Embed Size (px)
Citation preview

Dallas, TX • November 2–4, 2012
Peripheral Infusion
Complications Leading to
Sentinel EventsPresented by Pam Ohls, MSN, RN
RN Director, Clinical Education
Banner Health System

Dallas, TX • November 2–4, 2012
Peripheral Infusion Complications Leading to Sentinel Events
Session Code:101 Contact Hours: 0.8 CRNI Units: 2Please use session code shown above when completing
your speaker evaluation and CE form.
Return the evaluation to the registration desk or receptacles located outside meeting rooms at the end of the day.
Handouts for this session are available online at www.ins1.org. Session recordings will also be available post-meeting courtesy of
B.Braun Medical/Aesculap Academy.
As a courtesy to both presenters and attendees, please turn off all cell phones and refrain from talking during the session.
Tonight’s Event:Industrial Exhibition and Networking Reception
3:30-5:30pm

Dallas, TX • November 2–4, 2012
Objectives
• Discuss complications associated with peripheral IV therapy
• Discuss strategies to improve outcomes for patients receiving peripheral IV therapy

Dallas, TX • November 2–4, 2012
Case Presentation
• Geriatric-aged Caucasian female presented to ED-auto accident-back pain
• IV started, CT Head, pain meds, labs• Pain meds, K+, procedure for back
scheduled Monday. IV restarted on Friday on day 3.
• Old IV site continues to become more reddened over 2 days, wound consult.

Dallas, TX • November 2–4, 2012
Case Presentation
• Procedure cancelled on Monday. Pt febrile, BP dropped. To ICU.
• Diagnosis-Sepsis
• Patient expired 24 hours after admit to ICU
• Final diagnosis-sepsis from infected IV site-per Infectious Disease Physician.

Dallas, TX • November 2–4, 2012
Sentinel Event
• Defined by the Joint Commission (TJC)
• Unanticipated event
• Results in death, serious physical or psychological injury

Dallas, TX • November 2–4, 2012
Root Cause Analysis
• Involves interdisciplinary experts from the departments associated with the event
• Involves those who are the most familiar with the situation
• Digs deeper by repeatedly asking why at each level of cause and effect.
• Identifies changes needed to be made to systems
• Be impartial as possible

Dallas, TX • November 2–4, 2012
Goal of RCA
• What happened?
• Why did it happen?
• What do you do to prevent it from happening again?

Dallas, TX • November 2–4, 2012
Effective & Thorough
• Determine human factors • Analysis of related processes• Analysis of underlying cause and effect
systems through a series of why questions
• Identification of risks & their potential contributions
• Determination of potential improvement in processes or systems

Dallas, TX • November 2–4, 2012
Cause & Effect Diagram
Human Factors-Communication
Barriers/SafeguardsEquipment and Environmental Factors
Event
(Septic IV Site)
Human Factors-
Training
Human Factors-
Fatigue / Scheduling
Rules, Policies, Procedures, Leadership

Dallas, TX • November 2–4, 2012
Define PIV Terms for Team
• Phlebitis-expected/anticipated?
• Infiltration-expected/anticipated?
• Infection source from PIV?

Dallas, TX • November 2–4, 2012
Phlebitis• Defined as erythema, pain, swelling and or venous cord
along the PIV site.• Classified as:
– Chemical– Mechanical– Bacterial

Dallas, TX • November 2–4, 2012
Phlebitis
• Rates range from 2-80%
• INS recommendation rate 5% or less
• Risk factors– Drug related– Patient related– Health care related
Dallas, TX • November 2–4, 2012
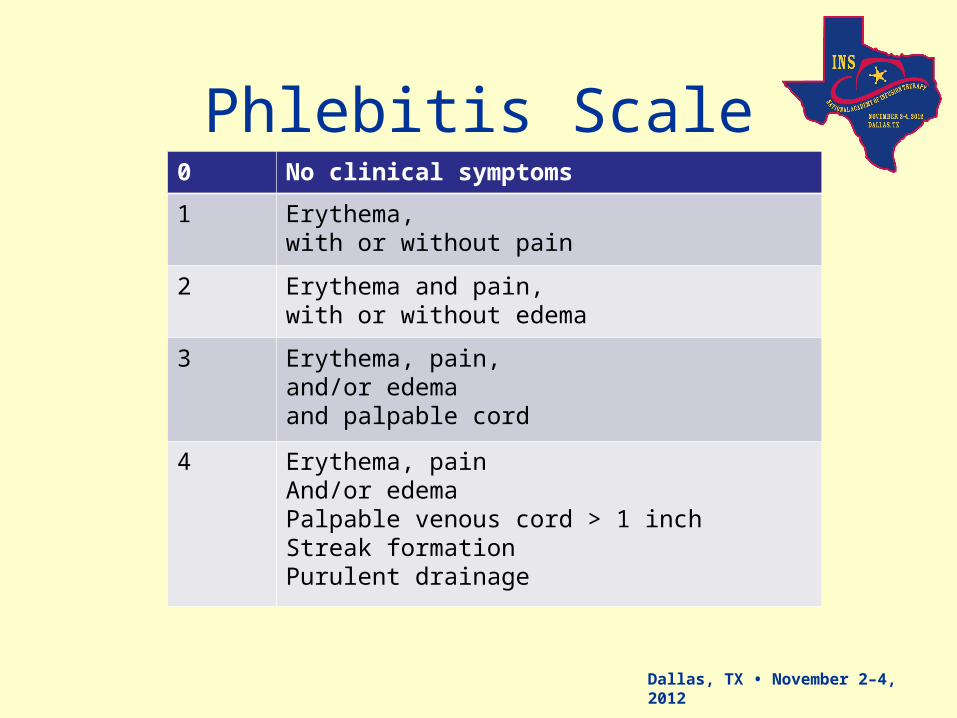
Phlebitis Scale0 No clinical symptoms
1 Erythema, with or without pain
2 Erythema and pain, with or without edema
3 Erythema, pain, and/or edema and palpable cord
4 Erythema, painAnd/or edemaPalpable venous cord > 1 inchStreak formationPurulent drainage

Dallas, TX • November 2–4, 2012
Chemical Phlebitis
• Typically associated with peripheral-short venous access devices, i.e., peripheral IV or Midlines.

Dallas, TX • November 2–4, 2012
Infiltration/Extravasation• Infiltration: inadvertent administration of a non
vesicant into the surrounding tissue.
• Extravasation: an inadvertent delivery of a vesicant into the tissues. Vesicants cause blistering, severe tissue damage, and even necrosis if extravasated.

Dallas, TX • November 2–4, 2012
Grade Clinical Criteria0 No signs or symptoms
1 •Skin blanched•Edema less than 1 inch
2 •Cool to touch •With or without pain•Skin blanched •Edema 1-6 inches in any direction
3 •Cool to touch•With or without pain•Skin blanched•Edema greater than 6 inches
4 •Cool to touch•Mild-mod pain•Possible numbness•Skin discolored •Gross edema greater than 6 inches•Circulatory impairment•Infiltration of any blood product, irritant, or vesicant
Infiltration Scale

Dallas, TX • November 2–4, 2012
Extreme pH IV Medications
pH <5
Ciprofloxin 3.3-4.6
Dopamine 2.5-5.0
Doxycycline 1.8-3.3
Morphine 2.5
Potassium 4.0
Pentamidine 4.1-5.4
Phenergan 4.0
Taxol 4.4-5.6
Vancomycin 2.4
Zofran 3.0-4.0
pH >9
Acyclovir 10.5-11.6
Ampicillin 8.0-10
Bactrim 10
Cerebyx 8.6-9.0
5FU 9.2
Ganciclovir 9-11
Phenytoin 12
Protonix 9-10.5

Dallas, TX • November 2–4, 2012
Classified Vesicant Infusates
• Acyclovir• Amiordarone• Ampho B• Ampicillin• Aramine• Bactrim• Calcium chloride• Calcium Gluconate 10%• Ciprofloxacin• Cerebyx• Contrast media
•Daptinomycin•Dextrose >10%•Digitoxin•Dobutamine•Dopamine•Doxapram•Doxycycline•Epinephrine•Erythromycin•Gancyclovir•Gentamycin

Dallas, TX • November 2–4, 2012
Vesicant InfusatesLevophed
Lorazepram
Magnesium sulfate
Mannitol 10% and 20%
Morphine
Nafcillin
Norepinephrine
Phenergan
Phenytoin
Phenylephrine
Pentamadine
PhenytoinPiperacillinPotassium chlorideProtonixSodium BicarbonateTaxolThiopentalValiumVancomycinVasopressinZofranZosyn

Dallas, TX • November 2–4, 2012
Mechanical Phlebitis• Associated with placement of device or extremity
movement resulting in irritation of vein intima • Early-stage mechanical phlebitis caused by
mechanical irritation of vein endothelium– Signs and symptoms are tenderness, erythema,
and edema

Dallas, TX • November 2–4, 2012
Bacterial Phlebitis• Inflammation of the vein intima associated with
bacterial infection• Less frequently seen but more serious because it
predisposes patient to systemic complications

Dallas, TX • November 2–4, 2012
Review of Literature
• 30-80% PIV during hospitalization
• 50% PIV placed in ED-routine procedure, but not used
• 150 million PIV placed annually– 15x higher than central lines
• Most literature focuses phlebitis and infiltration
• IV site change or needed
(ZIngg & Pittett, 2009)

Dallas, TX • November 2–4, 2012
Maki, Kluger, Crnich (2006)
• Meta-analysis of 200 prospective studies
• PIV BSI rate: 0.5 per 1000 device days
• Over 330 million PIV in US each year

Dallas, TX • November 2–4, 2012
Pujol, Hornero, Saballs et al. (2007).
• Prospective study-catheter related BSI
• 2001-2003
• Non-ICU patients
• 147 patients – 77 PIV (0.19/1000 patient days)– 73 CVC (0.18/1000 patient days)
• PIV infections– Inserted in ED, Staph aureus, 27%
mortality rate

Dallas, TX • November 2–4, 2012
Zingg & Pittet, (2009)
• Current data report PIV incidence density rates of 0.2-0.7 episodes per 1000 device days.
• 5-25% PIV colonized with bacteria at time of removal.
• Rare event or serious health care problem?

Dallas, TX • November 2–4, 2012
Trinh, Chan, Edwards, et al. (2011).
• Retrospective study-adult patients-2005-2008
• 24 PIV, median duration 3 days
• Site-antecubital, placed in ED or outside facility (p=.005)
• Treatment-19 days antibiotics
Dallas, TX • November 2–4, 2012
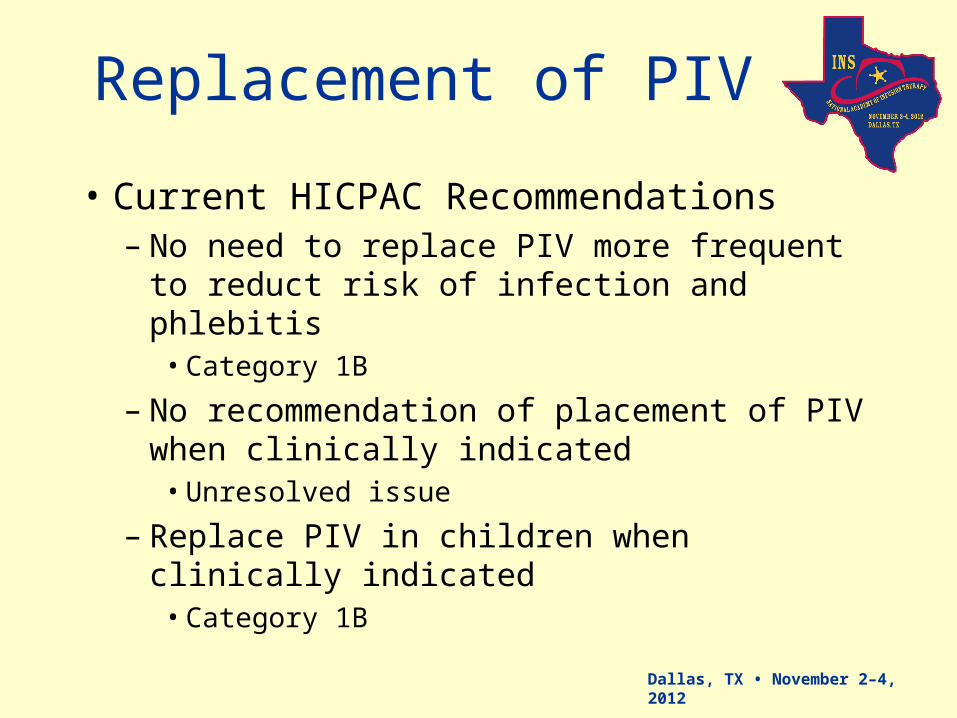
Replacement of PIV
• Current HICPAC Recommendations– No need to replace PIV more frequent to
reduct risk of infection and phlebitis• Category 1B
– No recommendation of placement of PIV when clinically indicated
• Unresolved issue
– Replace PIV in children when clinically indicated
• Category 1B

Dallas, TX • November 2–4, 2012
Policies & ProceduresCurrent Practice
• Change IV sites every three days, sooner if reddened
• Check for blood return for chemotherapy
• Check for blood return for vesicants
• Contrast Media is a vesicant?

Dallas, TX • November 2–4, 2012
What Effect Did Contrast Have on the
PIV?• What is the practice of Medical
Imaging?
• What is the policy?
• How old are the IV’s used for Contrast?
• Did the nurse change the IV site according to policy?
• Do we have a policy on Contrast Media and what do we know about Contrast?

Dallas, TX • November 2–4, 2012
Contrast Media Osmolarity

Dallas, TX • November 2–4, 2012
Equipment/Patient
;;;;;
• Contrast Injected 1-6mL per second

Dallas, TX • November 2–4, 2012
CT Rates of Injection
• 1mL per second = 3600 mL/hour
• 2mL per second = 7200 mL/hour
• 3mL per second = 10,800 mL/hour
• 4mL per second = 14,400 mL/hour
• 5mL per second = 18,000 mL/hour
• 6mL per second = 21,600 mL/hour

Dallas, TX • November 2–4, 2012
Contrast Extravasation

Dallas, TX • November 2–4, 2012
Facts About Contrast Media
• Vesicant
• Continues to burn intima of veins for 48 hours after administration
• Administration of contrast via IV in place longer than 20 hours increases risk of extravasation and phlebitis
• Multiple attempts at IV access at same site increases risk of extravasation
Patient Safety Advisory (2004), Extravasation of Radiologic Contrast
Dallas, TX • November 2–4, 2012
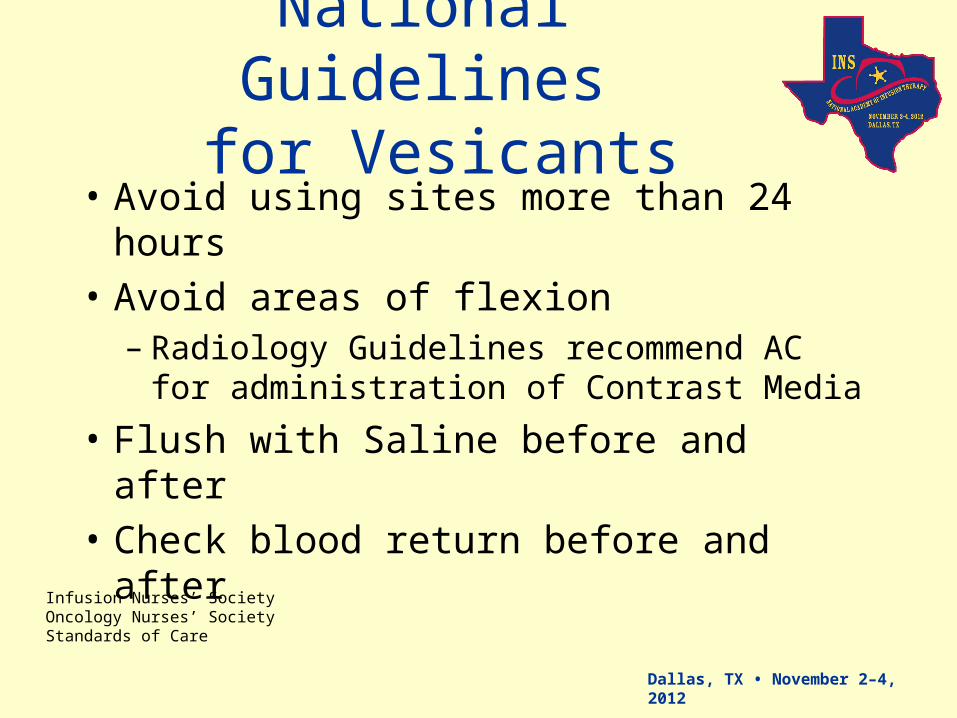
National Guidelines for Vesicants
• Avoid using sites more than 24 hours
• Avoid areas of flexion– Radiology Guidelines recommend AC for
administration of Contrast Media
• Flush with Saline before and after
• Check blood return before and after
Infusion Nurses’ Society Oncology Nurses’ SocietyStandards of Care

Dallas, TX • November 2–4, 2012
Question
• What affect did Contrast have with the other medications she was receiving– Morphine– Potassium– Zofran

Dallas, TX • November 2–4, 2012
Ask Questions
• What is the practice of CT Techs?
• Check for blood return?
• Check for patency?
• Scrub hub?
• Flush with Saline before and after?
• How old the IV site?

Dallas, TX • November 2–4, 2012
The questions
• CT check for blood return?
• Power injected?
• What other medications through IV site?
• How long do IV’s last after administration of Contrast Media

Dallas, TX • November 2–4, 2012
Results
• Collected data on 60 patients for CT & MRI
• Magnevist MRI-1960milli/osmL
• Omnipaque 350-844milli/osmL
• 60 patients, 63% (n=38) no extravasation or phlebitis
• 69% no blood return prior to injection
Kirschner, R. (2010).

Dallas, TX • November 2–4, 2012
Results
• 60 patients, 31% (n=22) had concurrent vesicant therapies
• 100% (n=22) developed phlebitis within 24 hours contrast and another vesicant– (n=10) MRI contrast– (n=12) CT contrast
• All CT patients power injected• No MRI patients power injected
Dallas, TX • November 2–4, 2012
Which Medications?
• Zofran
• Potassium
• Morphine
• Protonix
• Vancomycin

Dallas, TX • November 2–4, 2012
Action Plans
• All PIVs need to be started with 24 hours of contrast media
• All CT techs check for date of insertion before administration of contrast
• All CT techs check for blood return before administration of contrast
• If not within 24 hours and no blood return-restart PIV

Dallas, TX • November 2–4, 2012
Post Administration
• Discern alert placed in electronic documementation for nurses, alerting them to administration of contrast and top 5 medication. Site may develop phlebitis and may need changed within 24 hours.

Dallas, TX • November 2–4, 2012
Resource Team Assistance
Dallas, TX • November 2–4, 2012
Literature
• 90% of patients require PIV for procedures/medications
• IV education and skills have removed from many nursing school curriculum after Hegstad and Zsohar (1986) study showed no difference in outcomes from simulation versus live practice for IV skills
• Mentoring with an expert has been shown to improves skills and confidence (McGee, 2001)

Dallas, TX • November 2–4, 2012
Experience with IV’s16 participants (n = 16)
The mean age of participants was 30 years (range 23 – 44 years).
The majority of participants were female (n = 15)
Most staff nurses had one to five years of RN experience (n = 9)
About half of the participants worked on a med/surg unit as a staff RN (n = 8), while the other half were staff nurses in PCU or ICU (n = 7). One participant was from WIS.
Participants’ highest level of nursing education was equally divided
ADN (n = 8) and BSN (n = 8).
All but one participant had experience inserting IVs in nursing school.
The majority of participants (n = 14) had experience inserting IVs on both patients and mannequins / IV arms.
Practice with IV in nursing school varied
never (n=1)
one to two times (n=1)
three and five times (n = 8)
six to ten times (n = 4)
more than ten times (n = 2)

Dallas, TX • November 2–4, 2012
Human Factors-Training
• Ultrasound IV insertions
• Education
• Competency
• Outcomes

Dallas, TX • November 2–4, 2012
IV Cannulation OutcomesUsing 1 ¼” needles with US
622 IVs
242-41% failed in under 24 hours
531-90% failed in under 48 hours
62-10% made it to 72 hours
After 24 hours
Upper arm fails 78%
Antecubital fails 41%
Lower arm fails 28%
Unpublished data, Royer, T. (2006).

Dallas, TX • November 2–4, 2012
Length and Size of Needles
• The deeper the vein, the less needle in the vein.• Use longer catheters: 1 ¾ inch• No deeper than 1cm• Site selection:
– Lower arm– Upper arm-Cephalic veins– Antecubital

Dallas, TX • November 2–4, 2012
Bacterial Phlebitis• Inflammation of the vein intima associated with
bacterial infection• Less frequently seen but more serious because it
predisposes patient to systemic complications• Type of ultrasound gel for assessing and accessing
the vein– Clean to assess– Sterile to access
cleansterile
sterile
Dallas, TX • November 2–4, 2012
Claims and Dollars for the Systemfor Claims where
Medication Error was the Primary Event
Year No. Amount Incurred
• 2005 130 $ 2 million
• 2006 130 $ 5 million
• 2007 130 $ 7 million

Dallas, TX • November 2–4, 2012
Common Problems Identified in Claims
• Infiltration of IV contrast 14 of 58 claims
• Poor charting of IV site assessment
• IV not changed when patient complains
• IV not changed per policy
• MRSA infections after IV removed

Dallas, TX • November 2–4, 2012
Scope of Practice
• Anatomy and physiology limbs, to include vein, artery, and nerves
• Assessment of vessels• Appropriate vessels and cannulation techniques• Aseptic technique• Appropriate length and size of needles• Complications, management, and troubleshooting

Dallas, TX • November 2–4, 2012
Strategies
• Assessment of nurses’ IV knowledge and skills on hire
• Precepting and mentorship IV skills and knowledge
• Education, skills, competencies for US IV insertion
• Assessment of IV practice in your facility for vesicants/contrast media

Dallas, TX • November 2–4, 2012
Guidelines for PIV insertion

Dallas, TX • November 2–4, 2012
Algorhythm for Right Line?

Dallas, TX • November 2–4, 2012
Competencies

Dallas, TX • November 2–4, 2012
Summary• Assessment of knowledge,
competencies, practices, and policies
• Policies and Procedures
• Documentation
• INS Standards of Practice
• All nurses who start IVs are Infusion Nurses, not just nurses who are on IV teams and insert PICC lines
Dallas, TX • November 2–4, 2012
References• ECRI (2004). Extravasation of Radiologic Contrast, Patient Safety Advisory,
1(3), 1-5. • Infusion Nurses Society Standards of Practice, (2011). • Kirschner, R. (2010). Contrast media-Phlebitis implications. US Radiology,
27-30. • Maki, D., Kluger, D., Crnich, C. (2006). The risk of bloodstream infection in
adults with different intravascular devices: A systematic review of 200 published prospective studies. Mayo Clin Proc, 81(9), 1159-1171
• Pujol, M., Hornero, A., Saballs, M., et al. (2007). Clinical epidemiology and outcomes of PIV related blood stream infection at a university-affiliated hospital. Journal of Hospital Infection, 67(1), 22-29.
• Royer, T. (2006). Unpublished data for US IV Insertion.• Trinh, T., Chan, P., Edwards, O, et al. (2011). Peripheral venous catheter-
rated staphylococcus aureus bacteremia. Infection Control and Hospital Epidemiology, 32(6).
• Zingg, W. & Pittet, D. (2009). Peripheral venous catheters: An under-evaluated problem. International Journal of Antimicrobial Agents, 34S. S38-S42.





























