Embed Size (px)
Citation preview

©2013 Children's Mercy. All Rights Reserved. 09/13
Karen Rubio MT (ASCP)
Lead Technologist
Children’s Mercy Hospital Blood Bank
HAABB 2014
T activation Thomsen-Friedenreich Antigen
©2013 Children's Mercy. All Rights Reserved. 09/13 2
T activiation
• British Journal of Haematology, 2001, 112, 259-263
• In vitro polyagglutination first described by
Hubener in 1925 then Thomsen in 1927
• Thomsen’s graduate student Friedenreich
in 1930 defined the underlying mechanism
and called it T haemagglutination after
Thomsen

©2013 Children's Mercy. All Rights Reserved. 09/13 3
T activation
• Acquired and transient condition
– Polyagglutination is a result of a variety of
neuraminidase producing bacterial, viral, or
protozoa infections
– Removal of N-acetyl neuraminic acid residues
on portions of glycophorin A and B chains of
the MN, Ss, and other RBC disialylated
tatrasaccharides to expose T cryptantigen
©2013 Children's Mercy. All Rights Reserved. 09/13 4
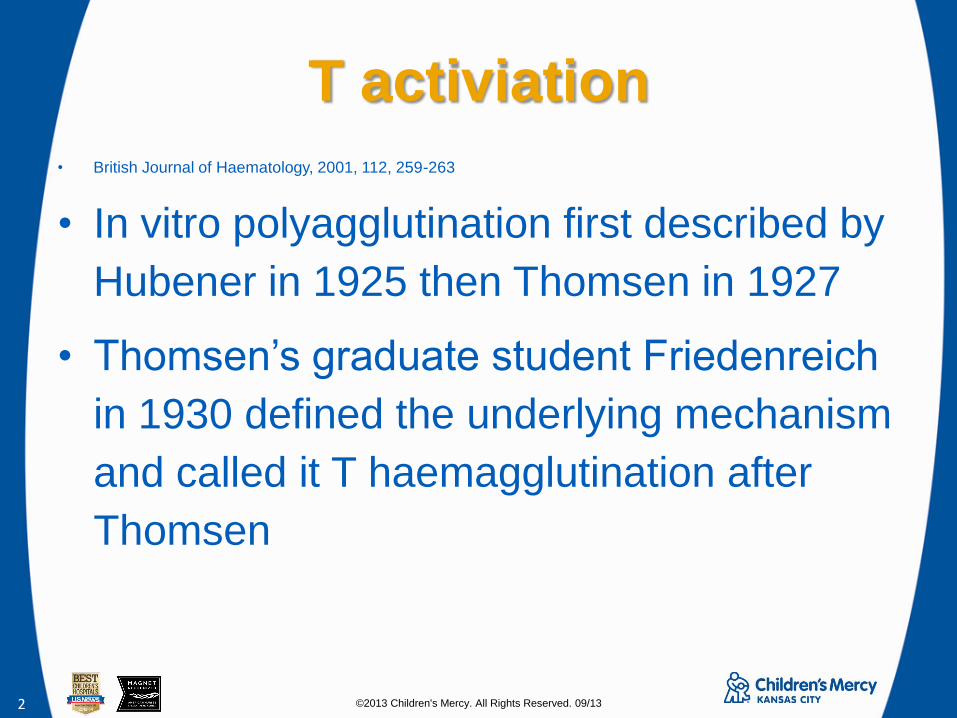
T activation
RBC surface molecules
* All numbers Fiscal 2012
Image by proprofs.com Google images

©2013 Children's Mercy. All Rights Reserved. 09/13 5
T activation
RBC Surface molecules
Dean L. Blood Groups and Red Cell Antigens [Internet]
2005
©2013 Children's Mercy. All Rights Reserved. 09/13 6
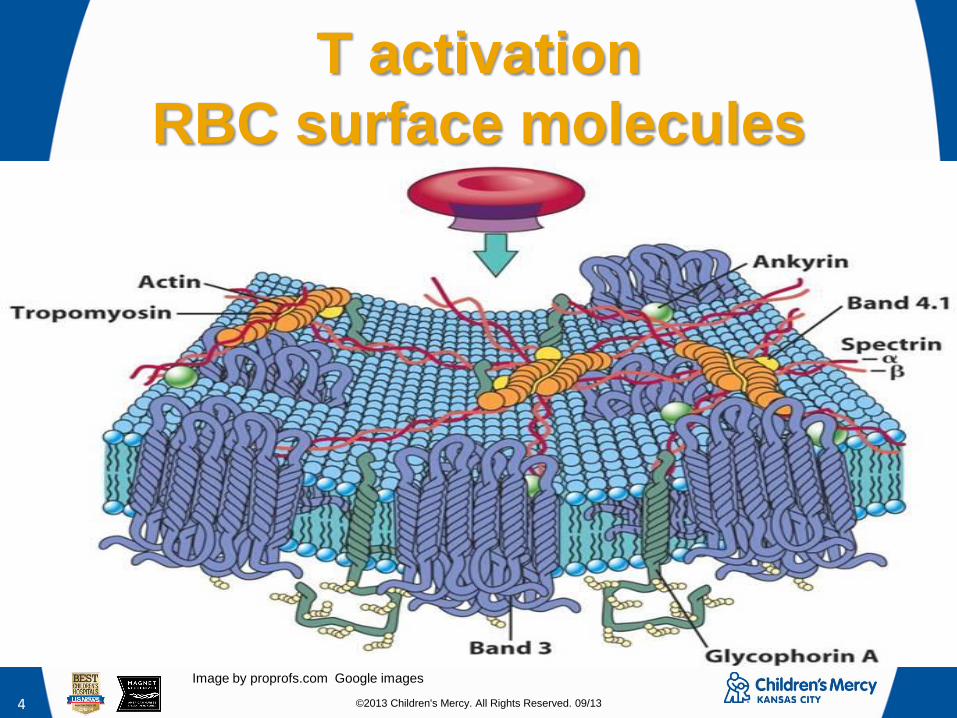
T activation
Testing Method AABB Technical Manual Method 2-16
• Principle: Saline extracts of
seeds react with specific
carbohydrates on red cells
membranes and make useful
typing reagents that are highly
specific at appropriate
dilutions.
• Reagents: Seeds may be
obtained from health-food
stores, pharmacies, or
commercial seed companies.
The seeds should be raw
Procedure: Grind seeds in a food
processor or blender until the particles
look like coarse sand. A mortar and
pestle may be used or seeds can be
used whole.
2. In a large test tube or small beaker,
place ground seeds and 3 to 4 times
their volume of saline.
3. Incubate at room temperature or 4 to
12 hours stirring occasionally.
4. Transfer supernatant fluid to a
centrifuge tube , centrifuge 5 minutes to
obtain a clear supernatant. Collect and
filter the supernatant fluid, and discard
seed residue
5. Test dilutions of extract to find the
dilution for the desired activity.

©2013 Children's Mercy. All Rights Reserved. 09/13 7
T activation Reactions between Lectins and
Polyaggluntinable Red Cells AABB Technical manual
T Th Tk Tn Cad
Arachis
hypogaea
+ + + 0 0
Dolichos
biflorus
0 0 0 + +
Glycine
max
+ 0 0 + +
Salvia
sclarea
0 0 0 + 0
Salvia
horminum
0 0 0 + +
©2013 Children's Mercy. All Rights Reserved. 09/13 8
T activation
CBC’s IRL TAT • Per Shay, Jack, & Mary in IRL at CBC
• The initial screen takes 2 – 3 hours
– If positive with screen, 5 – 8 hours or longer for
identification
• They use mostly homemade reagents at IRL that
may have been made and frozen ahead of time
for different cases. Not may commercial lectin
panels on the market
• Use donor tested Plasmas and Cord plasmas
and frozen control cells

©2013 Children's Mercy. All Rights Reserved. 09/13 9
• Test for T activation on pretransfusion
specimens especially in neonates
• If Positive: Wash all cellular products (RBC
and Platelets)
• Avoid if possible any plasma containing
products
– Vit K infusion or low titer anti-T FFP
Specification SPN204/1.1 Diagnosis and Management of T Antigen
Activation. Author: Dr Edwin Massey
• Some papers recommended exchange
transfusion with washed cells and albumin
2001 Blackwell Science Ltd, British Journal of Haematology 112; 259-263
T activation
Transfusion Guidelines

©2013 Children's Mercy. All Rights Reserved. 09/13 10
T activation
2 case studies • Patient: T, W
• 4 years old
• Transferred from an outside
ED
• Acute Respiratory failure
• Left side pleural effusion
• Left side pneumonia
• Patient: E, G
• 8 month old
• Transfer from a smaller area
hospital
• Pneumococcal meningitis and
bacteremia
• Altered mental status with
possible seizures
• Leukopenia
• Bilateral fluid collections with
Rt. Frontal area subdural bleed

©2013 Children's Mercy. All Rights Reserved. 09/13 11
T activation
Diagnosis T,W • Type and Screen ordered
• Our results were
discrepant. Suspect Cold
reactive antibody. T
activation also ordered at
the same time as T/S
• Specimen sent to IRL at
Community Blood Center

©2013 Children's Mercy. All Rights Reserved. 09/13 12
T activation
Patient: T, W lab data OCT/30/13
• Testing performed by IRL at the Community Blood Center:
• Investigate ABO Typing Problem:
• The patient's red cells were spontaneously agglutinated by saline. This agglutination was
circumvented by washing the patient's cells with 37C saline. With the warm washed cells,
the patient was found to be group O, Rh positive.
• The patient's warm washed cells are coated with complement. An IgG-specific antiglobulin
reagent was nonreactive. An eluate was not prepared from this sample. The patient's
plasma was found to contain a cold reactive autoantibody; no alloantibodies were detected.
Cold autoantibodies are not usually clinically significant.
• The patient's warm washed cells were reactive with the plasma from 12 random group O
donors and nonreactive with plasma from 4 group O cord blood samples. Her cells were
also reactive with the following lectins: Arachis hypogea and Baneirea II. The results of
these tests indicate the patient's cells are polyagglutinable. The pattern of the reactivity is
consistent with Tk polyagglutination. If transfusion is required, washed red cell products
should be provided; plasma containing components should be avoided.

©2013 Children's Mercy. All Rights Reserved. 09/13 13
T activation
Patient: T, W lab data

©2013 Children's Mercy. All Rights Reserved. 09/13 14
T activation
Patient: T, W lab data
©2013 Children's Mercy. All Rights Reserved. 09/13 15
T activation
Patient: E, G lab data APR/30/13
Antibody Identification by the IRL department at Community Blood Center:
• The patient’s cells were reactive with the plasma from six group O donors.
His cells were also reactive with the following lectins: Arachis hypogaea,
Glycine soja, Salvia Sclarea and Saliva horminum. The results of these tests
indicate the patient’s cells are polyagglutinable. The pattern of reactivity is not
consistent with a single type of polyagglutination this may indicate that the
patient has mixed forms of polyagglutination or an uncharacterized form of
polyagglutination. If transfusion is required, washed products should be
provided; plasma containing components should be avoided.

©2013 Children's Mercy. All Rights Reserved. 09/13 16
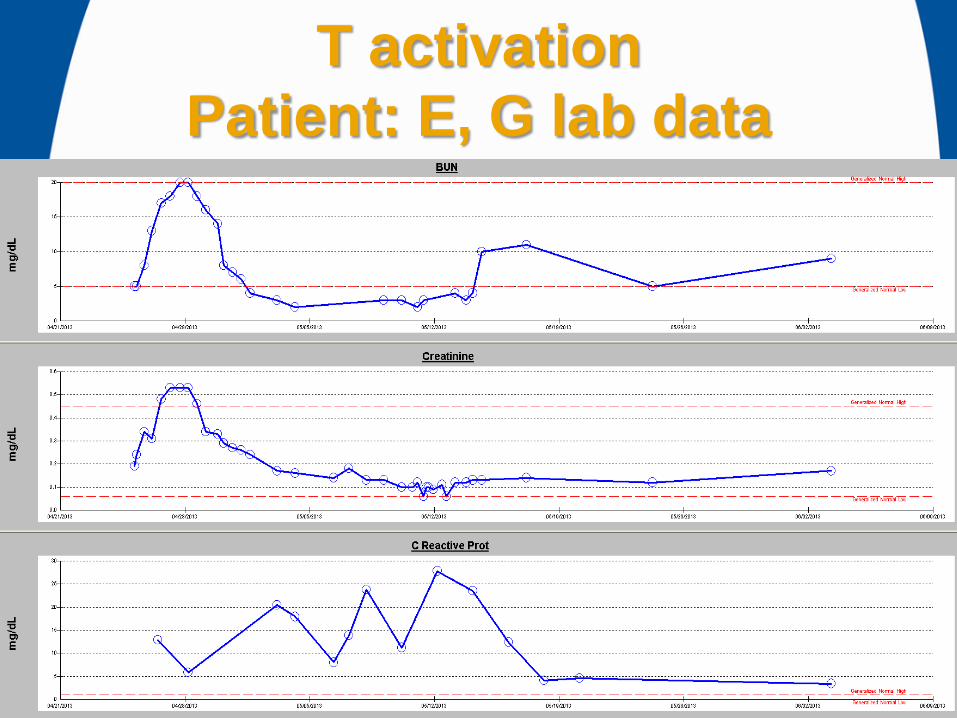
T activation
Patient: E, G Hgb lab data
0
2
4
6
8
10
12
4/2
5/2
013
4/2
6/2
013
4/2
7/2
013
4/2
8/2
013
4/2
9/2
013
4/3
0/2
013
5/1
/2013
5/2
/2013
5/3
/2013
5/4
/2013
5/5
/2013
5/6
/2013
5/7
/2013
5/8
/2013
5/9
/2013
5/1
0/2
013
5/1
1/2
013
5/1
2/2
013
5/1
3/2
013
5/1
4/2
013
5/1
5/2
013
5/1
6/2
013
5/1
7/2
013
5/1
8/2
013
5/1
9/2
013
5/2
0/2
013
5/2
1/2
013
5/2
2/2
013
5/2
3/2
013
5/2
4/2
013
5/2
5/2
013
5/2
6/2
013
5/2
7/2
013
5/2
8/2
013
5/2
9/2
013
5/3
0/2
013
5/3
1/2
013
6/1
/2013
6/2
/2013
6/3
/2013
7.6 7.5
6.1
10.9
10.1
9.3
8.6
7.6 7.1 7.1
5.9
10.1
9.1 9.3
8.3 8.6
8.3
6.8
11.4 11.1
10.5 10.3
9.4 9.1
7.9
6.8
9
10 10
10.7
9.2 9.6
9.3
10.5
Hgb 10.5-13.5 gm/dL

©2013 Children's Mercy. All Rights Reserved. 09/13 17
T activation
Patient: E, G lab data
©2013 Children's Mercy. All Rights Reserved. 09/13 18
T activation
Patient: E, G lab data

©2013 Children's Mercy. All Rights Reserved. 09/13 19
T activation
In Summary • Polyagglutination caused by the removal of portions of
glycophorin A and B by neuraminidase producing
pathogens to expose a cryptic antigen “T” on RBCs,
platelets, glomeruli and other tissues
• More common in children than adults
• Self limiting but can cause hemolytic events in rare
cases
• Wash all cellular products and avoid plasma
containing products like FFP.