Embed Size (px)
Citation preview

Food Security and Malnutrition ManagementMalnutrition Management
Cameron Gongwer MD, MPH, DTMH

Objectives
• Know the disease burden of malnutrition and the state of global food security
• Identify the causes of malnutrition
• Understand the classification, indicators, and management of malnutrition

Definition
Imbalance between the amount of food and nutrients the and nutrients the body needs and what the body actually gets.
Under and Over Nutrition

Double Burden in Children < 5 yrs
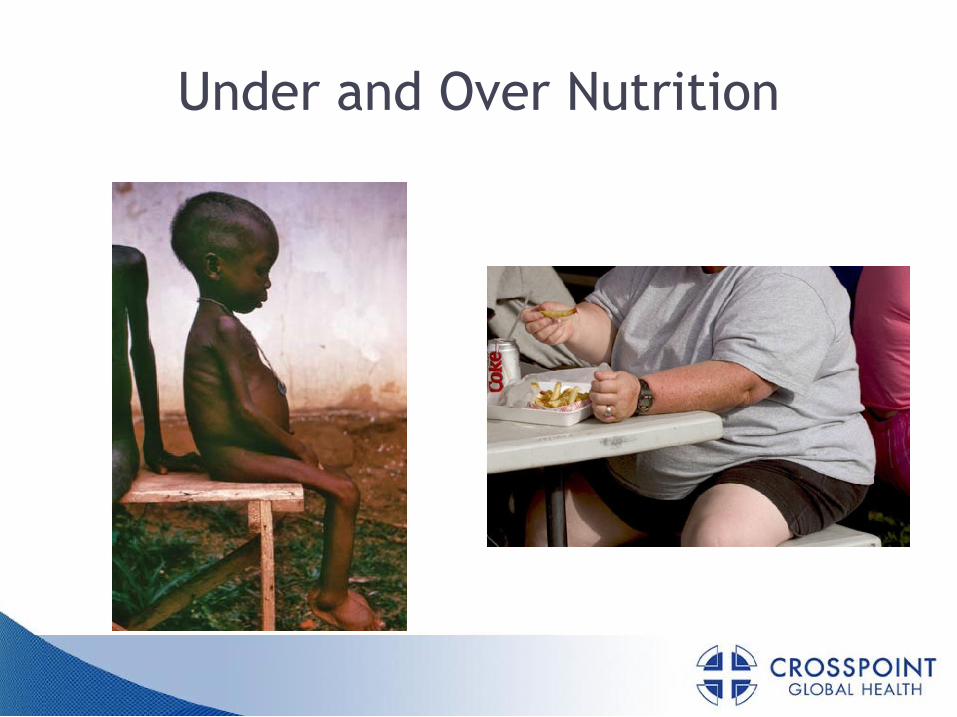
Focus on family planning,infectious disease control
Focus on faminealleviation/prevention
Nutrition Transition
Epidemiologic Transition
High prevalenceundernutrition
High prevalenceinfectious disease
High fertility/mortality
Receding famineReceding pestilence, poorenvironmental conditions
Reduced mortality,changing age structure
Changes in Nutrition, Health, and DemographicsDemographic
Transition
infectious disease control alleviation/prevention
Nutrition-related noncommunicable
diseases predominate
Chronic diseasespredominate
Reduced fertility,aging
Focus on medical intervention,policy initiatives, behavioral change
Focus on healthy aging spatial redistribution
Source: Popkin (2002). Pub. Health Nutr 5.


Undernutrition in Children

Leading Risk to Health

Global Disease Burden Risk Factors
WHO, 2004

Mortality

Global Burden and Prevalence
Stunting 1990-2015 Underweight 1990-2015
Source: UNICEF and WHO, 2012 Estimates




Micronutrient Deficiency: Deaths and Disability in Children < 5
Black et al, 2008 Lancet

Black et al, 2008 Lancet

Food Security
“when all people at all times have access to sufficient, safe, nutritious food to maintain a healthy maintain a healthy and active life.”
World Food Summit 1996

Pillars of Food Security
Household
Regional
From LSHTM Individual

Food Insecurity

Classification of Malnutrition
Marasmus (Wasting)
Kwashiorkor (Edema)
Mixed Marasmus-Mixed Marasmus-Kwashiorkor
Micronutrient Deficiencies

Marasmus
• Most common
• Inadequate intake of all nutrientsall nutrients
• Severe wasting of muscle mass and depleted body fat
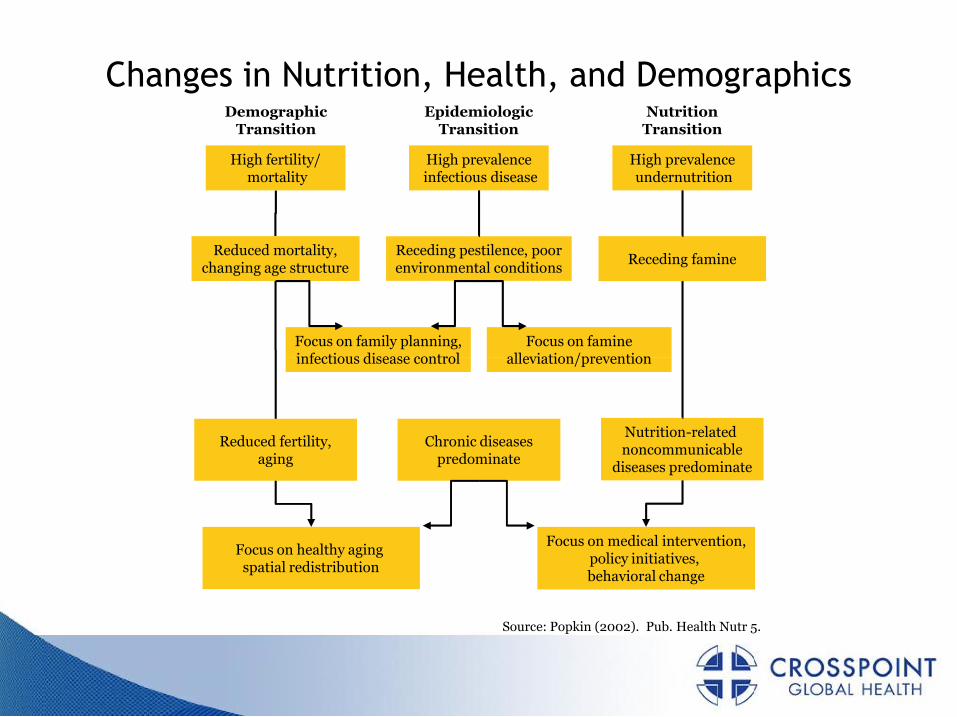
Kwashiorkor
• Undernutrition with edema
• “Kwashiorkor” from Ga in GhanaGa in Ghana
• Kwashiorkor patients die much more frequently

Mixed Marasmus and Kwashiorkor
• Usually in children 6 months to 2 years
• Early weaning period
Delayed • Delayed complementary foods
• Low protein diet
• Severe or frequent infections

• Deficiency in essential vitamins and minerals required for normal physiologic function
• Fat Soluble Vitamins (A,D,E,K), esp. Vit A
Micronutrient Malnutrition
“HIDDEN HUNGER”
• Water Soluble Vitamins (B,C)
• Minerals and Trace Elements
esp. Iron, Iodine and Zinc
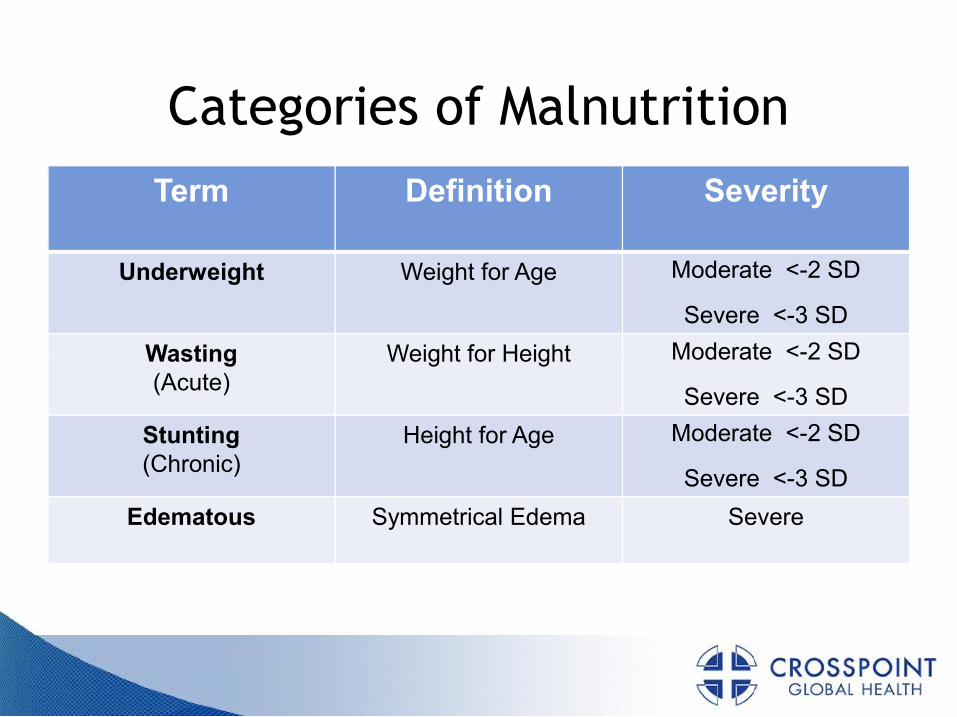
Categories of Malnutrition
Term Definition Severity
Underweight Weight for Age Moderate <-2 SD
Severe <-3 SD
Wasting Weight for Height Moderate <-2 SD Wasting(Acute)
Weight for Height Moderate <-2 SD
Severe <-3 SD
Stunting(Chronic)
Height for Age Moderate <-2 SD
Severe <-3 SD
Edematous Symmetrical Edema Severe
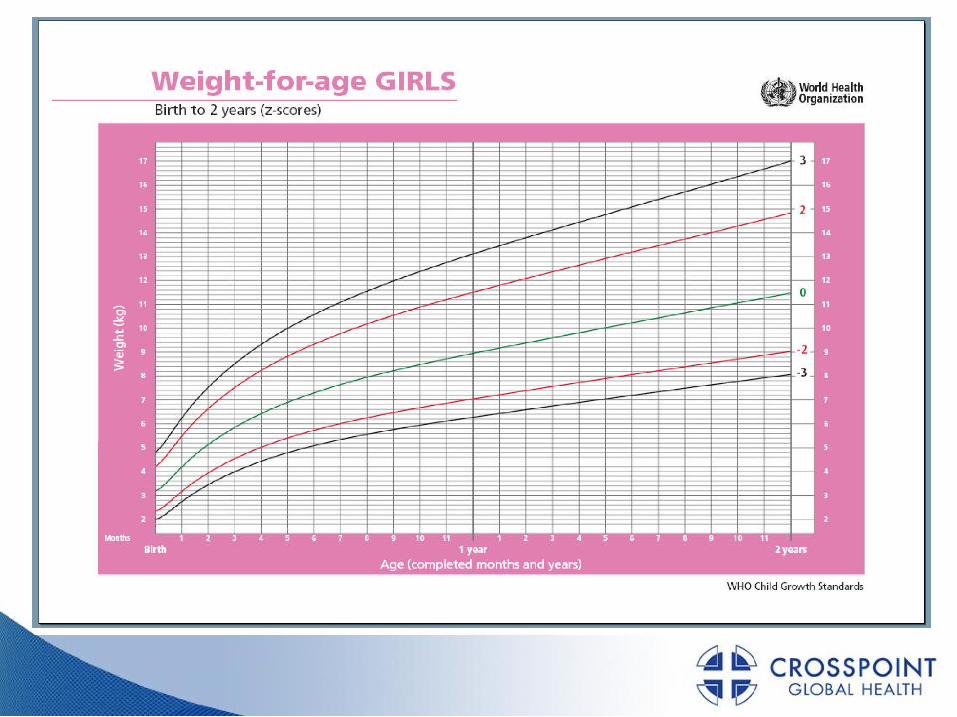

Growth Calculators for iPhone/iPod

Mid Upper Arm Circumference
• < 11.5 cm Severe
UNDERNUTRITION
• 11.6-12.4 cm Moderate
• 12.5-13.4 cm Mild
• > 13.5 cm Normal

Managing Malnutrition
• Outpatient Community based ManagementManagement
• Inpatient Facility Treatment

Acute Malnutrition
Without Complications
With Complications
Moderate Acute
Malnutrition
Supplementary Feeding
Severe Acute Malnutrition
Community Based Care
SAM & MAM
Inpatient Care

Complications
• Anorexia
• LRTI
• High Fever
• Severe dehydrationSevere dehydration
• Anemia
• Not alert
• Hypoglycemia
• Hypothermia

Inpatient Treatment

WHO 10 Step Treatment TimeframeStabilization Rehabilitation Follow-up
Days 1-2 Days 3-7 Weeks 2-6 Weeks 7-26
1 Hypoglycemia ---------→
2 Hypothermia ---------→
3 Dehydration ---------→
4 Infection --------------------→
5 Electrolytes ----------------------------------------------------→
6 Micronutrients ------NO Iron----→ ----With Iron--→
7 Initiate refeeding --------------------→
8 Catch up feeding ----------------------------------→
9 Sensory stimulation ------------------------------------------------------------------------→
10 Prepare discharge -----------------→
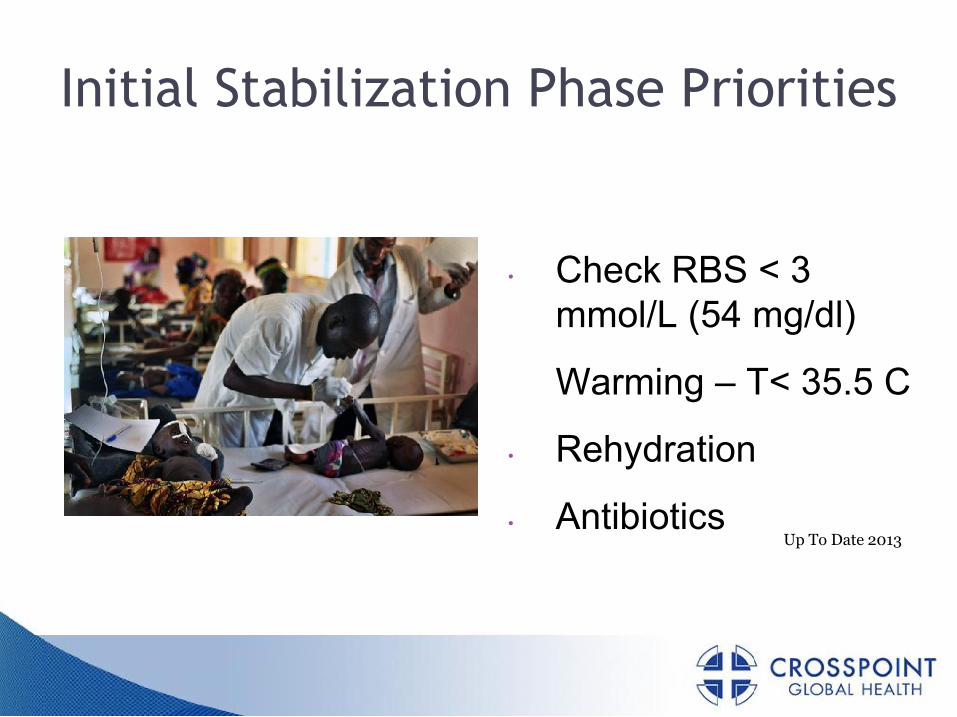
Initial Stabilization Phase Priorities
• Check RBS < 3 mmol/L (54 mg/dl)
Warming – T< 35.5 C
• Rehydration
• AntibioticsUp To Date 2013
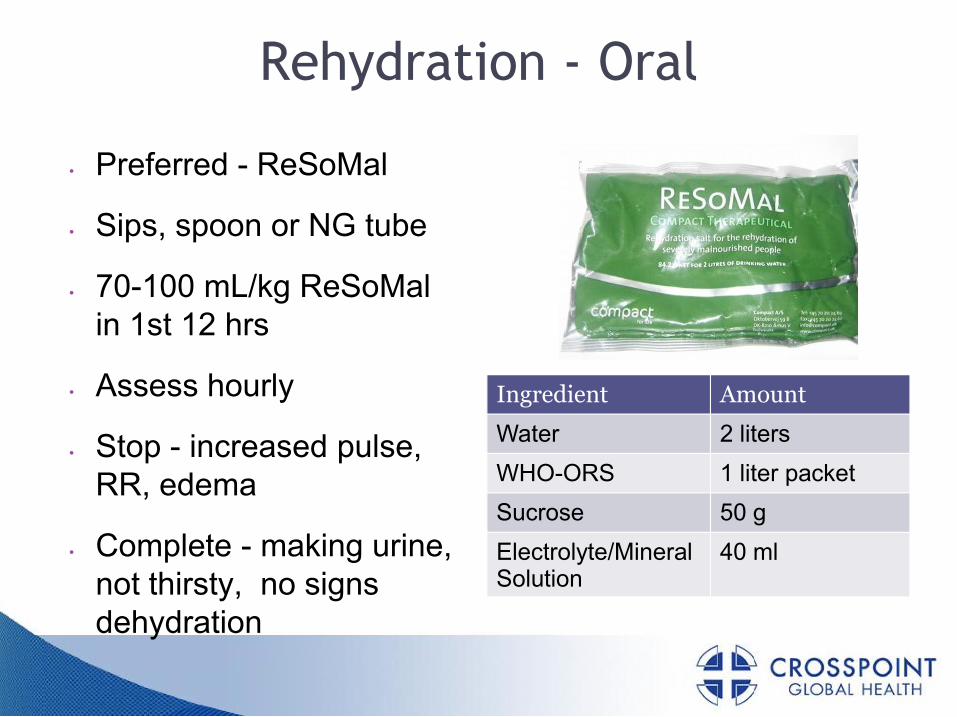
Rehydration - Oral
• Preferred - ReSoMal
• Sips, spoon or NG tube
• 70-100 mL/kg ReSoMal in 1st 12 hrs
• Assess hourly
• Stop - increased pulse, RR, edema
• Complete - making urine, not thirsty, no signs dehydration
Ingredient Amount
Water 2 liters
WHO-ORS 1 liter packet
Sucrose 50 g
Electrolyte/Mineral Solution
40 ml

Intravenous Rehydration
• ONLY for shock or severe hypovolemia
• D5W RL + 20 mEq KClpreferred
1st bolus – 15 mL/kg • 1st bolus – 15 mL/kg over 1 hr
• 2nd bolus 15 mL/kg if better and no PO intake
• Switch to oral ASAP

Treat Infection
• Complications
▫ Ampicillin (50 mg/kg IM/IV q 6h x 2d, then Amoxicillin (15 mg/kg tid x 5d)
▫ AND Gentamicin (7.5 mg/kg IM/IV daily x 7d)▫ AND Gentamicin (7.5 mg/kg IM/IV daily x 7d)
▫ If NO improvement in 48 hrs or worse in 24 hrs,
ADD Ceftriaxone (50-75 mg/kg/d IM/IV)
• Antimalarials if blood film +
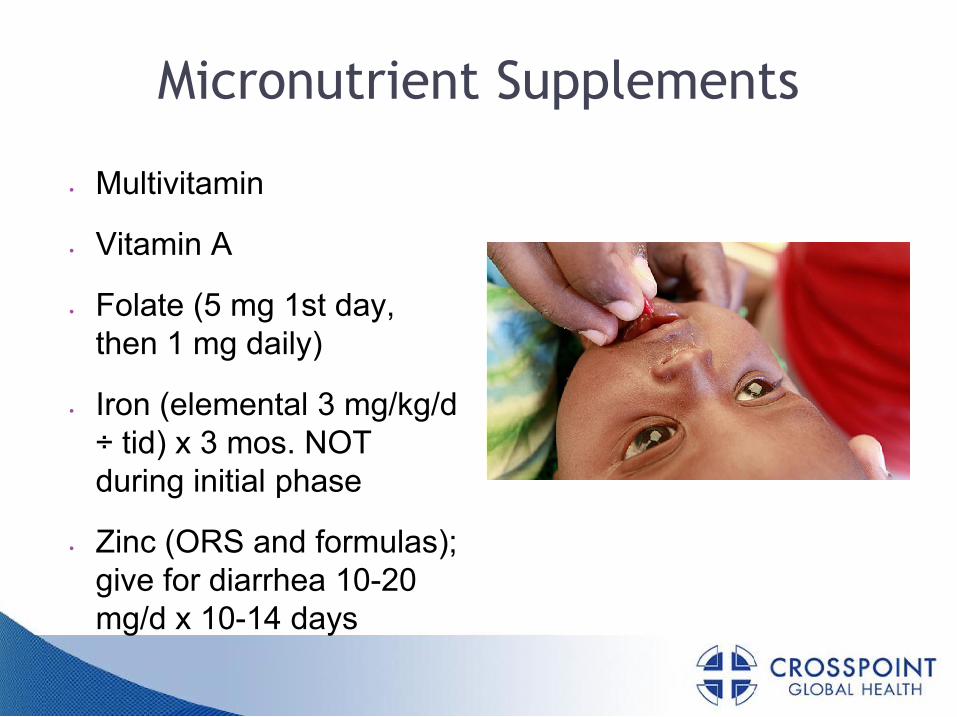
Micronutrient Supplements
• Multivitamin
• Vitamin A
• Folate (5 mg 1st day, then 1 mg daily)then 1 mg daily)
• Iron (elemental 3 mg/kg/d ÷ tid) x 3 mos. NOT during initial phase
• Zinc (ORS and formulas); give for diarrhea 10-20 mg/d x 10-14 days

Cautious Refeeding
• Begin after rehydration
• F-75 formula (75 kcal/100 ml)
• Small amounts, frequent intervalsintervals
• Cup / spoon, Dropper / syringe, or NG tube
• Intake 80-100 kcal/kg/d

Catch-up Diet
• F-100 (100 kcal/100 ml)
• Slowly increase volume to 150-220 kcal/kg/d
• Feed 5 x/d until Wt/Ht > -1 SD (> 10g/kg/d), then 3x/d
• For > 2 yo use infant formulas + local solid food with vit/mineral supplements

Sensory Stimulation
• Play programs for physical/emotional stimuli
• Cheerful environment • Cheerful environment – toys, playmates
• Physical activity or passive limb motion
• Avoid sensory deprivation

Failure to Respond
• Primary vs Secondary Failure
• Reevaluate: child, care given, records
CHECK for Infection!• CHECK for Infection!
• Causes – poor treatment facility, individual patient’s condition, insufficient food, vitamin/mineral deficiency, or malabsorption
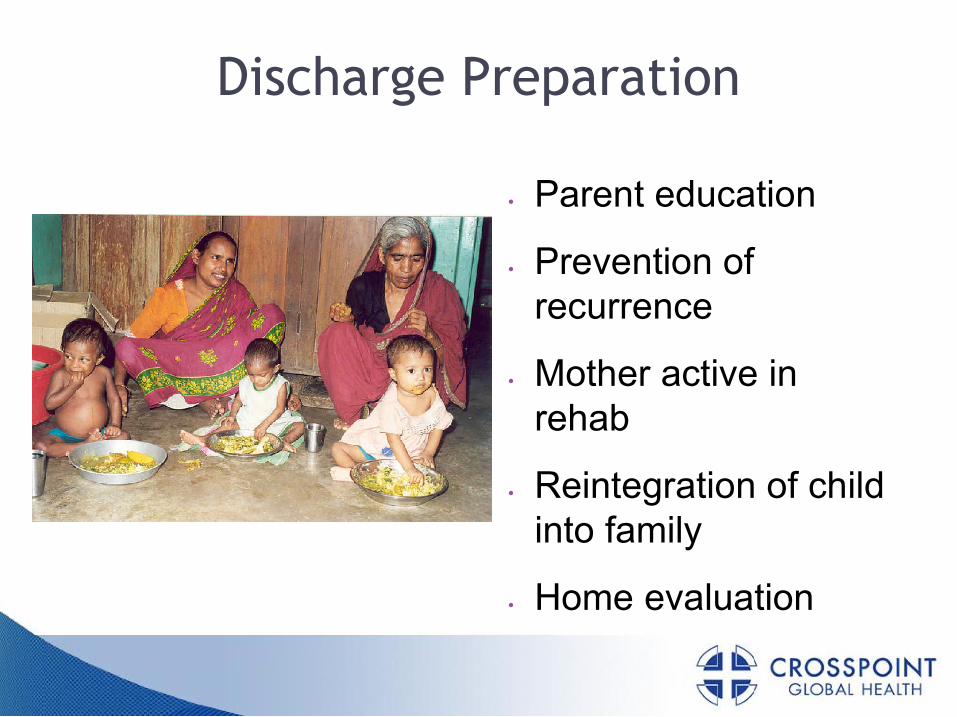
Discharge Preparation
• Parent education
• Prevention of recurrence
Mother active in • Mother active in rehab
• Reintegration of child into family
• Home evaluation

Discharge Criteria from Facility
• Clinically improved
• Wt/Ht is >-2 SD
• Treatments completed• Treatments completed
• Routine Immunizations
• Mother/caregiver willing for care
• Healthworker follow up

Follow Up
• Prevent relapse
• Biweekly initially
• Monthly until Wt/Ht Z > -1 or MUAC > 12.5 > -1 or MUAC > 12.5 cm
• Assess condition
• Treat common illness
• Counsel caregivers


Community Based Care Advantages
• Low Cost
• Decentralized
• No limits for adequate medical personnel and access to local health care services
Keys to Community Based Care
• Community involvement
• Early interventionEarly intervention
• Simple strategies and supplies
• Integrated approach
Up to Date 2013

Ready to Use Therapeutic Food
High nutritional quality
Inexpensive
Easily transportable
Minimal spoilage
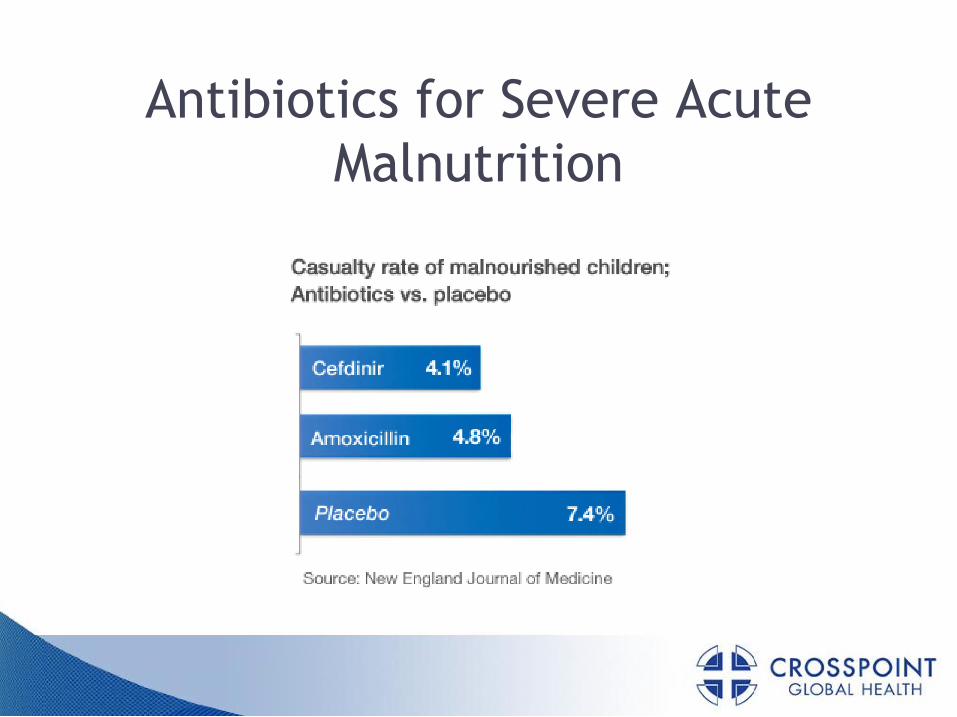
Antibiotics for Severe Acute Malnutrition

Community Based Care Results
• Used with increasing success as outpatient treatment for uncomplicated SAM
• Preferred approach for emergency relief programsprograms
• Rates
Recovery nearly 80%
Case fatality = 4.1% (=WHO protocol)
Coverage increased to 72%

Summary of Severe Acute Malnutrition Management
FACILITY BASED COMMUNITY BASED
CRITERIA • No Appetite
• Medical Complications
• Appetite
• No Medical Complications
INTERVENTION F75 -> F100/ RUTF
24 hour medical care
RUTF
Basic medical care
DISCHARGE CRITERIA
• Reduced edema
• Good appetite (acceptable intake of RUTF)
15-20% Weight Gain
From WHO/UNICEF Joint Statement 2011
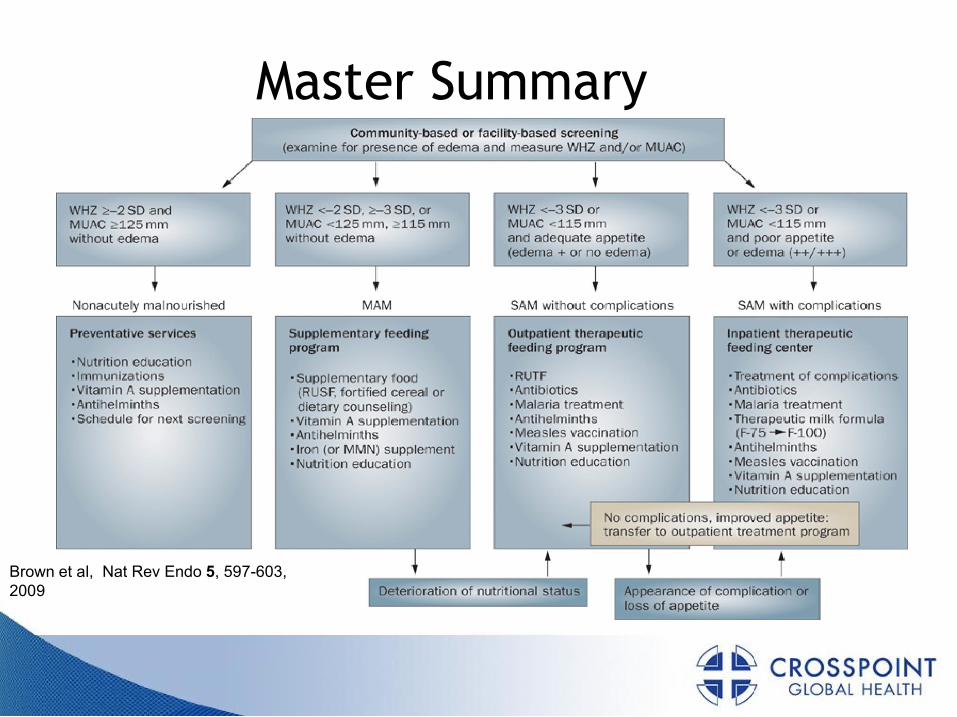
Master Summary
Brown et al, Nat Rev Endo 5, 597-603, 2009

Comments and Questions
Visit our website at www.crosspointglobalhealth.org









![The Pursuit of a Pestilence - American Antiquarian SocietyI9SO-] THE PURSUIT OF A PESTILENCE 23 not only that diphtheria was not a "new" disease as was sup-posed, but also as proof](https://img.pdfslide.us/doc/110x75/5f933a7c8a8be36ace252898/the-pursuit-of-a-pestilence-american-antiquarian-society-i9so-the-pursuit-of.jpg)