Embed Size (px)
Citation preview
Targeting Inflammation in Atherosclerosis:
Has CANTOS Nailed It? Controversies and Advances in the
Treatment of Cardiovascular Disease
The Seventeenth in the Series
Beverly Hills, November 16, 2017
Sanjay Kaul, MD, FACC, FAHA Division of Cardiology
Cedars-Sinai Medical Center
Los Angeles, California
The Laws of Diminishing Objectivity
in the Interpretation of Evidence
vehemence a evidence-1
Peter McCulloch
The Lancet, 2004;363;9004
vehemence a eminence2
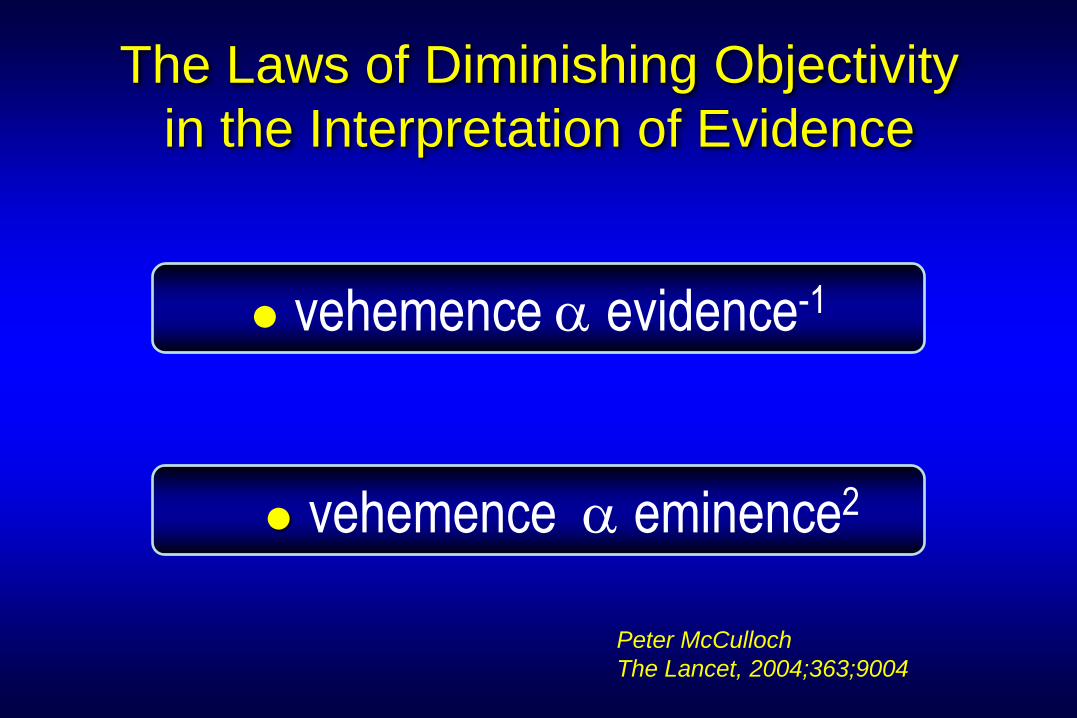
Libby P. JACC (October 31, 2017)
Interleukin-1b as a Target for Atherosclerosis
Biologic Basis for CANTOS and Beyond
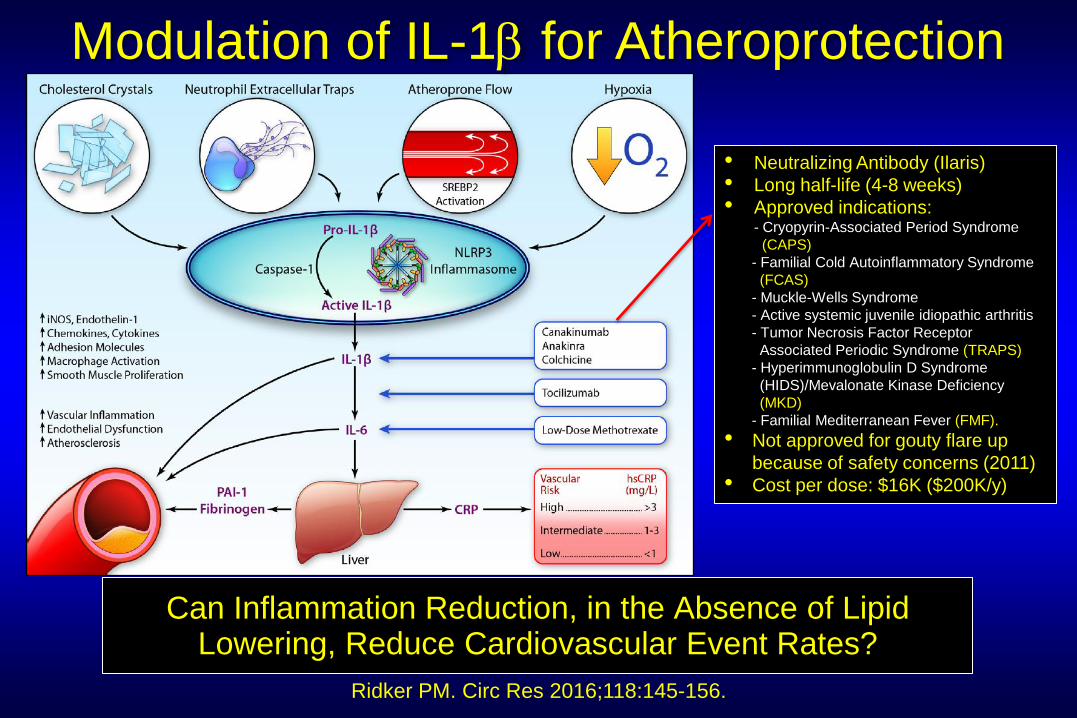
Ridker PM. Circ Res 2016;118:145-156.
Modulation of IL-1b for Atheroprotection
Can Inflammation Reduction, in the Absence of Lipid Lowering, Reduce Cardiovascular Event Rates?
• Neutralizing Antibody (Ilaris)
• Long half-life (4-8 weeks)
• Approved indications: - Cryopyrin-Associated Period Syndrome
(CAPS)
- Familial Cold Autoinflammatory Syndrome
(FCAS)
- Muckle-Wells Syndrome
- Active systemic juvenile idiopathic arthritis
- Tumor Necrosis Factor Receptor
Associated Periodic Syndrome (TRAPS)
- Hyperimmunoglobulin D Syndrome
(HIDS)/Mevalonate Kinase Deficiency
(MKD)
- Familial Mediterranean Fever (FMF).
• Not approved for gouty flare up
because of safety concerns (2011)
• Cost per dose: $16K ($200K/y)
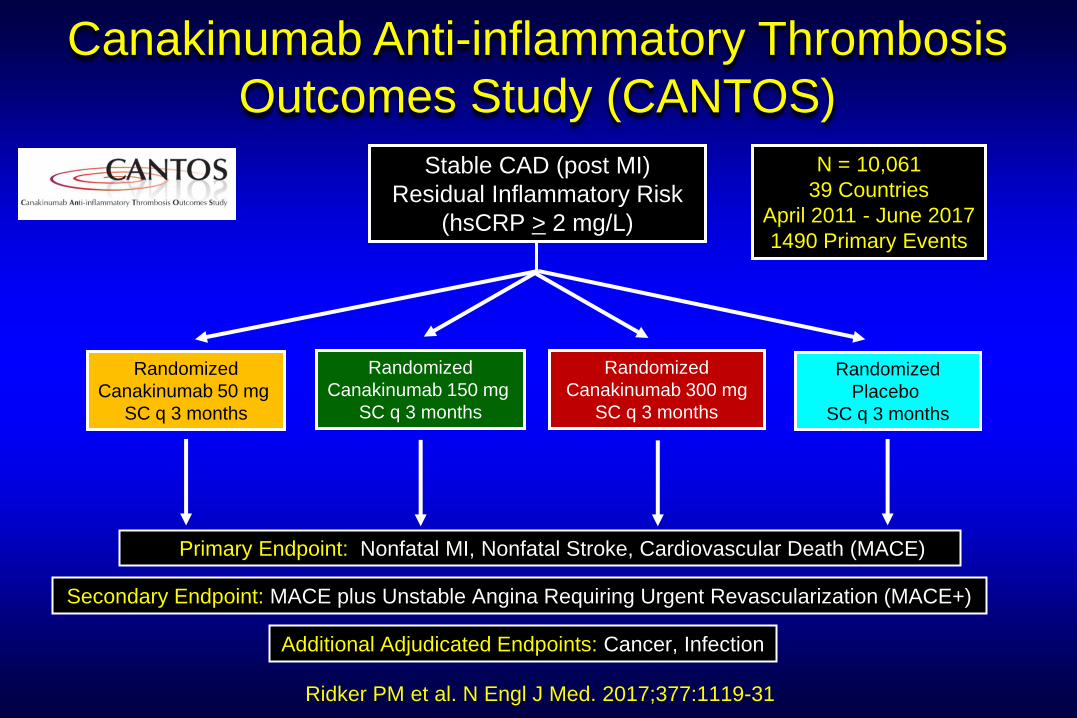
Canakinumab Anti-inflammatory Thrombosis
Outcomes Study (CANTOS)
Randomized
Canakinumab 150 mg
SC q 3 months
Randomized
Placebo
SC q 3 months
Primary Endpoint: Nonfatal MI, Nonfatal Stroke, Cardiovascular Death (MACE)
Randomized
Canakinumab 300 mg
SC q 3 months
Secondary Endpoint: MACE plus Unstable Angina Requiring Urgent Revascularization (MACE+)
Additional Adjudicated Endpoints: Cancer, Infection
Randomized
Canakinumab 50 mg
SC q 3 months
N = 10,061
39 Countries
April 2011 - June 2017
1490 Primary Events
Ridker PM et al. N Engl J Med. 2017;377:1119-31
Stable CAD (post MI)
Residual Inflammatory Risk
(hsCRP > 2 mg/L)
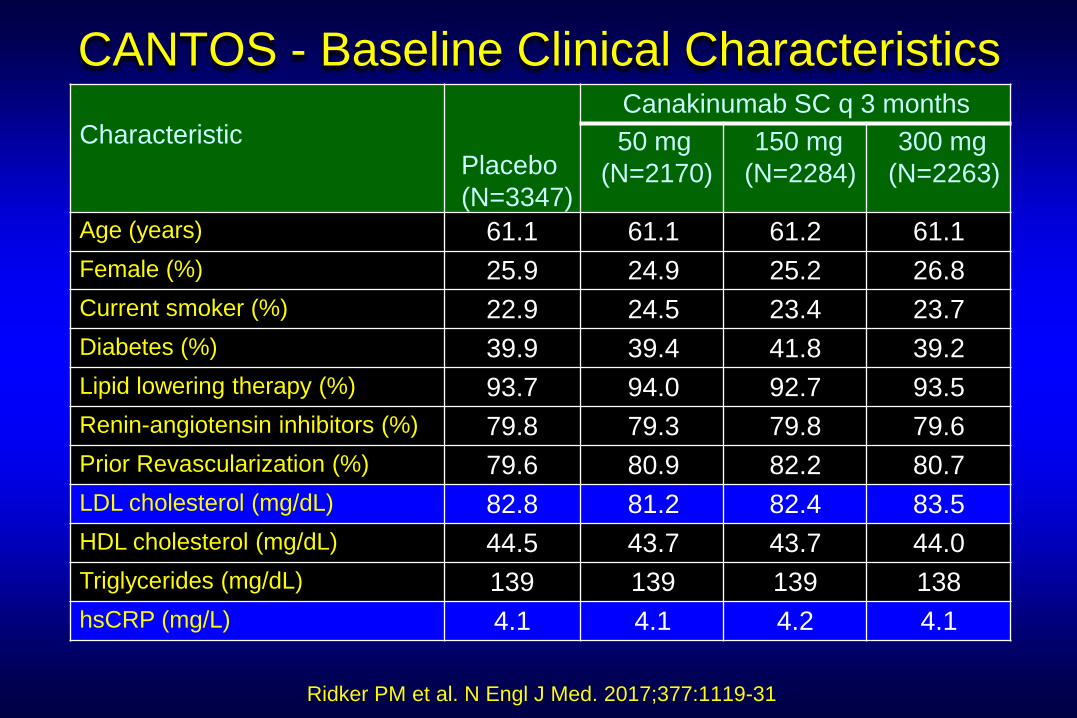
Characteristic
Placebo
(N=3347)
Canakinumab SC q 3 months
50 mg
(N=2170)
150 mg
(N=2284)
300 mg
(N=2263)
Age (years) 61.1 61.1 61.2 61.1
Female (%) 25.9 24.9 25.2 26.8
Current smoker (%) 22.9 24.5 23.4 23.7
Diabetes (%) 39.9 39.4 41.8 39.2
Lipid lowering therapy (%) 93.7 94.0 92.7 93.5
Renin-angiotensin inhibitors (%) 79.8 79.3 79.8 79.6
Prior Revascularization (%) 79.6 80.9 82.2 80.7
LDL cholesterol (mg/dL) 82.8 81.2 82.4 83.5
HDL cholesterol (mg/dL) 44.5 43.7 43.7 44.0
Triglycerides (mg/dL) 139 139 139 138
hsCRP (mg/L) 4.1 4.1 4.2 4.1
CANTOS - Baseline Clinical Characteristics
Ridker PM et al. N Engl J Med. 2017;377:1119-31
10
0
10
20
30
40
50
60
70
Pe
rcent C
ha
nge fro
m B
ase
line (
me
dia
n)
hs
CR
P
LD
LC
H
DL
C
TG
0 3 6 12 24 36 48
10
0
-10
10
0
-10
10
0
-10
Placebo Canakinumab 50 Canakinumab 150 Canakinumab 300
9
Months
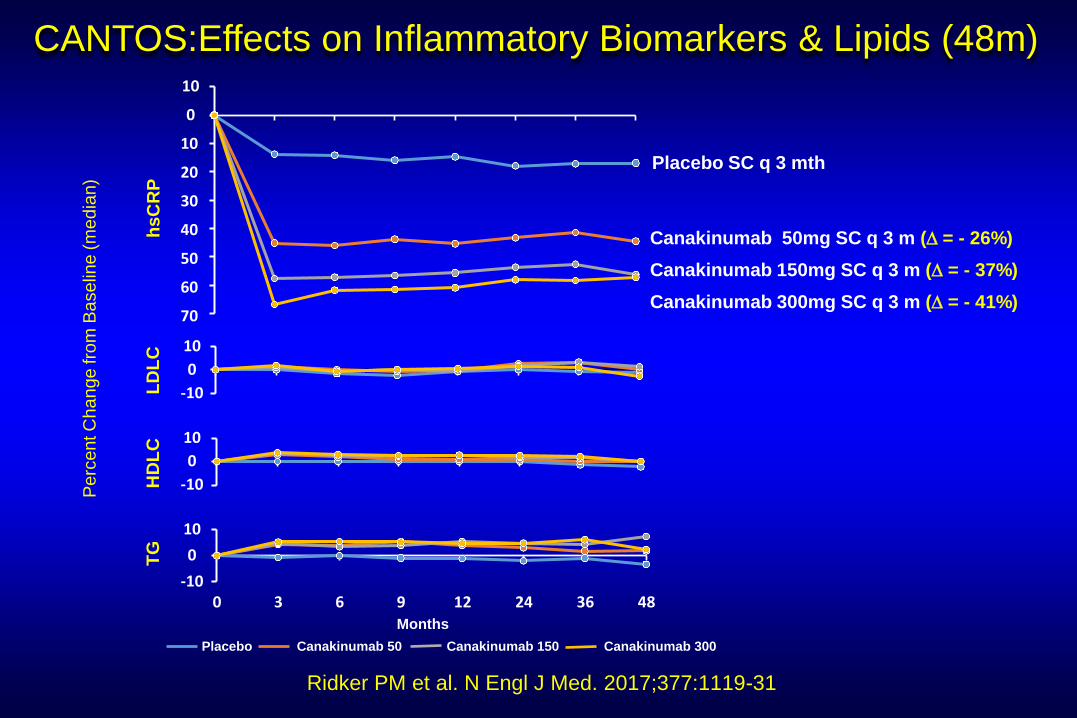
Placebo SC q 3 mth
Canakinumab 50mg SC q 3 m (D = - 26%)
Canakinumab 150mg SC q 3 m (D = - 37%)
Canakinumab 300mg SC q 3 m (D = - 41%)
CANTOS:Effects on Inflammatory Biomarkers & Lipids (48m)
Ridker PM et al. N Engl J Med. 2017;377:1119-31
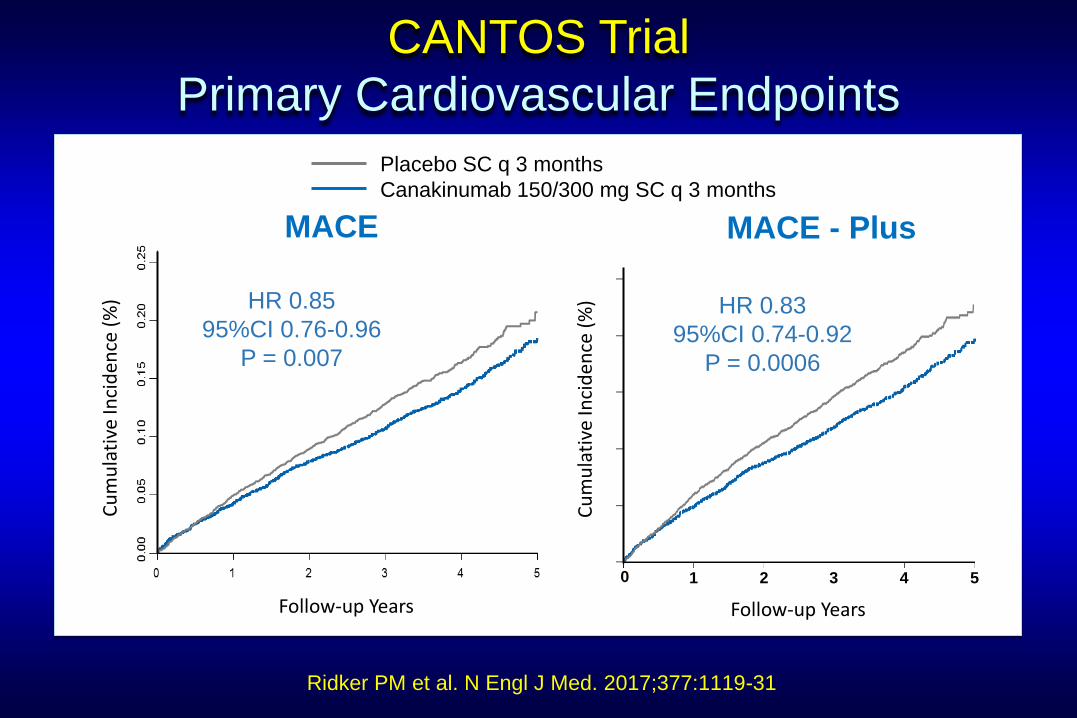
CANTOS Trial
Primary Cardiovascular Endpoints
Ridker PM et al. N Engl J Med. 2017;377:1119-31
HR 0.85
95%CI 0.76-0.96
P = 0.007
Cu
mu
lati
ve In
cid
ence
(%
)
Follow-up Years
HR 0.83
95%CI 0.74-0.92
P = 0.0006
MACE MACE - Plus
Follow-up Years
0 1 2 3 4 5 C
um
ula
tive
Inci
den
ce (
%) HR 0.83
95%CI 0.74-0.92
P = 0.0006
Placebo SC q 3 months
Canakinumab 150/300 mg SC q 3 months
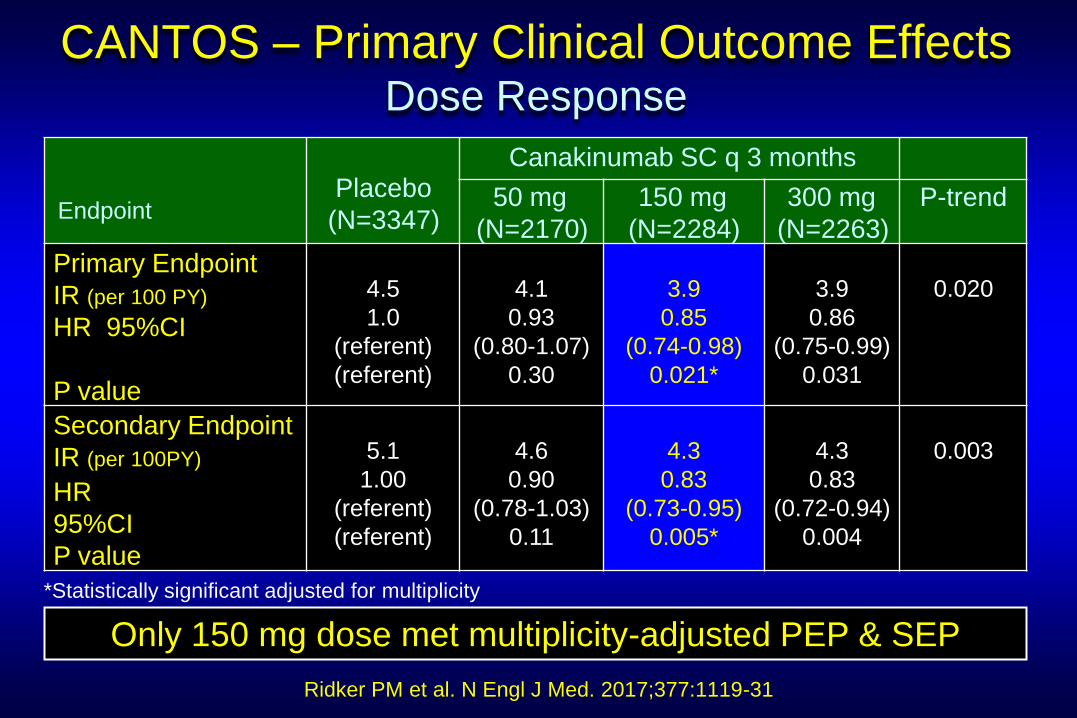
CANTOS – Primary Clinical Outcome Effects Dose Response
Ridker PM et al. N Engl J Med. 2017;377:1119-31
Endpoint
Placebo
(N=3347)
Canakinumab SC q 3 months
50 mg
(N=2170)
150 mg
(N=2284)
300 mg
(N=2263)
P-trend
Primary Endpoint
IR (per 100 PY)
HR 95%CI
P value
4.5
1.0
(referent)
(referent)
4.1
0.93
(0.80-1.07)
0.30
3.9
0.85
(0.74-0.98)
0.021*
3.9
0.86
(0.75-0.99)
0.031
0.020
Secondary Endpoint
IR (per 100PY)
HR
95%CI
P value
5.1
1.00
(referent)
(referent)
4.6
0.90
(0.78-1.03)
0.11
4.3
0.83
(0.73-0.95)
0.005*
4.3
0.83
(0.72-0.94)
0.004
0.003
*Statistically significant adjusted for multiplicity
Only 150 mg dose met multiplicity-adjusted PEP & SEP
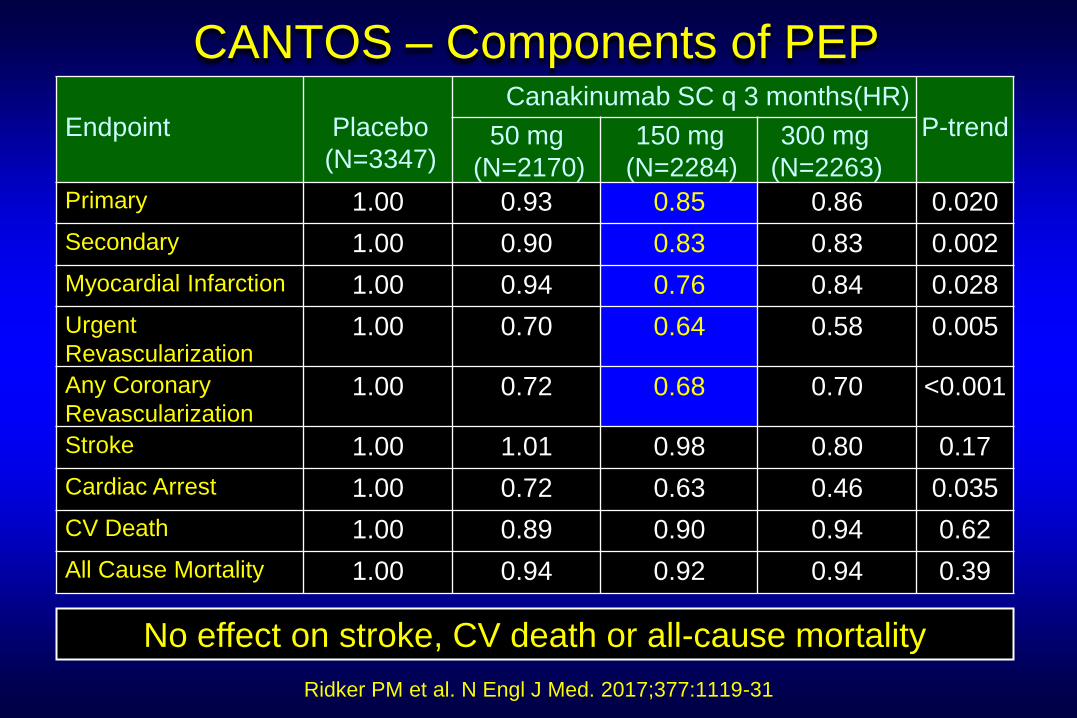
CANTOS – Components of PEP
Ridker PM et al. N Engl J Med. 2017;377:1119-31
Endpoint
Placebo
(N=3347)
Canakinumab SC q 3 months(HR)
P-trend 50 mg
(N=2170)
150 mg
(N=2284)
300 mg
(N=2263)
Primary 1.00 0.93 0.85 0.86 0.020
Secondary 1.00 0.90 0.83 0.83 0.002
Myocardial Infarction 1.00 0.94 0.76 0.84 0.028
Urgent
Revascularization 1.00 0.70 0.64 0.58 0.005
Any Coronary
Revascularization 1.00 0.72 0.68 0.70 <0.001
Stroke 1.00 1.01 0.98 0.80 0.17
Cardiac Arrest 1.00 0.72 0.63 0.46 0.035
CV Death 1.00 0.89 0.90 0.94 0.62
All Cause Mortality 1.00 0.94 0.92 0.94 0.39
No effect on stroke, CV death or all-cause mortality
Ridker PM et al. N Engl J Med. 2017;377:1119-31
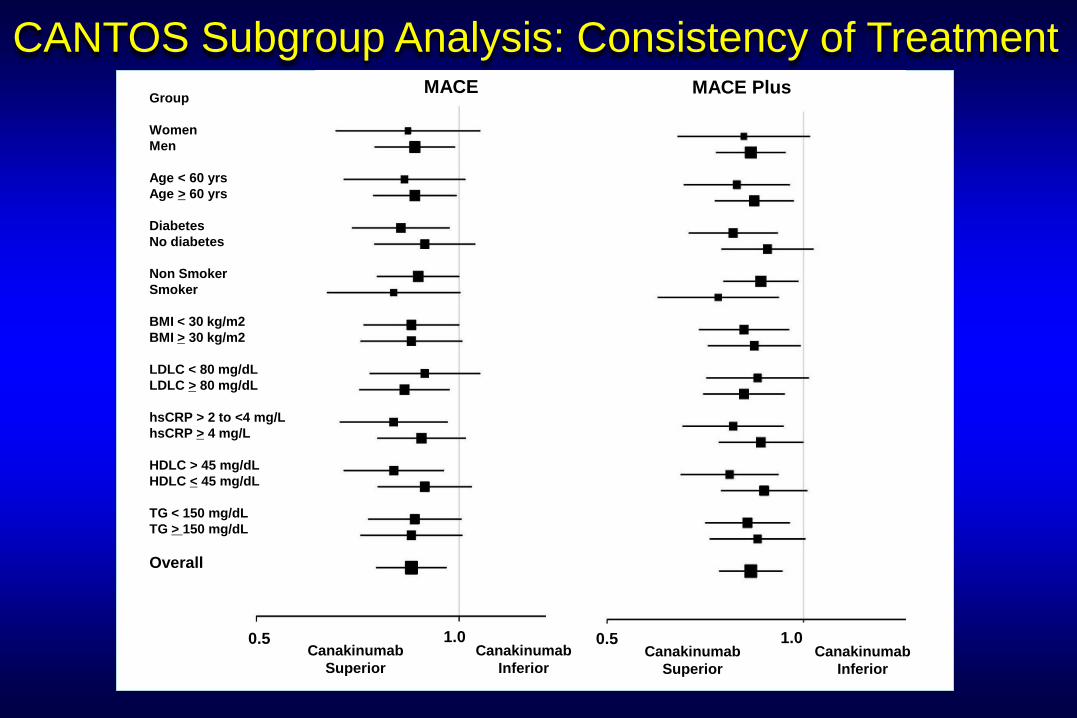
0.5 Canakinumab
Superior
Canakinumab
Inferior
0.5 Canakinumab
Superior
Canakinumab
Inferior
1.0
Group
Women
Men
Age < 60 yrs
Age > 60 yrs
Diabetes
No diabetes
Non Smoker
Smoker
BMI < 30 kg/m2
BMI > 30 kg/m2
LDLC < 80 mg/dL
LDLC > 80 mg/dL
hsCRP > 2 to <4 mg/L
hsCRP > 4 mg/L
HDLC > 45 mg/dL
HDLC < 45 mg/dL
TG < 150 mg/dL
TG > 150 mg/dL
Overall
MACE MACE Plus
1.0
CANTOS Subgroup Analysis: Consistency of Treatment
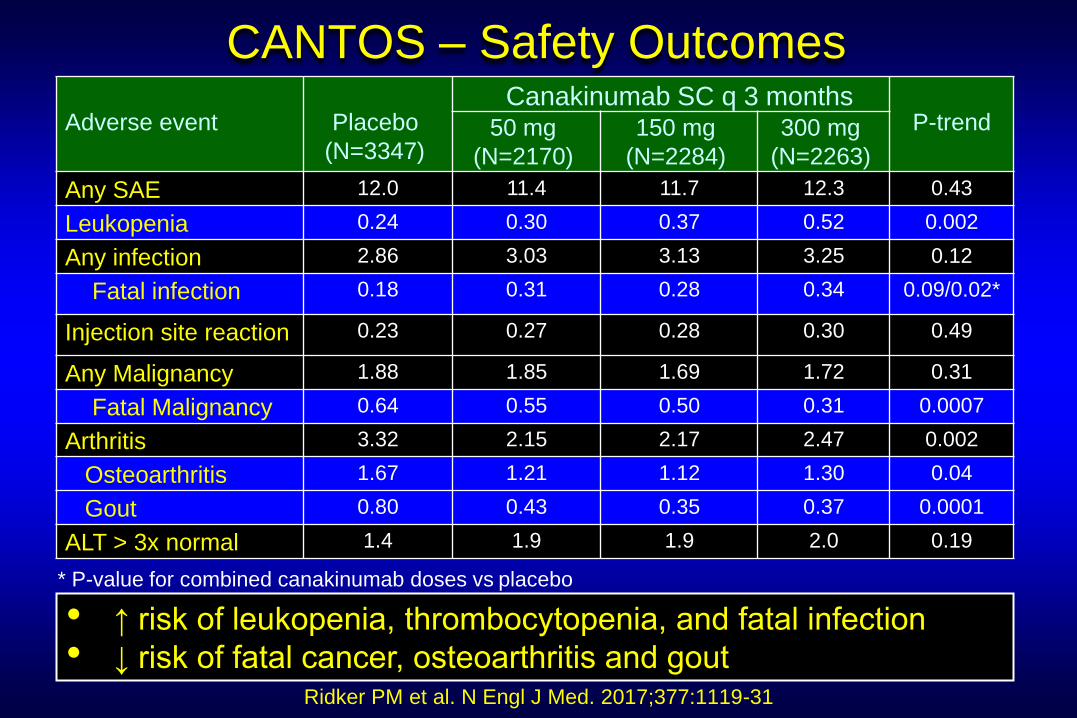
CANTOS – Safety Outcomes
Ridker PM et al. N Engl J Med. 2017;377:1119-31
Adverse event
Placebo
(N=3347)
Canakinumab SC q 3 months
P-trend 50 mg
(N=2170)
150 mg
(N=2284)
300 mg
(N=2263)
Any SAE 12.0 11.4 11.7 12.3 0.43
Leukopenia 0.24 0.30 0.37 0.52 0.002
Any infection 2.86 3.03 3.13 3.25 0.12
Fatal infection 0.18 0.31 0.28 0.34 0.09/0.02*
Injection site reaction 0.23 0.27 0.28 0.30 0.49
Any Malignancy 1.88 1.85 1.69 1.72 0.31
Fatal Malignancy 0.64 0.55 0.50 0.31 0.0007
Arthritis 3.32 2.15 2.17 2.47 0.002
Osteoarthritis 1.67 1.21 1.12 1.30 0.04
Gout 0.80 0.43 0.35 0.37 0.0001
ALT > 3x normal 1.4 1.9 1.9 2.0 0.19
• ↑ risk of leukopenia, thrombocytopenia, and fatal infection
• ↓ risk of fatal cancer, osteoarthritis and gout
* P-value for combined canakinumab doses vs placebo
• Benefit-risk balance of Canakinumab
• Robustness of outcomes
• Lack of low or normal hsCRP group
• Totality of evidence
• Implications
Evaluation of CANTOS Trial
Deep Dive
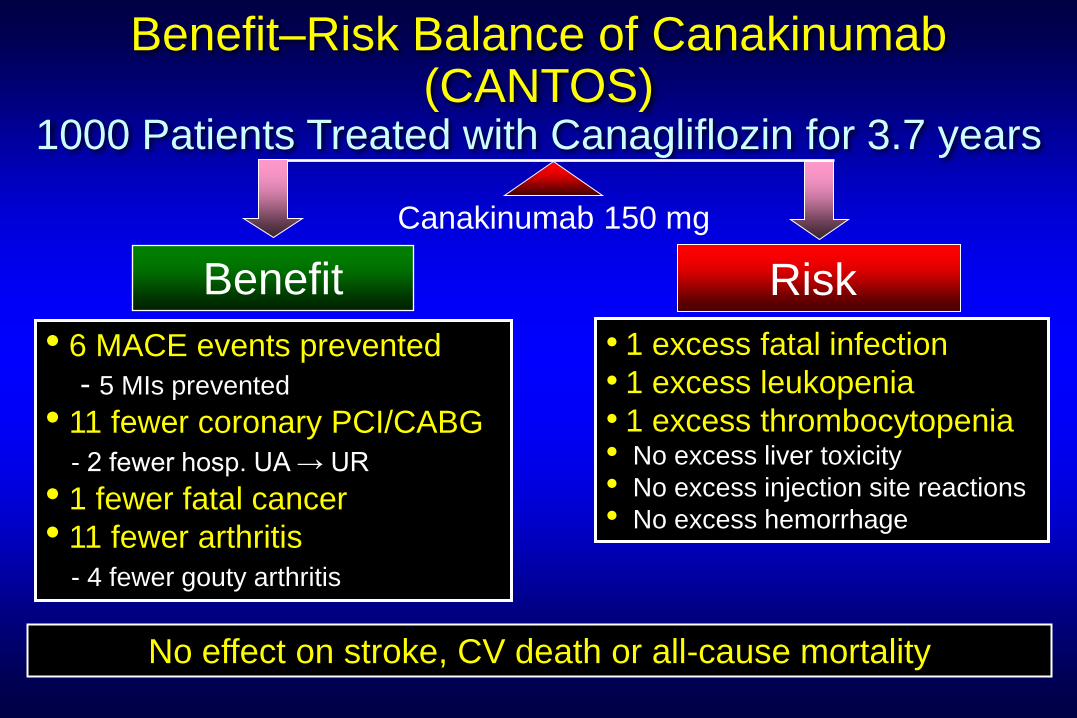
Benefit–Risk Balance of Canakinumab (CANTOS)
1000 Patients Treated with Canagliflozin for 3.7 years
Benefit Risk
Canakinumab 150 mg
• 6 MACE events prevented
- 5 MIs prevented
• 11 fewer coronary PCI/CABG
- 2 fewer hosp. UA → UR
• 1 fewer fatal cancer
• 11 fewer arthritis
- 4 fewer gouty arthritis
• 1 excess fatal infection
• 1 excess leukopenia
• 1 excess thrombocytopenia • No excess liver toxicity
• No excess injection site reactions
• No excess hemorrhage
No effect on stroke, CV death or all-cause mortality
• Benefit-risk balance of Canakinumab
• Robustness of outcomes
• Lack of low or normal hsCRP group
• Totality of evidence
• Implications
Evaluation of CANTOS Trial
Deep Dive
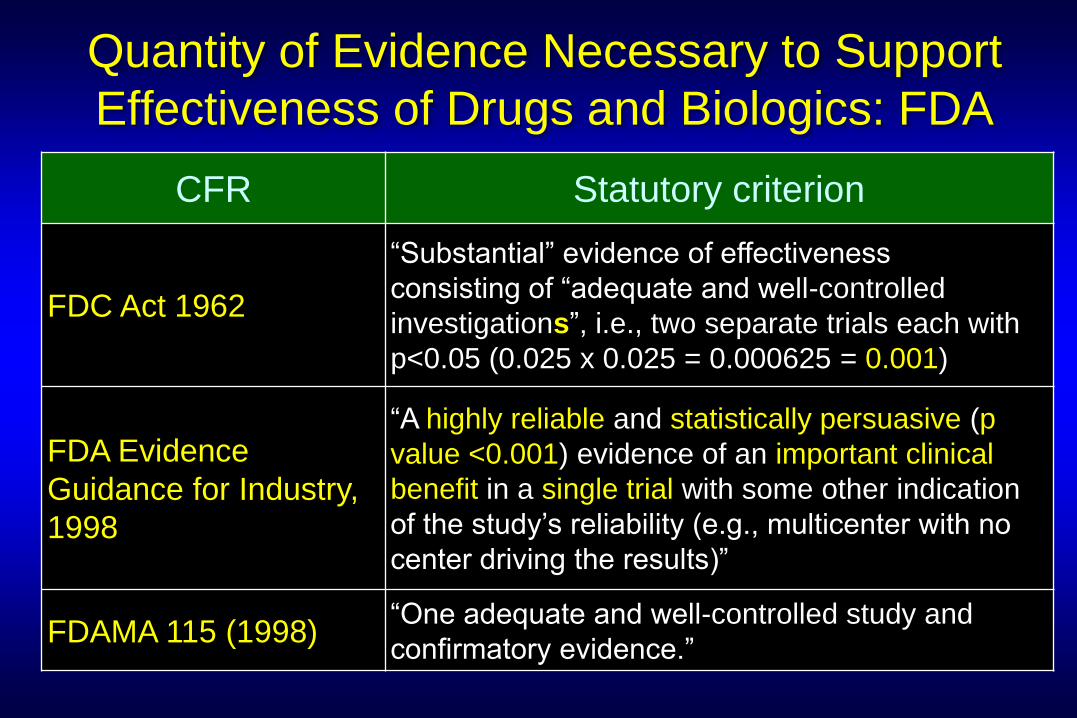
Quantity of Evidence Necessary to Support
Effectiveness of Drugs and Biologics: FDA
CFR Statutory criterion
FDC Act 1962
“Substantial” evidence of effectiveness
consisting of “adequate and well-controlled
investigations”, i.e., two separate trials each with
p<0.05 (0.025 x 0.025 = 0.000625 = 0.001)
FDA Evidence
Guidance for Industry,
1998
“A highly reliable and statistically persuasive (p
value <0.001) evidence of an important clinical
benefit in a single trial with some other indication
of the study’s reliability (e.g., multicenter with no
center driving the results)”
FDAMA 115 (1998) “One adequate and well-controlled study and
confirmatory evidence.”
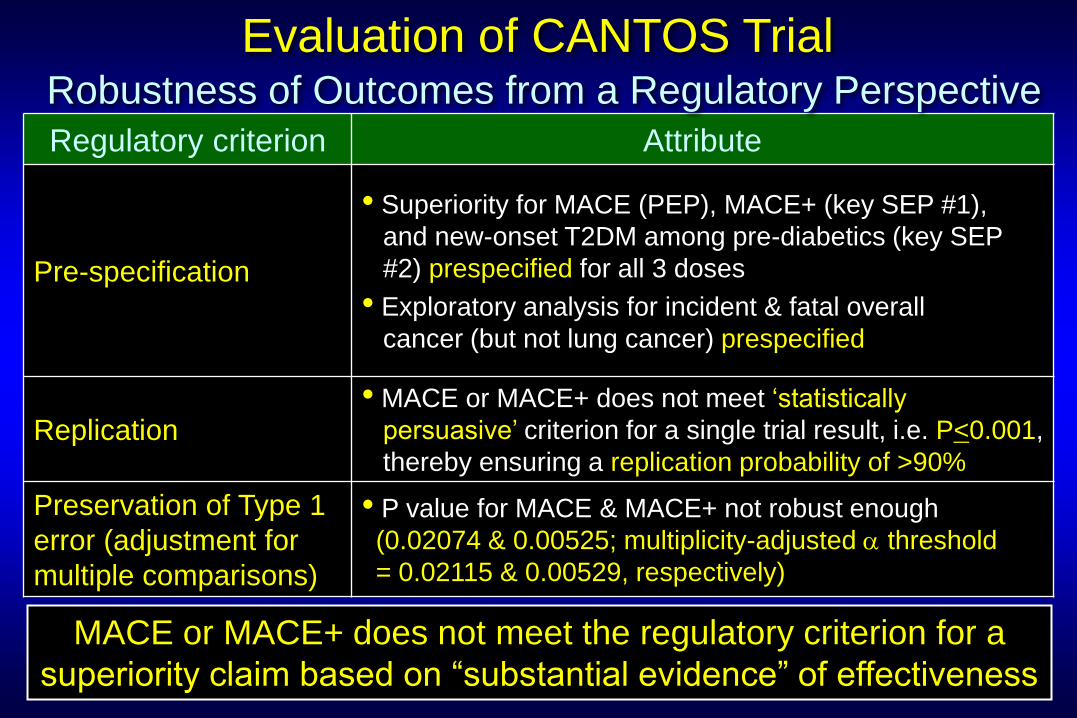
Regulatory criterion Attribute
Pre-specification
• Superiority for MACE (PEP), MACE+ (key SEP #1),
and new-onset T2DM among pre-diabetics (key SEP
#2) prespecified for all 3 doses
• Exploratory analysis for incident & fatal overall
cancer (but not lung cancer) prespecified
Replication • MACE or MACE+ does not meet ‘statistically
persuasive’ criterion for a single trial result, i.e. P<0.001,
thereby ensuring a replication probability of >90%
Preservation of Type 1
error (adjustment for
multiple comparisons)
• P value for MACE & MACE+ not robust enough
(0.02074 & 0.00525; multiplicity-adjusted a threshold
= 0.02115 & 0.00529, respectively)
Evaluation of CANTOS Trial
Robustness of Outcomes from a Regulatory Perspective
MACE or MACE+ does not meet the regulatory criterion for a
superiority claim based on “substantial evidence” of effectiveness
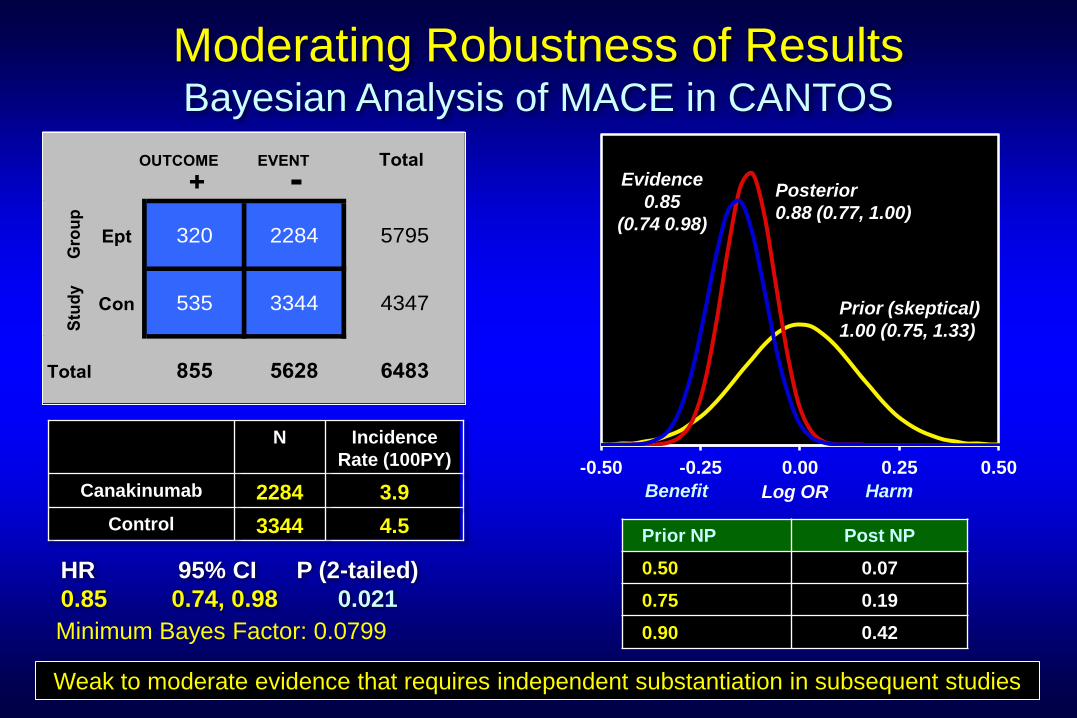
-0.50 -0.25 0.00 0.25 0.50
Moderating Robustness of Results Bayesian Analysis of MACE in CANTOS
Prior NP Post NP
0.50 0.07
0.75 0.19
0.90 0.42
HR 95% CI P (2-tailed)
0.85 0.74, 0.98 0.021
4.5
3.9
Incidence
Rate (100PY)
3344
2284
N
Control
Canakinumab
OUTCOME EVENT Total
+ -
Group
Ept 320 2284 5795
Study
Con 535 3344 4347
Total 855 5628 6483
Harm Benefit Log OR
Prior (skeptical)
1.00 (0.75, 1.33)
Evidence
0.85
(0.74 0.98)
Posterior
0.88 (0.77, 1.00)
Minimum Bayes Factor: 0.0799
Weak to moderate evidence that requires independent substantiation in subsequent studies
• Benefit-risk balance of Canakinumab
• Robustness of outcomes
• Lack of low or normal hsCRP arm
• Totality of evidence
• Implications
Evaluation of CANTOS Trial
Deep Dive
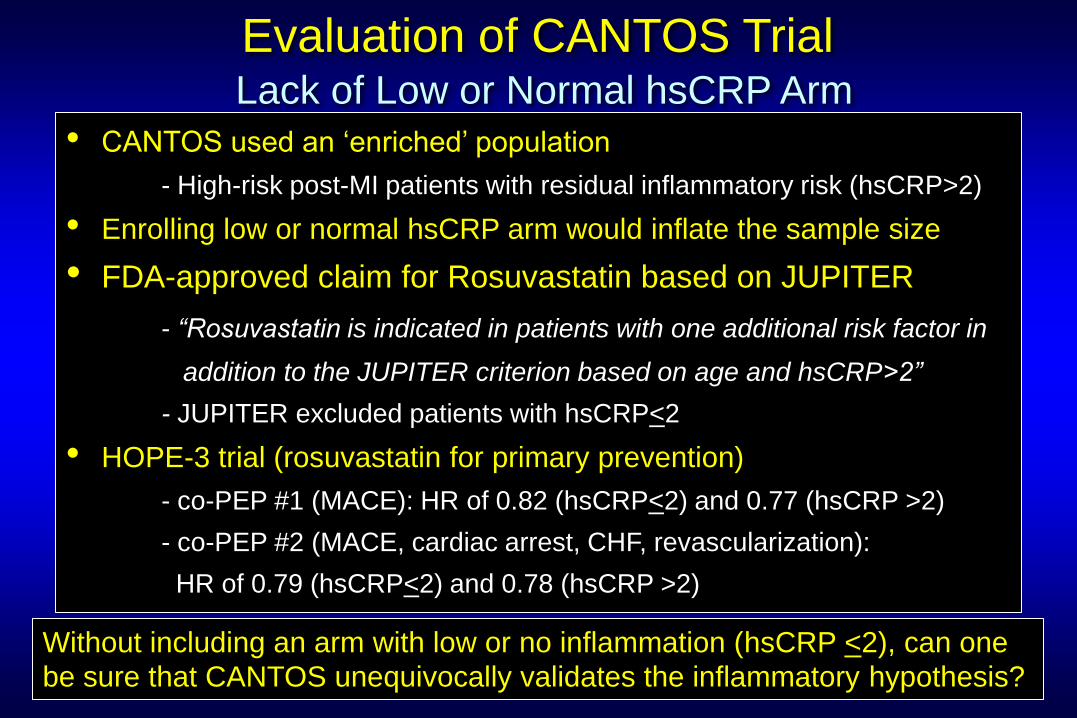
• CANTOS used an ‘enriched’ population
- High-risk post-MI patients with residual inflammatory risk (hsCRP>2)
• Enrolling low or normal hsCRP arm would inflate the sample size
• FDA-approved claim for Rosuvastatin based on JUPITER
- “Rosuvastatin is indicated in patients with one additional risk factor in
addition to the JUPITER criterion based on age and hsCRP>2”
- JUPITER excluded patients with hsCRP<2
• HOPE-3 trial (rosuvastatin for primary prevention)
- co-PEP #1 (MACE): HR of 0.82 (hsCRP<2) and 0.77 (hsCRP >2)
- co-PEP #2 (MACE, cardiac arrest, CHF, revascularization):
HR of 0.79 (hsCRP<2) and 0.78 (hsCRP >2)
Evaluation of CANTOS Trial
Lack of Low or Normal hsCRP Arm
Without including an arm with low or no inflammation (hsCRP <2), can one
be sure that CANTOS unequivocally validates the inflammatory hypothesis?
• Benefit-risk balance of Canakinumab
• Robustness of outcomes
• Lack of low or normal hsCRP group
• Totality of evidence
• Implications
Evaluation of CANTOS Trial
Deep Dive
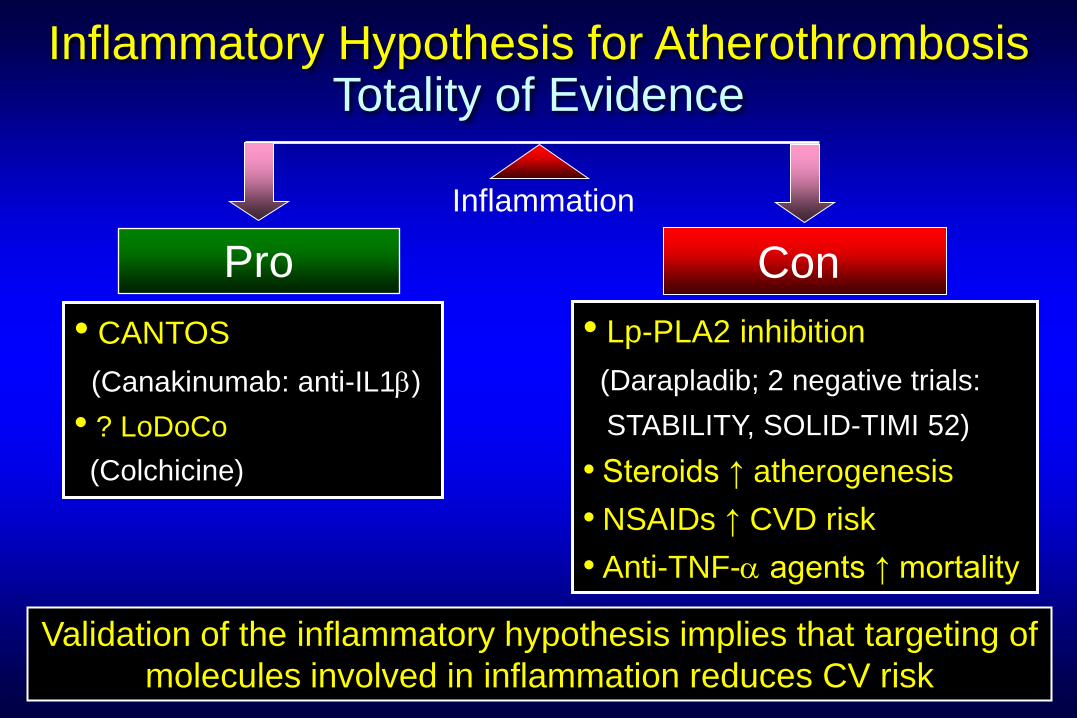
Inflammatory Hypothesis for Atherothrombosis Totality of Evidence
Pro Con
Inflammation
• CANTOS
(Canakinumab: anti-IL1b)
• ? LoDoCo
(Colchicine)
• Lp-PLA2 inhibition
(Darapladib; 2 negative trials:
STABILITY, SOLID-TIMI 52)
• Steroids ↑ atherogenesis
• NSAIDs ↑ CVD risk
• Anti-TNF-a agents ↑ mortality
Validation of the inflammatory hypothesis implies that targeting of
molecules involved in inflammation reduces CV risk
• Benefit-risk balance of Canakinumab
• Robustness of outcomes
• Lack of low or normal hsCRP group
• Totality of evidence
• Implications
Evaluation of CANTOS Trial
Deep Dive
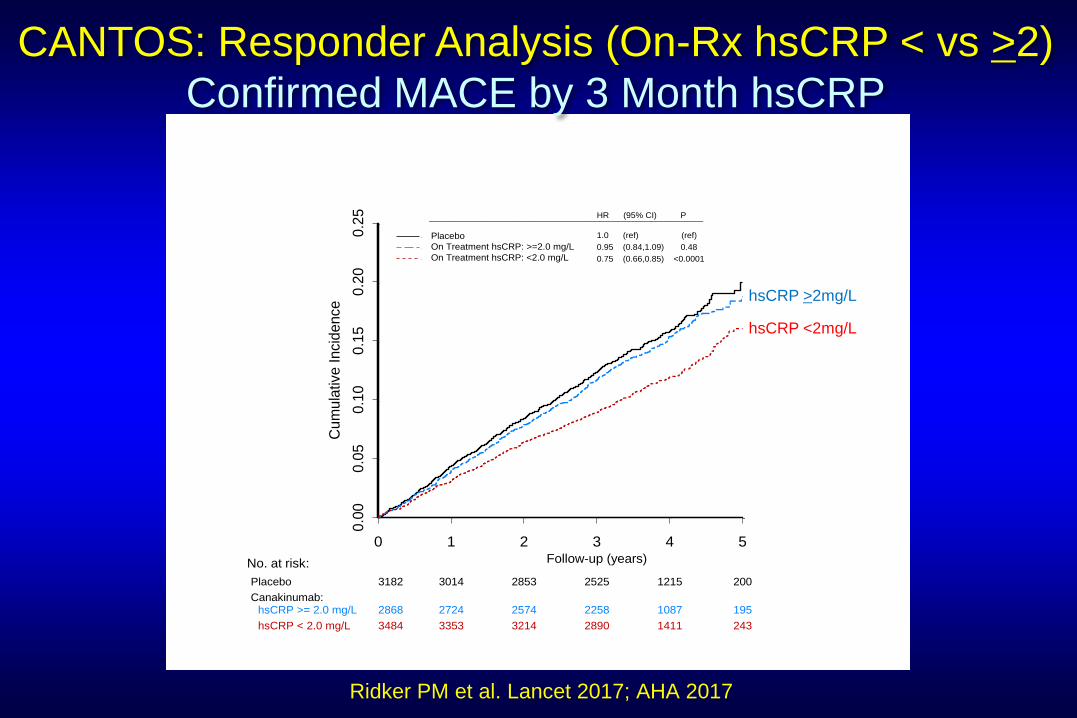
0 1 2 3 4 5
0.0
00.0
50.1
00.1
50.2
00.2
5
Cu
mu
lative
Incid
ence
Placebo
On Treatment hsCRP: >=2.0 mg/L
On Treatment hsCRP: <2.0 mg/L
Confirmed MACE by 3 Month hsCRP
HR (95% CI) P__________________________________________________________
1.0 (ref) (ref)
0.95 (0.84,1.09) 0.48
0.75 (0.66,0.85) <0.0001
Follow-up (years)No. at risk:
Placebo 3182 3014 2853 2525 1215 200
Canakinumab:hsCRP >= 2.0 mg/L 2868 2724 2574 2258 1087 195
hsCRP < 2.0 mg/L 3484 3353 3214 2890 1411 243
CANTOS: Responder Analysis (On-Rx hsCRP < vs >2)
Confirmed MACE by 3 Month hsCRP
Ridker PM et al. Lancet 2017; AHA 2017
hsCRP >2mg/L
hsCRP <2mg/L
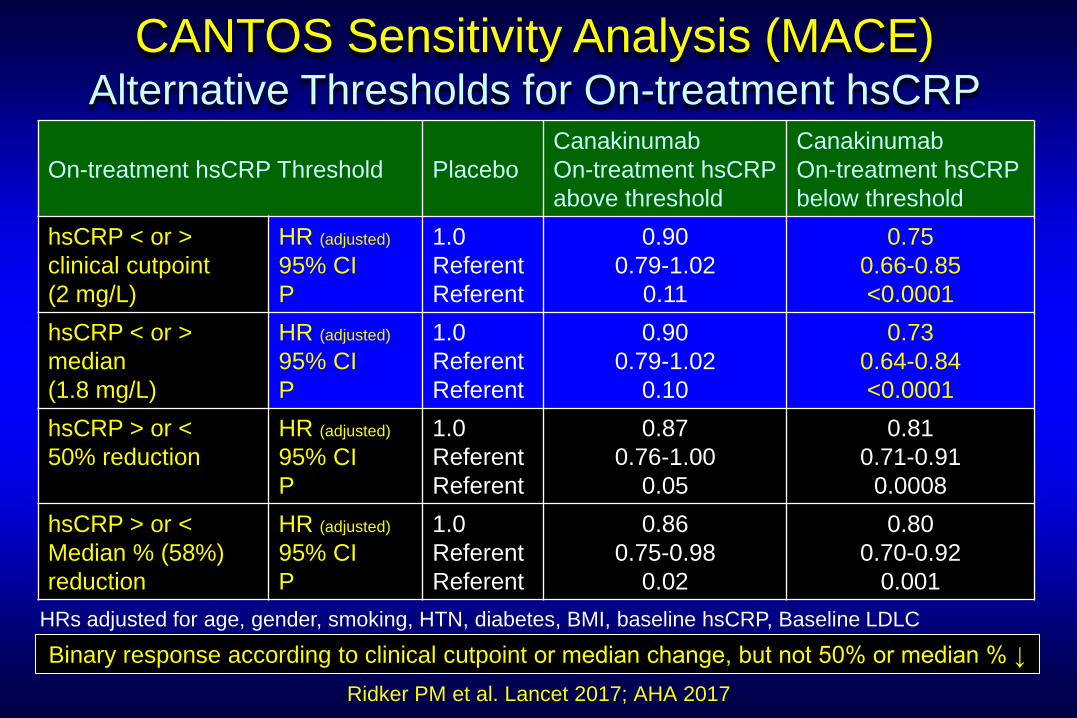
On-treatment hsCRP Threshold
Placebo
Canakinumab
On-treatment hsCRP
above threshold
Canakinumab
On-treatment hsCRP
below threshold
hsCRP < or >
clinical cutpoint
(2 mg/L)
HR (adjusted)
95% CI
P
1.0
Referent
Referent
0.90
0.79-1.02
0.11
0.75
0.66-0.85
<0.0001
hsCRP < or >
median
(1.8 mg/L)
HR (adjusted)
95% CI
P
1.0
Referent
Referent
0.90
0.79-1.02
0.10
0.73
0.64-0.84
<0.0001
hsCRP > or <
50% reduction
HR (adjusted)
95% CI
P
1.0
Referent
Referent
0.87
0.76-1.00
0.05
0.81
0.71-0.91
0.0008
hsCRP > or <
Median % (58%)
reduction
HR (adjusted)
95% CI
P
1.0
Referent
Referent
0.86
0.75-0.98
0.02
0.80
0.70-0.92
0.001
HRs adjusted for age, gender, smoking, HTN, diabetes, BMI, baseline hsCRP, Baseline LDLC
CANTOS Sensitivity Analysis (MACE) Alternative Thresholds for On-treatment hsCRP
Ridker PM et al. Lancet 2017; AHA 2017
Binary response according to clinical cutpoint or median change, but not 50% or median % ↓
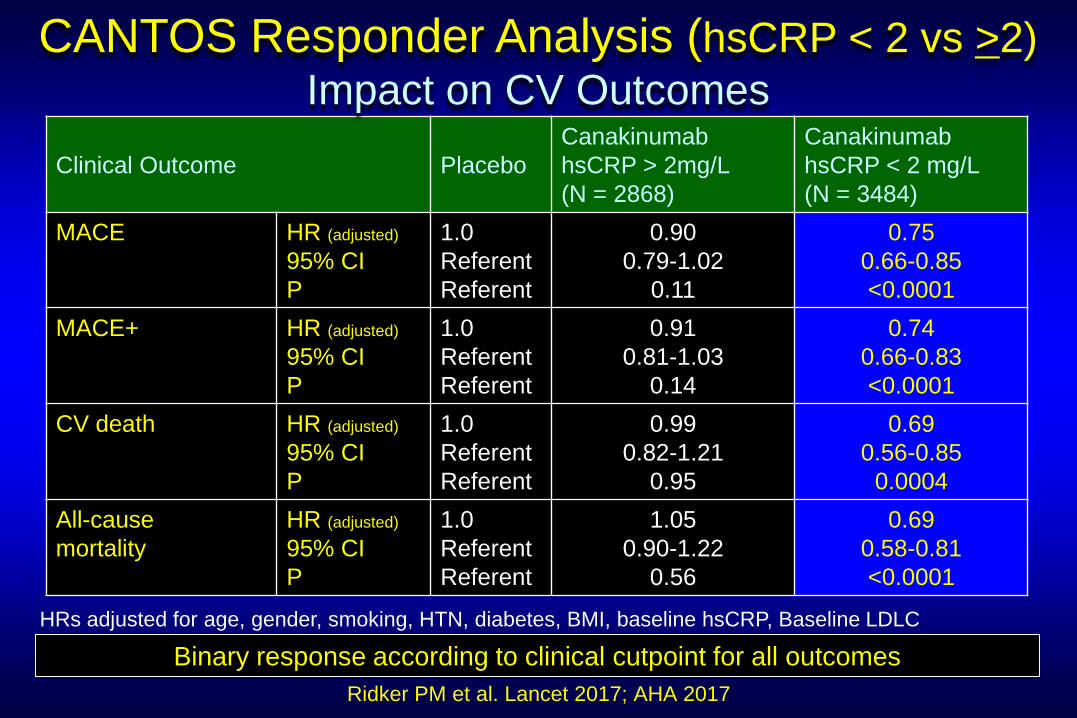
Clinical Outcome
Placebo
Canakinumab
hsCRP > 2mg/L
(N = 2868)
Canakinumab
hsCRP < 2 mg/L
(N = 3484)
MACE HR (adjusted)
95% CI
P
1.0
Referent
Referent
0.90
0.79-1.02
0.11
0.75
0.66-0.85
<0.0001
MACE+ HR (adjusted)
95% CI
P
1.0
Referent
Referent
0.91
0.81-1.03
0.14
0.74
0.66-0.83
<0.0001
CV death HR (adjusted)
95% CI
P
1.0
Referent
Referent
0.99
0.82-1.21
0.95
0.69
0.56-0.85
0.0004
All-cause
mortality
HR (adjusted)
95% CI
P
1.0
Referent
Referent
1.05
0.90-1.22
0.56
0.69
0.58-0.81
<0.0001
HRs adjusted for age, gender, smoking, HTN, diabetes, BMI, baseline hsCRP, Baseline LDLC
CANTOS Responder Analysis (hsCRP < 2 vs >2)
Impact on CV Outcomes
Ridker PM et al. Lancet 2017; AHA 2017
Binary response according to clinical cutpoint for all outcomes
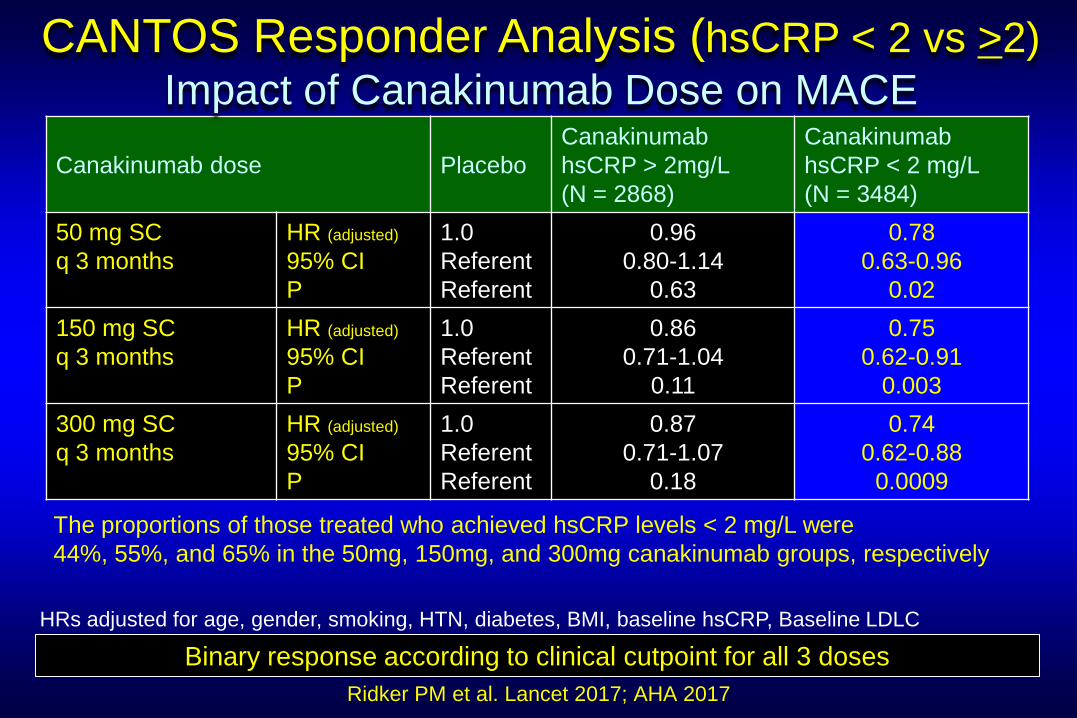
Canakinumab dose
Placebo
Canakinumab
hsCRP > 2mg/L
(N = 2868)
Canakinumab
hsCRP < 2 mg/L
(N = 3484)
50 mg SC
q 3 months
HR (adjusted)
95% CI
P
1.0
Referent
Referent
0.96
0.80-1.14
0.63
0.78
0.63-0.96
0.02
150 mg SC
q 3 months
HR (adjusted)
95% CI
P
1.0
Referent
Referent
0.86
0.71-1.04
0.11
0.75
0.62-0.91
0.003
300 mg SC
q 3 months
HR (adjusted)
95% CI
P
1.0
Referent
Referent
0.87
0.71-1.07
0.18
0.74
0.62-0.88
0.0009
HRs adjusted for age, gender, smoking, HTN, diabetes, BMI, baseline hsCRP, Baseline LDLC
Ridker PM et al. Lancet 2017; AHA 2017
Binary response according to clinical cutpoint for all 3 doses
CANTOS Responder Analysis (hsCRP < 2 vs >2)
Impact of Canakinumab Dose on MACE
The proportions of those treated who achieved hsCRP levels < 2 mg/L were
44%, 55%, and 65% in the 50mg, 150mg, and 300mg canakinumab groups, respectively
Clinical Outcome
Placebo
Canakinumab
hsCRP > 2mg/L
(N = 2868)
Canakinumab
hsCRP < 2 mg/L
(N = 3484)
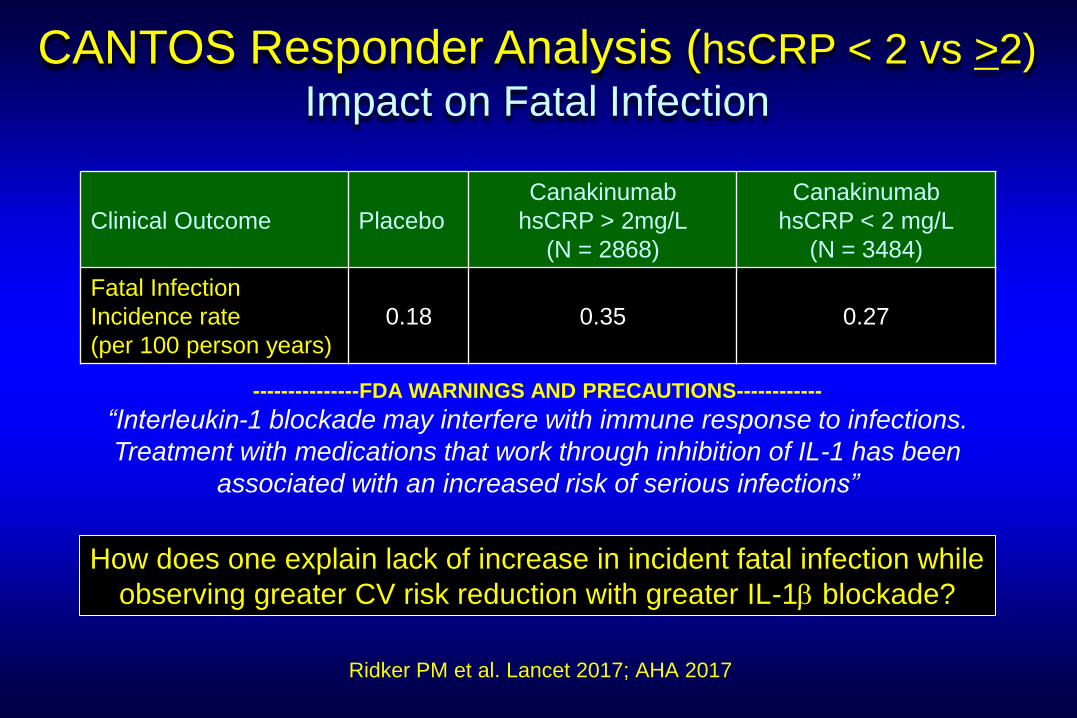
Fatal Infection
Incidence rate
(per 100 person years)
0.18
0.35
0.27
Ridker PM et al. Lancet 2017; AHA 2017
How does one explain lack of increase in incident fatal infection while
observing greater CV risk reduction with greater IL-1b blockade?
CANTOS Responder Analysis (hsCRP < 2 vs >2)
Impact on Fatal Infection
---------------FDA WARNINGS AND PRECAUTIONS------------
“Interleukin-1 blockade may interfere with immune response to infections.
Treatment with medications that work through inhibition of IL-1 has been
associated with an increased risk of serious infections”
CANTOS Responder Analysis Limitations that Challenge Interpretation
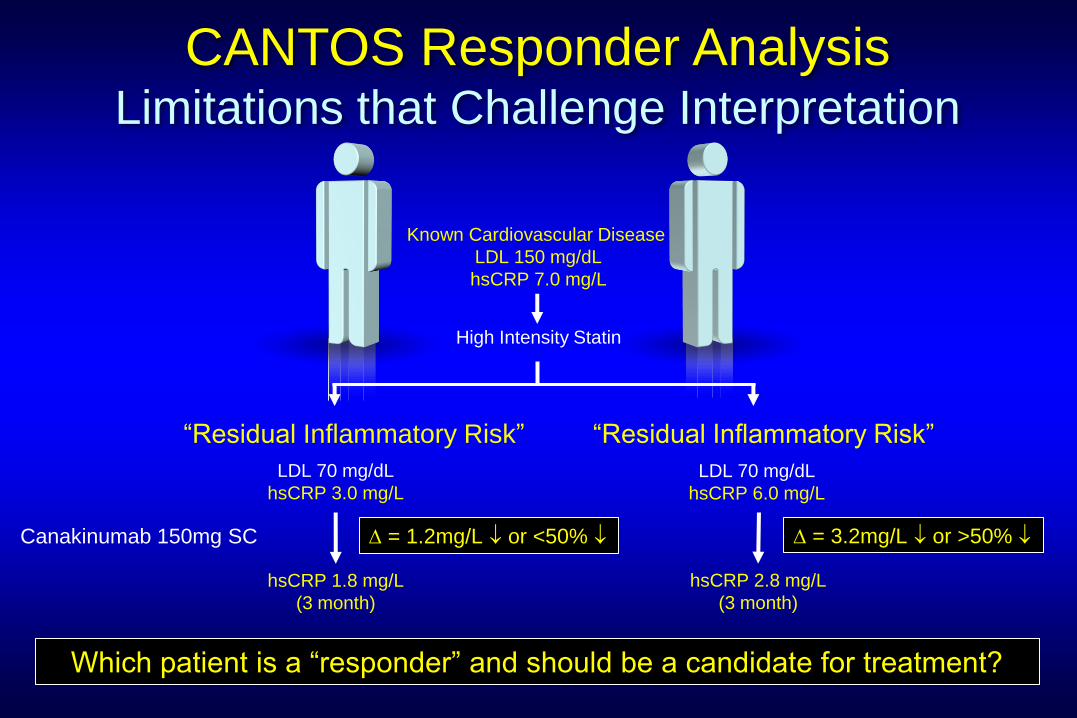
hsCRP 1.8 mg/L
(3 month)
Known Cardiovascular Disease
LDL 150 mg/dL
hsCRP 7.0 mg/L
hsCRP 2.8 mg/L
(3 month)
High Intensity Statin
LDL 70 mg/dL
hsCRP 6.0 mg/L
LDL 70 mg/dL
hsCRP 3.0 mg/L
“Residual Inflammatory Risk” “Residual Inflammatory Risk”
D = 1.2mg/L or <50% D = 3.2mg/L or >50% Canakinumab 150mg SC
Which patient is a “responder” and should be a candidate for treatment?
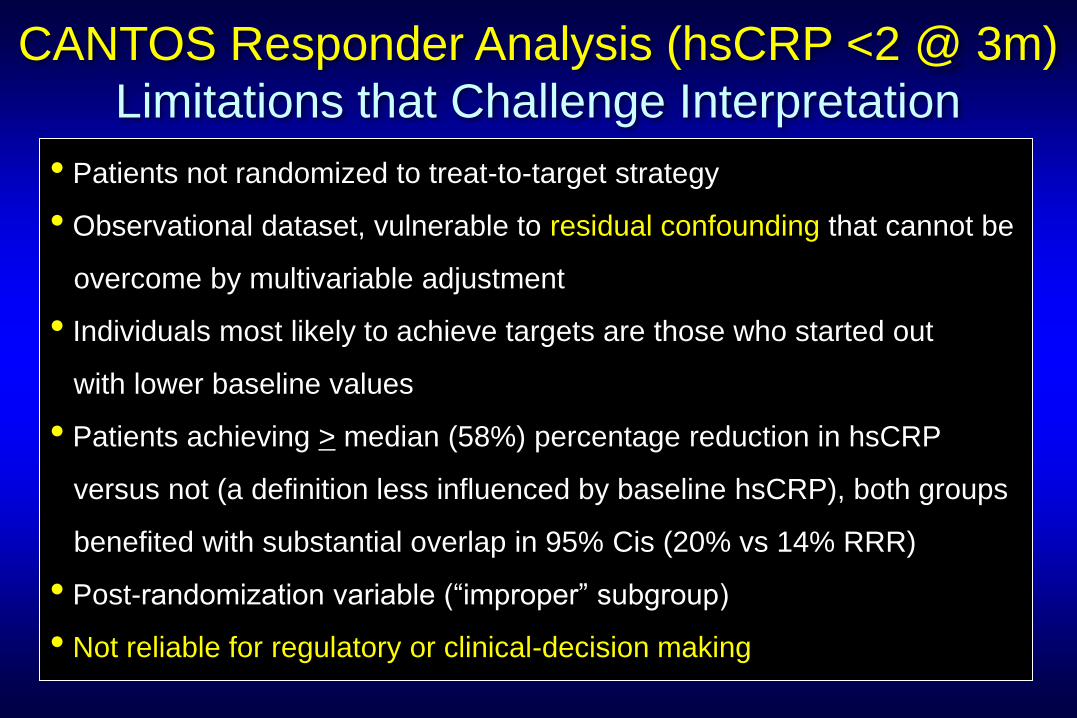
• Patients not randomized to treat-to-target strategy
• Observational dataset, vulnerable to residual confounding that cannot be
overcome by multivariable adjustment
• Individuals most likely to achieve targets are those who started out
with lower baseline values
• Patients achieving > median (58%) percentage reduction in hsCRP
versus not (a definition less influenced by baseline hsCRP), both groups
benefited with substantial overlap in 95% Cis (20% vs 14% RRR)
• Post-randomization variable (“improper” subgroup)
• Not reliable for regulatory or clinical-decision making
CANTOS Responder Analysis (hsCRP <2 @ 3m)
Limitations that Challenge Interpretation
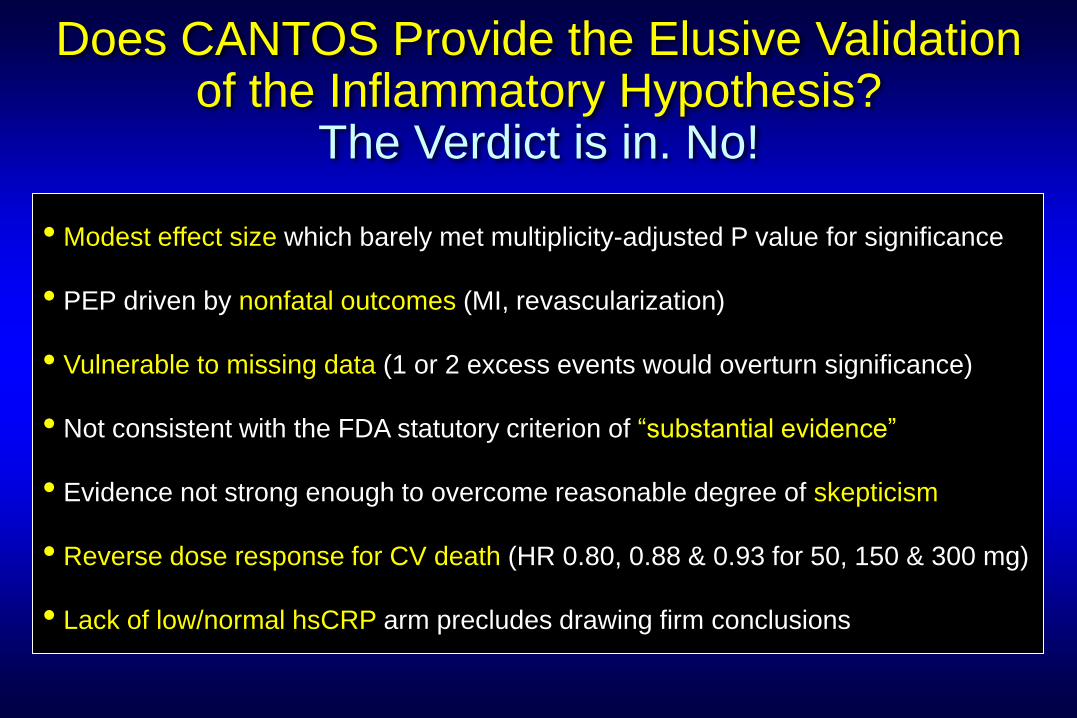
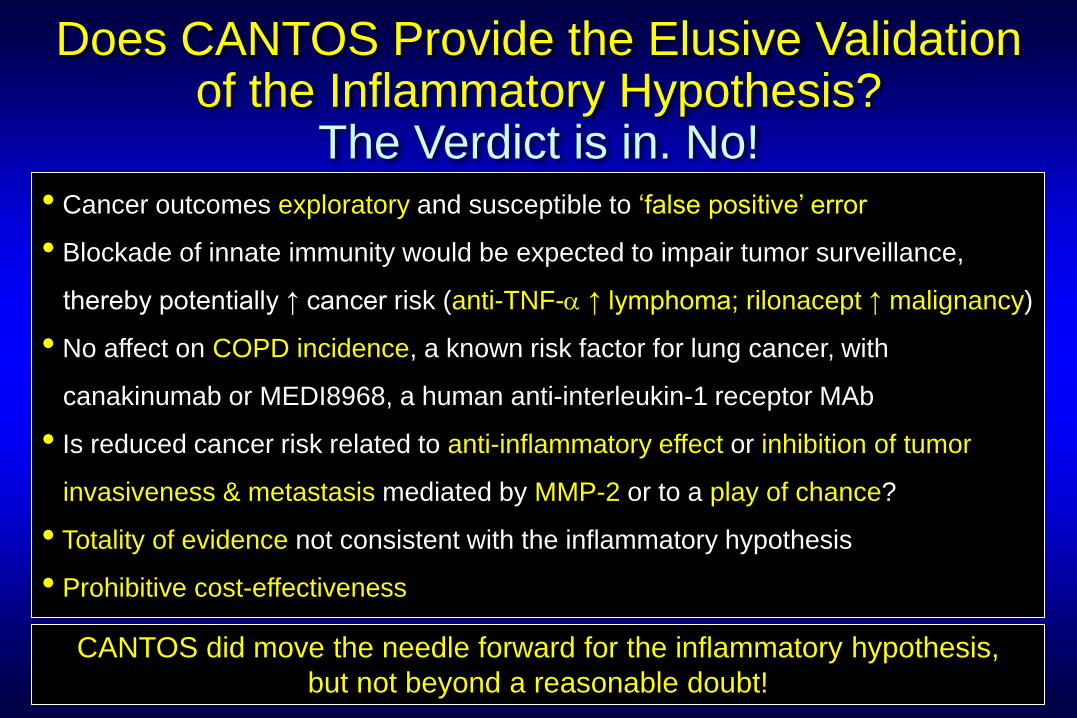
Does CANTOS Provide the Elusive Validation of the Inflammatory Hypothesis?
The Verdict is in. No!
• Modest effect size which barely met multiplicity-adjusted P value for significance
• PEP driven by nonfatal outcomes (MI, revascularization)
• Vulnerable to missing data (1 or 2 excess events would overturn significance)
• Not consistent with the FDA statutory criterion of “substantial evidence”
• Evidence not strong enough to overcome reasonable degree of skepticism
• Reverse dose response for CV death (HR 0.80, 0.88 & 0.93 for 50, 150 & 300 mg)
• Lack of low/normal hsCRP arm precludes drawing firm conclusions
Does CANTOS Provide the Elusive Validation of the Inflammatory Hypothesis?
The Verdict is in. No! • Cancer outcomes exploratory and susceptible to ‘false positive’ error
• Blockade of innate immunity would be expected to impair tumor surveillance,
thereby potentially ↑ cancer risk (anti-TNF-a ↑ lymphoma; rilonacept ↑ malignancy)
• No affect on COPD incidence, a known risk factor for lung cancer, with
canakinumab or MEDI8968, a human anti-interleukin-1 receptor MAb
• Is reduced cancer risk related to anti-inflammatory effect or inhibition of tumor
invasiveness & metastasis mediated by MMP-2 or to a play of chance?
• Totality of evidence not consistent with the inflammatory hypothesis
• Prohibitive cost-effectiveness
CANTOS did move the needle forward for the inflammatory hypothesis,
but not beyond a reasonable doubt!
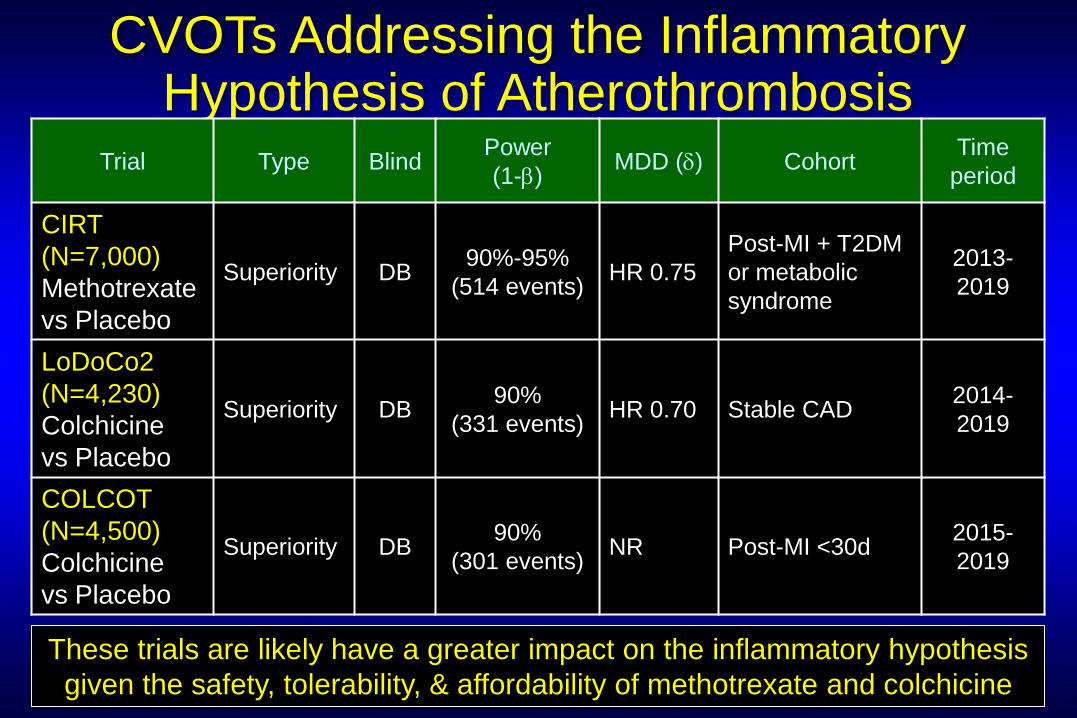
CVOTs Addressing the Inflammatory Hypothesis of Atherothrombosis
Trial Type Blind Power
(1-b) MDD (d) Cohort
Time
period
CIRT
(N=7,000)
Methotrexate
vs Placebo
Superiority DB 90%-95%
(514 events) HR 0.75
Post-MI + T2DM
or metabolic
syndrome
2013-
2019
LoDoCo2
(N=4,230)
Colchicine
vs Placebo
Superiority DB 90%
(331 events) HR 0.70 Stable CAD
2014-
2019
COLCOT
(N=4,500)
Colchicine
vs Placebo
Superiority DB 90%
(301 events) NR Post-MI <30d
2015-
2019
These trials are likely have a greater impact on the inflammatory hypothesis
given the safety, tolerability, & affordability of methotrexate and colchicine
“Extraordinary claims require extraordinary proof”
Marcello Truzzi