Embed Size (px)
Citation preview

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 1/24
Target Audience: Infusion Nurses
FacultyDeanne BirchJulie Winton, RN, BSN
*This monograph is not sponsored by, nor a par t of, the 2006 InfusionNurses Society Annual Meeting and Industrial E xhibition.
This program is supported by a continuing nursing education grant from
Talecris Biotherapeutics, Inc.
IGIV THERAPY: THE NURSE'S ROLE IN BALANCINGCOSTS AND QUALITY OF CARE
the nurse's role in balancingcosts and qua lity of care
optimizing patient care and o
The University of Nebraska Medical Center College of Nursing Continuing Nursing Education is accredited as aprovider of continuing nursing education by the
American Nurses Credentialing Center’s Commission on Accreditation.This activity is provided for 1.2 contact hours. Iowa Provider #78.Additionally, provider approved by the California Board of RegisteredNursing. Provider #13699 for 1.2 contact hours.
A CE monograph based on a symposium at the 2006 INS Annual Meeting*

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 2/24
IGIV THERAPY: THE NURSE'S ROLE IN BALANCINGCOSTS AND QUALITY OF CARE
the nur se's role in balancing
costs and quality of care
optimizing patient care and outc omesHow to Receive CreditInfusion nurses wishing to receive 1.2 contact hours must:1. Read the monograph (estimated time for completion: 1 hour).2. Relate the content material to the learning objectives.3. Answer at least 7 of the 10 self-assessment questions on
page 15 correctly.
4. Complete the evaluation form as indicated on page 16.Upon successful completion of the requirements, a CE certificate will bemailed to you. A certificate will be mailed within 4 to 6 weeks from thedate of receipt of your completed evaluation form.
Release date: July 30, 2006Expiration: To be eligible to earn (or receive) contact hours, requiredmaterials must be postmarked or received no later than July 30, 2007.
DisclaimerThe opinions or views expressed in this continuing education activityare those of the faculty and do not necessarily reflect the opinions orrecommendations of the Continuing Education Alliance, the Universityof Nebraska Medical Center College of Nursing Continuing Nursing Education, or Talecris Biotherapeutics, Inc.
Please contact the Continuing Education Alliance at [email protected] for questions regarding this activity.
©2006 Continuing Education Alliance Printed in USA CTE32606

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 3/24
GoalTo familiarize infusion nurses with immune globulin products, safety and tolerabilityconsiderations, and current issues regarding costs and reimbursement.
Learning ObjectivesAfter reading the articles in this monograph, participants will be better able to:• Describe the differences among currently available immune globulin products and their
impact on safety, tolerability, and economic considerations.• Discuss key policies and procedures related to reimbursement for immune globulin
therapy in various clinical settings.
FacultyDeanne Birch Julie Winton, RN, B SNDirector of Reimbursement Director of Business Development–WestManaging Member BioRx, LLCInfusion Innovations, LLC Baker City, OregonSalt Lake City, Utah
DisclosuresAll faculty and planners participating in continuing education activities sponsoredby the University of Nebraska Medical Center College of Nursing Continuing Nursing Education are expected to disclose to the audience any significant support or sub-
stantial relationship(s) with providers of commercial products and/or devices discussed in this activityand/or with any commercial supporters of the activity. In addition, all faculty are expected to openlydisclose any off-label, experimental, or investigational use of drugs or devices discussed in this activity.The faculty and planning committee have been advised that this activity must be free from commercialbias, and based upon all the available scientifically rigorous data from research that conforms toaccepted standards of experimental design, data collection, and analysis.
Ms Bir ch: partner: Infusion Innovations, LLC (provider of home infusion pharmacy products).
Ms Winton: has no significant relationships to disclose.
The Planning Committee for this activity included Catherine A. Bevil, RN, EdD, of the University of Nebraska Medical Center College of Nursing Continuing Nursing Education, and Craig Borders andIra Mills of the Continuing Education Alliance. The members of the Planning Committee have nosignificant relationships to disclose.
IGIV THERAPY: THE NURSE'S ROLE IN BALANCINGCOSTS AND QUALITY OF CARE
the nurse's role in balancingcosts and quality of care
optimizing patient care and outcom es

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 4/24
IGIV THERAPY: THE NURSE'S ROLE IN BALANCINGCOSTS AND QUALITY OF CARE
the nur se's role in balancing
costs and quality of care
optimizing patient care and outc omes
i
Table of Contents
Introduction .................................................................................................................. 1
Strategies for Optimizing Patient Care With IGIV Therapy........................................2
Current Issues in Cost Management
and Reimbursement for IGIV Therapy ..................................................................9
Self-Assessment Questions ......................................................................................15
Evaluation Form for Nurses ......................................................................................16

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 5/24
Introduction
Immune globulin therapy is used for antibody replacement and immune
system modulation. A wide range of immune globulin products areavailable. Patients with certain risk factors, however, may be affected
by differences in product formulations. In addition, the reimbursementclimate continues to change. New policies and procedures have an
impact on how immune globulin therapy is coded and what services
are covered in various clinical settings.This monograph is based on presentations from a program titled
IGIV Therapy: The Nurse’s Role in Balancing Costs and Quality of
Care , which was held during the Infusion Nurses Society AnnualMeeting and Industrial Exhibition in May 2006. In “Strategies for
Optimizing Patient Care With IGIV Therapy,” Julie Winton, RN, BSN,
addresses key strategies for planning optimal administration of immune globulin intravenous (IGIV) or immune globulin subcuta-
neous (IGSC), managing the infusion process, monitoring patientsfor adverse ef fects, and educating patients and their caregivers.
In “Current Issues in Cost Management and Reimbursement for
IGIV Therapy,” Deanne Birch discusses potential cost issues relatedto IGIV therapy (eg, product manufacturing costs, direct and indirect
administration costs, product allocation, and purchasing costs) and
the impact of today’s reimbursement climate on cost recovery in
hospital, physician’s office, and home healthcare settings.

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 6/24
Immune globulin products, which consist primarily of immunoglobulin G (IgG), are derived from pooledplasma from healthy blood donors.1 Currently, the Foodand Drug Administration (FDA) has approved IGIV for multiple indications (Table 1). Early in 2006, IGSCreceived FDA approval for the treatment of primary immune deficiency (PID). However, more than 50%of patients treated with IGIV products receive them
for off-label uses.2
Planning for Optimal AdministrationPatient Risk Assessment A patient risk assessment tool can help cliniciansdevelop a care plan that matches each patient’s risk profile with the appropriate immune globulin therapy and thereby minimize infusion reactions (Table 2). Atleast 70% of the nurses polled during theIGIV Therapy:The Nurse’s Role in Balancing Costs and Quality of Care program at the 2006 meeting of the Infusion NursesSociety reported that their facility or home healthcareunit does not use a risk-assessment tool to assist in theselection of an immune globulin product. Factors toconsider during the risk assessment include the condi-tion for which IGIV or IGSC therapy was prescribed,comorbidities (eg, cardiovascular disease, renal disease,or diabetes mellitus), allergies, history of infusion reac-tions with immune globulin therapy, and any barriersto intravenous (IV) or subcutaneous (SC) access. Theexistence of a family or caregiver support system is also
an important consideration, particularly when immuneglobulin therapy is provided at home.
Nurse’s Role in Risk AssessmentFrom their earliest initiation into nursing school, nursesare trained to carefully assess potential and real problemsassociated with their patients’ diagnoses and therapies. Accordingly, long hours are devoted to care planning.
Similarly, this should be viewed as the basis for thenurse’s role in risk assessment related to the infusion of IGIV and IGSC. Regardless of the setting (ie, hospital,clinic, or home care), the infusion nurse is responsiblefor making every effort to minimize the risk to thepatient of adverse events during infusion. This in turnminimizes risk for the infusion nurse, the prescriber, the
IGIV THERAPY: THE NURSE'S ROLE IN BALANCINGCOSTS AND QUALITY OF CARE
the nur se's role in balancing
costs and quality of care
optimizing patient care and outc omesStrategies for Optimizing Patient CareWith IGIV Therapy Julie Winton, RN, BSNDirector of Business Development–West BioRx, LLC
Baker Cit y, Oregon
Table 1.
FDA-Approved Indications for IGIV and IGSC
IGI V IGSCPrimary immune deficiency (PID)Idiopathic thrombocytopenic purpuraKawasaki syndromeChronic lymphocytic leukemiaPediatric HIV infection*Bone-marrow transplantation(allogeneic)*
PID
*Gamimune N, which is no longer manufactured, was the only IGIVproduct approved by the FDA for pediatric HIV infection and bone marrowtransplantation (allogeneic).

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 7/24
dispensing pharmacist, and the facility where the nurseis employed. If the infusion nurse is aware that IGIV and IGSC products may carry higher risk of adverseevent for certain patients (eg, high glucose in a patient with diabetes, high pH in a neonate, large fluid volumein a cardiac patient), the infusion nurse can choose aproduct that may minimize these potential issues. It isbasic nursing practice to incorporate a risk assessmentthat alerts the infusion nurse to these concerns and tochoose a product that best fits the particular patient,thus minimizing risk. Patient history and infusionhistory are other important items to have availableto the infusion nurse.
Clinical ConsiderationsBecause of differences in manufacturing processes, IGIV product characteristics vary (Table 3). Formulations,concentrations, osmolalities, and pH differ among theavailable products, as do their sodium, sugar, andimmunoglobulin A (IgA) content.3 These differences may have an impact on tolerability in certain patient popula-tions, including elderly patients, neonates, and patients with cardiac impairment or renal dysfunction (Table 4).Production processes used to inactivate or remove blood-borne pathogens also differ among the products.
Volume LoadPreparations of IGIV are available in concentrations rang-ing from 3% to 12%. When IGIV is given at higher con-centrations, the volume load is reduced, and the infusiontime is shortened. For example, a 70-kg patient who isadministered IGIV at a dosage of 2 g/kg would receive1400 mL of a 10% solution or 2800 mL of a 5% solu-tion. Minimizing volume load may be appropriate forpatients with congestive heart failure, hypertension, renaldysfunction, or vascular disease. Also, neonates and eld-erly patients (65 years of age or older) may tolerate high
volume loads less well than patients in other age groups.Patients who are intolerant of long infusion times may also benefit from reduced volume loads.
IGSC is available in a 16% concentration. Volumeload is not a consideration with IGSC therapy because itis not infused directly into the circulation and is adminis-tered at a very slow rate.
Sugar ContentSugar is added as a stabilizer to most IGIV products(only 2 products are stabilized with glycine). Sugar contentis an important consideration because it affects osmolality.The use of IGIV preparations containing sugar has beenassociated with renal adverse events: 90% of the IGIV-induced renal adverse events in the United States that were reported to the FDA between 1985 and 1998 wereattributed to products stabilized with sucrose.4 Sugar-containing IGIV products should be avoided or used with caution in patients at risk for renal adverse events(eg, patients with preexisting renal disease, diabetes, orsigns of prediabetes; patients 65 years of age or older).
3
Table 2.
Patient Risk-Assessment Checklist■ Current diagnosis. What is the condition requiring IGIV
or IGSC therapy?• Current signs and symptoms of condition• Changes in signs/symptoms since last infusion
■ Comorbidit ies. Does the patient have other conditionsor health-related concerns?• Cardiovascular disease?• Diabetes or prediabetes?• Renal dysfunction?• Selective IgA deficiency?
■ Recent illnesses. Has the patient had any recent illnesses(other than those noted above)?
■ Cur r ent medicat ion histor y. What drugs is the patient using?Is the patient receiving treatment with a nephrotoxic drug?• Prescription drugs?• Over-the-counter drugs?• Nephrotoxic drug use?
■ Allergies. Does the patient have any allergies?■ Infusion hist or y. Has the patient received prior immune
globulin infusions? If yes:• Which product?• Which administration route?
• Was the infusion well tolerated? (If not, specify theadverse reaction.)• Did the patient receive premedications? (If yes, specify.)
■ Weight. What is the patient’s current weight?■ I V or SC access. Are there any barriers to IV or SC access?■ Suppor t . Does the patient have adequate caregiver support?

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 8/24
Sodium ContentThe sodium content of available IGIV preparationsvaries widely.3 Infusions of preparations with a highsodium concentration may upset fluid and electrolytebalance in some patients (eg, elderly patients; neonates;patients with hypertension, congestive heart failure,vascular disease, or renal dysfunction).5
Osmolality The osmolality of IGIV preparations varies dependingon the formulation, concentration, and (if a lyophilizedproduct is used) the reconstitution fluid. Reconstitutionof lyophilized products at higher concentrations canresult in hyperosmolar solutions. The reference range forphysiologic osmolality (serum) is 275 to 295 mOsm/kg
of water. A 6% solution of a lyophilized sucrose-stabilizedproduct has an osmolality of 384 mOsm/kg if reconsti-tuted in sterile water or 690 mOsm/kg if reconstitutedin normal saline; at a 12% concentration, the osmolality rises to 768 mOsm/kg in sterile water or 1074 mOsm/kgin normal saline. The use of hyperosmolar IGIV solu-tions should be avoided in patients at risk for renal orthromboembolic complications.5-7
pHThe optimal pH for IGIV in solution ranges from 4.0to 4.5.8 Currently available IGIV preparations range inpH from 4.0 to 7.2.3 A product’s pH may be an impor-tant consideration for patients (eg, neonates) who areintolerant of acidic loads.9
IGIV THERAPY: THE NURSE'S ROLE IN BALANCINGCOSTS AND QUALITY OF CARE
the nur se's role in balancing
costs and quality of care
optimizing patient care and outc omes
Table 3.
Comparison of Currently Available IGIV Products
*The manufacturing process for this product provides reasonable assurance that prions associated with transmissible spongiform encephalopathy would beremoved if present in donated plasma.Manufacturers’ package inserts and Siegel J. Pharm Pract News. 2005.
Carimune® NF ( ZLB Behring )*
Flebogamma ®
( Grif ols)
Gammagar d®
Liquid( Baxter
Healthcar e)Gammagar d® S/D(Bax ter Healthcar e)
Gamunex ®( Talecris
Biotherapeutics)*
Iveegam EN®
(Bax ter Healthcar e)
Octagam®
(Octapharma)
Poly gam®
S/D(Bax ter
Healt hcar e)FDA-approvedindication(s)
PID, ITP PID PID PID, ITP, CLL, KS PID, ITP KS, PID PID PID, ITP, CLL,KS
Form Lyophilized Liquid Liquid Lyophilized Liquid Lyophilized Liquid LyophilizedConcentrationoptions
3%, 6%, 9%, 12% 5% 10% 5% or 10% 10% 5% 5% 5% or 10%
Sugar content Sucrose, 1.67 g per gram of
protein
D-Sorbitol,50 mg/mL
None(stabilized
with glycine)
Glucose,20 mg/mL
(5% concentration)
None(stabilized
with glycine)
Glucose,50 mg/mL
Maltose,100 mg/mL
Glucose,20 mg/mL
(5% solution)Sodium content <20 mg per
gram of protein<3.2 mEq/L
(<0.02%)None ~8.5 mg/mL Trace 3 mg/mL 30 mmol/L 8.5 mg/mL
(5% solution)
Osmolarity/osmolality
mOsm/kg:In sterile water:
192-768In 0.9% NaCl:
498-1074In 5% dextrose:
444-1020
240-350mOsm/L
240-300mOsm/kg
636 mOsm/L(5%)
1250 mOsm/L(10%)
258 mOsm/kg ≥ 240mOsm/L
310-380mOsm/kg
636 mOsm/L(5%)
1250 mOsm/L(10%)
pH 6.6 ± 0.2 5-6 4.6-5.1 6.8 ± 0.4(5% solution)
4.0-4.3 6.4-7.2 5.1-6.0 6.8 ± 0.4(5% solution)
Gammaglobulin
≥ 96% >99% ≥ 98% ≥ 90% ≥ 98% ≥ 95% ≥ 96% ≥ 90%
IgA content Trace <0.05 mg/mL 37 μg/mL ≤ 2.2 μg/mL(5% solution)
0.046 mg/mL Trace amounts ≤ 0.1 mg/mL ≤ 2.2 μg/mL(5% solution)

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 9/24
IgA ContentPatients with selective IgA deficiency, which is character-ized by production of immunoglobulin E (IgE)–or IgG-type anti-IgA antibodies–are at increased risk of severeimmediate hypersensitivity reactions (including anaphy-laxis).1,10,11 All immune globulin preparations containsome IgA. Although the risk of complications isextremely rare, IGIV and IGSC are contraindicatedin patients with selective IgA deficiency.3
Pathogen Safety Immune globulin products have an excellent safety record. However, because they are derived from pooledhuman plasma, they can potentially transmit blood-bornepathogens, such as viruses and prion proteins.12 Variousviral inactivation or removal steps have been integratedinto the manufacturing process to help ensure productsafety. They include preproduction screening, viral inacti-vation by physical (eg, dry heat and pasteurization) orchemical (eg, solvent/detergent incubation at low pHand caprylate treatment) methods, and viral clearance
(eg, with fractionation, chromatography, or filtration).13
The specific steps used vary by product manufacturer.Efforts to protect against emerging pathogens, such as
the prion proteins associated with transmissible spongi-form encephalopathy (TSE), are ongoing. Thecaprylate/chromatography process14 and the precipitation/depth filtration/nanofiltration process15 provide reasonableassurance of a reduced risk of pathogenic prion transmis-sion. The FDA has approved the inclusion of a statementregarding assurance of TSE-associated prion removal inthe labeling for 2 IGIV products (Table 5).
Managing the Infusion Processand Adverse Reactions
IGIV Before beginning the infusion, the nurse should confirmthat the institution’s infusion policy and procedures arebeing followed and that the appropriate risk-assessmentforms have been completed. The care plan should includethe physician’s orders for any premedications and anaphy-laxis treatment. If the physician did not specify an IGIV product, the nurse should look carefully at the patient’s risk
factors and history of infusion reactions and at the charac-teristics of the IGIV product selected, and should consultthe pharmacist if any potential problems are identified.
Manufacturers’ guidelines for IGIV administrationare available for all products. Infusing IGIV at a slowerrate than that recommended by the manufacturer may be
5
Table 4.
Clinical Considerations in IGIV TherapyIf the patient has: Consider: Age-related risk
Advanced age • Osmolality • Sodium content • Sugar content • Volume load
Young age (eg, neonates/infants) • Osmolality • pH• Sodium content • Volume load
Cardiovascular disease(eg, congestive heart failure,hypertension, vascular disease)
• Osmolality • Sodium content • Volume load
Diabetes or prediabetes • Sugar content IgA deficiency (anti-IgA antibodies) • IgA content Renal dysfunction • Osmolality
• Sodium content • Sugar content • Volume load
Thromboembolic risk factors • Osmolality • Sodium content • Volume load
Table 5.
TSE Prion Removal Labeling in CurrentlyAvailable IGIV and IGSC ProductsIGIV IGSCCarimune® NF: Yes*Flebogamma®: NoGammagard® Liquid:NoGammagard® S/D: NoGamunex ®: Yes*Iveegam EN®: NoOctagam®: NoPolygam® S/D: No
Vivaglobin®: No
*According to the FDA-approved labeling, the manufacturing process for this product provides reasonable assurance that prions associated with TSE would be removed if present in donated plasma.

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 10/24
considered, especially for a patient’s first infusion.Slowing the infusion rate can help to minimize infusionreactions. The most common infusion rate–relatedreactions include: blood pressure decreases; pulse rateincreases; fever; chills; headache; chest, back, or hip pain;dyspnea; and mild erythema. Other IV medicationsshould not be injected into the IGIV infusion line.
The patient’s vital signs should be assessed at baselineand at regular intervals during the infusion: every 15minutes during the first infusion hour, every 30 minutesduring the second hour, then hourly until the infusion iscompleted, and once post-infusion. Headache, chills, andback/joint pain were the most common reactions relatedto IGIV administration, according to a self-administered,self-reported, Web-based survey of 59 randomly selectedinfusion nurses working in a variety of settings (ie, office,clinic, and home care).16
If the patient experiences a mild IGIV infusion–relatedreaction, the nurse should reduce the infusion rate by half and continue to observe the patient closely and to monitorvital signs. In addition, the nurse should ensure that thepatient is in a comfortable position (eg, by adjusting thepillows supporting the back if the patient experiences back
pain). Any medications ordered for adverse reactions shouldbe administered as appropriate. The attending physicianshould be notified promptly if the adverse reaction persists.
The infusion should be stopped at once if the reac-tion is severe (eg, anaphylaxis) or if the physician orderstreatment discontinuation. Anaphylaxis treatment andsupportive care should be administered immediately.The infusion nurse should be aware of his or her work-place policy for anaphylaxis. The nursing basics of ABCs(Airway, Breathing, and Circulation) are critical.Emergency assistance should be called in a home setting,or, if in a hospital or clinic infusion suite, a crisis teamshould be alerted. It is always valuable to have practicedthese procedures beforehand, if possible.
Because of the potential for adverse reactions, patientsshould never be left alone during IGIV infusion. Athome, patients should have undergone at least 2 or 3 suc-cessful (ie, free of serious adverse effects) infusions beforeconsidering infusion administration in the absence of aninfusion nurse. A caregiver should always be presentduring independent IGIV infusion.
The IGIV infusion course and all adverse reactionsmust be properly and thoroughly documented by theinfusion nurse. Documentation ensures that subse-quent infusion nurses will have a full understandingof how each patient responded to previous treatmentand provides a high-quality continuum of caredesigned to minimize adverse reactions and maximizetherapeutic effect.
Accurate documentation of ongoing assessments with each infusion (eg, decreased numbness, increasedmobility, no hospitalizations for infections) assists invalidating therapy benefit to an insurance provider/payer.This can be critical for the reauthorization often requiredfor some of the most frequent off-label uses of IGIV orIGSC, such as chronic inflammatory demyelinatingpolyneuropathy (CIDP).
IGSC Administration of IGSC may be considered for patients who have venous access problems (eg, young children), who want greater autonomy, or who have had adversereactions to IGIV. IGSC may also provide an alternativeimmune globulin treatment modality for patients with
a central line infection or risk factors that warrant useof smaller infusion volumes. Because IGSC is absorbedmore slowly than IGIV, bioavailability may be reduced.IGSC may be administered once every other day, once weekly, or once every 2 weeks; in comparison, IGIV isadministered once every 3 to 4 weeks.
IGSC is generally performed in the home setting,requiring 2 to 3 training sessions to learn SC needleplacement as well as the therapy regimen. Adverse reac-tions are minimized due to the SC route of administra-tion. Typically, only the actual infusion site has reactionissues such as redness. Irritation and swelling may beminimized with site rotation, keeping in mind the initialplacement site and anatomic irregularities (skin folds,scar tissue, recently used sites, etc).
IGSC is infused at a steady rate over 1 to 2hours—depending on the patient’s weight and pre-scribed dose. Usually 2 or more sites are used simulta-neously. Infusion sites (eg, abdomen, thighs, upperarms, and lateral hip) should be selected according tothe patient’s body dynamics and rotated periodically.
IGIV THERAPY: THE NURSE'S ROLE IN BALANCINGCOSTS AND QUALITY OF CARE
the nur se's role in balancing
costs and quality of care
optimizing patient care and outc omes

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 11/24
The infusion nurse must check for blood return afterinsertion of the SC needle to be sure he or she is notinfusing intravenously. The only IG product FDA approved for SC administration clearly indicates inthe labeling that it is not to be infused intravenously.Other intramuscular or IGIV products are reconsti-tuted and used subcutaneously, but such use is beyondFDA-approved labeling.
In adults, IGSC volumes should not exceed 25 mLper injection site. A good rule to follow is to administer20 mL at 20 mL/h per injection site (the “20:20 rule”). Although most children can tolerate a 10-mL volumeper site, very young patients should be given a reducedvolume (5 mL or 7.5 mL).
Laboratory monitoring includes measurement of an initial IgG level, IgG trough/peak levels at periodicintervals to stabilize medication dose, and liver functiontests to monitor for signs of infection. These areordered per physician preference/protocol. Overallpatient health and infection status must also be care-fully and regularly monitored. This would includenumber of infections since last infusion that required aphysician visit, antibiotic usage, emergency department
visit, or hospitalization.The most common adverse effects associated with
IGSC administration are redness, slight swelling, andtenderness at the infusion site. Infusion-site irritationcan be minimized by using alcohol, not an iodine-based solution, for cleaning the skin prior to needleinsertion; paying close attention to body dynamics when selecting an infusion site; and rotating the infu-sion sites. If swelling persists beyond 3 to 4 days, thevolume infused at each site should be reduced. Otheradverse effects reported with IGSC are similar to thoseseen with IGIV.17
Educating Patients and CaregiversPatients and their caregivers should be fully informedabout the potential benefits of IGIV or IGSC treatment,safety issues, the rationale for any premedications orderedby their physicians, and what to expect during and afterthe infusion.
If IGSC is to be administered at home, patients andtheir caregivers also need to be instructed in the type of
equipment used for the infusion and its maintenance,selection of appropriate infusion sites, infusion techniques,the importance of maintaining a treatment diary todocument adverse reactions, and the appropriate mea-sures to take if an adverse reaction occurs (Table 6).
(Education on infusion pump maintenance, infusionsite selection, and record keeping is also important forpatients receiving IGIV at home.)
During the course of treatment, nurses mustcontinually reevaluate the extent of patient and care-giver understanding of the provided information.Further education should be provided and reinforcedas needed.
References1. Kazatchkine MD, Kaveri SV. Immunomodulation of
autoimmune and inflammatory diseases with intravenousimmune globulin. N Engl J Med.2001;345:747-755.2. Chen C, Danekas LH, Ratko TA, Vlasses PH, Matuszewski
KA. A multicenter drug use surveillance of intravenousimmunoglobulin utilization in US academic health centers.
Ann Pharmacother.2000;34:295-299.3. Siegel J. Intravenous immune globulins: therapeutics, phar-
maceutical, and cost considerations.Pharm Pract News.2005;Jan:19-23.
4. Centers for Disease Control and Prevention (CDC). Renalinsufficiency and failure associated with immune globulinintravenous therapy–United States, 1985-1998. MMWR
Morb Mortal Wkly Rep.1999;48:518-521.
7
Table 6.
Patient and Caregiver Education for IGSCInfusion in the Home Healthcare SettingMedications used (benefits, risk s)• IGSC• PremedicationsEquipment • Required components• MaintenanceInf usion• Site selection• Site rotation• Infusion technique Adver se reaction education• What to expect during the infusion• What to watch for and report after the infusion• Measures to take if an adverse reaction occursRecord keeping (treatment diar y )

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 12/24
5. Lemm G. Composition and properties of IVIg preparationsthat affect tolerability and therapeutic efficacy.Neurology.
2002;59(suppl 6):S28-S32.6. Reinhart WH, Berchtold PE. Effect of high-dose intra-venous immunoglobulin therapy on blood rheology.Lancet.1992;339:662-664.
7. Evan-Wong LA, Davidson RJ, Stowers JM. Alterations inerythrocytes in hyperosmolar diabetic decompensation: apathophysiological basis for impaired blood flow and foran improved design of fluid therapy.Diabetologia.1985;28:739-742.
8. McCue JP, Hein RH, Tenold R. Three generations of immunoglobulin G preparations for clinical use.Rev Infect Dis.1986;8(suppl 4):S374-S381.
9. Ratko TA, Burnett DA, Foulke GE, Matuszewski KA,Sacher RA, for the University Hospital Consortium ExpertPanel for Off-Label Use of Polyvalent Intravenously Administered Immunoglobulin Preparations.Recommendations for off-label use of intravenously administered immunoglobulin preparations. JAMA.1995;273:1865-1870.
10. Dalakas MC. Intravenous immunoglobulin in the treat-ment of autoimmune neuromuscular diseases: present statusand practical therapeutic guidelines. Muscle Nerve.1999;22:1479-1497.
11. National Institutes of Health Consensus DevelopmentConference. Intravenous immunoglobulin.Consens
Statement.1990;8:1-23.12. Miller JL, Petteway SR Jr, Lee DC. Ensuring pathogensafety of intravenous immunoglobulin and other humanplasma-derived therapeutic proteins. J Allergy ClinImmunol. 2001;108(suppl):S91-S94.
13. Shah S. Pharmacy considerations for the use of IGIV ther-apy. Am J Health Syst Pharm.2005;62(suppl 3):S5-S11.
14. Gamunex [package insert]. Research Triangle Park, NC:Talecris Biotherapeutics, Inc; 2005. Available at:http://www.talecris-pi.info/inserts/gamunex.pdf.
15. Carimune [package insert]. Kankakee, Ill: ZLB BehringLLC; 2005. Available at:http://www.zlbbehring.com/ZLBB/binary/CarimunePI.pdf.
16. Davis J, Duff K, Ganio S, et al. Criteria for selecting anIGIV preparation: the infusion nurses’ perspective. J Allergy Clin Immunol.2003;111(suppl 2):S121.
17. Chapel HM, Spickett GP, Ericson D, Engl W, Eibl MM,Bjorkander J. The comparison of the efficacy and safety of intravenous versus subcutaneous immunoglobulin replace-ment therapy. J Clin Immunol.2000;20:94-100.
IGIV THERAPY: THE NURSE'S ROLE IN BALANCINGCOSTS AND QUALITY OF CARE
the nur se's role in balancing
costs and quality of care
optimizing patient care and outc omes

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 13/24
Therapy with immune globulin intravenous (IGIV) is alife-saving treatment provided to many patients in settingsranging from hospitals to physicians’ offices and patients’homes. Economic issues that affect providers of IGIV ther-apy include the costs of product purchasing and adminis-tration, product availability, reimbursement for off-labeluse, and fluctuating reimbursement rates. The impact of
these issues varies depending on the medical needs andhealthcare coverage of the patients being served and thesite of administration. With increases in co-payments andcaps on reimbursement, cost considerations often play amajor role in selection of an IGIV product for a particularpatient. More than 70% of the infusion nurses polled dur-ing the IGIV symposium at the May 2006 meeting of theInfusion Nurses Society (INS) reported that cost considera-tions affected their selection of an IGIV product.
Potential Cost IssuesThe cost of IGIV therapy is the sum total of productmanufacturing costs, administration costs (includingequipment and supplies, clinical patient monitoring, andother indirect overhead costs), product allocation, andpurchasing costs.
Product Manufacturing CostsProduct acquisition costs for IGIV can vary significantly between the least expensive and the most expensive prod-uct. These variations stem largely from differences in the
manufacturing processes; they are also dependent onproduct availability and shortages. The IGIV productslicensed in the United States are all derived from pooledplasma obtained from 3000 to 10,000 healthy blooddonors—sometimes as many as 100,000 donors.1However, beyond the source of origin, the manufacturingprocesses of IGIV products differ widely in methods
used to maintain the integrity and biologic activity of immunoglobulins while simultaneously removing orinactivating unwanted viruses and other pathogens toensure product safety.2
Variability in manufacturing, viral inactivation, andchemical processes used to stabilize the preparationsmay lead to variations in clinical efficacy, safety frompathogens, and tolerability, as discussed by Ms Wintonin “Strategies for Optimizing Patient Care With IGIV Therapy.” Such variations may also lead to differences ineconomic benefits. Clinicians must select IGIV productson the basis of the risks and benefits to each individualpatient. However, product selection may have an impacton overall healthcare costs by reducing the risk of second-ary infection and complications as well as decreasinghealthcare resource utilization (eg, hospitalization andassociated drug costs).
In a retrospective multivariate analysis of results from a9-month trial, Mahadevia and colleagues3 compared thecosts of using an IGIV product manufactured with chro-matography and caprylate methods (IGIV-C; Gamunex,
9
Current Issues in Cost Managementand Reimbursement for IGIV TherapyDeanne BirchDirector of Reimbursement Managing Member
Infusion Innovations, LLCSalt Lake City, Utah

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 14/24
10% [Talecris Biotherapeutics, Inc., Research TrianglePark, NC]) with the costs of using an IGIV productproduced with solvent-detergent methods (IGIV-SD;Gamimune N, 10% [Bayer Corporation, Clayton, NC])
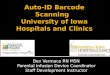
in patients with primary immune deficiency (PID). Forpurposes of the cost analysis, the product acquisition costs were assumed to be equivalent. The patients (n = 87) whoreceived IGIV-C had fewer visits to physicians’ offices andemergency departments, required fewer prescriptions(incident medications), and had fewer hospitalizations thandid the patients (n = 85) who received IGIV-SD (Table 1).Such differences translated into lower overall healthcarecosts. On average, compared with patients treated withIGIV-SD, patients treated with IGIV-C had significantly lower prescription costs (–$302; 95% CI, –$598 to –$6),hospitalization costs (–$1454; 95% CI, –$1828 to–$1080), and total costs (–$1304; 95% CI, –$1867to –$742; all P <.05) (Figure). Costs associated withphysician and emergency department visits and with lostproductivity were similar in the 2 groups.
Administration CostsIn addition to the direct cost of the IGIV product, theindirect administration costs incurred by the profes-sional services and supplies associated with all aspects
of IGIV therapy must be considered for appropriatereimbursement. These administration costs includenursing time for preevaluation, patient/caregivereducation, line insertion with continual monitoringduring both the IGIV line insertion and IGIV admin-istration, patient follow-up, clinical documentation,and nursing travel time. Added to this are pharmacy costs to allocate and store the product, to compoundin a class 100 clean room, to meetUnited States Pharmacopeiachapter 797 requirements to ensuresterility and stability, to deliver product as well assupplies and equipment, and for continued monitoringof the patient’s progress. In addition, there are many other operational costs related to qualifying andadmitting the patient, performing insurance screening,and obtaining prior authorization from the payer. Allof these costs are typically bundled under 1 or 2administrative reimbursement codes with a set reim-bursement regardless of the actual costs.
Product AllocationIn the past year, the American Society of Health-SystemPharmacists (ASHP) and various federal agencies received
reports of problems with access to IGIV.4 When nurses who attended the IGIV symposium at the 2006 INSmeeting were asked which of 5 cost/reimbursement issueshas the greatest impact on their practice, product avail-ability ranked first (41% of respondents), followed by product purchasing costs (22%), reimbursement for off-label use (22%), fluctuating reimbursement rates (11%),and product administration costs (4%).
The primary reason for the reported access and sup-ply issue is the change in reimbursement from average wholesale price (AWP) to average sales price (ASP) in theMedicare setting for physicians and hospital outpatients. While in early 2004 physicians were reimbursed at 95%of the AWP for the drug, later in the same year drugreimbursement was reduced to 85% of AWP. In 2005,reimbursement was changed to ASP plus 6%, a signifi-cant reduction that led physicians to shift their patientsfrom the physician clinic setting to hospitals, primarily tothe hospital outpatient setting. In early 2006, ASP plus6% reimbursement was implemented to hospital outpa-tient settings, placing the burden of cost containment
IGIV THERAPY: THE NURSE'S ROLE IN BALANCINGCOSTS AND QUALITY OF CARE
the nur se's role in balancing
costs and quality of care
optimizing patient care and outc omes
0
Table 1.
Healthcare Resource Utilization in PatientsWith PID: IGIV-C Compared With IGIV-SDHealthcare Resource
Utilization
Resource Categor y IGIV-C(n = 87)
IGI V-SD(n = 85)
Physician office/emergency depart-ment visits, total number
148 174
Incident prescriptions, total number 876 1076• For validated infections 19 39• For nonvalidated infections 269 344• For adverse events 15 16• For all other medications 573 677
Lost productivity, total days* 240 230Hospitalizations, total number 26 34
• Attributable to IGIV 1 7*Self-reported.Mahadevia PJ, et al.3

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 15/24
and product allocation on these systems, creating an issueof access by reducing hospitals’ ability to purchase these
products. According to a report by FFF Enterprises(a biopharmaceuticals, plasma products, and vaccinesdistributor based in Temecula, Calif), 9% of hospitalsclosed their infusion clinics and services.5 This led toanother shift in IGIV delivery to the home healthcareand home infusion setting. Reports continue of inade-quate access, with supply not keeping up with demand.
At 2 meetings in 2005, the Department of Healthand Human Services (DHHS) Advisory Committee onBlood Safety and Availability (ACBSA) recommendedthat the DHHS secretary declare a public health emer-gency to address the short-term problems of access toIGIV. 6,7 The Centers for Medicare and Medicaid Services(CMS) first responded that there are sufficient suppliesavailable to patients but that CMS will continue tomonitor the situation since there might be “ongoing mar-ketplace adjustments” affecting how inventories are man-aged.8 The CMS also suggested that increased off-labeluse might be contributing to rising demand and advisedphysicians to give first priority to IGIV treatment forFood and Drug Administration (FDA)–approved uses.8,9
More recently, a “temporary add-on payment” code wasestablished for 2006 to reflect the expenses incurred by the “additional preadministration-related services requiredto locate and acquire an adequate product and to preparefor an infusion of IGIV.”10
DHHS agencies are working with the various IGIV stakeholders (ie, patients, manufacturers, distributors,physicians, and hospitals) to understand the evolvingIGIV marketplace, ensure the continued collection of ASP data, and “focus attention on the evidence-basedmedical necessity of the utilization of IGIV.”10 TheDHHS Office of the Inspector General is also examiningIGIV availability and pricing. The CMS has committedto undertaking a study of the epidemiology of IGIV treatment of Medicare beneficiaries in the outpatientsetting.5 (The Immune Deficiency Foundation11 andThe Neuropathy Association12 are urging members toask that their representatives in the US Congress signthe McCrery/Foley/Israel letter to Secretary Leavitt askingthat his office declare a public health emergency forpatient access to IGIV.)
Purchasing CostsThe major class of trade (COT) groups relative to IGIV are physicians; hospitals, long-term care, and skillednursing facilities; home infusion providers; and retailpharmacies/specialty pharmacies. Each COT group hasdifferent buying power. Physicians hold the greatest leverageon purchasing costs because they select which product toprescribe. Hospitals have strong buying leverage becauseof volume and, thus, historically have enjoyed lower pur-chasing costs. COT groups with the least purchasingleverage usually pay the highest costs. Specialty pharma-cies have entered the distribution market for infusibleproducts like IGIV. They face the challenge of needingto coordinate their “high touch service” component witha local infusion pharmacy to provide the clinical compo-nent (ie, administration and patient care).
It is apparent why ASP is an inadequate measureof true cost when provider groups have different pur-chasing powers.
1
Physician and emergency department costsPrescription costs
Productivity costsHospitalization costsTotal costs
0
–500
–1000
–1500
–2000
500
–1304–1454
–302
–34 –8
P <.05
P <.05 P <.05
P e r
P a
t i e n
t ( $ )
Figure. Healthcar e utilizat ion cost r eductions wit h IGIV-C compared with IGIV-SD.Multivariate cost comparison shows significant differ-ences in healthcare utilization costs between patients with PIDreceiving IGIV-C (n = 87) and those receiving IGIV-SD (n = 85). Onaverage, compared with IGIV-SD, treatment with IGIV-C was associ-ated with significantly lower prescription costs, hospitalizationcosts, and total costs ( P <.05). Physician and emergency depart-ment costs as well as productivity costs were similar in the2 groups. From Mahadevia PJ, et al.3

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 16/24
Reimbursement Climate
Delivery ModelsThe 4 IGIV delivery models are hospitals, physicians/clinics, home infusion providers, and hospital outpatientambulatory infusion centers. Reimbursement regulationsand issues vary by both payer and delivery model. Forexample, Medicaid varies state by state, adding complex-ity beyond the scope of this article. However, with theimplementation of the Medicare Part D drug benefit, allstate Medicaid Dual Eligibles (patients eligible underboth Medicaid and Medicare) will look to MedicarePart D or Medicare Part B for IGIV coverage.
Drug Coding and PricingHealthcare Common Procedure Coding System(HCPCS) versus National Drug Code (NDC)Two major drug coding methodologies are used forIGIV: the HCPCS and the NDC. With the HCPCS,
J codes for IGIV payment are based on the code descrip-tion, which in 2006 is per 500 mg of IGIV dispensedregardless of which IGIV product is being used. UnderMedicare, all reimbursement models are reimbursed using
the HCPCS at ASP plus 6%, regardless of the productmanufacturer. Commercial payers may require eitherHCPCS coding, NDC coding, or both. Using the NDCmethodology for coding, the IGIV assigns a uniquelabeler code and product code for each individual IGIV
product. Typically this system reimburses based on a per-centage of the AWP of a specific product.
During the patients’ prequalification and insurancescreening, providers should be aware of which methodol-ogy the payer requires for the billing unit of measure(HCPCS or NDC). Consider the example of a 10-g vialof IGIV. If the payer uses NDC for the pricing andbilling unit, the provider would bill for 1 unit of theproduct used and is reimbursed on the basis of a percent-
age of the AWP for that particular 10-g product. If thepayer uses HCPCS as the pricing and billing unit, theprovider would bill for 20 units (500 mg) and is reim-bursed at the allowable rate per unit. Thus, if the payeris reimbursing on an HCPCS code billing unit but theprovider bills with an NDC billing unit, the provider would be grossly underpaid.
Key Changes in 2006Coding changes implemented in 2006 are listed inTables 2 through 5. New HCPCS J codes (J1566 and J1567) have been assigned to replace the temporary Q codes used in 2005 to differentiate lyophilized andnonlyophilized (liquid) IGIV products (Table 2). Thebilling units also changed from 1-g and 10-mg units tothe 500-mg (0.5-g) unit. The Medicare ASP plus 6%reimbursement rates are updated quarterly. The ratesfor the third quarter of 2006 (effective July 1, 2006,through September 30, 2006) allow $24.899 per unitof lyophilized IGIV and $30.116 per unit of non-lyophilized (liquid) IGIV. As an example, based on the
IGIV THERAPY: THE NURSE'S ROLE IN BALANCINGCOSTS AND QUALITY OF CARE
the nur se's role in balancing
costs and quality of care
optimizing patient care and outc omes
Table 2.
New HCPCS J Codes and Billing Units for IGIV
CodeProduct
Descr iptionBilling Unit Changes
J1566 Lyophilized 500 mg (0.5 g) • New J code replacesQ codes (Q9941 andQ9942)
• New billing unit replacesold billing units of 1 g and 10 mg
J1567 Nonlyophilized(liquid)
500 mg (0.5 g)
• New J code replacesQ codes (Q9943 andQ9944)
• New billing unit replacesold billing units of 1 g and 10 mg
Table 3.New HCPCS G Code for IGIV Preadministration Services
CodePayment
Rates ChangesG0332 Physician
office:$69.00Hospitaloutpatient:$75.00
• NewG code applies to preadministrationservices for each IGIV infusion in thephysician office or hospital outpatient setting
• Payment is in addition to payment for drug cost or infusion services
• Other G codes are no longer valid in thephysician office setting

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 17/24
2006 billing unit and the third-quarter reimbursementrates, one 10-g vial of lyophilized IGIV would be reim-
bursed at $497.98 and 10 g of nonlyophilized IGIV would be reimbursed at $602.32.
The new “add-on” G code for IGIV preadminis-tration services applies to the physician office andhospital outpatient settings (Table 3). The allowablepayment rates are per patient per administrationand vary by setting. OtherG codes are no longervalid in the physician office setting; they have beenreplaced by current procedural terminology (CPT)codes (Table 4).
Also in 2006, new C codes are being used underthe Hospital Outpatient Prospective Payment System(HOPPS; Table 5). The CMS no longer recognizes theold CPT codes.
Factors Affecting Reimbursement forDifferent Delivery MethodsUnder the hospital inpatient delivery model, for mostgovernment programs, the prospective payment system— wherein everything provided is bundled for reimburse-ment—places the burden of cost containment on the
provider. In the commercial setting, percentage of chargestill exits, wherein the provider bills their usual and cus-tomary charges with a percentage discount. The objectiveof the percentage of charge system is to keep prices as
high as possible without losing business to competitors.Given these restrictions, it is not surprising that hospitalsare moving patients into alternative delivery systems forIGIV administration.
Hospital outpatient prospective payment under APCsis seen in government programs for administration of IGIV. Services are billed with the new C codes, theG code for the “add-on fee,” and IGIV is billed withHCPCS J codes with ASP pricing.
Hospital outpatient cost in the commercial payermarket is usually covered as a fee for service or billed
using the per diem methodology, with IGIV being billedusing an HCPCS code or an NDC and reimbursed onthe basis of AWP. Because case management is assignedand preauthorization is required, this system usually pro-vides more flexibility with off-label use. There is someconcern in the industry that the commercial model willsoon move to the government prospective paymentmodel and ASP plus 6% pricing.
The most common scenario for home infusionadministration of IGIV involves commercial payersbecause the Medicare benefit for IGIV is not a com-
prehensive benefit: it lacks coverage for the supplies,equipment, and nursing components. This drug-only coverage applies to both the Medicare Part B durablemedical equipment regional carrier (DMERC)benefit and Medicare Part D. Medicare Part B alsolimits IGIV administration to the treatment of 5 PIDdiagnoses only.
In the commercial setting, billing for home IGIV therapy is usually done on a per diem basis (usingan S code) which bundles all supplies, equipment, and
1
Table 4.
New CPT Codes for IGIV Drug AdministrationServices (Physician Office Setting)Code Descr iption of Ser vices Change From 200590765 IV infusion therapy/prophylaxis/
diagnosis; initial,≤
1 hour
Replaces G code
G034790766 IV infusion therapy/prophylaxis/diagnosis; each additional hour (after the first hour), ≤ 8 hours
Replaces G codeG0348
90767 IV infusion therapy/prophylaxis/diagnosis; additional sequentialinfusion, ≤ 1 hour
Replaces G codeG0349
90768 IV infusion therapy; concurrent infusion
Replaces G codeG0350
90772 Therapeutic, prophylactic,or diagnostic injection;subcutaneous or intramuscular
Replaces G codeG0351
Table 5.
NewC
Codes for IGIV Drug AdministrationUnder HOPPS*
Code Description of Ser vices
C8950 IV infusion therapy/diagnosis; initial, ≤ 1 hour
C8951 IV infusion therapy/diagnosis; each additionalhour †
C8957 Prolonged IV infusion requiring pump
*Old CPT codes for drug administration are no longer recognized by CMS.†Should be listed in addition to C8950 for infusions lasting >1 hour.

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 18/24
professional pharmacy services into the S9338 HCPCScode. The drug cost is typically billed using NDC andreimbursed by AWP. The nursing services are billedseparately using the 99601 nursing administration codefor the first 2 hours and 99602 for subsequent hours.This system usually requires preauthorization.
The IGIV Reimbursement FutureProposed changes for 2007 include the establishmentof unique HCPCS codes for each brand of IGIV toreplace the current system that has only 2 codes, 1 forlyophilized and 1 for nonlyophilized (liquid) products. Another possibility would be to reclassify IGIV as abiologic response modifier so it can be reimbursed atthe higher rate associated with that classification.Concerns remain regarding whether these possiblepayment increases will be sufficient to have a positiveimpact on patient care because of all the administrationcosts (discussed above).
The infusion nurse’s primary concern is patient IGIV access and quality care. Clearly, there are serious issues inthis area. Hospitals already allocate to the most needy,and physicians have begun to prolong time between infu-
sions.5
Congressional action will be needed to change theMedicare reimbursement formula to cover costs of suppliesand professional services associated with IGIV therapy,particularly in the home setting. Concerned cliniciansshould contact their US representatives and senators tourge them to enact legislation that will improve accessto IGIV for all patients who need it.
References1. Kazatchkine MD, Kaveri SV. Immunomodulation of
autoimmune and inflammatory diseases with intravenous
immune globulin. N Engl J Med.2001;345:747-755.2. Gelfand EW. Critical decisions in selecting an intravenousimmunoglobulin product. J Infus Nurs.2005;28:366-374.
3. Mahadevia PJ, Strell J, Kunaprayoon D, Gelfand E. Costsavings from intravenous immunoglobulin manufacturedfrom chromatography/caprylate (IGIV-C) in persons withprimary humoral immunodeficiency disorder.Value Health.2005;8:488-494.
4. American Society of Health-System Pharmacists.Drug products with limited availability. Available at:http://www.ashp.org/shortage/availability-notices.cfm. Accessed May 23, 2006.
5. Vogel MB. CMS responds to IVIG availability concerns with add-on payments for outpatient use.Specialty Pharm
News 2.2005.6. Advisory Committee on Blood Safety and Availability.Recommandation [sic] subject: immune globulin intra-venous (IGIV) [letter]. Available at: http://www.hhs.gov/bloodsafety/resolutions/ressept05.pdf. AccessedMay 24, 2006.
7. Brecher ME, for the Advisory Committee on Blood Safety and Availability (ACBSA). Resolutions from the ACBSA Meeting, May 16-17, 2005 [letter]. Available at:http://www.hhs.gov/bloodsafety/resolutions/resmay05.pdf.
Accessed May 24, 2006.8. Beato CV, for the Department of Health and Human
Services. Response to Brecher et al: resolutions from the ACBSA May 2005 meeting [letter]. Available at:http://www.hhs.gov/bloodsafety/responses/May2005Response.pdf. Accessed May 24, 2006.
9. US Department of Health and Human Services. Advisory Committee on Blood Safety and Availability: status of immune globulin intravenous (IGIV) products. Availableat: http://www.hhs.gov/bloodsafety/igiv.html. AccessedMay 23, 2006.
10. Agwunobi JO, for the Department of Health and HumanServices. DHHS response to ACBSA September 2005 rec-ommendations [letter]. Available at: http://www.hhs.gov/bloodsafety/responses/Sept2005Response.pdf. AccessedMay 24, 2006.
11. Immune Deficiency Foundation Web site. Available at:
www.primaryimmune.org. Accessed May 24, 2006.12. The Neuropathy Association Web site. Available at: www.neuropathy.org. Accessed May 24, 2006.
IGIV THERAPY: THE NURSE'S ROLE IN BALANCINGCOSTS AND QUALITY OF CARE
the nur se's role in balancing
costs and quality of care
optimizing patient care and outc omes
4

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 19/24
1
Self-Assessment QuestionsPlease circle your answers on the evaluation form on page 16.
1. Which of the following represents an off-label useof IGIV?a. Primary immune deficiency (PID)b. Chronic inflammatory demyelinating polyneuro-
pathy (CIDP)c. Idiopathic thrombocytopenic purpura (ITP)d. Kawasaki syndrome
2. Which of the following isnot considered an impor-tant factor in assessing patient risk prior to IGIV or IGSC therapy?a. Current diagnosisb. Comorbiditiesc. Recent food intaked. Infusion history
3. What percentage of IGIV-induced renal events inthe United States reported to the FDA between1985 and 1998 were attributable to IGIV productsstabilized with sucrose?a. 30%b. 50%c. 70%d. 90%
4. IGIV and IGSC are contraindicated in patients withselective deficiency of:a. IgM.b. IgA.c. IgG.d. IgE.
5. The optimal pH range for IGIV in solutionranges from:a. 2.0-2.5.b. 3.0-3.5.c. 4.0-4.5.d. 5.0-5.5.
6. Which of the following procedures is considered toreduce the risk of pathogenic prion transmission inIGIV products?a. Pasteurizationb. Fractionationc. Caprylate/chromatography processd. Filtration
7. During the first hour of IGIV infusion, a patient’svital signs should be assessed every:a. 10 minutes.b. 15 minutes.c. 20 minutes.d. 30 minutes.
8. The IGIV reimbursement allocation implementedin early 2006 in the hospital outpatient setting forMedicare reimbursement (but not for commercialinsurance reimbursement) was:a. 85% of AWP.b. AWP plus 6%.c. 85% of ASP.d. ASP plus 6%.
9. Which group has the greatest leverage on IGIV purchasing costs?a. Physiciansb. Hospitals, long-term care, skilled nursing facilitiesc. Home infusion providersd. Retail pharmacies/specialty pharmacies
10. Medicare ASP plus 6% reimbursement rates areupdated:
a. Monthly.b. Quarterly.c. Semi-annually.d. Annually.

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 20/24
IGIV THERAPY: THE NURSE'S ROLE IN BALANCINGCOSTS AND QUALITY OF CARE
the nur se's role in balancing
costs and quality of care
optimizing patient care and outc omes
6
Photocopy and fax evaluation form to 402.559.6379 or mail it to University of Nebraska Medical Center College of
Continuing Nursing Education, 985330 Nebraska Medical Center, Omaha, NE 68198-5330, prior to July 30, 2007.Please print legibly. This form will be used to generate and mail your certificate within 4 to 6 weeks.
Activity Title: IGIV Therapy: The Nurse’s Role in Balancing Costs and Quality of Care Target Audience: Infusion Nurses Designated Contact Hour(s): 1.2 (with 70% or more correct)Goal: To familiarize infusion nurses with immune globulin products, safety and tolerability considerations, and issues regarding costs and reimbursement.
We would like your opinion regarding this educational activity. Please complete the evaluation form, includinself-assessment answers, and return it to the address or fax number indicated above.1.As a result of completing this learning activity are you now better able to: Yes No Some
a. Describe the differences among currently available immune globulinproducts and their impact on safety, tolerability, and economic considerations? ■ ■ ■
b. Discuss key policies and procedures related to reimbursement for immuneglobulin therapy in various clinical settings? ■ ■ ■
2. Were the objectives of this learning activity as stated initem #1 above related to its overall goal? ■ ■ ■
3. Was the content of this learning activity clearly written? ■ ■ ■
4. Was the content of this activity free of commercial bias? ■ ■ ■
5. Was the information/content relevant to your clinical practice? ■ ■ ■
If you answered NO or SOMEWHAT to any items above, please explain: _______________________________________________________________________________________________________________________
Please rank each of the formats below in order of preference from 1 (highest) to 8 (lowest).__ Teleconferences __ Home Study (printed) __ Home Study (CD-ROM) __ Internet-based__ Grand Rounds __ Symposia __ Roundtables __ Association Meetings
Comments/suggestions for future activities: ______________________________________________________I certify that I have completed this activity and the actual time I spent was:
■ 40 min ■ 50 min ■ 60 min ■ 75 min ■ Other (fill in number of minutes: ______)Signature ______________________________________________________________ Date ______________
ANSWER GRID (please circle 1 answer per question)1. a b c d 6. a b c d2. a b c d 7. a b c d3. a b c d 8. a b c d4. a b c d 9. a b c d5. a b c d 10. a b c d
Please contact the Continuing Education Alliance at [email protected] for questions regarding thisCTE32606
University of Nebraska Medical Center Evaluation Form for Nurses
First Name Middle Initial
Last Name Degree(s)
Address
City State ZIP Code
Phone Fax

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 21/24
1
NOTES

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 22/24
IGIV THERAPY: THE NURSE'S ROLE IN BALANCINGCOSTS AND QUALITY OF CARE
the nur se's role in balancing
costs and quality of care
optimizing patient care and outc omes
8
NOTES

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 23/24

8/3/2019 Talecris Infusion RN CE Program 2006
http://slidepdf.com/reader/full/talecris-infusion-rn-ce-program-2006 24/24
P R E
S O R T E D
S T A N D A R D
U S P
O S T A
G E
P A I D
L O U I S V I L L E K Y
P E R MI T 1
8 0 1
C on
t i n ui n
g
E d u c a t i onA l l i an
c e
O n
e S o un
d
S h or eD r i v
e , S ui t e2 1
0
G r e
enwi c h
, C T 0 6 8 3 0
I G I V T H E R A P Y :
T HE
N UR
S E ' S R
OL E I NB AL A
N CI N
G
A
D
A
Y
AR