Embed Size (px)
Citation preview

E
TP
KITR
giacun
vtwtm
1a
ctacopfoi(ttm(T
psctw
1d
Joint Bone Spine 77 (2010) 96–98
ditorial
argeting intracellular signaling pathways to treat rheumatoid arthritis:andora’s box?
eywords:ntracellular signaling peptides and proteinsreatmentheumatoid arthritis
The introduction of targeted biotherapies based on insightsained into the immunopathogenesis of rheumatoid arthritis (RA)s a major breakthrough. Currently available targeted biotherapiesct on cytokines (IL-1, TNF, or IL-6) or cell populations (B cells or T-ell activation) via monoclonal antibodies or fusion proteins. Theirse is limited by a number of factors (e.g., immunogenic potential,eed for parenteral administration, and high production costs).
Intracellular signaling pathways have been implicated in thearious stages of the inflammation and joint destruction processhat characterizes RA. They can be blocked by specific inhibitors,hich are already used to treat various malignancies. Treatments
argeting intracellular pathways may hold promise for the treat-ent of RA.
. Intracellular signaling pathways relevant to rheumatoidrthritis
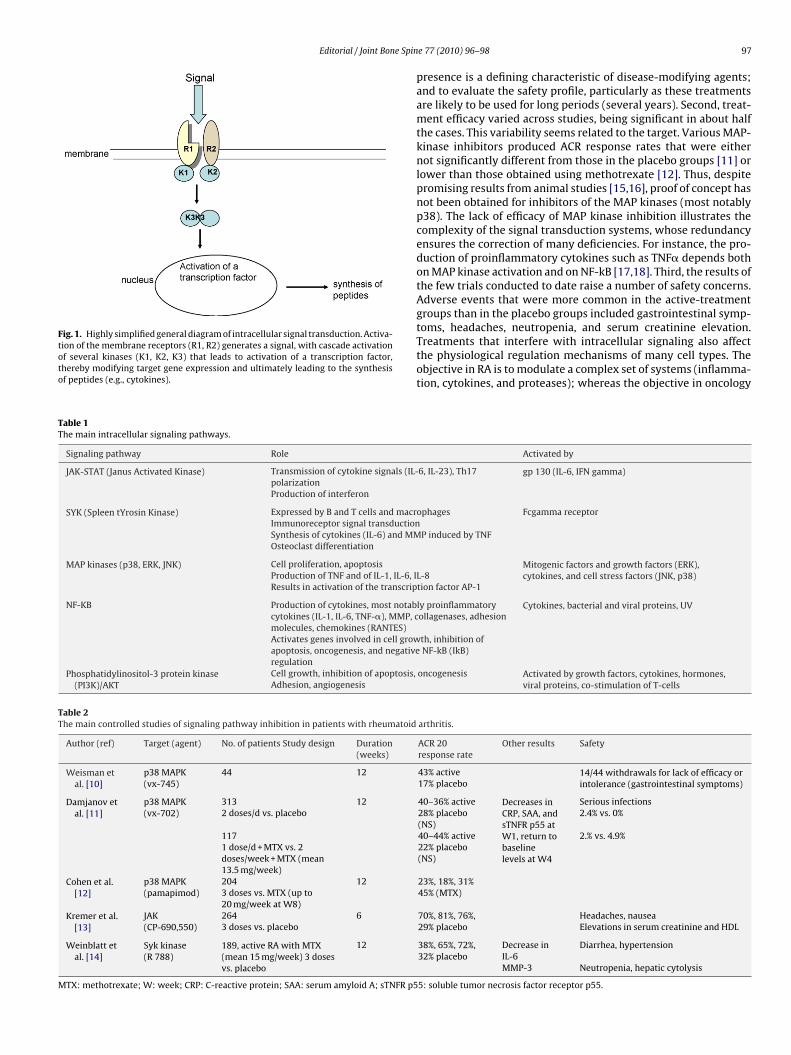
Signals travel from the cell membrane to the nucleus via intra-ellular signaling pathways that also modulate the signals duringheir transmission. Most signals are generated when a peptide (e.g.,cytokine) binds to a membrane receptor. The signal travels in theell via a sequence of kinase-induced activating phosphorylationsr phosphatase-induced inhibiting dephosphorylations [1,2]. Thehosphorylation cascade leads to the activation of a transcriptionactor (e.g., NF-kB or AP-1), which modifies the expression levelf the target genes (Fig. 1). Among the many signaling pathwaysdentified to date, some are selectively involved in inflammationTable 1) [1–7]. These pathways are interconnected into a networkhat shows substantial redundancy. They are also largely ubiqui-ous, being identical in most cells, although a few pathways are
ore specialized and occur only in limited numbers of cell typese.g., spleen tyrosine kinases [SYK] are expressed chiefly in B cells,cells, and macrophages).
Intracellular signaling pathways are composed of families of cell
roteins that recognize intracellular recognition molecules (e.g.,uppressors of cytokine signaling [SOCS] inhibit JAK/STAT3). Theonsiderable complexity of the signaling system that results fromhis cascade structure enables subtle regulation of cell activation,ith effects on a large number of potential targets. Furthermore,297-319X/$ – see front matter © 2010 Société francaise de rhumatologie. Published by Eoi:10.1016/j.jbspin.2010.01.004
activation of a given signaling pathway produces different effectsdepending on the cell type. Signaling pathways can be activatednot only by cytokines, but also by other factors such as viral andbacterial proteins, heat, ultraviolet radiation, and hormones [1].
Many studies have established that intracellular signaling path-ways are involved in the pathogenesis of RA. These pathways arecentral to the mechanisms underlying the inflammatory process,being both activated by cytokines and responsible for cytokine pro-duction. Thus, inhibition of signal transduction pathways mightabolish not only cell activation induced by cytokines or other stim-uli, but also the production of new molecules of proinflammatorycytokines. In RA, overexpression of molecules involved in intracel-lular signal transduction has been found at sites of inflammation,most notably in the rheumatoid synovium [1], where NF-KB, MAPK,and JAK/STAT are increased. A study of peripheral blood mononu-clear cells from RA patients showed increased NF-kB activation thatwas chiefly mediated by TNF� [8]. In a mouse model of arthritis,direct NF-kB inhibition (via the administration of mutated I-kB)inhibited the in vivo production of TNF and RANK-Ligand, abolishedthe manifestations of arthritis, and halted the osteoclast activation[9].
2. Inhibition of signaling pathways
Several approaches can be used. For instance, NF-kB activationcan be blocked by the administration of proteasome inhibitors (e.g.,bortezomib) that prevent the destruction of the NF-kB inhibitor (I-kB) or of antisense oligonucleotides or peptides that prevent NF-kBfrom accessing its site of action in the nucleus [4].
Inhibiting the kinases that induce phosphorylation blocks intra-cellular signal transduction. Thus, kinase inhibitors may holdpromise as treatments targeting intracellular signaling pathways.Several kinase inhibitors are already used in oncology.
3. Preliminary results of intracellular signaling pathwayinhibition used to treat rheumatoid arthritis
After preclinical studies in animal models, several randomizedcontrolled trials were conducted (Table 2) [10–14]. The resultsinvite several comments. First, follow-up was only 12 weeks, which
limits the relevance of the findings. Although the effect was rapidin some studies, being detectable after one week [13,14], longerfollow-ups are clearly needed to determine whether the thera-peutic effect is sustained over time (or whether the response rateincreases over time); to assess potential structural effects, whoselsevier Masson SAS. All rights reserved.
Editorial / Joint Bone Spin
Fig. 1. Highly simplified general diagram of intracellular signal transduction. Activa-tion of the membrane receptors (R1, R2) generates a signal, with cascade activationof several kinases (K1, K2, K3) that leads to activation of a transcription factor,thereby modifying target gene expression and ultimately leading to the synthesisof peptides (e.g., cytokines).
Table 1The main intracellular signaling pathways.
Signaling pathway Role
JAK-STAT (Janus Activated Kinase) Transmission of cytokine signals (IL-polarizationProduction of interferon
SYK (Spleen tYrosin Kinase) Expressed by B and T cells and macrImmunoreceptor signal transductionSynthesis of cytokines (IL-6) and MMOsteoclast differentiation
MAP kinases (p38, ERK, JNK) Cell proliferation, apoptosisProduction of TNF and of IL-1, IL-6, IResults in activation of the transcrip
NF-KB Production of cytokines, most notabcytokines (IL-1, IL-6, TNF-�), MMP, cmolecules, chemokines (RANTES)Activates genes involved in cell growapoptosis, oncogenesis, and negativeregulation
Phosphatidylinositol-3 protein kinase(PI3K)/AKT
Cell growth, inhibition of apoptosis,Adhesion, angiogenesis
Table 2The main controlled studies of signaling pathway inhibition in patients with rheumatoid
Author (ref) Target (agent) No. of patients Study design Duration(weeks)
Weisman etal. [10]
p38 MAPK(vx-745)
44 12
Damjanov etal. [11]
p38 MAPK(vx-702)
313 122 doses/d vs. placebo
1171 dose/d + MTX vs. 2doses/week + MTX (mean13.5 mg/week)
Cohen et al.[12]
p38 MAPK(pamapimod)
204 123 doses vs. MTX (up to20 mg/week at W8)
Kremer et al.[13]
JAK(CP-690,550)
264 63 doses vs. placebo
Weinblatt etal. [14]
Syk kinase(R 788)
189, active RA with MTX(mean 15 mg/week) 3 dosesvs. placebo
12
MTX: methotrexate; W: week; CRP: C-reactive protein; SAA: serum amyloid A; sTNFR p5
e 77 (2010) 96–98 97
presence is a defining characteristic of disease-modifying agents;and to evaluate the safety profile, particularly as these treatmentsare likely to be used for long periods (several years). Second, treat-ment efficacy varied across studies, being significant in about halfthe cases. This variability seems related to the target. Various MAP-kinase inhibitors produced ACR response rates that were eithernot significantly different from those in the placebo groups [11] orlower than those obtained using methotrexate [12]. Thus, despitepromising results from animal studies [15,16], proof of concept hasnot been obtained for inhibitors of the MAP kinases (most notablyp38). The lack of efficacy of MAP kinase inhibition illustrates thecomplexity of the signal transduction systems, whose redundancyensures the correction of many deficiencies. For instance, the pro-duction of proinflammatory cytokines such as TNF� depends bothon MAP kinase activation and on NF-kB [17,18]. Third, the results ofthe few trials conducted to date raise a number of safety concerns.Adverse events that were more common in the active-treatmentgroups than in the placebo groups included gastrointestinal symp-toms, headaches, neutropenia, and serum creatinine elevation.
Treatments that interfere with intracellular signaling also affectthe physiological regulation mechanisms of many cell types. Theobjective in RA is to modulate a complex set of systems (inflamma-tion, cytokines, and proteases); whereas the objective in oncologyActivated by
6, IL-23), Th17 gp 130 (IL-6, IFN gamma)
ophages Fcgamma receptor
P induced by TNF
Mitogenic factors and growth factors (ERK),cytokines, and cell stress factors (JNK, p38)L-8
tion factor AP-1
ly proinflammatoryollagenases, adhesion
Cytokines, bacterial and viral proteins, UV
th, inhibition ofNF-kB (IkB)
oncogenesis Activated by growth factors, cytokines, hormones,viral proteins, co-stimulation of T-cells
arthritis.
ACR 20response rate
Other results Safety
43% active 14/44 withdrawals for lack of efficacy orintolerance (gastrointestinal symptoms)17% placebo
40–36% active Decreases inCRP, SAA, andsTNFR p55 atW1, return tobaselinelevels at W4
Serious infections28% placebo(NS)
2.4% vs. 0%
40–44% active 2.% vs. 4.9%22% placebo(NS)
23%, 18%, 31%45% (MTX)
70%, 81%, 76%,29% placebo
Headaches, nauseaElevations in serum creatinine and HDL
38%, 65%, 72%,32% placebo
Decrease inIL-6
Diarrhea, hypertension
MMP-3 Neutropenia, hepatic cytolysis
5: soluble tumor necrosis factor receptor p55.

9 e Spin
ilcFpmTb
pimaa
utabest
C
R
[
[
[
[
[
[
[
[
[
[
8 Editorial / Joint Bon
s to limit the growth of, or to destroy, a cell population. Theong-term safety requirements are more stringent in patients withhronic and generally non-life-threatening diseases such as RA.urthermore, prolonged signaling pathway inhibition may inducearadoxical effects. For instance, inhibition of NF-kB activationay exacerbate the inflammatory process by allowing uncontrolled
NF production by macrophages [3]. Beware of opening Pandora’sox.
Signaling pathway inhibitors exhibit a number of favorableroperties that are generating considerable interest. Most of these
nhibitors are small biochemical compounds that can cross the cellembrane. Compared to biotherapies, they cost less to produce
nd are less likely to induce immunization. Finally, they can bedministered orally.
Signaling pathways are diverse and induce reaction cascadespon activation. As a result, the number of potential treatmentargets is high, and many different inhibition modalities may bevailable, including local treatments [19]. We are witnessing theirth of a new class of potential treatments. However, extensivevaluation and validation studies are needed to determine whetherignal pathway inhibition deserves consideration as a treatmentool for everyday clinical practice.
onflict of interest statement
The authors have no conflict of interest to declare.
eferences
[1] Morel J, Berenbaum F. Signal transduction pathways: new targets for treatingrheumatoid arthritis. Joint Bone Spine 2004;71:503–10.
[2] Sweeney SE, Firestein GS. Signal transduction in rheumatoid arthritis. Curr OpinRheumatol 2004;16:231–7.
[3] Simmonds RE, Foxwell BM. NF-kB and its relevance to arthritis and inflamma-tion. Rheumatology 2008;47:584–90.
[4] Roman-Blas JA, Jimenez SA. NF-kB as a potential therapeutic tar-get in osteoarthritis and rheumatoid arthritis. Osteoarthritis Cartilage2006;14:839–48.
[5] Schett G, Zwerina J, Firestein G. The p38 mitogen-activated proteinkinase (MAPK) pathway in rheumatoid arthritis. Ann Rheum Dis 2008;67:909–16.
[6] O’Shea JJ, Murray PJ. Cytokine signaling modules in inflammatory responses.Immunity 2008;28:477–87.
[7] Berton G, Mocsai A, Lowell CA. Src and Syk kinases: key regulators of phagocyticcell activation. Trends Immunol 2005;26:208–14.
[8] Dichamp I, Bourgeois A, Dirand C, et al. Increased nuclear factor-kB acti-
vation in peripheral blood monocytes of patients with rheumatoid arthritisis mediated primarily by tumor necrosis factor-�. J Rheumatol 2007;34:1976–83.[9] Clohisy JC, Roy BC, Biondo C, et al. Direct inhibition of NF-kB blocksbone erosion associated with inflammatory arthritis. J Immunol 2003;171:5547–53.
e 77 (2010) 96–98
10] Weisman M, Furst D, Schiff M, et al. A double-blind, placebo-controlled trialof VX-745, an oral p38 mitogen-activated protein kinase (MAPK) inhibitor inpatients with rheumatoid arthritis. Ann Rheum Dis 2002;61:166.
11] Damjanov N, Kauffman RS, Spencer-Green GT. Efficacy, pharmacodynamics,and safety of VX-702, a novel p38 MAPK inhibitor, in rheumatoid arthritisResults of two randomized, double-blind, placebo-controlled clinical studies.Arthritis Rheum 2009;60:1232–41.
12] Cohen SB, Cheng TT, Chindalore V, et al. Evaluation of the efficacy and safetyof pamapimod, a p38 MAP kinase inhibitor, in a double-blind, methotrexate-controlled study of patients with active rheumatoid arthritis. Arthritis Rheum2009;60:335–44.
13] Kremer J, Bloom BJ, Breedveld FC, et al. The safety and efficacy of a JAK inhibitorin patients with active rheumatoid arthritis. Results of a double-blind, placebo-controlled phase IIa trial of three dosage levels of CP-690,550 versus placebo.Arthritis Rheum 2009;60:1895–905.
14] Weinblatt ME, Kavanaugh A, Burgos-Vargas R, et al. Treatment of rheumatoidarthritis with a Syk kinase inhibitor. A twelve-week, randomized, placebo-controlled trial. Arthritis Rheum 2008;58:3309–18.
15] Kaminska B. MAPK signaling pathways as molecular targets for anti-inflammatory therapy. From molecular mechanisms to therapeutic benefits.Biochim Biophys Acta 2005;1754:253–62.
16] Sweeney SE, Firestein GS. Mitogen activated protein kinase inhibitors: whereare we now and where are we going? Ann Rheum Dis 2006;65(Suppl. 3):83–8[iii].
17] Mahlknecht U, Will J, Varin A, et al. Histone deacetylase 3, a class I histonedeacetylase, suppresses MAPK11-mediated activating transcription factor-2activation and represses TNF gene expression. J Immunol 2004;173:3979–90.
18] Vallabhapurapu S, Karin M. Regulation and function of NF-kappaB transcriptionfactors in the immune system. Annu Rev Immunol 2009;27:693–733.
19] Tas SW, Vervoordeldonk MJ, Hajji N, et al. Local treatment with the selectiveIkB kinase � inhibitor NEMO-binding domain peptide ameliorates synovialinflammation. Arthritis Res Ther 2006;8:R86.
Daniel Wendling a,∗
Clément Prati b
Éric Toussirot c
Georges Herbein d
a EA 3186, Service de Rhumatologie, CHU Minjoz,Université de Franche-Comté, Boulevard Fleming,
25030 Besancon, Franceb Service de Rhumatologie, CHU Minjoz, Université de
Franche-Comté, Besancon, Francec EA 3186, Service de Rhumatologie, CHU Minjoz,
Université de Franche-Comté, Besancon, Franced EA 3186, Service de Virologie, CHU, Université de
Franche-Comté, Besancon, France
∗ Corresponding author.E-mail address: [email protected]
(D. Wendling).
13 October 2009
Available online19 February 2010












![Employer Branding Journey: Pandora's Story [webcast]](https://img.pdfslide.us/doc/110x75/58f32ff71a28ab6d4a8b4587/employer-branding-journey-pandoras-story-webcast.jpg)















