Embed Size (px)
DESCRIPTION
Tabuk University. Hematology – 1, MLT 205 Hereditary Spherocytosis. Faculty of Applied Medical Sciences Department Of Medical Lab. Technology 2 nd Year – Level 4 – AY 1433-1434. Mr. Waggas Ela’as, M.Sc, MLT. Objectives. - PowerPoint PPT Presentation
Citation preview

Faculty of Applied Medical Sciences
Department Of Medical Lab. TechnologyDepartment Of Medical Lab. Technology2nd Year – Level 4 – AY 1433-1434
1
Mr. Waggas Ela’as, M.Sc, MLTMr. Waggas Ela’as, M.Sc, MLT

To know spherocytes and the difference between them and normal Biconcave red cells.
To review red cell membrane constituents.
To know H.S as one of the Hemolytic anemias.
To know the lab. Diagnosis of H.S and the principle of Osmotic fragility Test.
2

Defect in genes for the skeletal proteins of the red cells membrane . (spectrin, ankyrin and band 3 ).
Parts of the lipid bilayer not supported by skeleton are removed resulting in surface to volume ratio – causes the cells to become spheroidal.
Less deformable than normal RBCs. Destruction in micro circulations of the
spleen
3

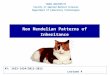
The red cell membrane
4

Normal red blood cells easily change shape to move effectively through the small blood vessels between organs of the body. In spherocytosis the red blood cells are very roundround and have difficulty changing this shape. The lack of ability to change shapes makes moving through the small blood vessels difficult. Therefore, the red blood cells stay in the spleen longer than normal. This lengthy stay in the spleen damages the cell membranes.
5

Bone marrow produce normal biconcave discs but they lose membrane in R.E.S = Reticulo Endothelial System (mainly Spleen).
Then they become spherical Ultimately, Spherocytes are destroyed in
the spleen. EXTRAVASCULAR HEMOLYSIS
Spectrin deficiency is the most common defect.
6

7

8

Fluctuating Jaundice . Anemia Mild to moderate splenomegaly Aplastic crises Gall stones
9

Laboratory Findings:
-minimal anemia-reticulocytosis (5 – 20%).
-increased mean corpuscular hemoglobin concentration (MCHC),
-spherocytes on the peripheral blood smear.
-DAT : Direct Antihuman Globulin Test is negative
-hyperbilirubinemia-The osmotic fragility test is increased .
-Autohaemolysis is increased and is corrected by Glucose .
10

Anisocytosis = cells vary in size Spherocytes.(less in diameter, greater
thickness, no central pallor). Polychromatic cells.
11

12

13
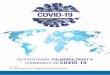
Polychromatic red cells are larger than mature erythrocytes and still contain ribosomes and mitochondria, giving the cell a blue tint. When polychromatic RBCs are stained with a supravital dye (new methylene blue or cresyl violet) ribosomes clump to form a blue stained granulars called reticulum. These are called reticulocytes.

Supravital stain of blood from a patient with hemolytic anemia. The reticulocytes are the cells with the dark blue dots and curved linear structures (reticulum) in the cytoplasm
14

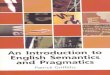
Scanning electron micrograph of a normal biconcave erythrocyte
Scanning electron micrograph of a spherocyte. It is smaller, round, and lacks concavities
15

Non specific test. The osmotic fragility test is a measure of the
resistance of erythrocytes to hemolysis by osmotic stress. The test consists of exposing red cells to decreasing strengths of hypotonic saline solutions and measuring the degree of hemolysis colorimetrically at room temperature. (15 ° - 20 ° C).
The osmotic fragility testThe osmotic fragility test
16

Fresh blood (g/l NaCl)Blood incubated 24 hours, 37°C (g/l NaCl)
Initial lysis5.07.0
Complete lysis3.02.0
MCF* (50% lysis)4.0 – 4.454.65 – 5.9
*MCF : Mean Cell Fragility
The osmotic fragility of freshly taken red cells reflects their ability to take up a certain amount of water before lysing. This is determined by their volume-to-surface area ratio. The ability of the normal red cell to withstand hypotonicity results from its biconcave shape, which allows the cell to increase its volume by about 70% before the surface membrane is stretched; once this limit is reached lysis occurs. Spherocytes have an increased volume-to-surface area ratio; their ability to take in water before stretching the surface membrane is thus more limited than normal and they are therefore particularly susceptible to osmotic lysis.Hypotonic solutions Cells will swell
Hpertonic solutions Cells will shrink
Isotonic solutions Cells will remain
17

Is increased and is corrected by Glucose .
when sterile defibrinated blood is incubated at 37°C, normal red blood cells hemolyze slowly; cells with membrane or metabolic defects do so to a greater
extent.
Normal Lysis at 48 hours :
without added glucose, 0.2-2.0%with added glucose, 0-0.9%.
In membrane disorders such as HS, the rate of glucose consumption is increased to compensate for an increased cation leak through the membrane
18

Also called Coomb’s Test. Red cells coated with antibodies do not
agglutinate directly when centrifuged. These cells are said to be sensitized .
In order for agglutination to occur, AHG is added. (Anti Human Globulin).
This will form a "bridge" between the antibodies coating red cells, causing agglutination.
19

20

Differential diagnosis Other causes of spherocytes in peripheral blood film:
1.Autoimmune hemolytic anaemias. (DAT +ve) 2.Hemolytic transfusion reactions.
3.Thermal injury 4.Clostridial septicaemia ,
5.Severe hypophosphataemia 6.ABO incompatibility (neonates)
21