Embed Size (px)
Citation preview

1
Exercise prescription in type 2 diabetes treatment
Prof. L.J.C. van Loon
Maastricht University Medical Centre+ Maastricht, the Netherlands
Maastricht, February 27 , 2016
Glycemic control in type 2 diabetes
The level of glycemia is associated with the development of cardiovascular complications Glycemic control is fundamental to type 2 diabetes treatment ADA; EASD; IDF
Therapeutic targets should be aimed at reducing
post-prandial blood glucose excursions
Standard parameters for the assessment of glycemic control
do not provide sufficient information on post-prandial
hyperglycemia
Target for diabetes intervention
Basal blood glucose and HbA1c content
Glycemic control
Self-monitored blood glucose concentration
Continuous Glucose Monitoring System
Maran et al., Diabetes Care, 2001

2
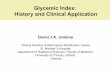
Continuous Glucose Monitoring System Glycemic control
van Dijk et al., Diabetes Res Clin Pract, 2011
Time (h)
7:00 11:00 15:00 19:00 23:00 3:00 7:00
Glucose con
centratio
n (m
mol/L)
0
4
6
8
10
12
14 Control Type 2 diabetes
Daily glycemic control
Prevalen
ce of h
yperglycem
ia (%
/ 24 h)
0
10
20
30
40
50
control type 2 diabetes
type 2 diabetes
control
A B
HbA1c <7%, (<53 mmol/mol)
*
*
van Dijk et al., Diabetes Res Clin Pract, 2011
Glycemic control in type 2 diabetes
Under standardized dietary conditions long-standing
type 2 diabetes patients are in a state of hyperglycemia
throughout the greater part of the day
Oral blood glucose lowering medication
does not provide ample protection
against (post-prandial) hyperglycemia Praet et al., Clinical Science, 2006
Type 2 diabetes treatment
Oral blood glucose lowering medication Exogenous insulin therapy
The type 2 diabetes epidemic
“100% of the increase in the prevalence of
type 2 diabetes and obesity in the United States
during the latter half of the 20th century must be
attributed to a changing environment interacting
with genes, because 0% of the human genome has
changed during this time period.”
Booth et al., JAP, 2000

3
Lifestyle changes Diabetes prevention - lifestyle
Finnish Diabetes Prevention Study Tuomiletho et al., NEJM, 2001 58% reduced risk type 2 diabetes Diabetes Prevention Program Knowler et al., NEJM, 2002 Lifestyle > Metformin > Placebo Da Qing Diabetes Prevention Pan et al., Diabetes Care, 1997 42-46% reduced risk type 2 diabetes
Malmö Preventive Trial Eriksson et al., Diabetologia, 1998 Significant reduction mortality
Diabetes treatment
Diabetes cohort studies report regular exercise to be associated with a 40-70% lower mortality rate for 8 to 14 years
Hu F. et al., Ann. Intern. Med., 1999
Wei et al., Ann. Intern. Med., 2000 Tanasescu., Circulation, 2003
Hu G. et al., Circulation, 2004
Exercise in diabetes treatment
• whole-body insulin sensitivity (0-80%)
• glycemic control (HbA1c : -0.7 %)
• oxidative capacity (VO2max : 0-15%)
• cardiovascular risk profile (LDL, TG, BP)
• fat mass and body composition
Boulé et al., Diabetologia, 2003; Sigal et al., Diabetes Care, 2006; Praet et al., J Appl Physiol, 2007; Umpierre et al., JAMA, 2011; Chudyk et al., Diabetes Care, 2011
Position statement A
To improve glycemic control, assist with weight maintenance, and
reduce risk of CVD, at least 150 min/wk of moderate-intensity aerobic
physical activity (50-70% HRmax) is recommended and/or at least
90 min/wk of vigorous aerobic exercise (70% HRmax). The physical
activity should be distributed over at least 3 days/wk and with
no more than 2 consecutive days without physical activity.
ADA 2007 - Standards of Medical Care in Diabetes
Diabetes Care, 2007
Exercise training and glycemic control
The improvements in glycemic control with exercise training are largely
attributed to the cumulative effects of transient improvements in glucose
tolerance following each successive bout of exercise
Goodyear and Kahn, Ann Rev Med, 1998
Effects of training on glycemic control may be
lost entirely 6-10 days after cessation of training
Praet and van Loon, J Appl Physiol, 2007

4
Endurance type exercise
An acute bout of endurance type exercise improves insulin sensitivity for a period up to 48 h. Schneider et al., Diabetologia, 1984
Devlin et al., Diabetes, 1987
Cusi et al., J. Clin. Invest., 2000
Wojtaszewski et al., Diabetes, 2000
Position statement A
To improve glycemic control, assist with weight maintenance, and
reduce risk of CVD, at least 150 min/wk of moderate-intensity aerobic
physical activity (50-70% HRmax) is recommended and/or at least
90 min/wk of vigorous aerobic exercise (70% HRmax). The physical
activity should be distributed over at least 3 days/wk and with
no more than 2 consecutive days without physical activity.
ADA 2007 - Standards of Medical Care in Diabetes
Diabetes Care, 2007
Acute exercise in type 2 diabetes
Praet et al., Med. Sci. Sports Exerc., 2006
Hyp
ergl
ycem
ia (
dura
tion
%/2
4h)
Exercise as therapy
Based on baseline aerobic fitness, level of co-morbidities,
appendicular skeletal muscle mass and strength, patients should
be provided with a fitting exercise intervention program to
optimize its therapeutic value.
Exercise modalities
- type of exercise
- intensity of exercise
- duration of exercise
- frequency
- timing
Type of exercise
Lance Armstrong Jay Cutler

5
Endurance type exercise
An acute bout of endurance type exercise improves insulin sensitivity for a period up to 48 h. Devlin et al., Diabetes, 1987
Mikines et al., AJP, 1988
Perseghin et al., NEJM, 1996
Endurance type exercise
Long-term weight loss and weight control Feasibility in elderly patients with type 2 diabetes
Feasibility in type 2 diabetes with co-morbidities
Long-standing type 2 diabetes
Fang et al., 2005 Sayer et al., 2005
Volpato et al., 2002
Thomas et al., 2004 Meyer et al., 1990
Muscle weakness
Cardiovascular co-morbidities
Exercise intolerance
Low adherence and compliance
Aging and sarcopenia
Loss of skeletal muscle mass, strength, and function
with aging is both cause as well as a consequence
of type 2 diabetes
Proportional relationship between muscle mass
and glucose disposal capacity
Park et al., 2006; Willey et al., 2003
Resistance type exercise
Muscle mass
Muscle strength
Functional capacity
Resistance type exercise
Progressive resistance type exercise training offers a safe and effective alternative to endurance type exercise training
An acute bout of resistance exercise improves insulin sensitivity to a similar extent as endurance exercise Fluckey et al.,1994 Fenicchia et al., 2004 Koopman et al., 2005

6
van Dijk et al., Diabetologia, 2012
Type of exercise, design
randomized, 3-way crossover
Type of exercise, intervention
45 min, 75% 1 RM 45 min, 50% Wmax
Time
6:00 9:00 12:00 15:00 18:00 21:00 0:00 3:00 6:00 9:00 12:00
Bloo
d glucose concen
tration (m
mol/L)
0
6
8
10
12
14
16Control: no exerciseResistance-‐type exerciseEndurance-‐type exercise
24-h glycemic profiles
van Dijk et al., Diabetologia, 2012
Prevalen
ce of h
yperglycem
ia (%
/ 24
h)
0
10
20
30
40
50
IGT OGLM INS
* *
**
* *
#
Prevalence of hyperglycemia
Control: no exerciseResistance-‐type exerciseEndurance-‐type exercise
van Dijk et al., Diabetologia, 2012
Resistance type exercise
- improved glucose disposal
- glycogen storage capacity
- GLUT-4 content
- glycemic control (HbA1c: -1.1%)
- insulin sensitivity
- oral glucose tolerance
- cardiovascular risk profile (HDL, LDL, BP)
- body composition
Castaneda et al., 2002; Dunstan et al., 1998, 2002;
Ishii et al., 1998, Cauza et al., 2005; Willey et al., 2003
Church et al., JAMA, 2010

7
Position statement B
In the absence of contraindications, people with type 2 diabetes should be encouraged to perform resistance exercise 3 times a week, targeting all major muscle groups, progressing to 3 sets of 8-10 repetitions at a weight that cannot be lifted more than 8-10 times. ADA 2007 - Standards of Medical Care in Diabetes Diabetes Care, 2007
Exercise modalities
- type of exercise
- intensity of exercise
- duration of exercise
- frequency
- timing
- interaction with pharmaceuticals
- interaction with food intake
Low versus high-intensity exercise
Manders et al., Med Sci Sports Exerc, 2010
Exercise intensity and glycemic control
Manders et al., Med Sci Sports Exerc, 2010
60 min @ 35% Wmax
30 min @ 70% Wmax
Newsom et al., Diabetes Care, 2013
Exercise intensity and insulin sensitivity
~70 min @ 50% VO2max
~55 min @ 65% VO2max

8
Exercise modalities
- type of exercise
- intensity of exercise
- duration of exercise
- frequency
- timing
06:00 12:00 18:00 00:00 06:00 12:00 18:00 00:00 06:00 12:00
DAILY
NON-‐DAILY
48 h analysis period
Day 1 Day 2 Day 3
CONTROL
(30 min)
(60 min)
(30 min)
randomized, 3-way crossover
Study design
van Dijk et al., Diabetes Care, 2012
Prev
alen
ce o
f hyp
ergl
ycem
ia (%
of t
he ti
me)
0
20
30
40
Total 48 h First 24 h Second 24 h
* * ** * *
van Dijk et al., Diabetes Care, 2012
Prevalence of hyperglycemia
CONTROL: no exerciseNON-DAILY exerciseDAILY exercise
Are the blood glucose lowering effects equal for all type 2 diabetic patients?
individual change in average glucose concentration over 24 h period following exercise
subject
0 10 20 30 40 50 60
delta
glu
cose
con
cent
ratio
n (m
mol
/L)
-5
-4
-3
-2
-1
0
1
2
Individual response to exercise
Well-controlled and suboptimally controlled patients
bloo
d gl
ucos
e co
ncen
tratio
n (m
mol
/L)
0
6
8
10
12
prev
alen
ce o
f hyp
ergl
ycem
ia (h
our/d
ay)
0
2
4
6
8
10
12
14control exercise
*
*
*
*
A B
-0.6 mmol/L
-1.2 mmol/L -3:24 h:min
-1:43 h:min
Hba1c <7% HbA1c ≥7% Hba1c <7% HbA1c ≥7%

9
Exercise or simply more habitual physical activity to improve blood glucose homeostasis?
Study design
12.00 12.00 0.00 18.00 6.00 0.00 18.00 6.00
day 1
6.00 18.00
day 2 day 3
12.00
Study protocol
6.00 8.00 10.00 12.00 14.00 16.00 18.00 20.00 22.00
Exercise
Habitual Physical Activity
Control
Blood
45 min
15 min 15 min 15 min
4
6
8
10
12
14
16
8:30 11:30 14:30 17:30 20:30 23:30 2:30 5:30 8:30
Blo
od g
luco
se (m
mol
/L)
Time (h)
Control Habitual Physical Activity Exercise
0
24-h blood glucose
van Dijk et al., Diabetes Care, 2013
0
1
2
3
4
5
6
7
8
9
Control Habitual Physical Activity
Exercise
Hyp
ergl
ycem
ia (h
ours
/day
)
24-h glycemic control
*
van Dijk et al., Diabetes Care, 2013

10
4
6
8
10
12
14
16
8:30 11:30 14:30 17:30 20:30 23:30 2:30 5:30 8:30
Blo
od g
luco
se (m
mol
/L)
Time (h)
Control Habitual Physical Activity Exercise
Postprandial glycemic control
0
van Dijk et al., Diabetes Care, 2013
Insulin iAUC
*
* †
-17±5%
-33±4%
10
15
20
25
30
35
40
45
Control Habitual Physical Activity
Exercise
insu
lin iA
UC
(mU
/mL/
11h)
0
van Dijk et al., Diabetes Care, 2013
Summary
Hyperglycemia is highly prevalent throughout the day in
type 2 diabetes patients.
Exercise strongly reduces the prevalence of hyperglycemia
throughout the day.
Resistance and endurance-type exercise are equally effective in
improving daily blood glucose homeostasis.
Summary II
Higher intensity exercise is not more effective than lower
intensity exercise to improve daily blood glucose homeostasis.
When total work is being matched, daily exercise does not
further improve glycemic control, when compared to exercise
performed every other day.
Even well-controlled patients can benefit from the glucose
lowering properties of exercise.
Summary III
Habitual physical activity attenuates the postprandial rise in
blood glucose and insulin concentrations.
When matched for duration, exercise is more effective than
more habitual physical activity to improve glycemic control.
The volume of physical activity seems to determine the
improvements in glycemic control.
Exercise prescription

11
Collaborators and sponsors
M3 research unit www.m3-research.nl