the loss of SFRP1 is often observed in human
cancers189,190. This deregulation of SFRP1 expression level in RCC may allude to its role in
abberant Wnt signalling in the development of solid tumours190,191. In addition, study by
Matsuyama and group found that kidneys from Sfrp1-/- mice showed significant expression of
myofibroblast markers, aSMA, as well as fibroblast genes, vimentin, after unilateral ureteral
obstruction (UUO), giving rise to significant expansion of renal fibrosis192. The inactivation of
SFRP1 also brought about an elevation of phosphorylated c-Jun and JNK levels, which are
mediators of non-canonical Wnt signalling activation, corroborating SFRP1’s role as a modulator
of renal damage through the non-canonical Wnt/PCP pathway. Thus, SFRP1 may be a key player
in regulation and development of Wnt/PCP-mediated renal interstitial fibrosis in CKD192.
KLK1 deficiency has been documented in experimental models of hypertension, diabetic
nephropathy, and kidney injury193. KLK1 is a highly-conserved serine protease expressed in the

70
kidney, which cleaves low molecular weight kininogen into kinin, which is then involved in
kidney function and blood pressure regulation via vasodilatory and natriuretic effects194. In
experimental acute kidney injury (AKI), renal KLK1 activity is markedly diminished, and the
gene transfer of KLK1 can abrogate renal injury by minimizing apoptosis and inflammatory cell
recruitment193,195,196. Recent research has also identified the kidney-secreted hormone, klotho, as
a central player in CKD-related inflammation with anti-aging and nephroprotective properties197.
A decrease in klotho level has been observed not only in chronic or acute animal models of renal
injury characterized by renal inflammation, such as diabetic nephropathy, but also in patients
with G1 category of CKD, in which normal GFR is accompanied by pathological albuminuria or
other evidence of kidney injury198,199. Furthermore, interestingly, studies have found that
inflammatory cytokines, including TWEAK and TNF-α, downregulate renal klotho gene
transcription via NF-κB both in vitro and in vivo200. Likewise, exogenous provision of klotho to
the kidneys of db/db mice negatively regulated NF-κB activation and the suppression of
subsequent production of proinflammatory cytokines, such as RANTES, MCP-1, IL-6, and IL-8,
in response to TNF-α stimulation, showcasing a bidirectional relationship between klotho and
inflammation197,201,202.
Downregulation of inward rectifier potassium channel 16 (KCNJ16; Kir5.1) was also
observed in Figure 8, which mirrors the findings reported in the literature, in which disruption of
KCNJ16 induced severe hypokalemia203. Human mutations in KCNJ16 are associated with renal
pathologies characterized by salt-wasting, renal tubulopathy, and hypokalemia, known as EAST
syndrome, highlighting the critical role of the Kir5.1 potassium channel in the distal
nephron203,204. Similarly, KCNJ1 (Kir1.1) loss brings about type II Bartter syndrome, which
features polyuria, renal salt wasting, and hypotension; such clinical manifestations are largely

71
recapitulated in Kcnj1-null mice205. Schmidt et al. (2007) further uncovered that
proinflammatory cytokines, IL-1β and TNF-α, extensively suppressed the expression of KCNJ1,
postulating the cytokines may mediate LPS-induced downregulation of tubular sodium
transporters206.
To fully delineate the molecular mechanisms behind the progressive deterioration of the
GBM in the early stages of AS, the changes in the gene expression in the glomeruli were
analyzed by microarrays in experimental model of AS immediately following the onset of
albuminuria. Microarray analysis has been extensively applied in the field of experimental
nephrology due to its efficiency in the analysis of changes in the transcriptome207. The results in
this study showed that there was a distinct pattern of differentially expressed genes between the
Col4a3 KO and WT kidneys before the materialization of major structural and functional
changes at 4 weeks of age (Figure 8). Many of the upregulated differentially expressed genes in
the KO glomeruli were implicated in chemokine- and cytokine-induced inflammatory pathways,
whereas those that were downregulated in diseased animals were involved in cell structure, cell
cycling, as well as metabolic and developmental processes. The serial changes in glomerular
gene expression in early experimental AS were in accordance with previous findings in other
nephropathies. Thus, it was found that at the onset of proteinuria, the kidneys of experimental AS
were marked with changes in gene expression prior to the development of structural and
functional manifestations of the disease compared to WT controls.

72
4.2 Pathway analysis of the differential gene expression established that pathways
converged on NF-κB
In this study, the gene expression profile of Col4a3-/- glomeruli was further investigated
to better understand the biological mechanisms of AS. The microarray dataset, which established
that the onset of proteinuria is marked with a change in gene expression with the identification of
771 differentially expressed genes in mice with experimental AS compared to controls, was
further analyzed for potent activated upstream regulators. This was done with the application of
the Ingenuity Pathway Analysis (IPA), which calculates the activation z-score that represents the
bias in gene regulation, thus reducing the chance that random data will generate significant
predictions208–210. With the z-scores filtered at 2.0, the IPA is then able to identify the cascade of
upstream transcriptional regulators that are predicted to be activated based on the expression
pattern of the target genes211,212. Table 1 shows the 55 predicted putative upstream regulators,
with NF-κB revealed to be the most activated upstream regulator, along with a multitude of
regulators that are implicated in Toll-like receptor (TLR) signalling213–216. Figure 8 then
schematically summarizes the signalling pathways in experimental AS as predicted by IPA,
emphasizing the central role of NF-κB in the modulation of inflammatory pathways in AS; its
function as a major downstream convergent point for a multitude of proinflammatory
transducers, including TLR4, is clearly recapitulated.
Renal inflammation is a universal response to injury, in which the the innate immune
system is stimulated to bring about an array of inflammatory responses as the first line of
defense215. The innate immune system, composed of germlike-encoded receptors expressed by
macrophages, dendritic cells, monocytes, neutrophils, and natural killer cells, collectively serves
to monitor extracellular and intracellular compartments for signs of infection or tissue injury217.

73
These sensors, appropriately called pattern recognition receptors (PRRs), recognize common
molecular patterns and translate these diverse triggers of renal inflammation into induction of
cell activation and secretion of proinflammatory cytokines and chemokines. PRRs may respond
to various bacterial and viral pathogen-associated molecular patterns (PAMPs), as well as non-
microbial host-derived stimuli, such as damage-associated molecular patterns (DAMPs), which
are endogenous molecules released by injured tissues during inflammation218. The activation of
the PRRs mediates downstream pathways through transcription factors that modulate the
expression of genes with proinflammatory phenotype219.
Among the several distinct classes of PRRs is the membrane-bound TLR family, which
effectuate inflammatory responses by being able to detect a wide array of PAMPs and DAMPs in
the extracellular space163. TLRs are expressed on a variety of immune cells, including
macrophages, neutrophil granulocytes, mast cells, dendritic cells, and T and B lymphocytes, as
well as on other cell types, such as parenchymal and epithelial cells194,220. The binding of a
ligand to a TLR activates numerous signalling pathways, in which TLR activates adaptor
proteins, which in turn initiate NF-κB in the actuation of inflammatory responses. Two main
TLR signalling pathways are myeloid differentiation factor 88 (MYD88)-dependent pathway and
the TIR-domain-containing adaptor protein-inducing IFN-β (TRIF)-dependent pathway221. The
MYD88-dependent pathway is activated by all known TLRs except TLR3, and leads to the
production of proinflammatory cytokines, such as TNF, IL-1β, IL-12, IL-6, IL-8, and CC-motif
chemokine ligand 2 (CCL2), whereas TLR3 and TLR4 can trigger the TRIF-dependent pathway,
which brings about the production of type I interferons (IFNs), IFN-α and IFN-β, against viral
infection222,223. Generally, all TLRs can induce the expression of NF-κB-dependent genes,
including most proinflammatory cytokines and chemokines, in addition to being able to induce

74
the expression of procytokines, IL-1 and IL-18163. Recent studies have suggested that TLRs have
an important role in the pathogenesis of renal diseases, with their exaggerated activation
documented in renal ischemia, acute kidney injury, ESRF, acute tubulointerstitial nephritis, renal
transplant rejection, as well as delayed allograft function224–227. Thus, although inflammation
mediated by PRRs can help to resolve and repair an initial insult, it has been recognized that
overactivation of DAMP signalling may trigger inappropriate sterile inflammation, thereby
contributing to unnecessary organ damage and dysfunction225. The data listed on Table 1 agrees
with previous reports that TLR and NF-κB signalling are important in the regulation of
inflammatory and repair processes in the kidneys of AS, with predicted upstream regulators
implicated in the activation of TLR signalling indicated in bolded letters222.
TLR4 is the most extensively studied amongst the numerous TLRs that have been
described in the literature, with significant implications in renal diseases194. TLR4 has been
shown to have an active role in the development of tubulointerstitial injury, albuminuria, as well
as glomerular damages. For instance, in patients with diabetic nephropathy, TLR4 was found to
be highly expressed in the renal tubules, positively correlating with interstitial macrophage
infiltration214. Furthermore, in animal models of glomerulosclerosis and mesangioproliferative
glomerulonephritis, it was shown that TLR4 activation in podocytes could induce
proinflammatory cytokines and promote podocyte injury228. Similarly, TLR4-deficient mice
exhibited less albuminuria, mesangial expansion, infiltration of macrophages, and decreased
proinflammatory and extracellular matrix-associated gene expression in the glomeruli compared
to wildtype mice229. Subsequently downstream of that, mice that lacked the adaptor protein,
MYD88, which is required for TLR signal transduction, presented a marked reduction in
inflammation as well230,231. This finding then led to an examination of the role of IL-1 receptor 1

75
(IL-1R1), which is a MYD88-dependent transmembrane receptor232. In IL-1R1 mutant mice, a
significant reduction in neutrophil response was observed, emphasizing IL-1R1’s essential
function in neutrophil recruitment in response to inflammation and injury221.
One of the ligands of IL-1R1 that was seen to be upregulated in the microarray data of
the Col4a3-/- mice (Table 1, Figure 10) is IL-1β, a potent multifunctional proinflammatory
cytokine that has been implicated in the sterile inflammatory response233,234. Unlike most
inflammatory cytokines that are mainly transcriptionally regulated, IL-1β is produced in the
cytosol as a biologically inactive pro-IL-1β, which is activated intracellularly via proteolytic
cleavage by caspase-1233. In turn, the activation and conversion of caspase-1 from its zymogen
form, pro-caspase-1, is under the direction of Nod-like receptor (NLR) protein family members,
which collectively forms an inflammasome complex235. This stimulation of inflammasomes
cleaves caspase-1, which then hydrolyzes pro-IL-1β into its mature and functional form, exciting
a proinflammatory response through the cleavage and thus activation of IL-1β, IL-18, as well as
pyroptosis, a programmed lytic cell death. Hence, IL-1β is yet another key mediator that drives
acute neutrophilic inflammatory response, with the microarray datasets mirroring that of the
observations documented in other studies in the literature.
Accordingly, heat maps representing the expression patterns of IL-1β, TLR4/MYD88,
and NF-κB target genes were generated in order to ascertain the cellular manifestations of
inflammation in the experimental model of AS (Figures 10-12). NF-κB target genes that are
differentially expressed in the 4-week-old KO glomeruli compared to their age-matched WT
controls confirmed the upregulation of genes involved in apoptosis signalling pathway, B and T
cell activation, inflammatory pathways mediated by chemokine and cytokine signalling, p53
pathway, as well as Toll receptor signalling pathway to name a few (Figure 12). This pattern of

76
differentially expressed gene profiling of IL-1β target genes (Figure 10) and TLR4 and MYD88
target genes (Figure 11) in the glomeruli of 4-week-old KO mice are also reiterated in the heat
maps generated by the microarray studies, illustrating the enhancement of pathways that are
involved in the recruitment and development of sterile inflammation that initiates renal injury
and dysfunction223.
4.3 A novel approach to inhibiting NF-κB-mediated gene expression: BRD4 antagonism
These findings suggest that the TLR4 pathway is a prominent mediator of sterile
inflammation in the pathophysiology of CKD and the inhibition of its signalling pathway could
block the damage brought about by the acute inflammatory response. However, blocking TLR4,
as a central endotoxin receptor that is the innate immune system’s primary responder to
pathogens, could also have detrimental effects in infectious and immunological settings,
compromising the host’s immunogenicity236. Therefore, targeting the downstream mediator of
TLR4 signalling, NF-κB, which is a point of convergence for a myriad of other signalling
pathways relevant to inflammation, may limit the risks of disrupting the rapid innate immunity
against microbial infections.
Numerous factors have been discovered to contribute to the transcriptional activation of
NF-kB target genes and with it multitudinous methods in which NF-κB has been inhibited have
been described in the literature, including genetic and pharmacologic maneuvers132,237–239.
However, due to its protective role in innate immune response to infection, a complete inhibition
of NF-κB may bring about adverse effects; thus, a selective blockade of its activity would help
maximize the beneficial effects240. Recently, emerging evidence has suggested that
posttranslational modifications of NF-κB may play a critical role in the transcriptional regulation

77
of NF-κB-mediated inflammatory response240,241. In particular, the acetylation of NF-κB’s RelA
subunit has emerged as a significant component of NF-κB signalling linked to the regulation of
DNA binding, IκB binding, as well as transactivation potential241. The acetylation at lysine-310
is recognized by two bromodomains of BRD4, which in turn recruits and activates CDK9 to
phosphorylate RNA polymerase II for the transcription of NF-κB target genes140,142,242. Hence,
lysine-310 acetylation, through its capacity to create docking sites for the recruitment of NF-κB
transcriptional cofactors, is required for the full transcriptional activity of NF-κB242.
Correspondingly, in order to study the biological effects of NF-κB inhibition via
pharmacological BRD4 blockade, an in vitro NF-κB luciferase study was carried out. NF-κB
stimulation was effected using Ang II in HK-2 cells and MS417/BRD4 activity was interfered
with the administration of MS417. The NF-κB luciferase assay revealed that MS417 was able to
efficiently inhibit NF-κB after induction with Ang II, supporting BRD4’s capability as an
effective NF-κB inhibitor (Figure 13). Other studies have demonstrated the efficacy of MS417 in
the potent suppression of NF-κB activity. For instance, Zhang et al. showed that MS417
effectively attenuated the NF-κB transcriptional activation of proinflammatory genes in kidney
cells treated with TNF or infected with HIV140. Moreover, MS417 treatment was able to
ameliorate inflammation and kidney injury in HIV-1 transgenic mice. Similarly, MS417 was
shown to inhibit NF-κB acetylation and its transcriptional activation in a murine model of
diabetic nephropathy142. Consistent with these findings, this study also clearly delineates and
exemplifies the role of acetylation of NF-κB and the effect of its inhibition via BRD4 blockade.

78
4.4 Treatment of BRD4 inhibitor led to a decrease in cytokine gene expression and a trend
towards improved creatinine levels and albuminuria
BET bromodomain-specific inhibitor, MS417, and its role in the modulation of NF-κB
transcriptional activity has been studied in other experimental models of nephropathies, such as
HIVAN and diabetic nephropathy; however, bromodomain inhibition has not been previously
examined in AS140,142. Thus, in this study, the effect of BRD4 antagonism on NF-κB-moderated
inflammatory gene expression was further investigated in vivo using Col4a3 KO and WT mice.
This pilot study was able to confirm that the drug, MS417, was first and foremost, well-tolerated
in the KO mice compared to the respective control groups via body weight measurements—
alterations in body weight is considered an indicator of in vivo toxicity (Figure 14)243,244.
Moreover, MS417 promoted a modest but therapeutic trend towards recovery in BUN, serum
creatinine, as well as UAE levels in the KO mice compared to the vehicle-treated WT mice
(Figures 15-17). Taken together, these results suggest that MS417 does not cause drug toxicity,
and is able to comparatively reduce proteinuria and improve renal function through its capacity
to inhibit NF-κB acetylation and transcriptional activation in the kidneys of the AS mice.
MS417 was discovered to also attenuate the expression of NF-κB target genes. The
analysis of the mRNA levels of proinflammatory cytokines, IL-6 and IL-1β suggested that BET
bromodomain inhibition downregulates NF-κB-mediated transcription of proinflammatory
cytokine and chemokine genes in Col4a3-/- mice (Figure 18). This finding corroborates previous
literature positing that selective inhibition of acetylated NF-kB binding to the transcriptional
cofactor, BRD4, does effectively attenuate NF-κB transcriptional activation of proinflammatory
genes, which are markers of kidney injury severity245,246. Elevated levels of IL-6 and IL-1β in
CKD have been observed in other studies in vivo and in vitro, in which their increased expression

79
levels were positively correlated with the severity of the renal disease progression119,247–249. One
study in 2014 found that upon analyzing the glomerular mRNA from an Alport mouse model,
there was a significant induction of proinflammatory cytokine, IL-6, that correlated with GBM
destruction119. Koga and group have examined the expression of proinflammatory cytokines, IL-
6, IL-1β, TNF-α, and TGF-β in a murine experimental model of AS, in which they were
discovered to be markedly induced in Alport kidneys compared with WT250. The elevation in
cytokine levels seen in the kidney tissues of Col4a3 KO mice were found to be significantly
preventable for IL-1β, while moderately ameliorated for IL-6 with the usage of NF-kB inhibitor,
MS417 (Figure 18).
To further investigate the mechanism of BRD4 inhibition in the pathophysiology of
experimental AS, a microarray study was performed to discern the effects of MS417 treatment on
the KO glomeruli compared to WT kidneys (Figures 19-22). However, perchance due to the
fallacious dosage administered to the mice, conflicting results were yielded in which there was
not a significant alteration in the gene expression levels in the treated mice compared to the KO.
4.5 Conclusions
Using a combination of in vitro and in vivo approaches, this thesis examined the potential
for NF-κB inhibition via pharmacological approach to BRD4 antagonism in experimental
models of AS, and the impact of that molecular obstruction on the pathologic manifestations. A
microarray study of the differentially expressed gene levels in the isolated glomeruli from
Col4a3 KO and WT mice revealed a defining genetic profile as early as 4 weeks of age in the
diseased state in comparison to healthy controls. A bioinformatic analysis via IPA of the
microarray dataset predicted activated upstream regulators, uncovering NF-κB as the most

80
activated transcription factor as well as its role as a key convergence centre for multiple affected
pathways, indicating sterile inflammation as a potential driver of the renal pathogenesis in AS—
an exaggerated reaction of the innate immune system gone awry. A novel BRD4 inhibitor,
MS417, was demonstrated to be an effective inhibitor of NF-κB activation both in vitro and in
vivo without effecting any biotoxicity in the HK-2 cells and Col4a3 mice. MS417 was
demonstrated to trend towards an attenuation of BUN, plasma creatinine, and UAE levels
compared to WT mice. Furthermore, MS417 administration attenuated the augmented
proinflammatory cytokine expression levels of IL-6 and IL-1β, with statistical significance for
the latter. Further microarray studies were accomplished with isolated glomeruli from 4-week-
old KO and WT mice with vehicle or MS417 treatment, which did not cause a similar attenuation
of inflammation previously observed, possibly due to the dosage error. However, overall, these
findings demonstrate the role of NF-κB-mediated sterile inflammation on the disease progression
in experimental AS, guiding the development of therapeutic strategies specifically targeting the
signalling pathway responsible for the deleterious effects of NF-κB.
4.6 Pitfalls and future directions
Several other hypotheses may be derived from the IPA analysis (Figure 9), for instance, it
is possible that early interaction between the podocytes and the abnormal basement membrane
leads to the activation of MMPs, subsequently bringing about a degradation of the ECM and the
generation of DAMPs that activate the innate immunity mediate in part by TLR4. However, this
aspect of the IPA analysis was not examined in this study and future experiments will be
necessary to address this hypothesis.

81
The study was based on Zhang et al. (2012) and Liu et al. (2014), both papers which used
an in vivo dosage of 0.08 mg/kg when treating db/db and HIV-1 transgenic mice with the BRD4-
antagonizing compound, MS417140,142. However, post-treatment renal analyses revealed that the
mice were dosed at a differing dosage of 0.0016 mg/kg due to a calculation error made. In
addition, the genotypes of the mice samples were rechecked during the microarray study using
the Col4a3 expression and it was discovered that there was an issue with the initial assignment of
the mice genotypes. At the time of the glomeruli sample submission for the microarray study, it
was presumed that n = 7 for each vehicle-treated WT, vehicle-treated KO, and MS417-treated
KO experimental groups were originally submitted (Table 2). However, the repeated genotyping
analysis reassigned vehicle-treated WT as n = 5, vehicle-treated KO n = 9, and MS417- treated
KO n = 2 (Table 4). For future studies, the correct dosage of MS417 as well as accurate
genotyping, resulting in a higher n value for each experimental group, would help in yielding
more effectual and precise outcomes. Despite the experimental errors, these analyses and the
yielded negative results still provided data that plays a part in the effort to uncover novel
therapies for AS.

82
References
1. Savige, J., Gregory, M., Gross, O., Kashtan, C., Ding, J. & Flinter, F. Expert Guidelines for the Management of Alport Syndrome and Thin Basement Membrane Nephropathy. J. Am. Soc. Nephrol. 24, 364–375 (2013).
2. Levy, M. & Feingold, J. Estimating prevalence in single-gene kidney diseases progressing to renal failure. Kidney Int. 58, 925–943 (2000).
3. Alport, A. C. Hereditary familial congenital haemorrhagic nephritis. Br. Med. J. 1, 504–6 (1927).
4. Savige, J. Alport syndrome: its effects on the glomerular filtration barrier and implications for future treatment. J. Physiol. 592, 4013–4023 (2014).
5. Miner, J. H., Baigent, C., Flinter, F., Gross, O., Judge, P., Kashtan, C. E., Lagas, S., Savige, J., Blatt, D., Ding, J., Gale, D. P., Midgley, J. P., Povey, S., Prunotto, M., Renault, D., Skelding, J., Turner, A. N. & Gear, S. The 2014 International Workshop on Alport Syndrome. Kidney Int. 86, 679–84 (2014).
6. Kashtan, C. E. Alport Syndrome and Thin Basement Membrane Nephropathy. NCBI Bookshelf 1–24 (2015).
7. Cosgrove, D. & Liu, S. Collagen IV diseases: A focus on the glomerular basement membrane in Alport syndrome. Matrix Biol. 57–58, 45–54 (2017).
8. Storey, H., Savige, J., Sivakumar, V., Abbs, S. & Flinter, F. A. COL4A3/COL4A4 Mutations and Features in Individuals with Autosomal Recessive Alport Syndrome. J. Am. Soc. Nephrol. 24, 1945–1954 (2013).
9. Sugimoto, M., Oohashi, T. & Ninomiya, Y. The Genes Col4a5 and Col4a6, Coding for Basement-Membrane Collagen Chains Alpha-5(Iv) and Alpha-6(Iv), Are Located Head-To-Head in Close Proximity on Human-Chromosome Xq22 and Col4a6 Is Transcribed From 2 Alternative Promoters. Proc. Natl. Acad. Sci. U. S. A. 91, 11679–11683 (1994).
10. Uzak, A. S., Tokgoz, B., Dundar, M. & Tekin, M. A novel COL4A3 mutation causes autosomal-recessive Alport syndrome in a large Turkish family. Genet. Test. Mol. Biomarkers 17, 260–4 (2013).
11. Hicks, J., Mierau, G., Wartchow, E. & Eldin, K. Renal Diseases Associated with Hematuria in Children and Adolescents: A Brief Tutorial. Ultrastruct. Pathol. 36, 1–18 (2012).
12. Jais, J. P., Knebelmann, B., Giatras, I., De Marchi, M., Rizzoni, G., Renieri, A., Weber, M., Gross, O., Netzer, K., Flinter, F., Pirson, Y., Verellen, C., Wieslander, J., Persson, U., Tryggvason, K., Martin, P., Hertz, J. M., Schroder, C., Sanak, M., Krejcova, S., Carvalho, M. F., Saus, J., Antignac, C., Smeets, H. & Gubler, M. C. X-linked Alport syndrome: natural history in 195 families and genotype- phenotype correlations in males. J. Am. Soc. Nephrol. 11, 649–657 (2000).
13. Kashtan, C. & Michael, A. Alport syndrome. Kidney Int. 50, 1445–1463 (1996). 14. Alves, F. R. a. & Ribeiro, F. D. a. Q. Revision about hearing loss in the Alport’s syndrome,
analyzing the clinical, genetic and bio-molecular aspects. Rev. Bras. Otorrinolaringol. 71, 813–819 (2005).
15. Jais, J. P. X-Linked Alport Syndrome: Natural History and Genotype-Phenotype Correlations in Girls and Women Belonging to 195 Families: A ‘European Community Alport Syndrome Concerted Action’ Study. J. Am. Soc. Nephrol. 14, 2603–2610 (2003).
16. Rheault, M. N., Kren, S. M., Hartich, L. A., Wall, M., Thomas, W., Mesa, H. A., Avner, P.,

83
Lees, G. E., Kashtan, C. E. & Segal, Y. X-inactivation modifies disease severity in female carriers of murine X-linked Alport syndrome. Nephrol. Dial. Transplant. 25, 764–769 (2010).
17. Pirson, Y. Making the diagnosis of Alport’s syndrome. Kidney Int. 56, 760–775 (1999). 18. Longo, I., Scala, E., Mari, F., Caselli, R., Pescucci, C., Mencarelli, M. A., Speciale, C.,
Giani, M., Bresin, E., Caringella, D. A., Borochowitz, Z., Siriwardena, K., Winship, I., Renieri, A. & Meloni, I. Autosomal recessive Alport syndrome: An in-depth clinical and molecular analysis of five families. Nephrol. Dial. Transplant. 21, 665–671 (2006).
19. Kashtan, C. E. Familial hematuria due to type IV collagen mutations: Alport syndrome and thin basement membrane nephropathy. Curr. Opin. Pediatr. 16, 177–181 (2004).
20. Heidet, L. & Gubler, M.-C. The renal lesions of Alport syndrome. J. Am. Soc. Nephrol. 20, 1210–1215 (2009).
21. Izzedine, H., Tankere, F., Launay-Vacher, V. & Deray, G. Ear and kidney syndromes: Molecular versus clinical approach. Kidney Int. 65, 369–385 (2004).
22. Merchant, S. N., Burguess, B. J., Adams, J. C., Kashtan, C. E., Gregory, M. C., Santi, P. A., Colvin, R., Collins, B. & Nadol, J. B. Temporal Bone Histopathology in Alport Syndrome. Laryngoscope 114, 1609–1618 (2004).
23. Aslanzadeh, G. A., Gharabaghi, D. & Naderi, N. Clear lens phacoemulsification in the anterior lenticonus due to Alport Syndrome: two case reports. J. Med. Case Rep. 2, 178 (2008).
24. Savige, J., Sheth, S., Leys, A., Nicholson, A., Mack, H. G. & Colville, D. Ocular features in Alport syndrome: Pathogenesis and clinical significance. Clin. J. Am. Soc. Nephrol. 10, 703–709 (2015).
25. Zhang, Y. & Ding, J. Renal, auricular, and ocular outcomes of Alport syndrome and their current management. Pediatr. Nephrol. (2017). doi:10.1007/s00467-017-3784-3
26. Colville, D. J. & Savige, J. Alport syndrome. A review of the ocular manifestations. Ophthalmic Genet. 18, 161–73 (1997).
27. Savige, J. & Colville, D. Opinion: Ocular features aid the diagnosis of Alport syndrome. Nat. Rev. Nephrol. 5, 356–60 (2009).
28. Grubb, R. L., Franks, M. E., Toro, J., Middelton, L., Choyke, L., Fowler, S., Torres-Cabala, C., Glenn, G. M., Choyke, P., Merino, M. J., Zbar, B., Pinto, P. A., Srinivasan, R., Coleman, J. A., Linehan, W. M. Hereditary Leiomyomatosis and Renal Cell Cancer: A Syndrome Associated With an Aggressive Form of Inherited Renal Cancer. J. Urol. 177, 2074–2080 (2007).
29. Misra, M., Maziak, D. E., Shamji, F. M., Michaud, C., Perkins, D. G. & Matzinger, F. Esophageal leiomyomatosis. Med. Sci. Monit. 9, CS98-101 (2003).
30. Dagbert, F., Pelascini, E., Pasquer, A., Gincul, R., Mion, F., Poncet, G. & Robert, M. Extensive preoperative workup in diffuse esophageal leiomyomatosis associated with Alport syndrome influences surgical treatment: A case report. Int. J. Surg. Case Rep. 10, 183–186 (2015).
31. Dahan, K., Heidet, L., Zhou, J., Mettler, G., Leppig, K. A., Proesmans, W., David, A., Roussel, B., Mongeau, J. G., Gould, J. M. D., Grunfeld, J., Gubler, M. & Antignac, C. Smooth muscle tumors associated with X-linked Alport syndrome: Carrier detection in females. Kidney Int. 48, 1900–1906 (1995).
32. Vaicys, C., Hunt, C. D. & Heary, R. F. Ruptured intracranial aneurysm in an adolescent with Alport’s syndrome—a new expression of type IV collagenopathy: Case report. Surg.

84
Neurol. 54, 68–72 (2000). 33. Lyons, O. T. A., St. John, E. R. C., Morales, J. P., Chan, Y. C. & Taylor, P. R. Ruptured
Thoracoabdominal Aortic Aneurysm in a Renal Transplant Patient with Alport’s Syndrome. Ann. Vasc. Surg. 21, 816–818 (2007).
34. Kashtan, C. E., Segal, Y., Flinter, F., Makanjuola, D., Gan, J. & Watnick, T. Aortic abnormalities in males with Alport syndrome. Nephrol. Dial. Transplant. 25, 3554–3560 (2010).
35. Bassareo, P. P., Marras, A. R. & Mercuro, G. Ventricular septal defect in a child with Alport syndrome: a case report. BMC Cardiovasc. Disord. 10, 48 (2010).
36. Haas, M. Alport syndrome and thin glomerular basement membrane nephropathy: a practical approach to diagnosis. Arch. Pathol. Lab. Med. 133, 224–232 (2009).
37. Gubler, M.-C. Inherited diseases of the glomerular basement membrane. Nature 4, 24–37 (2008).
38. Deegens, J. K. J., Dijkman, H. B. P. M., Borm, G. F., Steenbergen, E. J., van den Berg, J. G., Weening, J. J. & Wetzels, J. F. M. Podocyte foot process effacement as a diagnostic tool in focal segmental glomerulosclerosis. Kidney Int. 74, 1568–1576 (2008).
39. Kriz, W., Shirato, I., Nagata, M., LeHir, M. & Lemley, K. V. The podocyte’s response to stress: the enigma of foot process effacement. AJP Ren. Physiol. 304, F333–F347 (2013).
40. Wickman, L., Hodgin, J. B., Wang, S. Q., Afshinnia, F., Kershaw, D. & Wiggins, R. C. Podocyte depletion in Thin GBM and Alport Syndrome. PLoS One 11, 1–15 (2016).
41. Ding, F., Wickman, L., Wang, S. Q., Zhang, Y., Wang, F., Afshinnia, F., Hodgin, J., Ding, J. & Wiggins, R. C. Accelerated podocyte detachment and progressive podocyte loss from glomeruli with age in Alport Syndrome. Kidney Int. 1–11 (2017). doi:10.1016/j.kint.2017.05.017
42. Kim, M., Piaia, A., Shenoy, N., Kagan, D., Gapp, B., Kueng, B., Weber, D., Dietrich, W. & Ksiazek, I. Progression of Alport Kidney Disease in Col4a3 knock out mice is independent of sex or macrophage depletion by clodronate treatment. PLoS One 10, 1–17 (2015).
43. Fogo, A. B., Lusco, M. A., Najafian, B. & Alpers, C. E. AJKD Atlas of Renal Pathology: Alport Syndrome. Am. J. Kidney Dis. 68, e15–e16 (2016).
44. Bekheirnia, M. R., Reed, B., Gregory, M. C., McFann, K., Shamshirsaz, A. A., Masoumi, A. & Schrier, R. W. Genotype-phenotype correlation in X-linked Alport syndrome. J. Am. Soc. Nephrol. 21, 876–883 (2010).
45. Agrawal, S., Agarwal, S. & Naik, S. Genetic contribution and associated pathophysiology in end-stage renal disease. Appl. Clin. Genet. 3, 65–84 (2010).
46. Freedman, B. I., Parekh, R. S. & Kao, W. H. L. Genetic basis of nondiabetic end-stage renal disease. Semin. Nephrol. 30, 101–110 (2010).
47. Satko, S. G., Freedman, B. I. & Moossavi, S. Genetic factors in end-stage renal disease. Kidney Int Suppl 67, S46–S49 (2005).
48. Gross, O., Netzer, K.-O., Lambrecht, R., Seibold, S. & Weber, M. Meta-analysis of genotype-phenotype correlation in X-linked Alport syndrome: impact on clinical counselling. Nephrol. Dial. Transplant 17, 1218–27 (2002).
49. Yamamura, T., Nozu, K., Fu, X. J., Nozu, Y., Ye, M. J., Shono, A., Yamanouchi, S., Minamikawa, S., Morisada, N., Nakanishi, K., Shima, Y., Yoshikawa, N., Ninchoji, T., Morioka, I., Kaito, H. & Iijima, K. Natural History and Genotype–Phenotype Correlation in Female X-Linked Alport Syndrome. Kidney Int. Reports 2, 850–855 (2017).

85
50. Kashtan, C. Animal models of Alport syndrome. Nephrol. Dial. Transplant. 1359–1361 (2002). doi:10.1093/NDT/17.8.1359
51. Heikkila, P., Tryggvason, K. & Thorner, P. Animal Models of Alport Syndrome: Advancing the Prospects for Effective Human Gene Therapy. Exp. Nephrol. 8, 1–7 (2000).
52. Rheault, M. N., Kren, S. M., Thielen, B. K., Mesa, H. A., Crosson, J. T., Thomas, W., Sado, Y., Kashtan, C. E. & Segal, Y. Mouse model of X-linked Alport syndrome. J. Am. Soc. Nephrol. 15, 1466–1474 (2004).
53. Jansen, B., Singh, A., Lumsden, J. H., Valli, V. E., Baumal, R. & Basrur, P. K. Animal model of human disease: hereditary nephritis in Samoyed dogs. Am. J. Pathol. 116, 175–8 (1984).
54. Zheng, K., Thorner, P. S., Marrano, P., Baumal, R. & McInnes, R. R. Canine X chromosome-linked hereditary nephritis: a genetic model for human X-linked hereditary nephritis resulting from a single base mutation in the gene encoding the alpha 5 chain of collagen type IV. Proc. Natl. Acad. Sci. U. S. A. 91, 3989–3993 (1994).
55. Bell, R. J., Lees, G. E. & Murphy, K. E. X chromosome inactivation patterns in normal and X-linked hereditary nephropathy carrier dogs. Cytogenet. Genome Res. 122, 37–40 (2008).
56. Benali, S. L., Lees, G. E., Nabity, M. B., Arico, A., Drigo, M., Gallo, E., Giantin, M. & Aresu, L. X-Linked Hereditary Nephropathy in Navasota Dogs: Clinical Pathology, Morphology, and Gene Expression During Disease Progression. Vet. Pathol. 53, 803–812 (2016).
57. Hood, J. C., Savige, J., Hendtlass, A., Kleppel, M. M., Huxtable, C. R. & Robinson, W. F. Bull terrier hereditary nephritis: A model for autosomal dominant Alport syndrome. Kidney Int. 47, 758–765 (1995).
58. Cosgrove, D., Meehan, D. T., Grunkemeyer, J. A., Kornak, J. M., Sayers, R., Hunter, W. J. & Samuelson, G. C. Collagen COL4A3 knockout: A mouse model for autosomal Alport syndrome. Genes Dev. 10, 2981–2992 (1996).
59. Miner, J. H. & Sanes, J. R. Molecular and functional defects in kidneys of mice lacking collagen a3(IV): Implications for Alport syndrome. J. Cell Biol. 135, 1403–1413 (1996).
60. Kashtan, C. E. Alport syndrome: Abnormalities of type IV collagen genes and proteins. Ren. Fail. 22, 737–749 (2000).
61. Hudson, B. G., Tryggvason, K., Sundaramoorthy, M. & Neilson, E. G. Alport’s syndrome, Goodpasture’s syndrome, and type IV collagen. N. Engl. J. Med. 348, 2543–56 (2003).
62. Suh, J. H. & Miner, J. H. The glomerular basement membrane as a barrier to albumin. Nat. Rev. Nephrol. 9, 470–477 (2013).
63. Borza, D. B. Glomerular basement membrane heparan sulfate in health and disease: A regulator of local complement activation. Matrix Biol. 57–58, 299–310 (2017).
64. Miner, J. Glomerular basement membrane composition and the filtration barrier. Pediatr. Nephrol. 26, 1413–1417 (2011).
65. Miner, J. H. The Glomerular Basement Membrane. Exp Cell Res 318, 973–978 (2012). 66. Yurchenco, P. D. & Patton, B. L. Developmental and Pathogenic Mechanisms of
Basement Membrane Assembly. Curr Pharm Des 42, 1277–1294 (2009). 67. Hohenester, E. & Yurchenco, P. D. Laminins in basement membrane assembly. Cell Adh.
Migr. 7, 56–63 (2013). 68. Chen, Y. M. & Miner, J. H. Glomerular basement membrane and related glomerular
disease. Transl. Res. 160, 291–297 (2012).

86
69. Miner, J. H. Building the glomerulus: a matricentric view. J. Am. Soc. Nephrol. 16, 857–861 (2005).
70. Miner, J. H. & Li, C. Defective Glomerulogenesis in the Absence of Laminin a5 Demonstrates a Developmental Role for the Kidney Glomerular Basement Membrane. Dev. Biol. 289, 278–289 (2000).
71. Abrahamson, D. R., Prettyman, A. C., Robert, B. & St. John, P. L. Laminin-1 reexpression in Alport mouse glomerular basement membranes. Kidney Int. 63, 826–834 (2003).
72. Miner, J. H., Cunningham, J. & Sanes, J. R. Roles for laminin in embryogenesis: Exencephaly, syndactyly, and placentopathy in mice lacking the laminin a5 chain. J. Cell Biol. 143, 1713–1723 (1998).
73. Noone, D. & Licht, C. An update on the pathomechanisms and future therapies of Alport syndrome. Pediatr. Nephrol. 28, 1025–1036 (2013).
74. Abrahamson, D. R., Hudson, B. G., Stroganova, L., Borza, D.-B. & St. John, P. L. Cellular Origins of Type IV Collagen Networks in Developing Glomeruli. J. Am. Soc. Nephrol. 20, 1471–1479 (2009).
75. Deltas, C., Pierides, A. & Voskarides, K. Molecular genetics of familial hematuric diseases. Nephrol. Dial. Transplant 28, 2946–60 (2013).
76. Abrahamson, D. R. Role of the Podocyte (and Glomerular Endothelium) in Building the GBM. Semin. Nephrol. 32, 342–349 (2012).
77. Gross, O., Perin, L. & Deltas, C. Alport syndrome from bench to bedside: the potential of current treatment beyond RAAS blockade and the horizon of future therapies. Nephrol. Dial. Transplant 29, iv124-iv130 (2014).
78. Miner, J. H. Organogenesis of the kidney glomerulus: focus on the glomerular basement membrane. Organogenesis 7, 75–82 (2011).
79. Bader, B. L., Smyth, N., Nedbal, S., Miosge, N., Baranowsky, A., Mokkapati, S., Murshed, M. & Nischt, R. Compound Genetic Ablation of Nidogen 1 and 2 Causes Basement Membrane Defects and Perinatal Lethality in Mice Compound Genetic Ablation of Nidogen 1 and 2 Causes Basement Membrane Defects and Perinatal Lethality in Mice. Mol Cell Biol 25, 6846–6856 (2005).
80. Groffen, A. J., Veerkamp, J. H., Monnens, L. A. & van den Heuvel, L. P. Recent insights into the structure and functions of heparan sulfate proteoglycans in the human glomerular basement membrane. Nephrol. Dial. Transplant 14, 2119–29 (1999).
81. Goldberg, S., Harvey, S. J., Cunningham, J., Tryggvason, K. & Miner, J. H. Glomerular filtration is normal in the absence of both agrin and perlecan-heparan sulfate from the glomerular basement membrane. Nephrol. Dial. Transplant. 24, 2044–2051 (2009).
82. Harvey, S. J. & Miner, J. H. Revisiting the glomerular charge barrier in the molecular era. Curr. Opin. Nephrol. Hypertens. 17, 393–8 (2008).
83. Gunwar, S., Ballester, F., Noelken, M. E., Sado, Y., Ninomiya, Y. & Hudson, B. G. Glomerular Basement Membrane. J. Biol. Chem. 273, 8767–8775 (1998).
84. Wyss, H. M. H., Henderson, J. M., Byfield, F. J., Bruggeman, L. A., Ding, Y., Huang, C., Suh, J. H., Franke, T., Mele, E., Pollak, M. R., Miner, J. H., Janmey, P. A., Weitz, D. A. & Miller, R. T. Biophysical properties of normal and diseased renal glomeruli. Am. J. cell Physiol. 300, 397–405 (2011).
85. Kalluri, R., Shield, C. F., Todd, P., Hudson, B. G. & Neilson, E. G. Isoform switching of type IV collagen is developmentally arrested in X- linked Aport syndrome leading to increased susceptibility of renal basement membranes to endoproteolysis. J. Clin. Invest.

87
99, 2470–2478 (1997). 86. Abrahamson, D. R., St John, P. L., Isom, K., Robert, B. & Miner, J. H. Partial rescue of
glomerular laminin alpha5 mutations by wild-type endothelia produce hybrid glomeruli. J Am Soc Nephrol 18, 2285–2293 (2007).
87. Kruegel, J., Rubel, D. & Gross, O. Alport syndrome--insights from basic and clinical research. Nat. Rev. Nephrol. 9, 170–8 (2013).
88. Liu, Y. New Insights into Epithelial-Mesenchymal Transition in Kidney Fibrosis. J. Am. Soc. Nephrol. 21, 212–222 (2010).
89. Gratton, M. A., Rao, V. H., Meehan, D. T., Askew, C. & Cosgrove, D. Matrix Metalloproteinase Dysregulation in the Stria Vascularis of Mice with Alport Syndrome. Am. J. Pathol. 166, 1465–1474 (2005).
90. Cosgrove, D., Meehan, D. T., Delimont, D., Pozzi, A., Chen, X., Rodgers, K. D., Tempero, R. M., Zallocchi, M. & Rao, V. H. Integrin α1β1 Regulates Matrix Metalloproteinases via P38 Mitogen-Activated Protein Kinase in Mesangial Cells. Am. J. Pathol. 172, 761–773 (2008).
91. Zeisberg, M., Khurana, M., Rao, V. H., Cosgrove, D., Rougier, J., Werner, M., Shield, C. F., Werb, Z. & Kalluri, R. Stage-specific action of matrix metalloproteinases influences progressive hereditary kidney disease. PLoS Med. 3, 535–546 (2006).
92. Rao, V. H.,, Meehan, D. T., Delimont, D., Nakajima, M., Wada, T., Gratton, M. A. & Cosgrove, D. Role for Macrophage Metalloelastase in Glomerular Basement Membrane Damage Associated with Alport Syndrome. Am. J. Pathol. 169, 32–46 (2006).
93. Meehan, D. T., Delimont, D., Cheung, L., Zallocchi, M., Sansom, S. C., Holzclaw, J. D., Rao, V. & Cosgrove, D. Biomechanical strain causes maladaptive gene regulation, contributing to alport glomerular disease. Kidney Int. 76, 968–976 (2009).
94. Gross, O. & Kashtan, C. E. Treatment of Alport syndrome: beyond animal models. Kidney Int. 76, 599–603 (2009).
95. Katayama, K., Kawano, M., Naito, I., Ishikawa, H., Sado, Y., Asakawa, N., Murata, T., Oosugi, K., Kiyohara, M., Ishikawa, E., Ito, M. & Nomura, S. Irradiation Prolongs Survival of Alport Mice. J Am Soc Nephrol 19, 1692–1700 (2008).
96. Ninichuk, V., Gross, O., Segerer, S., Hoffmann, R., Radomska, E., Buchstaller, A., Huss, R., Akis, N., Schlondorff, D. & Anders, H. Multipotent mesenchymal stem cells reduce interstitial fibrosis but do not delay progression of chronic kidney disease in collagen4A3-deficient mice. Kidney Int. 70, 121–129 (2006).
97. Gross, O., Beirowski, B., Koepke, M., Kuck, J., Reiner, M., Addicks, K., Smyth, N., Schulze-Lohoff, E. & Weber, M. Preemptive ramipril therapy delays renal failure and reduces renal fibrosis in COL4A3-knockout mice with Alport syndrome. Kidney Int. 63, 438–446 (2003).
98. Gross, O., Koepke, M., Beirowski, B., Schulze-Lohoff, E., Segerer, S. & Weber, M. Nephroprotection by antifibrotic and anti-inflammatory effects of the vasopeptidase inhibitor AVE7688. Kidney Int. 68, 456–463 (2005).
99. Chen, D., Jefferson, B., Harvey, S. J., Zheng, K., Gartley, C. J., Jacobs, R. M. & Thorner, P. S. Cyclosporine A slows the progressive renal disease of Alport syndrome (X-linked hereditary nephritis): Results from a canine model. J. Am. Soc. Nephrol. 14, 690–698 (2003).
100. Ninichuk, V., Gross, O., Reichel, C., Khandoga, A., Pawar, R. D., Ciubar, R., Segerer, S., Belemezova, E., Radomska, E., Luckow, B., de Lema, G. P., Murphy, P. M., Gao, J.,

88
Henger, A., Kretzler, M., Horuk, R., Weber, M., Krombach, F., Schlondorff, B. & Anders, H. Delayed Chemokine Receptor 1 Blockade Prolongs Survival in Collagen 4A3-Deficient Mice with Alport Disease. J. Am. Soc. Nephrol. 16, 977–985 (2005).
101. Koepke, M. L., Weber, M., Schulze-Lohoff, E., Beirowski, B., Segerer, S. & Gross, O. Nephroprotective effect of the HMG-CoA-reductase inhibitor cerivastatin in a mouse model of progressive renal fibrosis in Alport syndrome. Nephrol. Dial. Transplant. 22, 1062–1069 (2007).
102. Zeisberg, M., Bottiglio, C., Kumar, N., Maeshima, Y., Strutz, F., Muller, G. A. & Kalluri, R. Bone morphogenic protein-7 inhibits progression of chronic renal fibrosis associated with two genetic mouse models. Am. J. Physiol. - Ren. Physiol. 285, F1060–F1067 (2003).
103. Prodromidi, E. I., Poulsom, R., Jeffery, R., Roufosse, C. A., Pollard, P. J., Pusey, C. D. & Cook, H. T. Bone Marrow-Derived Cells Contribute to Podocyte Regeneration and Amelioration of Renal Disease in a Mouse Model of Alport Syndrome. Stem Cells 24, 2448–2455 (2006).
104. Sugimoto, H., Mundel, T. M., Sund, M., Xie, L., Cosgrove, D. & Kalluri, R. Bone-marrow-derived stem cells repair basement membrane collagen defects and reverse genetic kidney disease. Proc. Natl. Acad. Sci. 103, 7321–7326 (2006).
105. Kashtan, C. E., Ding, J., Gregory, M., Gross, O., Heidet, L., Knebelmann, B., Rheault, M. & Licht, C. Clinical practice recommendations for the treatment of Alport syndrome: A statement of the Alport Syndrome Research Collaborative. Pediatr. Nephrol. 28, 5–11 (2013).
106. Gross, O., Licht, C., Anders, H. J., Hoppe, B., Beck, B., Tonshoff, B., Hocker, B., Wygoda, S., Ehrich, J. H. H., Pape, L., Konrad, M., Rascher, W., Dotsch, J., Muller-Wiefel, D. E., Hoyer, P., Study Group Members of the Gesellschaft fur Padiatrische Nephrologie (GPN), Knebelmann, B., Pirson, Y., Grunfeld, J., Niaudet, P., Cochat, P., Heidet, L., Lebbah, S., Torra, R., Friede, T., Lange, K., Muller, G. A. & Weber, M. Early angiotensin-converting enzyme inhibition in Alport syndrome delays renal failure and improves life expectancy. Kidney Int. 81, 494–501 (2012).
107. Wühl, E., Trivelli, A., Picca, S., Litwin, M., Peco-Antic, A., Zurowska, A., Testa, S., Jankauskiene, A., Emre, S., Caldas-Afonso, A., Anarat, A., Niaudet, P., Mir, S., Bakkaloglu, A., Enke, B., Montini, G., Wingen, A., Sallay, P., Jeck, N., Berg, U., Caliskan, S., Wygoda, S., Hohbach-Hohenfellner, K., Dusek, J., Urasinski, T., Arbeiter, K., Neuhaus, T., Gellermann, J., Drozdz, D., Fischbach, M., Moller, K., Wigger, M., Peruzzi, L., Mehls, O. & Schaefer, F. Strict blood-pressure control and progression of renal failure in children. N. Engl. J. Med. 361, 1639–50 (2009).
108. Tazkarji, B., Ganeshamoorthy, A. & Auten, B. Angiotensin-Converting Enzyme Inhibitors vs. Angiotensin Receptor Blockers. Am. Fam. Physician 91, 9–10 (2015).
109. Izzo, J. L. & Weir, M. R. Angiotensin-converting enzyme inhibitors. J. Clin. Hypertens. 13, 667–675 (2011).
110. Arumugam, S., Sreedhar, R., Thandavarayan, R. A., Karuppagounder, V., Krishnamurthy, P., Suzuki, K., Nakamura, M. & Watanabe, K. Angiotensin receptor blockers: Focus on cardiac and renal injury. Trends Cardiovasc. Med. 26, 221–228 (2016).
111. Ellis, D., Moritz, M. L., Vats, A. & Janosky, J. E. Antihypertensive and renoprotective efficacy and safety of losartan: A long-term study in children with renal disorders. Am. J. Hypertens. 17, 928–935 (2004).

89
112. Webb, N. J. A., Lam, C., Shahinfar, S., Strehlau, J., Wells, T. G., Gleim, G. W. & de Tilleghem, C. L. B. Efficacy and safety of losartan in children with Alport syndrome - Results from a subgroup analysis of a prospective, randomized, placebo- or amlodipine-controlled trial. Nephrol. Dial. Transplant. 26, 2521–2526 (2011).
113. Charbit, M., Gubler, M., Dechaux, M., Gagnadoux, M., Grunfeld, J. & Niaudet, P. Cyclosporin therapy in patients with Alport syndrome. Pediatr. Nephrol. 22, 57–63 (2007).
114. Massella, L., Muda, A. O., Legato, A., Di Zazzo, G., Giannakakis, K. & Emma, F. Cyclosporine A treatment in patients with Alport syndrome: A single-center experience. Pediatr. Nephrol. 25, 1269–1275 (2010).
115. Sugimoto, K., Fujita, S., Miyazawa, T., Nishi, H., Enya, T., Izu, A., Wada, N., Sakata, N., Okada, M. & Takemura, T. Cyclosporin A may cause injury to undifferentiated glomeruli persisting in patients with Alport syndrome. Clin. Exp. Nephrol. 18, 492–498 (2014).
116. Faul, C., Donnelly, M., Merscher-Gomez, S., Chang, Y. H., Franz, S., Delfgaauw, J., Chang, J., Choi, H. Y., Campbell, K. N., Kim, K., Reiser, J. & Mundel, P. The actin cytoskeleton of kidney podocytes is a direct target of the antiproteinuric effect of cyclosporine A. Nat. Med. 14, 931–938 (2008).
117. Rao, V. H., Lees, G. E., Kashtan, C. E., Nemori, R., Singh, R. K., Meehan, D. T., Rodgers, K., Berridge, B. R., Bhattacharya, G. & Cosgrove, D. Increased expression of MMP-2, MMP-9 (type IV collagenases/gelatinases), and MT1-MMP in canine X-linked Alport syndrome (XLAS). Kidney Int. 63, 1736–1748 (2003).
118. Rao, V. H., Lees, G. E., Kashtan, C. E., Delimont, D. C., Singh, R., Meehan, D. T., Bhattacharya, G., Berridge, B. R. & Cosgrove, D. Dysregulation of renal MMP-3 and MMP-7 in canine X-linked Alport syndrome. Pediatr. Nephrol. 20, 732–739 (2005).
119. Delimont, D., Dufek, B. M., Meehan, D. T., Zallocchi, M., Gratton, M. A., Phillipos, G. & Cosgrove, D. Laminin α2-mediated focal adhesion kinase activation triggers Alport glomerular pathogenesis. PLoS One 9, (2014).
120. Sayers, R., Kalluri, R., Rodgers, K. D., Shield, C. F., Meehan, D. T. & Cosgrove, D. Role for transforming growth factor-β1 in Alport renal disease progression. Kidney Int. 56, 1662–1673 (1999).
121. Imai, E. & Isaka, Y. Perspectives for gene therapy in renal diseases. Intern. Med. 43, 85–96 (2004).
122. Gross, O., Borza, D., Anders, H., Licht, C., Weber, M., Segerer, S., Torra, R., Gubler, M., Heidet, L., Harvey, S., Cosgrove, D., Lees, G., Kashtan, C., Gregory, M., Savige, J., Ding, J., Thorner, P., Abrahamson, D. R., Antignac, C., Tryggvason, K., Hudson, B. & Miner, J. H. Stem cell therapy for Alport syndrome: the hope beyond the hype. Nephrol. Dial. Transplant. 24, 731–734 (2008).
123. Floege, J., Kunter, U., Weber, M. & Gross, O. Bone marrow transplantation rescues Alport mice. Nephrol. Dial. Transplant. 21, 2721–2723 (2006).
124. LeBleu, V., Sugimoto, H., Mundel, T. M., Gerami-Naini, B., Finan, E., Miller, C. A., Gattone, V. H., Lu, L., Shield, C. F., Folkman, J. & Kalluri, R. Stem Cell Therapies Benefit Alport Syndrome. J. Am. Soc. Nephrol. 20, 2359–2370 (2009).
125. Hickson, L. J., Eirin, A. & Lerman, L. O. Challenges and opportunities for stem cell therapy in patients with chronic kidney disease. Kidney Int. 89, 767–778 (2016).
126. Mohammed-Ali, Z., Cruz, G. L. & Dickhout, J. G. Crosstalk between the unfolded protein response and NF-κB-mediated inflammation in the progression of chronic kidney disease.

90
J. Immunol. Res. 2015, 428508 (2015). 127. Cao, Q., Harris, D. C. H. & Wang, Y. Macrophages in Kidney Injury, Inflammation, and
Fibrosis. Physiology 30, 183–194 (2015). 128. Lan, H. Y. & Chung, A. C. K. TGF-β/Smad Signaling in Kidney Disease. Semin. Nephrol.
32, 236–243 (2012). 129. Sato, Y. & Yanagita, M. Resident fibroblasts in the kidney: a major driver of fibrosis and
inflammation. Inflamm. Regen. 37, 17 (2017). 130. Lv, W., Booz, G. W., Wang, Y., Fan, F. & Roman, R. J. Inflammation and renal fibrosis:
Recent developments on key signaling molecules as potential therapeutic targets. Eur. J. Pharmacol. 820, 65–76 (2018).
131. Carlsen, H., Alexander, G., Austenaa, L. M. I., Ebihara, K. & Blomhoff, R. Molecular imaging of the transcription factor NF-κB, a primary regulator of stress response. Mutat. Res. - Fundam. Mol. Mech. Mutagen. 551, 199–211 (2004).
132. Lawrence, T. Inflammation. Cold Spring Harb. Perspect. Biol. 1–10 (2009). 133. Pedruzzi, L. M., Stockler-Pinto, M. B., Leite, M. & Mafra, D. Nrf2-keap1 system versus
NF-κB: The good and the evil in chronic kidney disease? Biochimie 94, 2461–2466 (2012).
134. Huang, B., Yang, X. D., Zhou, M. M., Ozato, K. & Chen, L. F. Brd4 coactivates transcriptional activation of NF-kappaB via specific binding to acetylated RelA. Mol Cell Biol 29, 1375–1387 (2009).
135. Zou, Z., Huang, B., Wu, X., Zhang, H., Qi, J., Bradner, J., Nair, S. & Chen, L. Brd4 maintains constitutively active NF-κB in cancer cells by binding to acetylated RelA. Oncogene 33, 2395–2404 (2014).
136. Brown, J. D., Lin, C. Y., Duan, Q., Grifin, G., Federation, A., Paranal, R. M., Bair, S., Newton, G., Lichtman, A., Kung, A., Yang, T., Wang, H., Luscinskas, F. W., Croce, K., Bradner, J. E. & Plutzky, J. NF-kB directs dynamic super enhancer formation in inflammation and atherogenesis. Mol Cell. 56, 219–231 (2014).
137. Tian, B., Yang, J., Zhao, Y., Ivanciuc, T., Sun, H., Garofalo, R. P. & Brasier, A. R. BRD4 Couples NF-κB/RelA with Airway Inflammation and the IRF-RIG-I Amplification Loop in Respiratory Syncytial Virus Infection. J. Virol. 91, 1–28 (2017).
138. Huang, F., Shao, W., Fujinaga, K. & Peterlin, B. M. Bromodomian-containing protein 4-independent transcriptional activation by autoimmune regulator (AIRE) and NF-κB. J. Biol. Chem. jbc.RA117.001518 (2018). doi:10.1074/jbc.RA117.001518
139. Hytti, M., Tokarz, P., Maatta, E., Piippo, N., Korhonen, E., Suuronen, T., Honkakoski, P., Kaarniranta, K., Lahtela-Kakkonen, M. & Kauppinen, A. Inhibition of BET bromodomains alleviates inflammation in human RPE cells. Biochem. Pharmacol. 110–111, 71–79 (2016).
140. Zhang, G., Liu, R., Zhong, Y., Plotnikov, A. N., Zhang, W., Zeng, L., Rusinova, E., Gerona-Nevarro, G., Moshkina, N., Joshua, J., Chuang, P. Y., Ohlmeyer, M., He, J. C. & Zhou, M. Down-regulation of NF-κB transcriptional activity in HIV-associated kidney disease by BRD4 inhibition. J. Biol. Chem. 287, 28840–28851 (2012).
141. Breyer, M. D. & Susztak, K. The next generation of therapeutics for chronic kidney disease. Nat. Rev. Drug Discov. 15, 568–588 (2016).
142. Liu, R., Zhong, Y., Li, X., Chen, H., Jim, B., Zhou, M., Chuang, P. Y. & He, J. C. Role of transcription factor acetylation in diabetic kidney disease. Diabetes 63, 2440–2453 (2014).
143. Chen, C. J., Kono, H., Golenbock, D., Reed, G., Akira, S. & Rock, K. L. Identification of

91
a key pathway required for the sterile inflammatory response triggered by dying cells. Nat. Med. 13, 851–856 (2007).
144. Ernandez, T. & Mayadas, T. N. The Changing landscape of renal inflammation. Trends Mol. Med. 22, 151–163 (2016).
145. Takemoto, M., Asker, N., Gerhardt, H., Lundkvist, A., Johansson, B. R., Saito, Y. & Betsholtz, C. A new method for large scale isolation of kidney glomeruli from mice. Am. J. Pathol. 161, 799–805 (2002).
146. Schwarz, M., Taubitz, A., Eltrich, N., Mulay, S. R., Allam, R. & Vielhauer, V. Analysis of TNF-mediated recruitment and activation of glomerular dendritic cells in mouse kidneys by compartment-specific flow cytometry. Kidney Int. 84, 116–29 (2013).
147. Cosgrove, D., Samuleson, G., Meehan, D. T., Miller, C., McGee, J., Walsh, E. J. & Siegel, M. Ultrastructural, physiological, and molecular defects in the inner ear of a gene-knockout mouse model for autosomal Alport syndrome. Hear. Res. 121, 84–98 (1998).
148. Lu, W., Phillips, C. L., Killen, P. D., Hlaing, T., Harrison, W. R., Elder, F. F. B., Miner, J. H., Overbeek, P. A. & Meisler, M. H. Insertional mutation of the collagen genes Col4a3 and Col4a4 in a mouse model of Alport syndrome. Genomics 61, 113–124 (1999).
149. Heidet, L., Borza, D., Jouin, M., Sich, M., Mattei, M., Sado, Y., Hudson, B. G., Hastie, N., Antignac, C. & Gubler, M. A human-mouse chimera of the α3α4α5(IV) collagen protomer rescues the renal phenotype in Col4a3-/-alport mice. Am. J. Pathol. 163, 1633–1644 (2003).
150. Beirowski, B. Chronic Renal Failure and Shortened Lifespan in COL4A3+/- Mice: An Animal Model for Thin Basement Membrane Nephropathy. J. Am. Soc. Nephrol. 17, 1986–1994 (2006).
151. Katayama, K. Searching for a treatment for Alport syndrome using mouse models. World J. Nephrol. 3, 230 (2014).
152. Bae, E. H., Konvalinka, A., Fang, F., Zhou, X., Williams, V., Maksimowski, N., Song, X., Zhang, S. L., John, R., Oudit, G. Y., Pei, Y. & Scholey, J. W. Characterization of the Intrarenal Renin-Angiotensin System in Experimental Alport Syndrome. Am. J. Pathol. 185, 1423–1435 (2015).
153. Bae, E. H., Fang, F., Williams, V., Konvalinka, A., Zhou, X., Patel, V. B., Song, X., John, R., Oudit, G. Y., Pei, Y. & Scholey, J. W. Murine recombinant angiotensin-converting enzyme 2 attenuates kidney injury in experimental Alport syndrome. Kidney Int. 91, 1347–1361 (2017).
154. Neuburg, S., Dussold, C., Gerber, C., Wang, X., Francis, C., Qi, L., David, V., Wolf, M. & Martin, A. Genetic background influences cardiac phenotype in murine chronic kidney disease. Nephrol. Dial. Transplant. 1–9 (2017). doi:10.1093/ndt/gfx332
155. Mueller, O. & Schroeder, A. RNA Integrity Number ( RIN ) – Standardization of RNA Quality Control Application. Nano 1–8 (2004). doi:10.1101/gr.189621.115.7
156. Scientific, T. T042-Technical Bulletin NanoDrop Spectrophotometers 260/280 and 260/230 Ratios. doi:10.1002/jobm.19770170116
157. Cosgrove, D. Glomerular pathology in Alport syndrome: a molecular perspective. 18, 1199–1216 (2012).
158. Kamiyoshi, N., Nozu, K., Fu, X. J., Morisada, N., Nozu, Y., Ye, M. J., Imafuku, A., Miura, K., Yamamura, T., Minamikawa, S., Shono, A., Ninchoji, T., Morioka, I., Nakanishi, K., Yoshikawa, N., Kaito, H. & Iijima, K. Genetic, clinical, and pathologic backgrounds of patients with autosomal dominant alport syndrome. Clin. J. Am. Soc. Nephrol. 11, 1441–

92
1449 (2016). 159. Li, Z., Su, Z., Wen, Z., Shi, L. & Chen, T. Microarray platform consistency is revealed by
biologically functional analysis of gene expression profiles. BMC Bioinformatics 10, 1–8 (2009).
160. Hauser, P. V., Perco, P., Muhlberger, I., Pippin, J., Blonski, M., Mayer, B., Alpers, C. E., Oberbauer, R. & Shankland, S. J. Microarray and bioinformatics analysis of gene expression in experimental membranous nephropathy. Nephron - Exp. Nephrol. 112, 43–58 (2009).
161. Hopcroft, L. E. M., McBride, M. W., Harris, K. J., Sampson, A. K., McClure, J. D., Graham, D., Young, G., Holyoake, T. L., Girolami, M. A. & Dominiczak, A. F. Predictive response-relevant clustering of expression data provides insights into disease processes. Nucleic Acids Res. 38, 6831–6840 (2010).
162. Jedlicka, J., Soleiman, A., Draganovici, D., Mandelbaum, J., Ziegler, U., Regele, H., Wuthrich, R. P., Gross, O., Anders, H. & Segerer, S. Interstitial inflammation in Alport syndrome. Hum. Pathol. 41, 582–593 (2010).
163. Gonçalves, G. M., Zamboni, D. S. & Cĝmara, N. O. S. The role of innate immunity in septic acute kidney injuries. Shock 34, 22–26 (2010).
164. Al-Lamki, R. S. & Mayadas, T. N. TNF receptors: Signaling pathways and contribution to renal dysfunction. Kidney Int. 87, 281–296 (2015).
165. Sanz, A. B., Sanchez-Nĩo, M. D. & Ortiz, A. TWEAK, a multifunctional cytokine in kidney injury. Kidney Int. 80, 708–718 (2011).
166. Poveda, J., Tabara, L. C., Fernandez-Fernandez, B., Martin-Cleary, C., Sanz, A. B., Selgas, R., Ortiz, A. & Sanchez-Nino, M. D. TWEAK/Fn14 and non-canonical NF-kappaB signaling in kidney disease. Front. Immunol. 4, 1–7 (2013).
167. Liu, M., Guo, S., Hibbert, J. M., Jain, V., Singh, N., Wilson, N. O. & Stiles, J. K. CXCL10/IP-10 in infectious diseases pathogenesis and potential therapeutic implications. Cytokine Growth Factor Rev. 22, 121–130 (2011).
168. Petrovic-Djergovic, D., Popovic, M., Chittiprol, S., Cortado, H., Ransom, R. F. & Partida-Sanchez, S. CXCL10 induces the recruitment of monocyte-derived macrophages into kidney, which aggravate puromycin aminonucleoside nephrosis. Clin. Exp. Immunol. 180, 305–315 (2015).
169. Kaffe, E., Fiorotto, R., Pellegrino, F., Mariotti, V., Amenduni, M., Cadamuro, M., Fabris, L., Strazzabosco, M. & Spirli, C. β-Catenin and interleukin-1β–dependent chemokine (C-X-C motif) ligand 10 production drives progression of disease in a mouse model of congenital hepatic fibrosis. Hepatology 67, 1903–1919 (2018).
170. Plank, C., Hartner, A., Klanke, B., Geissler, B., Porst, M., Amann, K., Hilgers, K. F., Rascher, W. & Dotsch, J. Adrenomedullin reduces mesangial cell number and glomerular inflammation in experimental mesangioproliferative glomerulonephritis. Kidney Int. 68, 1086–1095 (2005).
171. Bunton, D. C., Petrie, M. C., Hillier, C., Johnston, F. & McMurray, J. J. V. The clinical relevance of adrenomedullin: A promising profile? Pharmacol. Ther. 103, 179–201 (2004).
172. Shah, K. G. Rajan, D., Jacob, A., Wu, R., Krishnasastry, K., Nicastro, J., Molmenti, E. P., Coppa, G. F. & Wang, P. Attenuation of renal ischemia and reperfusion injury by human adrenomedullin and its binding protein. J. Surg. Res. 163, 110–117 (2010).
173. Zhang, J. J., Yoshida, H., Chao, L. & Chao, J. Human adrenomedullin gene delivery

93
protects against cardiac hypertrophy, fibrosis, and renal damage in hypertensive dahl salt-sensitive rats. Hum. Gene Ther. 11, 1817–1827 (2000).
174. Mukoyama, M., Sugawara, A., Nagae, T., Mori, K., Murabe, H., Itoh, H., Tanaka, I. & Nakao, K. Role of adrenomedullin and its receptor system in renal pathophysiology. Peptides 22, 1925–1931 (2001).
175. Malik, K. U., Jennings, B. L., Yaghini, F. A., Sahan-Firat, S., Song, C. Y., Estes, A. M. & Fang, X. R. Contribution of cytochrome P450 1B1 to hypertension and associated pathophysiology: A novel target for antihypertensive agents. Prostaglandins Other Lipid Mediat. 98, 69–74 (2012).
176. Cheung, Y.-L., Kerr, A. C., McFadyen, M. C. E., Melvin, W. T. & Murray, G. I. Differential expression of CYP1A1 and CYP1B1 in human breast cancer. Biochem. Soc. Trans. 24, 327S (1966).
177. Zordoky, B. N. M., Anwar-mohamed, A., Aboutabl, M. E. & El-kadi, A. O. S. Acute Doxorubicin Toxicity Differentially Alters Cytochrome P450 Expression and Arachidonic Acid Metabolism in Rat Kidney and Liver ABSTRACT : Drug Metab. Dispos. 39, 1440–1450 (2011).
178. McFadyen, M. C. E., Melvin, W. T. & Murray, G. I. Cytochrome P450 CYP1B1 activity in renal cell carcinoma. Br. J. Cancer 966–971 (2004). doi:10.1038/sj.bjc.6602053
179. Ward, J. M., Nikolov, N. P., Tschetter, J. R., Kopp, J. B., Gonzalez, F. J., Kimura, S. & Siegel, R. M. Progressive glomerulonephritis and histiocytic sarcoma associated with macrophage functional defects in CYP1B1-deficient mice. Toxicol. Pathol. 32, 710–718 (2004).
180. Jennings, B. L., Anderson, L. J., Estes, A. M., Yaghini, F. A., Fang, X. R., Porter, J., Gonzalez, F. J., Campbell, W. B. & Malik, K. U. Cytochrome P450 1B1 contributes to renal dysfunction and damage caused by angiotensin II in mice. Hypertension 59, 348–354 (2012).
181. Pingili, A. K., Thirunavukkarasu, S., Kara, M., Barnd, D. D., Katsurada, A., Majid, D. S., Navar, L. G., Gonzalez, F. J. & Malik, K. U. 6β-hydroxytestosterone, a cytochrome P450 1B1-testosterone-metabolite, mediates angiotensin II-induced renal dysfunction in male mice. Hypertension 67, 916–926 (2016).
182. Wang, T. Renal outer medullary potassium channel knockout models reveal thick ascending limb function and dysfunction. Clin. Exp. Nephrol. 16, 49–54 (2012).
183. Miao, J., Fan, Q., Cui, Q., Zhang, H., Chen, L., Wang, S., Guan, N., Guan, Y. & Ding, J. Newly identified cytoskeletal components are associated with dynamic changes of podocyte foot processes. Nephrol. Dial. Transplant. 24, 3297–3305 (2009).
184. Gerolymos, M., Karagianni, F., Papsotiriou, M., Kalliakmani, P., Sotsiou, F., Charonis, A. & Goumenos, D. S. Expression of Transgelin in Human Glomerulonephritis of Various Etiology. Nephron Clin Pr. 119, 74–82 (2011).
185. Daniel, C., Ludke, A., Wagner, A., Todorov, V. T., Hohenstein, B. & Hugo, C. Transgelin is a marker of repopulating mesangial cells after injury and promotes their proliferation and migration. Lab. Investig. 92, 812–826 (2012).
186. Marshall, C. B., Krofft, R. D., Blonski, M. J., Kowalewska, J., Logar, C. M., Pippin, J. W., Kim, F., Feil, R., Alpers, C. E. & Shankland, S. J. Role of smooth muscle protein SM22α in glomerular epithelial cell injury. Am. J. Physiol. - Ren. Physiol. 300, 1026–1042 (2011).
187. Karagianni, F., Prakoura, N., Kaltsa, G., Politis, P., Arvaniti, E., Kaltezioti, V., Psarras, S., Pagakis, S., Katsimboulas, M., Abed, A., Chatziantoniou, C. & Charonis, A. Transgelin

94
Up-Regulation in Obstructive Nephropathy. PLoS One 8, 1–10 (2013). 188. Elzi, D. J., Song, M., Hakala, K., Weintraub, S. T. & Shiio, Y. Wnt Antagonist SFRP1
Functions as a Secreted Mediator of Senescence. Mol. Cell. Biol. 32, 4388–4399 (2012). 189. Bovolenta, P., Esteve, P., Ruiz, J. M., Cisneros, E. & Lopez-Rios, J. Beyond Wnt
inhibition: new functions of secreted Frizzled-related proteins in development and disease. J. Cell Sci. 121, 737–746 (2008).
190. Dahl, E., Wiesmann, F., Woenckhaus, M., Stoehr, R., Wild, P. J., Veeck, J., Knuchel, R., Klopocki, E., Sauter, G., Simon, R., Wieland, W. F., Walter, B., Denzinger, S., Hartmann, A. & Hammerschmied, C. G. Frequent loss of SFRP1 expression in multiple human solid tumours: Association with aberrant promoter methylation in renal cell carcinoma. Oncogene 26, 5680–5691 (2007).
191. Atschekzei, F., Hennenlotter, J., Janisch, S., Grobhennig, A., Trankenschuh, W., Waalkes, S., Peters, I., Dork, T., Merseburger, A. S., Stenzl, A., Kuczyk, M. A. & Serth, J. SFRP1 CpG island methylation locus is associated with renal cell cancer susceptibility and disease recurrence. Epigenetics 7, 447–457 (2012).
192. Matsuyama, M., Nomori, A., Nakakuni, K., Shimono, A. & Fukushima, M. Secreted frizzled-related protein 1 (Sfrp1) regulates the progression of renal fibrosis in a mouse model of obstructive nephropathy. J. Biol. Chem. 289, 31526–31533 (2014).
193. Susantitaphong, P., Perianayagam, M. C., Kang, S. W., Zhang, W., Rao, F., O'Connor, D. T. & Jaber, B. L. Association of functional kallikrein-1 promoter polymorphisms and acute kidney injury: A case-control and longitudinal cohort study. Nephron - Clin. Pract. 122, 107–113 (2012).
194. Yiu, W. H., Lin, M. & Tang, S. C. W. Toll-like receptor activation: From renal inflammation to fibrosis. Kidney Int. Suppl. 4, 20–25 (2014).
195. Chao, J. & Chao, L. Kallikrein gene therapy in hypertension, cardiovascular and renal diseases. Gene Ther. Mol. Biol. 1, 301–308 (1998).
196. Bledsoe, G., Crickman, S., Mao, J., Xia, C. F., Murakami, H., Chao, L. & Chao, J. Kallikrein/kinin protects against gentamicin-induced nephrotoxicity by inhibition of inflammation and apoptosis. Nephrol. Dial. Transplant. 21, 624–633 (2006).
197. Buendía, P., Ramírez, R., Aljama, P. & Carracedo, J. Klotho Prevents Translocation of NFκB. Vitam. Horm. 101, 119–150 (2016).
198. Kang, S. W., Shih, P. A., Mathew, R. O., Mahata, M., Biswas, N., Rao, F., Yan, L., Bouchard, J., Malhotra, R., Tolwani, A., Khandrika, S., Mehta, R. L. & O'Connor, D. T. Renal kallikrein excretion and epigenetics in human acute kidney injury: Expression, mechanisms and consequences. BMC Nephrol. 12, (2011).
199. Ruiz-Andres, O., Sanchez-Nino, M. D., Moreno, J. A., Ruiz-Ortega, M., Ramos, A. M., Sanz, A. B. & Ortiz, A. Downregulation of kidney protective factors by inflammation: role of transcription factors and epigenetic mechanisms. Am. J. Physiol. - Ren. Physiol. 311, F1329–F1340 (2016).
200. Moreno, J. A., Izquierdo, M. C., Sanchez-Nino, M. D., Suarez-Alvarez, B., Lopez-Larrea, C., Jakubowski, A., Blanco, J., Ramirez, R., Selgas, R., Ruiz-Ortega, M., Egido, J., Ortiz, A. & Sanz, A. B. The Inflammatory Cytokines TWEAK and TNF Reduce Renal Klotho Expression through NF B. J. Am. Soc. Nephrol. 22, 1315–1325 (2011).
201. Zhao, Y., Banerjee, S., Dey, N., LeJeune, W. S., Sarkar, P. S., Brobey, R., Rosenblatt, K. P., Tilton, R. G. & Choudhary, S.. Klotho depletion contributes to increased inflammation in kidney of the db/db mouse model of diabetes via RelA (serine)536 phosphorylation.

95
Diabetes 60, 1907–1916 (2011). 202. Izquierdo, M. C., Perez-Gomez, M. V., Sanchez-Nino, M. D., Sanz, A. B., Ruiz-Andres,
O., Poveda, J., Moreno, J. A., Egido, J. & Ortiz, A. Klotho, phosphate and inflammation/ageing in chronic kidney disease. Nephrol. Dial. Transplant. 27, 6–10 (2012).
203. Paulais, M., Bloch-Faure, M., Picard, N., Jacques, T., Ramakrishnan, S. K., Keck, M., Sohet, F., Eladari, D., Houillier, P., Lourdel, S., Teulon, J. & Tucker, S. J. Renal phenotype in mice lacking the Kir5.1 (Kcnj16) K+ channel subunit contrasts with that observed in SeSAME/EAST syndrome. Proc. Natl. Acad. Sci. 108, 10361–10366 (2011).
204. Abdelhadi, O., Iancu, D., Stanescu, H., Kleta, R. & Bockenhauer, D. EAST syndrome: Clinical, pathophysiological, and genetic aspects of mutations in KCNJ10. Rare Dis. 4, e1195043 (2016).
205. Wang, X., Sakatsume, M., Sakamaki, Y., Inomata, S., Yamamoto, T. & Narita, I. Quantitative histological analysis of SM22α (Transgelin) in an adriamycin-induced focal segmental glomerulosclerosis model. Nephron - Exp. Nephrol. 120, 1–11 (2012).
206. Schmidt, C., Hocherl, K., Schweda, F., Kurtz, A. & Bucher, M. Regulation of Renal Sodium Transporters during Severe Inflammation. J. Am. Soc. Nephrol. 18, 1072–1083 (2007).
207. Kim, J. H., Ha, I. S., Hwang, C. I., Lee, Y. J., Kim, J., Yang, S. H., Kim, Y. S., Cao, Y. A., Choi, S. & Park, W. Y. Gene expression profiling of anti-GBM glomerulonephritis model: the role of NF-kappaB in immune complex kidney disease. Kidney Int. 66, 1826–37 (2004).
208. Khan, M. I., Dębski, K. J., Dabrowski, M., Czarnecka, A. M. & Szczylik, C. Gene set enrichment analysis and ingenuity pathway analysis of metastatic clear cell renal cell carcinoma cell line. Am. J. Physiol. - Ren. Physiol. 311, F424–F436 (2016).
209. L.-T., L., Chang, C. Y., Chang, C. H., Wang, H. E., Chiou, S. H., Liu, R. S., Lee, T. W. & Lee, Y. J. Involvement of let-7 microRNA for the therapeutic effects of Rhenium-188-embedded liposomal nanoparticles on orthotopic human head and neck cancer model. Oncotarget 7, 65782–65796 (2016).
210. Hilbert, T., Markowski, P., Frede, S., Boehm, O., Kneufermann, P., Baumgarten, G., Hoeft, A. & Klaschik, S. Synthetic CpG oligonucleotides induce a genetic profile ameliorating murine myocardial I/R injury. J. Cell. Mol. Med. 22, 3397–3407 (2018).
211. O’Brown, Z. K., Van Nostrand, E. L., Higgins, J. P. & Kim, S. K. The Inflammatory Transcription Factors NFκB, STAT1 and STAT3 Drive Age-Associated Transcriptional Changes in the Human Kidney. PLoS Genet. 11, 1–28 (2015).
212. Nakagawa, S., Nishihara, K., Miyata, H., Shinke, H., Tomita, E., Kajiwara, M., Matsubara, T., Iehara, N., Igarashi, Y., Yamada, H., Fukatsu, A., Yanagita, M., Matsubara, K. & Masuda, S. Molecular markers of tubulointerstitial fibrosis and tubular cell damage in patients with chronic kidney disease. PLoS One 10, 1–14 (2015).
213. Smith, K. D. Toll-like receptors in kidney disease. Curr. Opin. Nephrol. Hypertens. 18, 189–196 (2009).
214. Lin, M. & Tang, S. C. W. Toll-like receptors: Sensing and reacting to diabetic injury in the kidney. Nephrol. Dial. Transplant. 29, 746–754 (2014).
215. Anderberg, S. B., Luther, T. & Frithiof, R. Physiological aspects of Toll-like receptor 4 activation in sepsis-induced acute kidney injury. Acta Physiol. 219, 573–588 (2017).
216. Kezic, A., Stajic, N. & Thaiss, F. Review Article Innate Immune Response in Kidney

96
Ischemia / Reperfusion Injury : Potential Target for Therapy. J. Immunol. Res. 2017, 1–10 (2017).
217. Chen, G. Y. & Nuñez, G. Sterile inflammation: sensing and reacting to damage. Nat. Rev. Immunol. 10, 826–37 (2010).
218. Hu, X., Chung, A. Y., Wu, I., Foldi, J., Ji, J. D., Tateya, T., Kang, Y. J., Han, J., Gessler, M., Kageyama, R. & Ivashkiv, L. B. Integrated Regulation of Toll-like Receptor Responses by Notch and Interferon-γ Pathways. Immunity 29, 691–703 (2008).
219. Kuzmich, N., Sivak, K. V., Chubarev, V. N., Porozov, Y. B., Savateeva-Lyubimova, T. N. & Peri, F. TLR4 Signaling Pathway Modulators as Potential Therapeutics in Inflammation and Sepsis. Vaccines 5, 34 (2017).
220. Anders, H. J. & Lech, M. NOD-like and Toll-like receptors or inflammasomes contribute to kidney disease in a canonical and a non-canonical manner. Kidney Int. 84, 225–228 (2013).
221. Anders, H.-J. & Muruve, D. A. The Inflammasomes in Kidney Disease. J. Am. Soc. Nephrol. 22, 1007–1018 (2011).
222. Garibotto, G., Carta, A., Picciotto, D., Viazzi, F. & Verzola, D. Toll-like receptor-4 signaling mediates inflammation and tissue injury in diabetic nephropathy. J. Nephrol. 30, 719–727 (2017).
223. Mathur, A., Hayward, J. A. & Man, S. M. Molecular mechanisms of inflammasome signaling. J. Leukoc. Biol. jlb.3MR0617-250R (2017). doi:10.1189/jlb.3MR0617-250R
224. Gluba, A., Banach, M., Hannam, S., Mikhailidis, D. P., Sakowicz, A. & Rysz, J. The role of Toll-like receptors in renal diseases. Nat. Rev. Nephrol. 6, 224–235 (2010).
225. Rathinam, V. A. K., Vanaja, S. K. & Fitzgerald, K. A. Regulation of inflammasome signaling. Nat. Immunol. 13, 333–342 (2012).
226. Mao, S. & Huang, S. Toll-like receptors signaling in glomerular diseases. J. Recept. Signal Transduct. 34, 81–84 (2014).
227. Leemans, J. C., Kors, L., Anders, H.-J. & Florquin, S. Pattern recognition receptors and the inflammasome in kidney disease. Nat. Rev. Nephrol. 10, 398–414 (2014).
228. Zhao, H., Perez, J. S., Lu, K., George, A. J. & Ma, D. Role of Toll-like receptor-4 in renal graft ischemia-reperfusion injury. Am J Physiol Ren. Physiol 306, F801-11 (2014).
229. Ma, J., Chadban, S. J., Zhao, C. Y., Chen, X., Kwan, T., Panchapakesan, U., Pollock, C. A. & Wu, H. TLR4 activation promotes podocyte injury and interstitial fibrosis in diabetic nephropathy. PLoS One 9, (2014).
230. Chen, C. J., Shi, Y., Hearn, A., Fitzgerald, K., Golenbock, D., Reed, G., Akira, S. & Rock, K. L. MyD88-dependent IL-1 receptor signaling is essential for gouty inflammation stimulated by monosodium urate crystals. J. Clin. Invest. 116, 2262–2271 (2006).
231. Layoun, A., Huang, H., Calvé, A. & Santos, M. M. Toll-like receptor signal adaptor protein MyD88 is required for sustained endotoxin-induced acute hypoferremic response in mice. Am. J. Pathol. 180, 2340–2350 (2012).
232. Perrone, L. A., Szretter, K. J., Katz, J. M., Mizgerd, J. P. & Tumpey, T. M. Mice lacking both TNF and IL-1 receptors exhibit reduced lung inflammation and delay in onset of death following infection with a highly virulent H5N1 virus. J Infect Dis 202, 1161–1170 (2010).
233. Lukens, J. R., Gross, J. M. & Kanneganti, T. D. IL-1 family cytokines trigger sterile inflammatory disease. Front. Immunol. 3, 1–12 (2012).
234. Borthwick, L. A. The IL-1 cytokine family and its role in inflammation and fibrosis in the

97
lung. Semin. Immunopathol. 38, 517–534 (2016). 235. Franchi, L., Eigenbrod, T., Muñoz-Planillo, R. & Nuñez, G. The Inflammasome: A
Caspase-1 Activation Platform Regulating Immune Responses and Disease Pathogenesis. Nat. Immun. 10, 241 (2009).
236. Shang, L., Daubeuf, B., Triantafilou, M., Olden, R., Depis, F., Raby, A. C., Herren, S., Dos Santos, A., Malinge, P., Dunn-Siegrist, I., Benmkaddem, S., Geinoz, A., Magistrelli, G., Rousseau, F., Buatois, V., Salgado-Pires, S., Reith, W., Monteiro, R., Pugin, J., Leger, O., Ferlin, W., Kosco-Vilbois, M., Triantafilou, K. & Elson, G. Selective antibody intervention of toll-like receptor 4 activation through Fc γ receptor tethering. J. Biol. Chem. 289, 15309–15318 (2014).
237. Liu, T., Zhang, L., Joo, D. & Sun, S.-C. NF-κB signaling in inflammation. Signal Transduct. Target. Ther. 2, 17023 (2017).
238. Khasnavis, S., Jana, A., Roy, A., Wood, T. & Ghosh, S. Suppression of nuclear factor-kappa B activation and inflammation in microglia by a physically-modified saline. J. Biol. Chem. 287, 29529–29542 (2012).
239. Souza, G. R., Cunha, T. M., Silva, R. L., Lotufo, C. M., Verri, W. A., Funez, M. I., Villarreal, C. F., Talbot, J., Sousa, L. P., Parada, C. A., Cunha, F. Q. & Ferreira, S. H. Involvement of nuclear factor kappa B in the maintenance of persistent inflammatory hypernociception. Pharmacol. Biochem. Behav. 134, 49–56 (2015).
240. Oeckinghaus, A. & Ghosh, S. The NF- k B Family of Transcription Factors and Its Regulation. Cold Spring Harb. Perspect. Biol. 1, 1–14 (2009).
241. Huang, B., Yang, X.-D., Lamb, A. & Chen, L.-F. Posttranslational modifications of NF-κB: another layer of regulation for NF-κB signaling pathway Bo. Cell Signal 22, 1282–1290 (2010).
242. Hajmirza, A., Emadali, A., Gauthier, A., Casasnovas, O., Gressin, R. & Callana, M. B. BET Family Protein BRD4 : An Emerging Actor in NF κ B Signaling in Inflammation and Cancer. Biomedicines 6, 1–9 (2018).
243. Yumi, T., Kanno, N., Sensiate, L. A. & Paula, N. A. De. Toxic effects of different doses of cyclophosphamide on the reproductive parameters of male mice. Brazilian J. Pharm. Sci. 45, (2009).
244. Silva, A. H., Locatelli, C., Filippin-Monteiro, F. B., Martin, P., Liptrott, N. J., Zanetti-Ramos, B. G., Benetti, L. C., Nazari, E. M., Albuquerque, C. A., Pasa, A. A., Owen, A. & Creczynski-Pasa, T. B. Toxicity and inflammatory response in Swiss albino mice after intraperitoneal and oral administration of polyurethane nanoparticles. Toxicol. Lett. 246, 17–27 (2016).
245. Imig, J. D. & Ryan, M. J. Immune and Inflammatory Role in Renal Disease. Compr Physiol 3, 957–976 (2013).
246. Du, T. & Zhu, Y. The Regulation of Inflammatory Mediators in Acute Kidney Injury via Exogenous Mesenchymal Stem Cells. Mediators Inflamm. 2014, 11 (2014).
247. Kim, S. Il & Choi, M. E. Kidney Research and Clinical Practice TGF- b -activated kinase-1 : New insights into the mechanism of TGF- b signaling and kidney disease. Kidney Res. Clin. Pract. 31, 94–105 (2012).
248. Chen, L., Yang, T., Lu, D. W., Zhao, H., Feng, Y. L., Chen, H., Chen, D. Q., Vaziri, N. D. & Zhao, Y. Y. Central role of dysregulation of TGF- β / Smad in CKD progression and potential targets of its treatment. Biomed. Pharmacother. 101, 670–681 (2018).
249. Tbahriti, H. F., Meknassi, D., Moussaoui, R., Messaoudi, A., Zemour, L., Kaddous, A.,

98
Bouchenak, M. & Mekki, K. Inflammatory status in chronic renal failure: The role of homocysteinemia and pro-inflammatory cytokines. World J Nephrol 2, 31–37 (2013).
250. Koga, T., Kai, Y., Fukuda, R., Morino-Koga, S., Suico, M. A., Koyama, K., Sato, T., Shuto, T. & Kai, H. Mild Electrical Stimulation and Heat Shock Ameliorates Progressive Proteinuria and Renal Inflammation in Mouse Model of Alport Syndrome. PLoS One 7, 1–11 (2012).



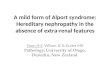










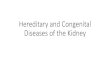
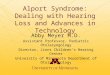







![Alport Syndrome[1]](https://img.pdfslide.us/doc/110x75/5451f437b1af9f7a248b4b70/alport-syndrome1.jpg)





