United Republic of Tanzania Ministry of Health
Cost per child managed correctly in Tanzania
London , 13-14 Dec 2005
United Republic of Tanzania Ministry of Health
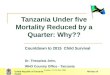
Evidence for recent child survival gainsRufiji District Sentinel
surveillance (RDSS)-48%-60%Source: MOH TEHIP / NSS
London , 13-14 Dec 2005
Rufiji DSS Mortality Trend
1411513.8108.213.212.1
113.212.511.673.210.29.3
102.111.710.866.19.58.7
109.512.211.167.69.78.7
72.910.19.145.78.17.2
Under-five
Infant
Mortality (nq0)
National DHS Mortality Trend
14192
136.45211.6811.6887.4719.3799.379
146.59318.15718.15799.13914.19214.192
11268
Under-five
Infant
Mortality (nq0)
Data
DHS Trends - Tanzania
Rates and 95% CI
1992199619992004
Under-five141136.452146.593112
+2SE11.6818.157
-2SE11.6818.157
Infant9287.47199.13968
+2SE9.37914.192
-2SE9.37914.192
DSS Trends - Rufiji
Rates and 95% CI
19992000200120022003
Under-five141113.2102.1109.572.9
+2SE1512.511.712.210.1
-2SE13.811.610.811.19.1
Infant108.273.266.167.645.7
+2SE13.210.29.59.78.1
-2SE12.19.38.78.77.2
Sheet2
Sheet3
United Republic of Tanzania Ministry of Health
Key message 3Better access to quality health services as a
result of policies and investments supporting the Tanzanian Health
System.
London , 13-14 Dec 2005
United Republic of Tanzania Ministry of Health
Strong Investment in Rural Health Infrastructure & Primary
Health careStructural adjustment and Debt CrisisHealth Sector
ReformsEssential health interventions &Sector wide
ApproachEvolution of health sector in Tanzania
London , 13-14 Dec 2005
United Republic of Tanzania Ministry of Health
Aligning budgets with priorities
1996-97Before basket funding and planning tools..
2000-01After basket funding and planning tools..
London , 13-14 Dec 2005
United Republic of Tanzania Ministry of Health
ChallengesSustaining the observed child health gains
Inadequate coverage of interventions and tools e.g District
burden-of-disease planning tool & health budget mapping
tools
HIV/AIDS pandemic threatening to reverse the gains
Co-ordination at national, district and community level
London , 13-14 Dec 2005
United Republic of Tanzania Ministry of Health
ConclusionsTanzania has a comparative advantage for Child
SurvivalGood access & utilization of health facilitiesHealth
sector reform Poverty Reduction Strategy- PRSP II (NSGRP)Potential
for achieving the child survival ;Mobilizing available resources
for child health interventionsScaling up of and universal access to
effective interventionsStrengthening Partnership at all levels e.g.
Maternal, Newborn and Child Health Partnership
London , 13-14 Dec 2005
United Republic of Tanzania Ministry of Health
Implications for universal coverageNational Health Sector
Strategic plan and Development frameworks to support Child
survivalIncreasing resource allocation for scaling up of child
survival delivery interventions and strategiesDecentralization at
district including;capacity building for planning and budgeting Use
of data for decision making and resource allocation e.g. DHA,
BOD,SHMPrioritization of essential interventions
Harmonization and convergence of partners through National
Partnerships e.g. Maternal Newborn and Child Survival
Partnership
London , 13-14 Dec 2005
United Republic of Tanzania Ministry of Health
Implications for Universal Coverage It is never too late to
invest in developing sustainable health systems that provide
evidence based, cost effective and high impact interventions with
high coverage and quality.
London , 13-14 Dec 2005
United Republic of Tanzania Ministry of Health
Thank you
London , 13-14 Dec 2005
Gains in child survival were stagnant and sometimes worsening
during the 1990s according to three consecutive DHS national child
mortality surveys. But in the fourth and most recent 2004/2005 DHS
survey, a substantial reduction in under-five and infant mortality
has been seen.
Declines over the past 5 years were also seen in various
districts running continuous mortality surveillance systems. One
district, implementing health system reforms starting in 1997-8 is
shown. Some of these reforms (e.g. basket funding) were extended to
the rest of the country starting in 2002.
Some of the survival gain in MCE /TEHIP supported districts was
shown to be due to IMCI (13% between 2000 and 2002).
[Note the current national DHS value is the estimate for the
previous five years from the survey. We are attempting to get the
data to parse out the year by year mortality estimates during this
period. The 2002 census showed no mortality decline (U5M 153), so
it is possible that much of this five year decline occurred since
2001. While Child and under five mortality show downward trend the
neonatal mortality is still stagnant
The red solid line reflects The MDG target for Tanzania which is
48.4 per 1000 Live births is estimated from the 1990 U5mortality
which was 145 per 1,000 Live births.
With the 24% reduction in U5M represents 39,200 child deaths
prevented per year..With the current trends Tanzania is likely to
attain the target even before 2015 Tanzania has experienced
increased effort to scaling interventions which have proven to be
effective for reducing child mortality.These interventions has been
prioritized in the national Essential Interventions Package for
Health services and all the districts are directed to include these
interventions into their comprehensive district health plans. They
include; (next slide)
These are some of the interventions.IMCI was introduced in
Tanzania in 1996 starting with 7 districts, the review which was
conducted in 1998 recommended scaling up of IMCI to all districts s
in a phased up manner.As shown in 1999 IMCI was in 20 out of 114
districts, we currently in 107 out of 114 (93.8%).. But all
districts have included IMCI in their plans. The rapid expansion
was observed in the last 2 years as a result of results from Multi
country evaluation of IMCI that IMCI works and cost more money as
it was originally thoughtImmunizations coverage has equally
improved as a result of strengthening both routine and
supplementary campaigns and surveillance systemVitamin Coverage
varies from source. TDHS reports a lower rate of 46%. However the
figure from the Population Based Assessment on Vit A
supplementation coverage, conducted in Sept 2004 was 85%
RBM Monitoring for ITN 2005 survey conducted in August found out
ITN use in U5 was 30%Access to anti malarial treatment within first
24 hours 58% (TDHS 2004-2005)
Exclusive breast feeding rate is estimated to be 41% While
skilled attendants at birth is still very low 47% despite very high
ANC attendance of >90% for 4 visits Key messages from MCE have
facilitated to change the mind set of people who did not believe in
IMCI and resources have been increased to support IMCI
implementation at all levels
IMCI was also associated with high quality of care of children
who were correctly managed as compared to non IMCI districtsThe
cost of the child correctly managed is extremely lower in IMCI
districts as compared to non IMCI districts..Declines over the past
5 years were also seen in various districts running continuous
mortality surveillance systems. One district, implementing health
system reforms starting in 1997-8 is shown. Some of these reforms
(e.g. basket funding) were extended to the rest of the country
starting in 2002.If we could be able to implement as in this rural
district through out the country we could be able to attain the MD
target.The other components included Capacity building for
management, BOD and DHA tool, Integrated mangement cascade for
supportive supervision Phase 1: 1960- 1970s: Primary health Care,
strong investment in rural health infrastructure, health human
resources, and health systems which formed a basis for improved
health status
Phase II: 1970- 1990: Structural adjustments, debt crisis,
escalating costs which was subsequently followed by poor quality of
services and increase in mortality
Phase III: 1990-todate: Health Sector reform with
decentralization, Essential interventions package e.e IMCI,
Immunization, Nutrition, Sector wide approaches, health strategic
plan, PRSP I & IIResulting in improved quality of services and
decline in mortality.
Use of Planning tools in Morogoro Rural. Among the tools which
were used included; DHA, BOD and Health management has helped the
districts to allocated resources to interventions with high burden
e.g. 1997 more resources to EPI, TB DOTs proportionately the
picture changed in 2001, now more resources are allocated to
interventions with high burden e.g. Malaria and IMCI