Embed Size (px)
DESCRIPTION
http://www.hepatitisfoundation.org.nz/files/6113/6547/8383/Talking_hep_C_final_for_print_single_pages.pdf
Citation preview

Are you ready for treatment? How to tell when the time is right I What do your fi ngernails say about you? I Rena Owen shares her story
talkingheptalkingheptalkingtalkingtalkinghephepheptalkinghepSummer 2012/13: Edition 03

The end of the year is nigh, and what a year it has been!
From my perspective, one of the highlights has been seeing an increasing level of commitment from the government to confront viral hepatitis - particularly hepatitis C - in New Zealand. In September this year, Hon. Tony Ryall, Minister of Health, opened the 8th Australasian Viral Hepatitis Conference asking health services to improve early diagnosis and
treatment (see page 7). Associate Minister of Health, Hon. Jo Goodhew, spoke at World Hepatitis Day remarking: “we need to face this issue head on.” To drive change, it is essential we get policy-makers on board, and it looks like we are well on the way to achieving this.
Another highlight has been the launch of this magazine: talking hep C. We have received such positive feedback from our readers; it is encouraging to hear your comments, and we hope to continue providing you with an enjoyable read.
Looking forward to next year, our pilot will be in full swing in the Bay of Plenty, Wellington, Hutt Valley, and Wairarapa. We will be actively identifying people living with hepatitis C, to give them the support they need.
I hope you’ve had a rewarding year, and can fi nd time to relax over the holiday break with your loved ones. The Hepatitis Foundation of New Zealand staff will be taking a well-deserved break, and the offi ces will be closing for two weeks over Christmas (returning Monday 7th January 2013).
From all the team at the Foundation, we wish you and your family a very Merry Christmas and a Happy New Year.
Publisher: The Hepatitis Foundation
of New Zealand
Editor/Design/Production:Kate Perkins
Copy Editor:Matt Walker
Editorial Contributors:Professor Ed Gane
Dr Frank WeilertAnn HornellMatt Walker
Clare Chapman
Website: www.hepatitisfoundation.org.nz
Mailing Address: PO Box 15 347
Tauranga New Zealand
Phone:+64 7 579 0923
Hepatitis Helpline:0800 33 20 10
Contact Talking Hep C:[email protected]
talking hep
The Hepatitis Foundation of New Zealand is a charitable trust governed by a board of trustees.
The Foundation is currently working in partnership with the
Ministry of Health to improve hepatitis C services in New Zealand.
John Hornell
Chief Executive Offi cer
The Hepatitis Foundation of New Zealand
Talking hep C is a quarterly publication, released in summer, autumn, winter, and spring. For more information about publication dates, contributions, or advertising, email [email protected].
The views expressed in this magazine are not necessarily the views of The Hepatitis Foundation of New Zealand, or any of the contributors to this publication.
Some of the people shown in this magazine are taken from online image libraries such as www.shutterstock.com. The people in these images have no connection to hepatitis or the Foundation.
While the publisher is happy for content from this publication to be reprinted, please seek permission from The Hepatitis Foundation of New Zealand before doing so. Any information that is reprinted or reproduced must acknowledge talking hep C, and the edition number and date.
No images are to be reprinted.

contents
page 3
Errors in Spring 2012 edition
We apologise for a number of mistakes printed in the previous edition of talking hep C, due to clerical errors.
In Q and A, page 15, the article answered a question on the most common ways of contracting hepatitis C. While this article correctly identifi ed some of the risk factors associated with contraction of hepatitis C, it omitted the following risk factors: people who have ever injected drugs, people who have ever received a tattoo or body piercing using unsterile equipment, and people born to mothers who were infected with hepatitis C.
Additional errors were found on pages 4, 6, 7, and 8.
The Foundation apologises for any inconvenience these errors may have caused, and would like to reassure its readers every eff ort is made to identify errors before they go to print.
errors
5What do your fingernails say about you?
9The great Christmas expedition
10If sharing my story saves just one life then why keep it a secret?
Once Were Warriors actress, Rena Owen, shares her story
News.......................................................................
Fast facts: clinical trials.....................................
Hep C pilot update...........................................
The great Christmas expedition...................
Personal story: Rena Owen.............................
Research...............................................................
Personal story.....................................................
Christchurch community clinic.....................
Q and A.................................................................
Personal story......................................................
Feature: Are you ready for treatment?..........
All that jargon.....................................................
Letters to the editor..........................................
Editorial: FibroScan®..........................................
Introducing: The Foundation’s hepatitis
B and C nurses......................................................
Contacts and support......................................
4
4
8
9
10
12
13
14
14
15
16
18
18
18
19
20

news
The medicinal characteristics of frankincense – useful or not?For centuries, frankincense has been regarded as a valuable healing substance, both on a spiritual and medicinal level. The role of frankincense appears in The Bible, in ancient Egyptian temples, in ancient Greek history, and throughout time as a valuable commodity.
Obtained from the resin of Boswellia trees, frankincense is used in many cultures for its medicinal purposes, including as an antiseptic, stimulant, astringent, anti-arthritic, and expectorant.
Professor Oliver Werz, of Friedrich-Schiller-Universität Jena, found the resin from the trunk of the Boswellia tree has anti-infl ammatory properties. This discovery has gained the attention of health professionals worldwide, particularly for use in combating infl ammatory diseases, including hepatitis C.
“Boswellic acids interact with several diff erent proteins that are part of infl ammatory reactions, but most of all with an enzyme which is responsible for the synthesis of prostaglandin E2,” Werz said.
The Journal of Virology (2005) reported levels of prostaglandin E2 were elevated in cells infected with hepatitis C, and a natural substance capable of blocking prostaglandin E2 would be a positive leap forward in hepatitis C therapeutics.
To date, there is not enough evidence to recommend the use of frankincense in hepatitis C therapy. It is advised people living with hepatitis C should focus on substances scientifi cally proven to work.
In terms of frankincense, and its eff ect on the hepatitis C virus… watch this space.
For centuries, frankincense has been regarded as a valuable healing substance, both on a spiritual and medicinal level. The role of frankincense appears in in ancient Greek history, and throughout time as a valuable commodity.
Obtained from the resin of Boswellia trees, frankincense is used in many cultures for its medicinal purposes, including as an antiseptic, stimulant, astringent, anti-arthritic, and expectorant.
Professor Oliver Werz, of Friedrich-Schiller-Universität Jena, found the resin from the trunk of the Boswellia tree has anti-infl ammatory properties. This discovery has gained the attention of health professionals worldwide, particularly for use in combating infl ammatory diseases, including hepatitis C.
“Boswellic acids interact with several diff erent proteins that are part of infl ammatory reactions, but most of all with an enzyme which is responsible for the synthesis of prostaglandin E2,” Werz said.
In November, top clinicians worldwide met in Boston for The Liver Meeting®, the 63rd annual meeting of the American Association for the Study of Liver Disease (AASLD). Central to the meeting was the release of results from hepatitis C clinical trials.
“There is signifi cant unmet medical need for genotype 1, the most common form of HCV in the U.S and Europe,” said Kris Kowdley, Director of the Liver Centre of Excellence at Virginia Mason Medical Centre.
“[Results] suggest that sustained virological response can be achieved without interferon in a high proportion of genotype 1 patients, including patients who have not responded to previous treatment. This is exciting news.”
Findings from the Abbott Phase IIb trial show sustained virological response at 12 weeks post-treatment in 97 per cent of treatment-naïve patients and 93 per cent in null-responders. Gilead Sciences found 100 per cent of participants with genotype 1 achieved a sustained virological response four weeks post-treatment.
“It appears we are moving closer to potential oral treatment regimens that do not require interferon to treat hepatitis C,” Kris said.
For the full story, visit www.hepatitisfoundation.org.nz (research section) or call 0800 33 20 10.
fast facts: clinical trials
Clinical trials involving new drugs are usually categorised into four phases. Each phase is considered a separate clinical trial.
Phase III
20 - 80 participants test the drug or treatment for the fi rst time.Purpose: To test safety, dosage, and identify side eff ects.
100 - 300 participants.Purpose: To further test safety and eff ectiveness.
1,000 - 3,000 participants.Purpose: Confi rms eff ectiveness, monitors side eff ects, and data collection.
Post-marketing studies defi ne additional information, such as treatment risks, benefi ts, and optimal use.
Latest developments in interferon-free HCV treatment
Phase II
Phase I
Phase IV

Clinical study in New Zealand looking for participants
Auckland Clinical Studies (investigator: Professor Ed Gane) and Christchurch Clinical Studies (investigator: Catherine Stedman) are dedicated, state of the art, clinical trial units, which have recently conducted ground-breaking research in the development of all-oral, interferon-free, treatments for hepatitis C.
They are currently running a very exciting study of 12 weeks’ treatment with two oral drugs, which have demonstrated high response rates and are very well tolerated in people with hepatitis C.
They are off ering this to patients who are infected with HCV genotype 1 (both 1a and 1b, cirrhotic or non-cirrhotic) who have been treated since 2004 with pegylated interferon and ribavirin for at least 12 weeks, and are non-responders to treatment.
If you fi t the above criteria, please contact Vithika (in Auckland) on 09 373 3474 or Chris (in Christchurch) on 03 372 9477 to fi nd out more.
Changes in fingernail appearance may indicate liver damageFingernail abnormalities may expose details about internal health, including the performance of the liver.
Changes in the colour, texture, or shape of fi ngernails may be an indicator of internal health problems. Pale nails, clubbing (enlargement of the fi ngertips), double white lines running horizontally, or a dark band at the tip of the nail may indicate liver disease or reduced liver health.
According to a report in the Journal of the European Academy of Dermatology and Venereology (2010), changes in fi ngernails were frequently observed in people with liver cirrhosis, and viral hepatitis B and C infections.
While the appearance of fi ngernails may often change, sustained changes in appearance or abnormalities (as listed above), should be reported to a health professional.
(in Christchurch) on 03 372 9477 to fi nd out more.
news
page 5
Listen to the Foundation’s hepatitis C podcast series at HepCentral -www.hepatitisfoundation.org.nz/podcasts
Predictive variables of a major depressive episode during treatmentA Spanish study found a quarter of people who undergo treatment using pegylated interferon and ribavirin developed a major depressive episode.
People who presented with one or more specifi c factors were more likely to develop a major depressive episode during treatment. These factors included: high baseline levels of interleukin (a type of protein for regulating immune responses), history of a major depressive episode or psychiatric disorder, subthreshold depressive symptoms, low educational level, and female sex.
Researchers advised clinicians to undertake full evaluation of patients prior to antiviral treatment, to identify those at risk of developing interferon-induced depression.Reference: Udina M et al. Interferon-induced depression in chronic hepatitis C: a systematic review and meta-analysis. J Clin Psychiatry 73(8). doi: 10.4088/JCP.12r07694, 2012.

HCV treatment may reduce risk of liver cancerResearchers at Copenhagen University found the use of antiviral drugs to treat hepatitis C may greatly reduce the risk of liver cancer.
Participants of the study were monitored for between fi ve and eight years after interferon and/or ribavirin treatment, along with 1,200 people who did not receive treatment.
The researchers found that antiviral therapy reduced the risk of liver cancer by 47 per cent.
“This study confi rms something that most of us who treat hepatitis C knew on a gut level, but had never seen demonstrated so eff ectively,” said Dr Douglas Dieterich, Professor of Liver Diseases at Mount Sinai School of Medicine.
Five other studies were reviewed by the Danish researchers, which found antiviral treatment reducing the risk of liver cancer by 70 per cent.
“If we are able to extrapolate this data to the newer approved stand-of-care therapies, which have sustained viral response rates of greater than 70 per cent, one would expect these results would be even better in preventing the development of primary liver cancer,” said Dr David Bernstein, Chief of the Division of Hepatology at North Shore University Hospital. These improved outcomes “should encourage physicians to treat patients with advance fi brosis and cirrhosis, and encourage those patients to seek out therapy,” he added.
Findings published in BMJ Open 2012; 2: e001313.
Keep up-to-date with the latest hepatitis C news and research at HepCentral - www.hepatitisfoundation.org.nz
news
People who inject drugs can be successfully treated with hepatitis C and HIV co-infectionHepatitis C can be treated successfully for people with a history of injecting drug use, regardless of HIV status, researchers reported at the 52nd Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC 2012) in September 2012.
Researchers at the University of British Columbia investigated responses to hepatitis C treatment between 2003 and 2012 at two clinics in Vancouver. All study participants had a history of injecting drug use.
Sustained virological response rates among HCV mono-infected participants were 45 per cent for genotype 1, and 65 per cent for genotype 2 and 3, while HCV/HIV co-infected participant response rates were 42 per cent and 60 per cent respectively. The study found response rates to hepatitis C treatment were not signifi cantly diff erent for people living with or without HIV.
Reference: H Tossonian, L Gallagher, S Nouch, et al. Long-term Follow-up of Inner City Populations Treated for HCV Infection. 52nd Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC 2012). San Francisco. September 9-12, 2012. Abstract V-371.
Vitamin D linked to improved response to treatmentAustrian researchers found people who are co-infected with hepatitis C and HIV, who have a defi ciency in vitamin D, had a poorer response to hepatitis C treatment. An AIDS article reported people with this vitamin D defi ciency were signifi cantly less likely to have an early or sustained virological response to treatment than those with normal levels of the vitamin.
“Vitamin D supplementation may result in higher rates of virologic response in HCV/HIV co-infected patients”, an investigator from AIDS said.
Vitamin D acts as an antiviral agent, impeding production of hepatitis C. People living with hepatitis C, who have suffi cient levels of vitamin D, have been known to have improved response rates to treatment with pegylated interferon and ribavirin.
Previous research has found a high prevalence of vitamin D defi ciency in people co-infected with hepatitis C and HIV.
Reference: Mandorfer M et al. Low vitamin D levels are associated with impaired virologic response to PEGIFN+RBV therapy in HIV/HCV coinfected patients. AIDS 26, online edition. doi: 10.1097/QAD.0b013e32835aa161, 2012.

page 7
news
September 2012: Working towards working together was raised as a way of moving forward in the successful management of chronic hepatitis in New Zealand during the 2012 Australasian Viral Hepatitis Conference.
In his speech at the conference’s opening ceremony, Health Minister, Hon Tony Ryall said the government was continuing to build on services already in place to stop the spread of viral hepatitis.
He spoke of an integrated approach to tackling the virus, and said the management of hepatitis B and C in New Zealand in the future would depend on the integration of services.
Deputy Director of the New Zealand Liver Transplant Unit at Auckland Hospital, Professor Ed Gane, reported that 2,000 people died last year in Australia and New Zealand as a result of viral hepatitis.
“This will treble by 2030,” he said.
“There is hope. This is an incredibly exciting time for all of us who manage patients with viral hepatitis.”
“Our countries have led the world in the battle against viral hepatitis. Australia has led the world in research and modelling of the hepatitis C epidemic. “
“Working together, we can win the battle against chronic hepatitis,” he said.
New Zealand actress Rena Owen spoke publicly about her battle with hepatitis C for the first time at the conference.
“We need to raise awareness, and change the current low levels of diagnosis and treatment,” she said.
Hepatitis C Programme Manager for The Hepatitis Foundation of New Zealand, Kelly Barclay, said, with the launch of the Hepatitis C Pilot in four DHB areas, the first green shoots were appearing.
“The pilot will incorporate the Community Assessment and Support Programme which will provide an integrated approach to hepatitis C management, bringing services into the community, and ensuring more services are accessible to more patients,” he said.
“We are also launching a concerted campaign to increase awareness about hepatitis C in New Zealand.”
“The pilot’s integrated approach is a first for New Zealand, and we hope, with the two-year pilot, to provide a benchmark for the roll-out of a national programme,” he said.
More than 600 delegates from around the world attended the conference, including health professionals, patients, and representatives of community organisations.
Written by Clare Chapman.
Working towards working together in viral hepatitisAt the 2012 Australasian Viral Hepatitis Conference, an integrated approach to care emerged as a common theme for the future success of chronic hepatitis management.

hep C pilot update
page 9
“This is a new model of care; an exciting model of care,” said Professor Ed Gane (Ministry of Health Champion for Hepatitis C) as he gave the opening address at the launch of the Hepatitis C Pilot. “[This pilot] will take assessment out of secondary care and into the community. By doing so, we think we’ll overcome some of the barriers for people going to hospital.”
Health professionals and service providers came together to celebrate the launch of the Hepatitis C Pilot in the two pilot regions. John Hornell, Chief Executive of The Hepatitis Foundation of New Zealand, spoke to those who attended, saying, “The Foundation is now
piloting an innovative programme to address hepatitis C. By the end of tonight, I hope you will leave here with a greater understanding of what we want to achieve, and commit to supporting this programme.”
The aim of the launch events were to educate key professionals in the community about hepatitis C and the pilot. Attendees included staff from the Ministry of Health, District Health Boards, Needle Exchange, CADS, and doctors and nurses from the region.
Dr Frank Weilert, Director of Endoscopy at Waikato District Health Board said, “I encourage you all to get involved.” Dr Massimo Giola, Infectious Diseases Physician at Tauranga Hospital agreed, saying, “These are really exciting times for the care of hepatitis C.”
Dr Jeff Wong, Gastroenterologist at Hutt Hospital, spoke of the benefi ts of the portable FibroScan® machine available in a community setting, and the need to fi nd people who are unaware they are living with the disease.
The Hepatitis C Pilot will operate in two regions: the Bay of Plenty and greater Wellington area, which includes the Hutt Valley and Wairarapa. The aim of the pilot is to improve health outcomes for people living with hepatitis C through increasing the number of people diagnosed, assessed, and off ered treatment and support.
The slogan of the pilot is: ‘Hepatitis C. Know it. Test it. Treat it.’ This message came across loud and clear to health professionals and service providers in the regions.
The pilot will continue until June 2014, culminating in a national action plan for hepatitis C for 2015 - 2020.
The Hepatitis C Pilot has offi cially launched with health professionals and service providers in the pilot regions.
for 2015 - 2020.
page 8

The great Christmas expedition...
Join the online chat forum at www.hepatitisfoundation.org.nz and write a Christmas greeting!
1
2
Go to our facebook page www.facebook.com/hepCentral.
Upload a picture of yourself to become one of the
100 faces of hepatitis C
in New Zealand.
4
Join twitter at www.twitter.com/Hep_Central.
Send us a Christmas message for your loved ones and we will post it
on our twitter page.
5Have a safe, enjoyable Christmas with your family and friends.
3
Share your story with the world! Send us your hepatitis
C story or a video of your experience to help others
living with hepatitis C.

F
Rena Owen is an international award-winning actress, who is best known in New Zealand for her role as Beth in the 1994 fi lm, Once Were Warriors.
had been in her system for about 30 years, it started to take its toll on her health and wellbeing.
“I was getting sick,” she said. “I was too skinny and couldn’t keep any weight on due to chronic night sweats. I often felt like I had the fl u and suff ered chronic fatigue because my liver was constantly working over time.”
In late 2010, Professor Gane invited her onto a new drug trial run.
“It was time to get treated. According to a FibroScan®, I had mild liver scarring due to hepatitis C, but I also turned 50 that year. Age makes a diff erence to the condition of our internal organs, and the longer hepatitis C is in one’s system the more virulent it becomes.”
“But by week four of the 12-week treatment, I wanted out of the trial,” she said.
“That interferon makes you gaga. You are in another zone. I kept my sanity by going in the bush, getting out in the water. I had a lot of energy throughout the trial, but I couldn’t sleep. The great thing about this trial was we all knew by week three our viral load had considerably reduced.”
Rena has now been clear of the virus for nearly two years, and is back in good spirits and physical health.
To this day, Rena is unsure how she got the blood-borne hepatitis C virus, but she has narrowed it down to a few possible sources.
“I started my hospital based nursing training in 1979 and qualifi ed as a registered nurse in early 1982.”
“In the early ‘80s I also had a tattoo and multiple ear piercings, and I got into IV drug use. Hepatitis C and HIV weren’t known about back then,” she said.
Rena recently spoke publicly of her battle with hepatitis C for the fi rst time.
“If sharing my story saves just one life then why keep it a secret?” she said.
“It is an insidious virus that does not discriminate. It shows no mercy. I was lucky because I found out I was positive and had the chance to do something about it.”
“It was nerve-wracking speaking about it, but the more people who think they might be at risk, and go and get checked for it, the better. We need to raise awareness and change the current low levels of diagnosis and treatment.”
“I have been aff orded the gift of life, and for that gift I am profoundly and eternally grateful.”
ive years after telling Jake the Muss to cook his own eggs in the role that shot her to international fame, Rena Owen was in the middle of cooking eggs for an old friend when she realised something wasn’t right.
It was the late 1990s, and Rena was in Brisbane fi lming a television series for Channel 7. She had a friend from the Bay of Islands and his girlfriend visit for a Bledisloe Cup game. Following an All Black victory, they attended the offi cial after-match party.
“Because of Once Were Warriors and the fame, I got bought drinks all night,” she said.
Rena was thrust into the international spotlight after Once Were Warriors premiered at the Cannes Film Festival while opening in New Zealand on the same day.
“I was ill-prepared, and wasn’t coping with the instant fame. I thought no-one would recognise me and I couldn’t cope with the pressure that came with being in the public eye,” she said. “Alcohol gave me a fake confi dence, but drinking was ultimately self-destructive. I wasn’t a seasoned drinker so it went straight to my head and I made a fool of myself.”
“The [All Blacks after party] was a big one for me. The next day, I got up and cooked my friends some breakfast.”
“I cooked eggs. They were hung over, but I was sick as a dog. I was literally lying in bed sweating. I just knew this was not a normal hang over and something was wrong.”
Rena went to the doctor the following week and tests showed she had hepatitis C.
“I was shocked. I was angry. I thought: What the f__ are you talking about?”
“I had no idea about hepatitis C; I didn’t even know it existed.”
Because Rena used IV drugs between 1982 and 1984, she got annual blood tests for HIV and hepatitis (between 1985 and 1988) but the results were always negative so she thought she was out of the woods. “I later learnt the hepatitis strands had only been separated and identifi ed in the late ‘80s.”
When Rena returned to New Zealand in 1999, she was referred to Auckland liver specialist, Professor Ed Gane.
“I did my fi rst liver biopsy and there was no scarring, but I had a fatty liver, which is a precursor to scarring.”
After discussing treatment options, Rena chose to take care of her liver while waiting for better treatment options. She had already curbed her drinking and was refocused on work, but she had to be even more disciplined.
“I kept alcohol consumption to a minimum, but I did have the odd moments of being human, at Christmases and birthdays, and that sort of thing.”
Rena continued to eat wholesome fresh food, take supplements, and be physically active. But after the virus
I just knew this was not a normal hang over...
If sharing my story saves just one life then why keep it a secret?

personal story
page 11
Aresearch
European liver patient organisation releases consensus statement on mental health and treatment for hepatitis C.
By Matt Walker
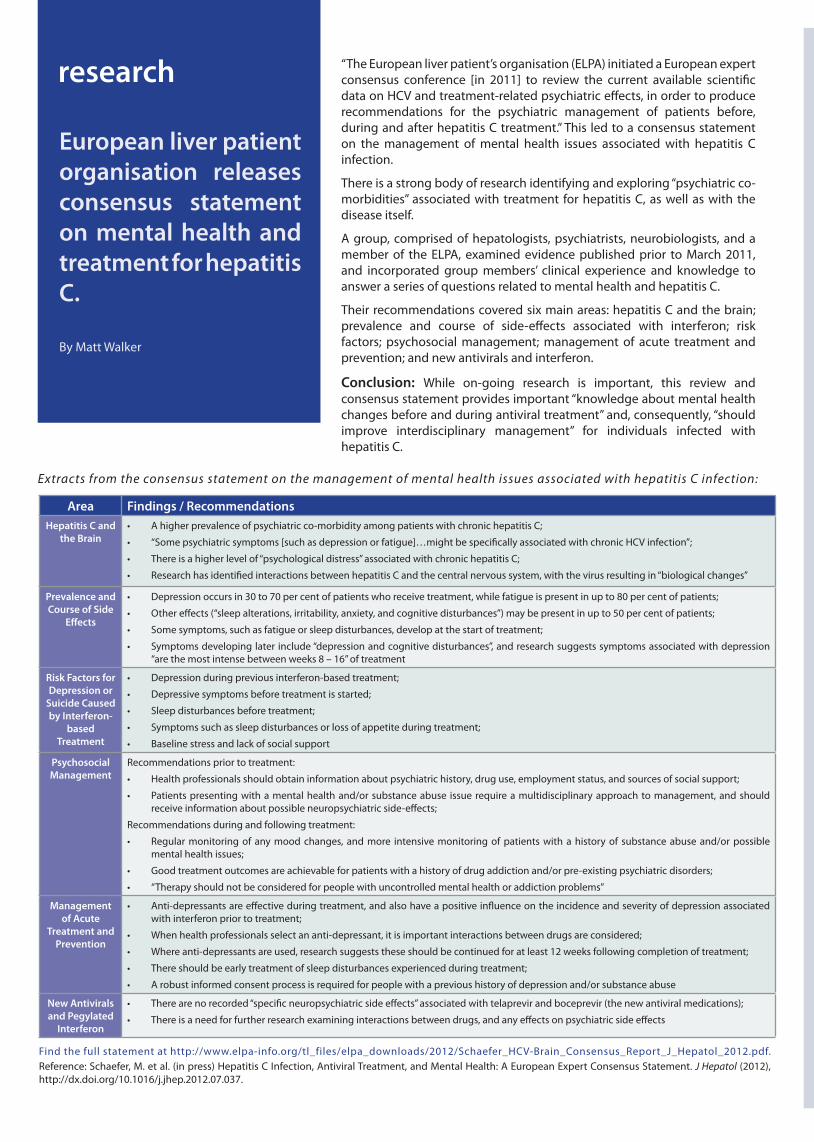
“The European liver patient’s organisation (ELPA) initiated a European expert consensus conference [in 2011] to review the current available scientific data on HCV and treatment-related psychiatric effects, in order to produce recommendations for the psychiatric management of patients before, during and after hepatitis C treatment.” This led to a consensus statement on the management of mental health issues associated with hepatitis C infection.
There is a strong body of research identifying and exploring “psychiatric co-morbidities” associated with treatment for hepatitis C, as well as with the disease itself.
A group, comprised of hepatologists, psychiatrists, neurobiologists, and a member of the ELPA, examined evidence published prior to March 2011, and incorporated group members’ clinical experience and knowledge to answer a series of questions related to mental health and hepatitis C.
Their recommendations covered six main areas: hepatitis C and the brain; prevalence and course of side-effects associated with interferon; risk factors; psychosocial management; management of acute treatment and prevention; and new antivirals and interferon.
Conclusion: While on-going research is important, this review and consensus statement provides important “knowledge about mental health changes before and during antiviral treatment” and, consequently, “should improve interdisciplinary management” for individuals infected with hepatitis C.
Area Findings / RecommendationsHepatitis C and
the Brain• A higher prevalence of psychiatric co-morbidity among patients with chronic hepatitis C;
• “Some psychiatric symptoms [such as depression or fatigue]…might be specifically associated with chronic HCV infection”;
• There is a higher level of “psychological distress” associated with chronic hepatitis C;
• Research has identified interactions between hepatitis C and the central nervous system, with the virus resulting in “biological changes”
Prevalence and Course of Side
Effects
• Depression occurs in 30 to 70 per cent of patients who receive treatment, while fatigue is present in up to 80 per cent of patients;
• Other effects (“sleep alterations, irritability, anxiety, and cognitive disturbances”) may be present in up to 50 per cent of patients;
• Some symptoms, such as fatigue or sleep disturbances, develop at the start of treatment;
• Symptoms developing later include “depression and cognitive disturbances”, and research suggests symptoms associated with depression “are the most intense between weeks 8 – 16” of treatment
Risk Factors for Depression or
Suicide Caused by Interferon-
based Treatment
• Depression during previous interferon-based treatment;
• Depressive symptoms before treatment is started;
• Sleep disturbances before treatment;
• Symptoms such as sleep disturbances or loss of appetite during treatment;
• Baseline stress and lack of social support
Psychosocial Management
Recommendations prior to treatment:
• Health professionals should obtain information about psychiatric history, drug use, employment status, and sources of social support;
• Patients presenting with a mental health and/or substance abuse issue require a multidisciplinary approach to management, and should receive information about possible neuropsychiatric side-effects;
Recommendations during and following treatment:
• Regular monitoring of any mood changes, and more intensive monitoring of patients with a history of substance abuse and/or possible mental health issues;
• Good treatment outcomes are achievable for patients with a history of drug addiction and/or pre-existing psychiatric disorders;
• “Therapy should not be considered for people with uncontrolled mental health or addiction problems”
Management of Acute
Treatment and Prevention
• Anti-depressants are effective during treatment, and also have a positive influence on the incidence and severity of depression associated with interferon prior to treatment;
• When health professionals select an anti-depressant, it is important interactions between drugs are considered;
• Where anti-depressants are used, research suggests these should be continued for at least 12 weeks following completion of treatment;
• There should be early treatment of sleep disturbances experienced during treatment;
• A robust informed consent process is required for people with a previous history of depression and/or substance abuse
New Antivirals and Pegylated
Interferon
• There are no recorded “specific neuropsychiatric side effects” associated with telaprevir and boceprevir (the new antiviral medications);
• There is a need for further research examining interactions between drugs, and any effects on psychiatric side effects
Extracts from the consensus statement on the management of mental health issues associated with hepatitis C infection:
Find the full statement at http://www.elpa-info.org/tl_files/elpa_downloads/2012/Schaefer_HCV-Brain_Consensus_Report_J_Hepatol_2012.pdf.Reference: Schaefer, M. et al. (in press) Hepatitis C Infection, Antiviral Treatment, and Mental Health: A European Expert Consensus Statement. J Hepatol (2012), http://dx.doi.org/10.1016/j.jhep.2012.07.037.

personal storyAndrew saw himself as a bit of a hippie. He smoked weed now and again, and hung out with a crowd who occasionally dabbled in harder drugs.
Dealing with low self-confi dence and stray feelings of depression, Andrew took a friend up on an off er to try injecting a drug. He was in his early twenties.
“The drugs like that made me feel like I was bullet proof. They made the problems go away,” he said.
“I was on and off drugs until I was about 28 or 29.”
“Then I met my wife and I haven’t touched them since.”
Andrew had never heard of hepatitis C when he was doing drugs. “I had no idea it could kill you, I didn’t even know what it was or how you could get it,” he said.
Now aged 60, Andrew is acutely aware of the virus and the damage it can do if it goes undiagnosed.
“I found out I had it when I was 57. I have been told I could have had it for 30 or 40 years.”
Although Andrew felt generally well throughout most of his life post-drugs, he caught Dengue Fever during a trip to the Pacifi c Islands a few years ago, and, since then, has noticed his health deteriorating.
“I was then diagnosed with high iron content (haemochromatosis). It caused dizziness and I often felt sick.”
“I was living in Whakatane at this time and I just started feeling worse and worse. I started feeling very tired and generally run down, and then depressed.”
“My doctor couldn’t work out what was wrong with me. I ended up changing doctors and started getting blood taken every couple of weeks to reduce the high iron content.”
“When this didn’t make me feel better, a nurse mentioned she thought something else was wrong with me and I got tested for hepatitis C.”
“It took one and a half years before I got to the root of the problem.”
Andrew was then referred to The Hepatitis Foundation of New Zealand and discussed his options. He went through a 48-week course of treatment.
“I had a bad reaction to the treatment, but just because I did, it doesn’t mean someone else will,” he said.“I started to get really bad mood swings and depression. It was awful.”Andrew’s dose was adjusted early into the course of treatment, but he continued to struggle with a number of side eff ects.“I couldn’t have got through those 48 weeks without Ann’s (hepatitis nurse) constant encouragement and advice.”
“I will always be really thankful to her.”
Andrew kept his hepatitis C diagnosis from his colleagues, and initially from his friends and family as well.
“I just felt there was a bit of a stigma attached to it. Everyone thinks ‘druggie’, which is not the case.”
After fi nishing treatment and getting a blood test in late December to confi rm whether the treatment was successful, Andrew spent the holiday period anxiously waiting for his results while the labs were closed.
“Ann rang me up one day. I had been waiting. I could tell she was pretty upset. I could just tell in her voice,” he said.
“It just hit me like a brick wall. I got quite upset. That really sort of knocked me back.”
Unfortunately Andrew’s body did not respond to the treatment and the virus remains active in his liver.
“My body just couldn’t handle the interferon part of the treatment.“
“Now I’m looking at other options. There is a trial up in Auckland I’m waiting to hear if I can get on next year; they are trialling drugs without interferon so I’m hoping to get onto that.”
“I reacted badly to the treatment, especially with depression and mood swings. But that doesn’t
mean everybody does. I think possibly I have been depressed most of my life and what treatment did was exaggerate it.”
Andrew is now looking forward to other options and enjoying feeling well again; his main regret is he didn’t get checked and diagnosed earlier.
“If there is any doubt, go and get it checked right away,” he said.
“You are messing about with your life if you don’t. It’s not worth it.”
Andrew wants to tell his story to make people more aware of the importance of getting tested earlier than he was.
“If I can help someone get diagnosed before their disease is too advanced, then it will have been more than worth it.”
Area Findings / RecommendationsHepatitis C and
the Brain• A higher prevalence of psychiatric co-morbidity among patients with chronic hepatitis C;
• “Some psychiatric symptoms [such as depression or fatigue]…might be specifi cally associated with chronic HCV infection”;
• There is a higher level of “psychological distress” associated with chronic hepatitis C;
• Research has identifi ed interactions between hepatitis C and the central nervous system, with the virus resulting in “biological changes”
Prevalence and Course of Side
Eff ects
• Depression occurs in 30 to 70 per cent of patients who receive treatment, while fatigue is present in up to 80 per cent of patients;
• Other eff ects (“sleep alterations, irritability, anxiety, and cognitive disturbances”) may be present in up to 50 per cent of patients;
• Some symptoms, such as fatigue or sleep disturbances, develop at the start of treatment;
• Symptoms developing later include “depression and cognitive disturbances”, and research suggests symptoms associated with depression “are the most intense between weeks 8 – 16” of treatment
Risk Factors for Depression or
Suicide Caused by Interferon-
based Treatment
• Depression during previous interferon-based treatment;
• Depressive symptoms before treatment is started;
• Sleep disturbances before treatment;
• Symptoms such as sleep disturbances or loss of appetite during treatment;
• Baseline stress and lack of social support
Psychosocial Management
Recommendations prior to treatment:
• Health professionals should obtain information about psychiatric history, drug use, employment status, and sources of social support;
• Patients presenting with a mental health and/or substance abuse issue require a multidisciplinary approach to management, and should receive information about possible neuropsychiatric side-eff ects;
Recommendations during and following treatment:
• Regular monitoring of any mood changes, and more intensive monitoring of patients with a history of substance abuse and/or possible mental health issues;
• Good treatment outcomes are achievable for patients with a history of drug addiction and/or pre-existing psychiatric disorders;
• “Therapy should not be considered for people with uncontrolled mental health or addiction problems”
Management of Acute
Treatment and Prevention
• Anti-depressants are eff ective during treatment, and also have a positive infl uence on the incidence and severity of depression associated with interferon prior to treatment;
• When health professionals select an anti-depressant, it is important interactions between drugs are considered;
• Where anti-depressants are used, research suggests these should be continued for at least 12 weeks following completion of treatment;
• There should be early treatment of sleep disturbances experienced during treatment;
• A robust informed consent process is required for people with a previous history of depression and/or substance abuse
New Antivirals and Pegylated
Interferon
• There are no recorded “specifi c neuropsychiatric side eff ects” associated with telaprevir and boceprevir (the new antiviral medications);
• There is a need for further research examining interactions between drugs, and any eff ects on psychiatric side eff ects
page 13
Names have been changed in this story to respect the subject’s privacy.
If I can help someone get diagnosed before their disease is too advanced, then it will have been more than worth it.

Contact Talking Hep C. Email us at [email protected]
profi le
?q and a
q and a
While aftershocks rocked the city, hepatitis C patients and staff at the Hepatitis C Community Clinic in Christchurch required fl exibility and a lot of Kiwi ingenuity. As the city reeled, the nurse at the clinic, Jenny Bourke observed her patients putting hepatitis C on the
back burner.
“Clients continued to access [our services], but some were anxious, fearful ... they required a lot more support and assistance, and they needed extra help and mentoring, so, at this time, social needs came to the fore,” Jenny said.
The clinic was battered and bruised, but managed to pick itself up after a couple of days and operate as usual.
That was after the fi rst earthquake.
When the second big one hit on February 22 last year, it was a diff erent story.
The clinic’s backbone - its building - collapsed, and staff and clients alike were unable to access it when the red cordon around the city centre went up. Client fi les and the organisation’s hard drive were trapped behind the cordon, leaving a degree of inventiveness needed to rescue the essential documents.
Armed with the recovered items, Jenny and her team contacted as many clients as possible and arranged visits at their homes.
“During this time, a lot of our clients couch-surfed, while we building-surfed,” Jenny said. “They tracked us down though.”
The team moved around, setting up anywhere they could, including the clinic receptionist’s front lounge.
After the February 2011 earthquake, the number of people enrolled at the clinic increased dramatically.
“The clients were absolutely amazing.“
They had feelings of a lucky escape. If they lived through this, they could live through anything.”
“We are still continuing to grow.”
The Christchurch Hepatitis C Community Clinic is a nurse-led clinic (Jenny Bourke) that has been working with those with hepatitis C in the Christchurch community for over 3 years.
The clinic off ers services of a GP, a nurse, and a social worker, and provides testing, diagnosis, management, support, and referral to HCV treatment in a community setting. It is open to anyone in Christchurch who has been at risk of hepatitis and wants to be tested.
Jenny and her team are now based at 27 Cashel Street, Christchurch. For more information phone the Christchurch Hepatitis C Community Clinic on (03) 377 8689.
Christchurch community clinic lives on
QA
I have hepatitis C and I recently found out I was pregnant. Will it aff ect my unborn child?
It is advised you inform your midwife or obstetrician of your hepatitis C status, as they can take additional steps to prevent your baby being exposed to your blood.
Your baby will have a blood test 18 months after birth to determine whether it has hepatitis C.
If your baby is born with hepatitis C, there is a 45 per cent chance they will clear the virus naturally within the fi rst 12 months.
Being born to a mother with hepatitis C is a risk factor. However, there is a less than seven per cent chance your child will contract hepatitis C from you.
QA
I have hepatitis C and I’m not sure whether
to tell my employers. What do you think?
Legally, people living with hepatitis C are under no obligation to inform employers, unless they are a health worker who performs exposure-prone procedures, in which case you have a responsibility to disclose.
While there are a number of cases where people have been discriminated against because of their HCV status, there are also benefi ts to talking to your employer. A caring employer may
give you more fl exibility when you are on treatment or when you’re not feeling well enough to work.
You are the person in the best position to determine how your employer will react if you tell them you have hepatitis C.
Do you have a question you would like answered? Visit our website or email us at [email protected].
page 14

personal storyis mother told him to leave the family home in Auckland when he was just a young teenager.
But Edward Williams has only gratitude for the decision his mother made 31 years ago.
“My mother sent me away to sea when I was 16,” he said. “She told me I wasn’t going to get into gangs. And I thank her so much for that now. I have travelled the world on the boats.”
In 1985, Edward was in downtown Auckland during some time off from the ships, and was mugged.
“They fully fractured my forehead and across my cheek. I had a blood transfusion after that.”
Twenty five years later, Edward needed a double hip operation. ”Before they did the operation I had to have a few blood tests. It was then they found out that my liver wasn’t working properly,” Edward said.
“They informed me that I had liver disease. It was a big shock. I think I got hepatitis C from the blood transfusion in 1985,” he said. “I never went near IV drugs, I was scared of them. But I was a big drinker.”
“I always felt something was wrong. When I drank I just felt terrible the next day; it was crippling.”
Edward had to wait for nearly a year after undergoing hip surgery to start treatment for hepatitis C.
“Nicola [the hepatitis nurse] told me I had to cut out the piss, and so I did. It was hard. At friends’ places and
H barbeques, everyone is having a drink and I just had to not do it.”
“I gave up smoking for about six weeks too but I ended up back on those.”
When Edward did start treatment he wasn’t working, and had a good support person. “It was the hardest thing doing the treatment,” he said. “I went from 100kg down to 60kg while I was doing it and I was tired all the time.”
“Some days I wouldn’t even be able to get out of bed. Other days it was just ... I didn’t even want to talk, and noises were even too much. I got quick-tempered as well.”
“But I got away to the beach to walk the dogs and had time out for myself, which helped. My landlady was a good support, she has done so much for me. I was lucky.”
“After treatment, the hepatitis C wasn’t detected in my blood. It was such an awesome feeling. I was just elated, thanking the Lord. I was happy as.”
“I haven’t worked for over two years now but I feel I can take control, make my own decisions, and go back to work. I’ll do anything now, just to be back at work,” he said.
“It was definitely worth it, doing the treatment. It’s hard. You just have to hold on and have faith, and hope it is going to work.”
“I warn everyone about hep C now. I tell them, this could happen to you.”
Edward had genotype 2 hepatitis C. He is 47 and lives in Mount Maunganui. His three adult children also live in the area.
Written by Clare Chapman.
I feel I can take control, make my own decisions, and go back to work.
page 15

feature
Are you ready for treatment? How to tell when the time is right
Talking hep C sits down with Hepatologist, Dr Frank Weilert, to fi nd out when is the right time to commit to treatment.
Dr Frank Weilert explains: We are often asked as doctors to assess someone’s readiness for treatment. As hepatitis C is a chronic infection that can be cured, timing of treatment is important, as the side-eff ects and treatment options of currently funded treatments are fairly predictable.
We know most individuals will experience side-eff ects, which can be eff ectively treated. However, to be ‘ready for treatment’ is a concept revolving primarily around
attitude. You have to be ready to deal with the consequences of treatment in order to gain the ultimate prize of being cured. This is not always simplistic or limited to the eff ects of treatment, but we must consider other impacts on your daily life before recommending treatment. How does the treatment aff ect your ability to work, play, and sleep? What makes treatment possible is having good support from family, friends, work mates, and employers. Once you have eff ectively secured your support structure, you will be ready to be treated.
At this time, we can lay out a treatment plan and deal with the known side-eff ects of treatment. This is a team eff ort involving you and your family, the nurse specialist, doctor, and others. With such an approach, we have shown that very few who commit to treatment don’t complete the course. Cure is achievable even though the side-eff ects are sometimes frightening. With the right attitude and the right support - you can be ready too!
After deciding to proceed with treatment, the next diffi cult question is when?
In most cases, treatment for hepatitis C is not urgent, so you have the ability to prepare and ensure the time is right for you.
Dr Weilert recommends assessing your readiness for treatment against the following three dimensions; physical, laboratory, and social needs.
Social Physical
Laboratory (& investigations)
welcome to......Debbie Norris. Debbie is the Foundation’s friendly offi ce administrator / helpline co-ordinator at the Tauranga offi ce. She will be providing administration support for the Hepatitis C Pilot. Debbie has worked on and off with the Foundation over the past
decade and we welcome her back with open arms.
...Lorna Scoon. Lorna has joined The Hepatitis Foundation of New Zealand as our community hepatitis C nurse for the greater Wellington region. Lorna has been a registered nurse for over 20 years. During this time she has worked in corrections, and in a number of general practices in New Zealand
and overseas. We look forward to having her on our team.
page 16

Are you ready for treatment? How to tell when the time is right The laboratory (and
investigations) dimensionPrior to treatment, you will need to complete a range of blood tests. Your doctor will review the results to determine whether it is safe for you to proceed with treatment. The complete range of blood tests will be repeated at specifi c times during treatment to monitor your response. The specialist nurse will advise if any dose adjustments are required.
Some people may have the opportunity to have a FibroScan® assessment prior to treatment. A FibroScan® is a type of ultrasound measuring the stiff ness of the liver. It can determine the level of liver damage; this will infl uence the timing of treatment.
Laboratory (& investigations)
The social dimension
As treatment can continue for up to a year, and side eff ects can go on beyond this, it’s nearly impossible to fi nd a block of time that would suit. • Support network: Having a good
support network is important when accessing treatment. Support can be found from friends, family, workmates, treatment staff , peer support, or other support services in the community. If you live with other people, it may be important for them to understand what’s involved in treatment so they can prepare for potential mood swings. Call 0800 33 20 10 for information on support services available in your area.
• Flexibility in employment: The fear of being unable to work during treatment is a big concern for people. You may need time off work for appointments or days when you feel too unwell to work. If you haven’t disclosed your hepatitis C status to your employer, consider telling them you are having treatment for liver disease.
• Financial support: Most people are able to continue working throughout treatment. However, if you are unable to, your doctor will decide whether the sickness benefi t is right for you.
• Contraception: It is important both men and women practice eff ective contraception for the duration of treatment. Discuss this with your doctor or nurse as the treatment is associated with serious risks to the unborn baby.
• Support from the specialist nurse: Once you are on treatment, the specialist nurse can provide support for you and your partner. It is important you clearly communicate any side eff ects you may be experiencing. The nurse will be able to provide you with advice on how to manage these side eff ects to help get you through treatment.
Social
The physical dimension
Side eff ects of hepatitis C vary from person to person. It is important to manage these side eff ects and address other health issues, to ensure your body is in peak condition prior to treatment. Call the Hepatitis Helpline on 0800 33 20 10 for more information.• Mood: Hepatitis C treatment
can cause mood swings. If you have suff ered from depression or anxiety in the past, speak to your doctor. Treatment may stimulate depression, so prophylactic anti-depressants may be required at least six weeks prior to starting treatment to prevent this problem recurring. Daily gentle exercise, such as walking or swimming, may help lift your mood.
• Sleep: If you are not sleeping well, take steps to minimise sleep disturbance, such as sleeping in a quiet, warm environment, avoid exercising late in the evening, or avoid taking short naps during the day.
• Fatigue: Fatigue is the most common side eff ect of the hepatitis C virus. Assess other lifestyle factors that could be causing this fatigue, such as stress, a busy lifestyle, or other health conditions. Having smaller meals may help with fatigue levels.
• Nutrition: When you are on treatment, your appetite may decrease. Aim to eat a healthy, balanced diet before treatment to ensure you are in the best health. Avoiding large or high fat meals during treatment may help if you are suff ering from nausea.
• Skin and dental care: Before starting treatment, it is important to clear any skin or dental infections. It is common for your white cell count to decrease, when on treatment, so your body may not be as eff ective at fi ghting infection.
Physical
Call the Hepatitis Helpline on 0800 33 20 10to talk to a community nurse about treatment.
page 17
farewell to......Clare Chapman, former Media Publications Offi cer at the Foundation. Clare joined the Foundation
early 2012. Her signifi cant contributions to the project and her easy-going nature will be missed by the team.

letters to the editor
Write us a letter.Send any comments, concerns or questions to the editor at PO Box 15 347, Tauranga, or email [email protected].
Chosen letters to the editor will be published online or in future magazines.
Do you have an experience you would like to tell us about? Any thoughts or comments you would like to share?
page 18
editorial Women who are pregnant should not receive a FibroScan®, but these scans are safe for children.
By reliably detecting whether cirrhosis is present, the FibroScan® determines the life-long risks of liver cancer and liver failure. Where cirrhosis is identifi ed, patients will require life-long surveillance, however, this is not necessary for patients in whom cirrhosis is not present.
FibroScans® also have the advantage of being able to stage the severity of liver disease in patients with bleeding disorders, such as haemophilia.
Because the machine is portable, the scan can be completed in the clinic, without the need for preparation. The FibroScan® takes fi ve minutes to complete, and there is no need for anaesthesia. The assessment is pain-free, and patients are able to return to work immediately after the scan. Results are available immediately, which allows patients to be able to begin to weigh up the pros and cons of beginning, or waiting for, treatment.
Until recently, the liver biopsy was a real barrier, preventing people from attending hepatitis clinics and was, therefore, a barrier to starting treatment. In the future, access to community-based FibroScan® services should enhance uptake of testing and treatment, which will help reduce the burden of hepatitis C.
Professor Ed Gane, Deputy Director of the New Zealand Liver Transplant Unit at Auckland City Hospital, talks about the benefi ts of FibroScan® assessments.
Liver biopsy is associated with a range of complications, which include pain, blood transfusion for haemorrhage, and emergency procedures. In addition, the direct costs of liver biopsy are more than $2,000, while indirect costs (for example, days off work) are much larger.
FibroScan® is a technology providing an inexpensive, rapid, non-invasive alternative to liver biopsy. It measures liver stiff ness through a technology called transient elastography. This technology works in a similar fashion to an ultrasound, sending an elastic wave through the liver, which then provides information about the amount of fi brosis in the liver.
Studies have demonstrated a high level of effi cacy associated with the FibroScan®’s ability to distinguish cirrhosis (expressed as “F4”) from non-cirrhosis (F0 – F3). In particular, FibroScan® has been shown to be eff ective for use with chronic hepatitis C, with which it may even be superior to liver biopsy.
Despite this demonstrated effi cacy, some conditions may prevent the machine from attaining a reliable measurement. These include obesity, or fl uid in the abdomen (ascites). However, in some cases, this can be overcome through the use of a more powerful XL probe. Obtaining a clear reading may also be diffi cult for people in whom the hepatitis virus is very active.
Here’s a plain English explanation of some medical jargon, which, chances are, you will have heard your specialist using, or read elsewhere. Sometimes medical terminology can become a barrier to understanding your health. In every issue of talking hep C Dr Frank Weilert will explain a few commonly used terms.
RVR - Rapid Virological Response: The level of the virus after four weeks of treatment. If the test is negative, the likelihood of cure is usually 80 - 90 per cent.
SVR - Sustained Virological Response: A negative virus test six months after completing treatment. This is equivalent to complete cure of the hepatitis virus.
Relapse: This can either be breakthrough during treatment or after completion of treatment. This indicates the virus has not been cured and has returned. This is considered treatment failure.
standard of care
genotype suppresion suppresion suppresion
genotype suppresion
genotypenull responders
protease inhibitors
reversible resistancereversible resistancereversible resistanceSOCSOC
naive cohorts
response guided
SVR
metabolised
effi cacy
all that jargon
FibroScan®: the alternative to liver biopsy

introducing...Out and about with the women on the ground - The Foundation’s hepatitis B and C nurses
page 19
Back row (from left to right): Kerry, Helen, and Diane.Front row (from left to right): Alannah, Marty, and Janette.
How do you gain your patient’s trust?
Diane: By showing them respect and treating them as individuals.
How do you know when you’ve made a diff erence to someone’s lives?
Helen: You do see a diff erence in them. My patients will sometimes say to me, “you’re the only one that cares about us.” It’s very touching.
Marty: I see a diff erence when the patient “gets it”. [I had one patient who] confused her [type of ] hepatitis with hepatitis A. For years [she] had her own eating utensils and cups. She would not bake for church functions for fear of infecting the congregation. She shed tears when I explained to her it was quite safe for her to do the baking and she did not require her own eating utensils. She was so grateful for my visit.
How would you summarise your job?
Diane: I feel very privileged to have this job, and I just want to continue doing it.
Marty: I love my job, [am] very fond of my patients and strive to do my very best for them and their families.
With thousands under their care, these nurses have great stamina and enthusiasm to ensure all their patients are kept in check.
As for coff ee with strawberry milk, I think the jury is still out on this one!
standard of care
null responders
protease inhibitors
naive cohortsnaive cohorts
SVR
metabolised
What do you enjoy most about your job?
Alannah: I really enjoy visiting patients and educating them; I see education as empowerment.
Kerry: I agree. Having the time to make sure they really understand what is happening, and what they can do to improve their health.
Janette: It ‘s satisfying. I get a lot of job satisfaction because what we do is improve the health of our patients ultimately.
Diane: I love that every day is diff erent. I use a wide range of my nursing skills plus life experience.
Tell us about some interesting parts of your job:
Marty: Getting coff ee with strawberry milk - delicious!
Alannah: The places I take blood is sometimes veryinteresting. As I say to them, “I can take blood wherever it suits you.” I’ve got one patient who I’ve never seen off his farm bike. He sees me coming and drives up to one side of the farm fence. I drive up to the other side. He takes one arm out of his overalls, I take his blood, then he goes back to work.
How long have you known some of your patients for?
Helen: I’ve known some of my patients for 31 years, due to my previous nursing role. I’ve seen them grow up, get into trouble, get out of trouble, get married, have children. I’ve been there. I’ve seen all of that. I think that’s why it’s been so successful, it’s the same person all the time.
There are six of them - Helen, Marty, Alannah, Janette, Kerry, and Diane. When they all get together, it’s hard to get a word in edge ways! It’s not surprising, as they only see each other a few times a year. “But we support each other really well”, said Helen. “We talk to each other often. It’s great.”
These hepatitis B and C nurses have been working with The Hepatitis Foundation of New Zealand for a period ranging from one year to over 20 years, but one thing is for certain, they are all very good at what they do.
While Ann and Lorna are the hepatitis C nurses focussing on the pilot sites, these six nurses move around diff erent parts of the country, visiting people living with either hepatitis B and/or C.
While they rattled off an exhaustive list of why they love their job, they were all in agreement on what a bad day on the job was; “visiting heaps of patients and not fi nding anyone at home,” said Marty.
Talking hep C investigates further.

contacts and support
The Hepatitis Helpline is a free, confidential, service run by The Hepatitis Foundation of New Zealand, which provides general advice, information and guidance about hepatitis C, diagnosis, treatment and on-going care.
The Hepatitis Helpline is linked with a number of other agencies, and staff can point you in the right direction if you require any other support or advice regarding issues that are not related to hepatitis C.
www.hepatitisfoundation.org.nzwww.hepatitisfoundation.org.nz
New Zealand Needle Exchange Programme03 366 9403www.needle.co.nz
The Hepatitis Foundation of New Zealand0800 33 20 10www.hepatitisfoundation.org.nz
Hepatitis C Resource Centre (Otago)03 477 0407www.hepcnz.org/otago
Community Alcohol and Drug Services09 845 1818www.cads.org.nz
Alcohol and Drug Helpline0800 787 797www.adanz.org.nz
Haemophilia Foundation of New Zealand03 371 7477www.haemophilia.org.nz
Christchurch Hepatitis C Resource Centre03 366 3608www.hepcnz.org
New Zealand AIDS Foundation09 303 3124www.nzaf.org.nz





























