Embed Size (px)
Citation preview
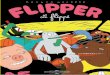
Taking Advanced Dentistry to Exceptional!
PORC. TO ZIRCONIAPARADIGM
DELIVER BY 5PM ON
E.MAX
ALL ZIRCONIA
77% AU - HIGH NOBLE59% AU - HIGH NOBLE50% AU - NOBLE20% AU - NOBLENOBLE WHITENON-PRECIOUS
Rev. 12/26/12
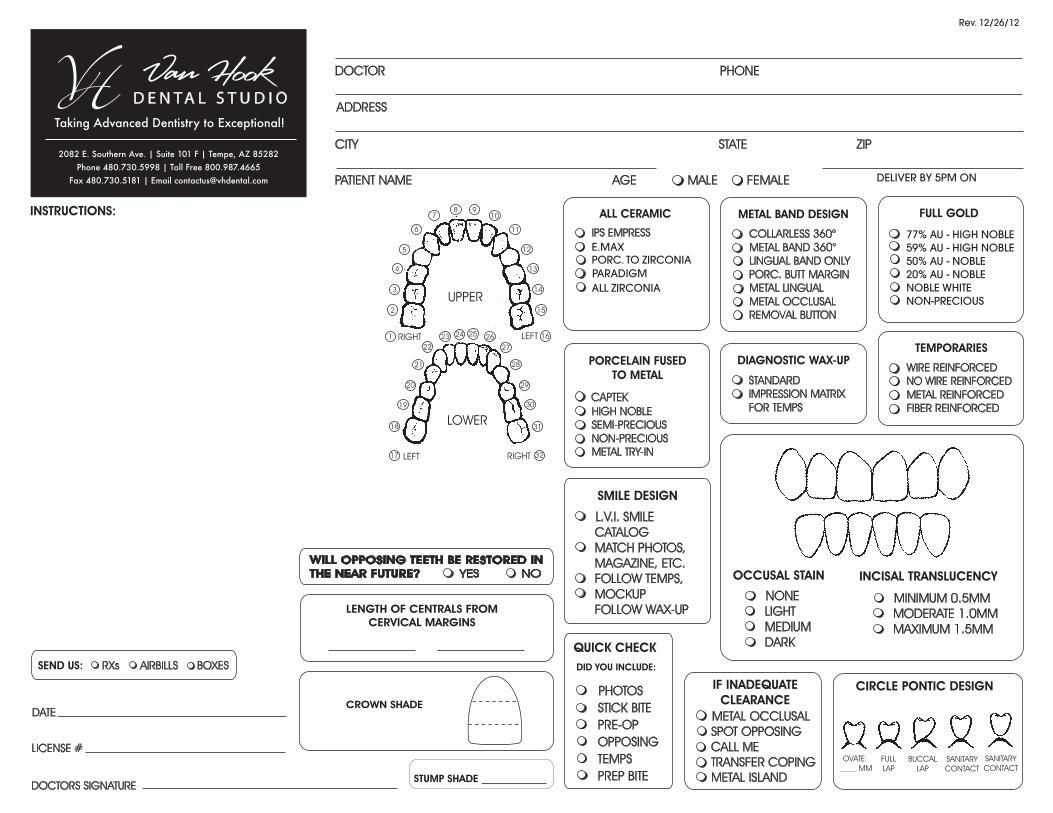
Taking Advanced Dentistry to Exceptional!
Removable
OCCLUSAL RIM
TRIAD BASEPROCESSED BASE (SR-IVOCAP)
SEND US:
RXS AIRBILLSBOXES
PARTIAL DENTURES
ALL ACRYLIC (FLIPPER)
FLEXIBLE
CAST FRAMEWORK
CAST W/TOOTH COLORED CLASP
SHADE ___________
NIGHTGUARDS
UPPER
LOWER
SOFT THEROMOPLASTIC
HARD SR-IVOCAP
FLAT PLANE W/ ANTERIOR GUIDANCE
FLAT PLANE
FULL DENTURES
SET-UP
IDEAL
CHARACTERIZED
FOLLOW WAX RIM
FINISH
SMOOTH
ANATOMICAL
COLOR ____________
IMPLANT BAR (CAD/CAM)
HYBRID
HADER BAR - TISSUE BORNE
DOLDER BAR - IMPLANT BORNE
PRIMARY MILLED
SWISS LOC
LEW PASSIVE
BREDENT VKS
LOCATOR
CEKA
ERA
OTHER _________________________
ENCLOSED WITH CASE
IMPRESSIONS
MODELS
BITES
PHOTOS
SCREWS
ARTICULATOR
FRAMEWORK DESIGN
LAB DESIGN
MAXILLARY TOOTH #
HORSESHOE __________________
CIRCULAR BAR (A-P) __________________
MANDIBULAR
LINGUAL BAR __________________
LINGUAL PLATE __________________
FLEXIBLE __________________
RELINES
HARD (HEAT CURED)
SOFT
REPAIRS
REPAIR
(DESCRIBE IN RX)
Compliant Denture Identi�cation
Patient Accepts (additional $25)
Patient Declines
DELIVER BY 5PM ON
ATTACHMENTS
CLASPING
I-BAR __________________
AKERS __________________
ROACH (T-CLASP) __________________
CLASP TOOTH COLOR __________________
CLASP CLEAR __________________
FLEXIBLE __________________
Rev. 12/26/12
DOCTOR
ADDRESS
CITY STATE ZIP
PHONE
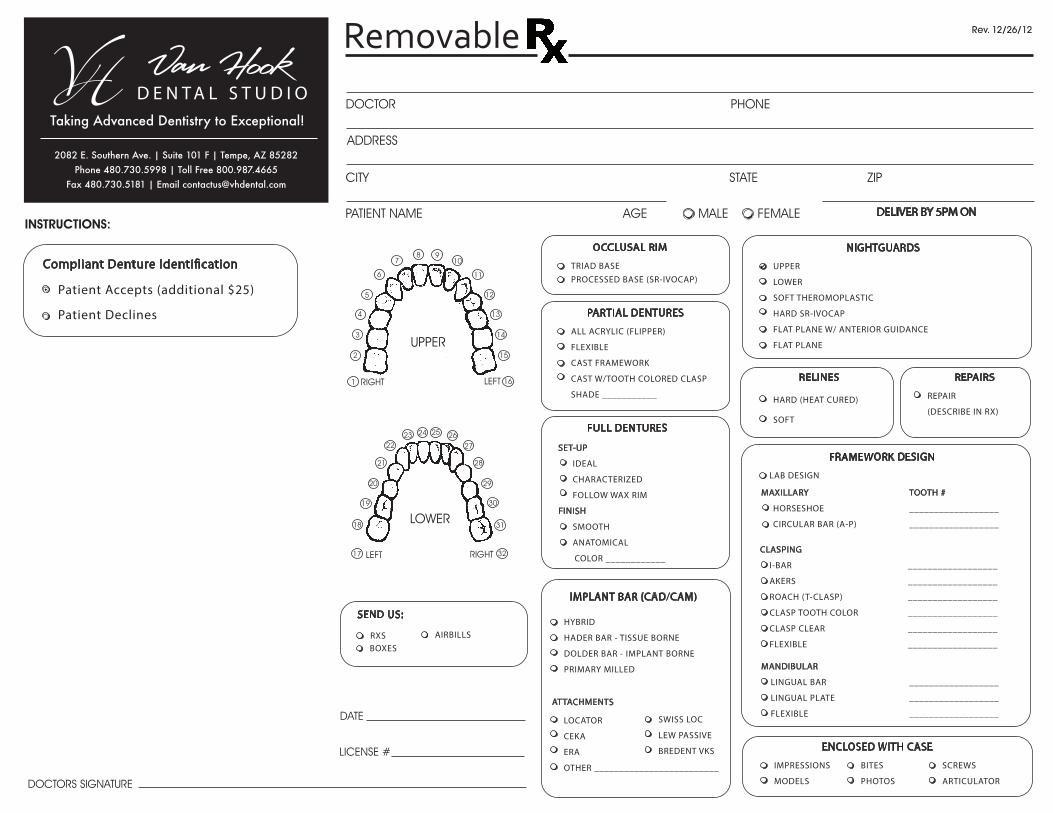
Van Hook Dental Studio now offers and recommends the All-Esthetic Package for your
anterior restorations!
PATIENT NAME AGE MALE/FEMALE
TODAY’S DATE DELIVER BY 5PM ON
DOCTOR SIGNATURE
SHADE
TOOTH #
LICENSE NUMBER
All-Exclusive Implant Solution
Instructions:
Select Abutment and Crown:$499 Titanium Abutment/PFM Crown*
$499 Titanium Abutment/Bruxzir Type Crown*
$499 Titanium Abutment/Zirconia Crown*
*INCLUDES: Lab and Final Screw, Lab Analog, Easy-Place Jig Tissue Model, Shipping and Handling of Parts
**Lab and Final Screw, Lab Analog, Easy-Place Jig, Tissue Model, Shipping and Handling of Parts
INCLUDES
10 DAYSIN LAB
Van HookDENTAL STUDIO
Van Hook Dental Studio, Inc.480.730.5998 | [email protected] | vhdental.com
2082 E Southern Ave | Suite 101F | Tempe, AZ 85282
NEW!All-Esthetic Package!**
$599 Zirconia All-Esthetic Package w/Crown**(recommended for anterior)
Terms: Pricing excludes 3% pass-through MDET. Limited to approved platforms. Payments not recieved within 30 days of statement date are subject to a 2% per month service charge. Account balances exceeding60 days will be placed on C.O.D. Prices subject to change without notice. Warranty information available upon request. Rev. 04/13
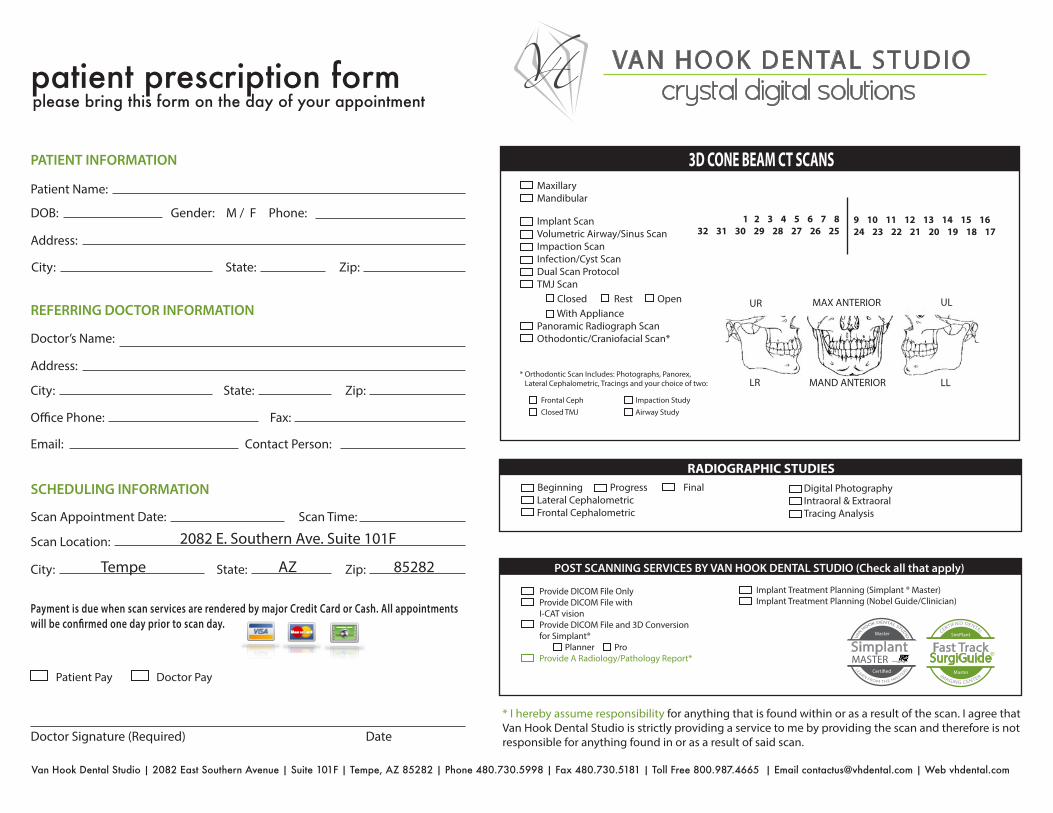
patient prescription form
Lateral CephalometricFrontal Cephalometric
Digital PhotographyIntraoral & ExtraoralTracing Analysis
Beginning Progress Final
RADIOGRAPHIC STUDIES
3D CONE BEAM CT SCANS
* I hereby assume responsibility for anything that is found within or as a result of the scan. I agree that Van Hook Dental Studio is strictly providing a service to me by providing the scan and therefore is not responsible for anything found in or as a result of said scan.
Patient Name:
DOB: Gender: M / F
Address:
City: State: Zip:
Phone:
PATIENT INFORMATION
REFERRING DOCTOR INFORMATION
Doctor’s Name:
Contact Person:
Address:
City: State: Zip:
O�ce Phone: Fax:
Email:
SCHEDULING INFORMATION
Scan Appointment Date: Scan Time:
Scan Location:
City:
Doctor Signature (Required) Date
State: Zip:
Payment is due when scan services are rendered by major Credit Card or Cash. All appointments will be con�rmed one day prior to scan day.
POST SCANNING SERVICES BY VAN HOOK DENTAL STUDIO (Check all that apply)
Provide DICOM File OnlyProvide DICOM File with I-CAT visionProvide DICOM File and 3D Conversion for Simplant® Planner Pro Provide A Radiology/Pathology Report*
Implant Treatment Planning (Simplant ® Master)Implant Treatment Planning (Nobel Guide/Clinician)
1 2 3 4 5 6 7 832 31 30 29 28 27 26 25
9 10 11 12 13 14 15 1624 23 22 21 20 19 18 17
UR
LR
MAX ANTERIOR
MAND ANTERIOR
UL
LL
Implant ScanVolumetric Airway/Sinus ScanImpaction ScanInfection/Cyst ScanDual Scan ProtocolTMJ Scan Closed Rest Open With Appliance Panoramic Radiograph ScanOthodontic/Craniofacial Scan*
Frontal CephClosed TMJ
Impaction StudyAirway Study
* Orthodontic Scan Includes: Photographs, Panorex, Lateral Cephalometric, Tracings and your choice of two:
MaxillaryMandibular
Master
Certi�ed
Fast TrackSurgiGuide
Master
SimPlant
RSimplantMASTER
Master
Certi�ed
please bring this form on the day of your appointment
Patient Pay Doctor Pay
Van Hook Dental Studio | 2082 East Southern Avenue | Suite 101F | Tempe, AZ 85282 | Phone 480.730.5998 | Fax 480.730.5181 | Toll Free 800.987.4665 | Email [email protected] | Web vhdental.com
crystal digital solutionsVAN HOOK DENTAL STUDIO
2082 E. Southern Ave. Suite 101F
Tempe AZ 85282