Embed Size (px)
Citation preview

lable at ScienceDirect
Complementary Therapies in Clinical Practice 15 (2009) 158–160
Contents lists avai
Complementary Therapies in Clinical Practice
journal homepage: www.elsevier .com/locate/ctnm
Tactile massage within the primary health care setting
Katarina Andersson*, Lena Tornkvist, Per WandellCenter for Family and Community Medicine, Karolinska Institutet, Alfred Nobels Alle 12, SE-141 83 Huddinge, Sweden
* Corresponding author. Tel.: þ46 704845372; fax:E-mail addresses: katarina.andersson5@comhem
karolinska.se (K. Andersson).
1744-3881/$ – see front matter � 2009 Elsevier Ltd.doi:10.1016/j.ctcp.2008.10.007
a b s t r a c t
This paper describes an observational study describing how Tactile Massage (TM) was integrated intoSwedish clinical medical care, the impact of this initiative suggests a foundation for future research.Subjects completed three questionnaires pre- and post-tactile massage. These were: Sense of Coherence(SOC), an enlarged Health Index (HI) and the Borg CR10 scale.
Results: A convenience sample of forty-three subjects (37 women and 6 men) were referred to TMtreatment for a range of problems including for pain, sleep disorders, inability to move, headache andtense body. Patients received 10 TM treatments, each lasting approx. 1 h in length. The enlarged HIquestionnaire indicated that eleven out of fourteen parameters were significantly affected according(p-values between 0.0015 and <0.001). These included energy, mood, tiredness, sleep, pain, movement,health, general health and physical health. Pain reduction was also significantly reduced using the BorgCR10 scale (p< 0.001).
Conclusion: TM seems to affect several dimensions of health, and this should be explored more fully infuture research.
� 2009 Elsevier Ltd. All rights reserved.
1. Introduction
Thirty years ago Ardeby, a Swedish nurse, developed tactilemassage (TM). TM and classic Swedish massage differ. TM followsa set of patterns involving touch and light pressure and focuses onsensory integration excluding deep tissue massage.1,2
In contrast Swedish massage systematically manipulates softtissue through: effleurage (light gliding over the skin), petrissage(lifting, pressing and kneading skin and muscles), friction (rubbingskin and muscles), tapotement (rapid, tapping, rhythmical move-ments on skin and muscles) and vibration (vibration of the skin).3–5
Patients currently receive TM for a wide range of symptomaticrelief1,6–15 such as rheumatic diseases, stroke rehabilitation andnausea during pregnancy.6,10,14 Patients recovering from cerebralvascular accidents (CVA) have reported improved quality of lifefollowing TM.14 TM may also provide a complementary treatmentfor stress-related diseases.
In Sweden, the TM method has been integrated in clinical/medical care in several primary health care centres (PHCs).Seventy-five percent of Stockholm residents surveyed in 2000 were
þ46 8 524 886 24..se, katarina.2.andersson@
All rights reserved.
positive towards further research into complementary medicineand felt that such care should be provided through the publiclyfunded healthcare system.16
The authors have previously completed two studies about TM,a pilot study exploring the effects of TM on blood glucose levels inpatients with type 2 diabetes and about practitioners experience ofworking with TM.8,9
2. Design and setting
This observational study was conducted across six PHCs inStockholm, Sweden.
In Sweden, training in Tactile Massage requires 1-week theoryand practice followed by an additional 60 h of documentedpractice culminating in a theoretical and practical examination. Allpractitioners had undergone this training, were certified and alsotraining district nurses. Patient referral was usually fromphysicians.
TM treatment involves specific movements. Treatment starts onthe backs of the legs, back, nape of the neck and scalp. Followingthis the face, chest, stomach, arms, hands, and fingers, front of legs,feet and toes are lightly massaged. Massage occurs slowly in orderto achieve a calm ‘awakening’ and gentle music played duringtreatment.

Table 1Median values (95% CI) of quality of life (HI) and Sense of Coherence (SOC) estimates,or number (%) in different SOC groups, before and after treatment by tactile massage(TM) (n¼ 43), with differences by Wilcoxon’s paired test or Fisher’s exact test.
Before TM After TM Wilcoxon’s test, p-value
Energy 2 (2;2) 3 (2;3) 0.0005Mood 2 (2;3) 3 (3;3) 0.0000Tiredness 1 (1;2) 2 (2;2) 0.0000Loneliness 3 (2;3) 3 (2;3) 0.4048Sleep 2 (1;2) 2 (2;3) 0.0001Vertigo 3 (2;3) 3 (2;3) 0.2686Digestion 3 (2;3) 3 (3;3) 0.1873Pain 1 (1;1) 2 (2;2) 0.0001Movement 3 (2;3) 3 (3;3) 0.0015Health 2 (2;2) 3 (2;3) 0.0002Work performance 2 (2;3) 3 (2;3) 0.3429General health 2 (2;2) 3 (2;3) 0.0005Physical health 2 (2;2) 3 (2;3) 0.0000Emotional health 3 (2;3) 3 (3;3) 0.0183Pain estimate (Borg) 7 (5;8) 5 (4;6) 0.0006SOC, points 55 (48;64.8) 60.5 (49.6;67.4) 0.2283SOC, by group 0.000
Low 22 (61%) 19 (51%)Medium 10 (28%) 14 (38%)High 4 (11%) 4 (11%)
K. Andersson et al. / Complementary Therapies in Clinical Practice 15 (2009) 158–160 159
3. Participants and inclusion criteria
A convenience sample was drawn from men and women whowere over the age of 18 years, not pregnant or who had beendiagnosed with women or persons whose health did not allowparticipation. Participation was voluntary and patients whodeclined participation in the study received TM treatment unre-lated to the study. Patients registering their interest in participatingin the evaluation were informed both orally and in writing aboutthe study and that all information would be treated confidentially.The Southern Research Ethics Committee of Karolinska Institutet atHuddinge University Hospital approved the study (Dnr 371/02).
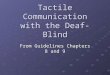
Pre- and post-TM participants completed three questionnaires:SOC (Sense of Coherence),17 enlarged HI (the Health Index)18 andthe Borg CR10 scale.19 All data were recorded in accordance withthe Patient Record Act.20 After the last TM treatment the patients’results were printed out and un-blinded (see Fig. 1).
The Health Index (HI) developed by Hansagi and Rosenqvist18
includes ten questions concerning feelings of well being; itmeasures individual’s subjectively experienced state of health. Thefirst ten questions focus upon energy, mood, fatigue, loneliness,sleep, vertigo, bowel function, pain and mobility and workability.The eleventh question addresses patients’ perception of theirhealth in the last week. For each statement participants rate theirhealth status on a four-grade Lickert scale graded from 1 to 4 (1being poor; 4 being very good). Scores are summarized to createa Health Index ranging from 11 to 44. The higher the score, thebetter the self-rated health. This questionnaire has been internallyand externally validated, clinically tested in Sweden and docu-mented in a number of studies.21–27
Questions regarding general health were shown as a strongpredictor to early death and often seen in quality of life question-naires. Therefore three questions were added to the questionnairein order to obtain a more specific appraisal of participants’ generalhealth. These included ‘‘How do you assess your general state ofhealth? How do you assess your physical state of health? and Howdo you assess your mental state of health?’’
The Borg CR10 scale measures intensity of perceptions andfeelings. In reference to this study, patients were asked to estimatetheir perceived pain. The scale ranges from 0 to 10 (0¼ hardlynoticeable to 10¼maximum pain). The scale continues thereafterto a point called ‘‘absolute maximum’’, which is an individual painlimit for each patient to estimate. The scale is useful in clinicaldiagnoses of pain, and commonly used within medicine, ergo-nomics and sports.19
The Sense of Coherence (SOC) questionnaire addresses patients’ability to handle and adjust to the life situation.17 SOC measuresthree aspects: meaningfulness, comprehensibility, and manage-ability. Scores are divided into three levels: low, medium and highSOC. A high score indicates a strong SOC. A number of scientificstudies have used the SOC questionnaire in connection withcomplementary methods.28,29
Referrals toTM inPrimaryHealth CareCentre
Patients that fitthe inclusioncriteria areasked toparticipate inthe study(n=57)
The participantsfill in threequestionnairesHI, SOC (n=57) Borg CR10scale (n=51)
Patientsterminate thestudy (n=11)
Fig. 1. Outline of the study design for evaluating the effe
4. Data analysis
The STATA statistical programme was used to analyse data. Allthe results were analysed using both Wilcoxon’s paired test andFisher’s exact test.30 Statistical significance was accepted whenp< 0.01 occurred owing to multiple comparisons.
5. Results
Fifty-seven persons commenced the study with forty-threesubjects completing the study (n¼ 43; 37 women; 6 men). Theaverage age of participants was 48.1 years (range 25–80) (see Fig. 1).It was not possible to identify reasons for people leaving the study.
Patients received TM once a week for approximately 1 h overa ten-week period. The most common reasons for patient referralwere pain (n¼ 43), sleep disorders (n¼ 26), inability to move(n¼ 8), headache (n¼ 7) and tension (n¼ 7).
5.1. Effects of TM
Effects on Health Index (HI) and Sense of Coherence (SOC) areshown in Table 1. Eleven out of fourteen parameters improvedaccording to the enlarged HI questionnaire (p-values between0.0015 and <0.001). These included perceptions of energy, mood,tiredness, sleep, pain, movement, health (last week), general healthand physical health. The median value for the total Health Indexwas 24 (range 14–34) pre-TM and 29 (range 20–37) post-TM.
Participants treatedwith TactileMassage nine to tentimes at 30–75minutes (n=46)
The participantsfill in threequestionnairesHI, SOC (n=43), Borg CR10scale (n= 41)
Tactile Massagetherapists documentthe treatment andeffects in thepatients’ records
The TactileMassage therapistgathers effects inthe records, printsit out and de-identifies it
ct of TM on patients in Primary Health Care Centres.

K. Andersson et al. / Complementary Therapies in Clinical Practice 15 (2009) 158–160160
Seventy two percent of patients reported their general state ofhealth as very/rather poor before TM compared with 37% after TM.Pain estimates according to the Borg CR10 scale was also improved(p< 0.001) suggesting TM reduced perceptions of pain.
SOC scores did not change significantly; however, the number ofsubjects classified into the different groups, i.e. low, medium orhigh Sense of Coherence, did change (p< 0.001). The effects of TMreported upon by patients were documented in the patients’records. These included reduced pain (n¼ 32), improved sleep(n¼ 22), enhanced relaxation (n¼ 13), greater energy (n¼ 12) andfeeling happier (n¼ 11).
6. Discussion
The positive effects of TM were documented in relation to pain,sleep, relaxation, energy and mood. Improvements reported by thepatients are derived from the questionnaires and express increasedenergy, feeling happier, decreased tiredness, improved sleep, lowerpain, increased ability to move their bodies, and improved generaland physical health in the previous week (last week). Interestingly,fewer patients were classified in the low SOC group followingtreatment, even if the median scores did not change significantly.
This study is an observational study. It did not have controlgroup and so it is not appropriate to generalise from these results.However, the results are interesting and it is hoped that they willinspire research employing an RCT design. The findings couldsuggest that TM should be explored more fully in order to evaluatethe extent to which the variables of pain relief, improved sleep,relaxation and so on could improve physical and emotional. Whatalso could be of interest are which symptoms TM did not seem toaffect. These included perceptions of loneliness, vertigo anddigestion.
This study suggests that the main effect of TM seems to berelaxation and pain relief. In a small pilot study (9), the authors alsonoted an effect on metabolic control in subjects with type 2 dia-betes where cortisone levels decreased, possibly due to relaxation.9
The lower effect on the general emotional well being could be thatTM may bring up a range of different feelings resulting from a morerelaxed state, however this would need to be explored more fully. Infurther studies it is also of interest to explore if any causal relation-ships or correlations exist between relaxation and pain relief.
Acknowledgements
We thank the tactile massage therapists, Carin Asker, Ann-MarieBlomberg, Karin Bråneryd, Anne Hedbom, Christina Larsson,Inga-Lill Wrede Holm, Agneta Waller, and all the patients whoparticipated in the study.
References
1. Ardeby S. When words are not enough: on hands, skin and nervous system froma tactile perspective, and the background of the original tactile massage method(Nar orden inte racker: om hander, hud, nervsystem ur ett taktilt perspektivsamt bakgrunden till originalmetoden taktil massage)in Swedish. Stockholm:Ambosantus; 2003. p. 66.
2. Forsberg C, Krusebrant Å, Bjorvell H. Tactile massage (Taktil massage; inSwedish). Stockholm: National Swedish Board of Health and Welfare; 1996.
3. Braverman DL, Schulman RA. Massage techniques in rehabilitation medicine.Phys Med Rehabil Clin N Am 1999;10:631–49. ix.
4. Field T. Massage therapy effects. Am Psychol 1998;53:1270–81.5. Field T. Massage therapy. Med Clin North Am 2002;86:163–71.6. Agren A, Berg M. Tactile massage and severe nausea and vomiting during
pregnancy – women’s experiences. Scand J Caring Sci 2006;20:169–76.7. Alexandersson M, Dehlen C, Johansson I, Petersson I, Langius A. Therapeutic
massage as a complementary treatment in palliative care. Nordic J Nurs Res ClinStud 2003;23:27–30.
8. Andersson K, Wandell P, Tornkvist L. Working with tactile massage – a groun-ded theory about the energy controlling system. Complement Ther Clin Pract2007;13:258–65.
9. Andersson K, Wandell P, Tornkvist L. Tactile massage improves glycaemiccontrol in women with type 2 diabetes: a pilot study. Pract Diabetes Int2004;21:105–9.
10. Bergsten U, Petersson IF, Arvidsson B. Perception of tactile massage asa complement to other forms of pain relief in rheumatic disease. Musculo-skeletal Care 2005;3:157–67.
11. Edvardsson JD, Sandman PO, Rasmussen BH. Meanings of giving touch in thecare of older patients: becoming a valuable person and professional. J Clin Nurs2003;12:601–9.
12. Henricson M, Berglund AL, Maatta S, Ekman R, Segesten K. The outcome oftactile touch on oxytocin in intensive care patients: a randomised controlledtrial. J Clin Nurs 2008;17:2624–33.
13. Henricson M, Berglund A-L, Maatta S, Segersten K. A transition from nurse totouch therapist – a study of preparation before giving tactile touch in anintensive care unit. Intensive Crit Care Nurs 2006;22:239–45.
14. Olsson I, Rahm V, Hogberg H. Tactile massage after a stroke and improvedquality of life. Nordic J Nurs Res Clin Stud 2004;24:21–6.
15. Skovdahl K, Sorlie V, Kihlgren M. Tactile stimulation associated with nursingcare to individuals with demantia showing aggressive or restless tendencies: anintervention study in dementia care. Int J Older People Nurs 2007;2(3):162–70.
16. Stockholm County Council, Local Health and Medical Care Committee. Stock-holm inhibitants and complementary medicine (Stockholmare och den komple-mentara medicinen; in Swedish). Stockholm: Halso- och sjukvårdsnamndenStockholms lans landsting; 2001. p. 91.
17. Antonovsky A. The structure and properties of the sense of coherence scale. SocSci Med 1993;36:725–33.
18. Nordstrom G, Nyman CR, Theorell T. Psychosocial adjustment and general stateof health in patients with ileal conduit urinary diversion. Scand J Urol Nephrol1992;26:139–47.
19. Borg G. Borg’s perceived exertion and pain scales. USA: Human Kinetics; 1998.20. Ehrenberg A, Ehnfors M, Thorell-Ekstrand I. The VIPS model – implementation
and validity in different areas of nursing care. Stud Health Technol Inform1997;46:408–10.
21. Klang B, Bjorvell H, Clyne N. Quality of life in predialytic uremic patients. QualLife Res 1996;5:109–16.
22. Forsberg C, Cedermark B. Well-being, general health and coping ability: 1-yearfollow-up of patients treated for colorectal and gastric cancer. Eur J Cancer Care(Engl) 1996;5:209–16.
23. Forsberg C, Bjorvell H. Swedish population norms for the GHRI, HI and STAI-state. Qual Life Res 1993;2:349–56.
24. Forsberg C, Bjorvell H, Cedermark B. Well-being and its relation to copingability in patients with colo-rectal and gastric cancer before and after surgery.Scand J Caring Sci 1996;10:35–44.
25. Eriksson LE, Nordstrom G, Berglund T, Sandstrom E. The health-relatedquality of life in a Swedish sample of HIV-infected persons. J Adv Nurs 2000;32:1213–23.
26. Langius A, Bjorvell H, Lind MG. Oral- and pharyngeal-cancer patients’ perceivedsymptoms and health. Cancer Nurs 1993;16:214–21.
27. Sandstrom V, Bjorvell H, Olofsson P. Functional status and well-being in a groupof patients with abdominal aortic aneurysm. Scand J Caring Sci 1996;10:186–91.
28. Haraldsson K, Fridlund B, Baigi A, Marklund B. The self-reported healthcondition of women after their participation in a stress management pro-gramme: a pilot study. Health Soc Care Community 2005;13:224–30.
29. Majumdar M, Grossman P, Dietz-Waschkowski B, Kersig S, Walach H. Doesmindfulness meditation contribute to health? Outcome evaluation of a Germansample. J Altern Complement Med 2002;8:719–30 [discussion: 731–715].
30. Corporation S. Stata statistical software: release 7.0. 7.0 ed. Texas: StataCorporation; 2001.