Embed Size (px)
Citation preview

SYSTEMS BASED PRACTICE
Part IDr. James Rohack

General CompetenciesGeneral Competencies
• Medical knowledgeMedical knowledge
• Patient CarePatient Care
• Practice-based learningPractice-based learning
• Interpersonal skills and communicationInterpersonal skills and communication
• ProfessionalismProfessionalism
• Systems-based practiceSystems-based practice

The medical profession has long The medical profession has long subscribed to a body of ethical subscribed to a body of ethical
statements developed primarily for the statements developed primarily for the benefit of the patient. A physician benefit of the patient. A physician
must recognize responsibility not only must recognize responsibility not only to patients, but also to society, to to patients, but also to society, to
other health professionals and to self.other health professionals and to self.
The Competent PhysicianThe Competent Physician
• Possesses medical knowledge, Possesses medical knowledge, judgment, professionalism, clinical judgment, professionalism, clinical and communication skills to provide and communication skills to provide high quality patient carehigh quality patient care

• Evidence of professional standingEvidence of professional standing
• Evidence of commitment to life-long Evidence of commitment to life-long learning and involvement in periodic learning and involvement in periodic self-assessmentself-assessment
• Evidence of cognitive expertiseEvidence of cognitive expertise
• Evidence of evaluation of performance Evidence of evaluation of performance in practicein practice

You don't know what you You don't know what you know until you knowknow until you know

Systems-Based PracticeSystems-Based Practice
• Awareness of and responsiveness Awareness of and responsiveness to the larger context of the system to the larger context of the system of healthcareof healthcare
• Ability to call on system resources to Ability to call on system resources to provide care that is of optimal valueprovide care that is of optimal value


Traditional Fee-For-ServiceTraditional Fee-For-Service
Total CostTotal Cost
FixedFixed
RevenueRevenue
Net IncomeNet Income
VolumeVolumenn11
VariableVariable
$$
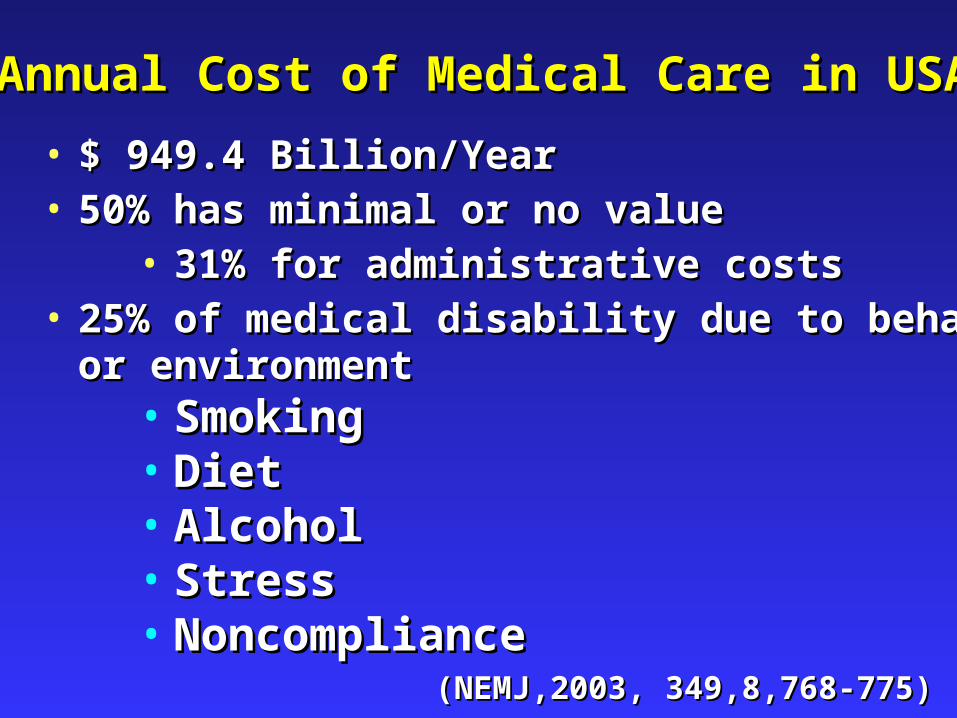
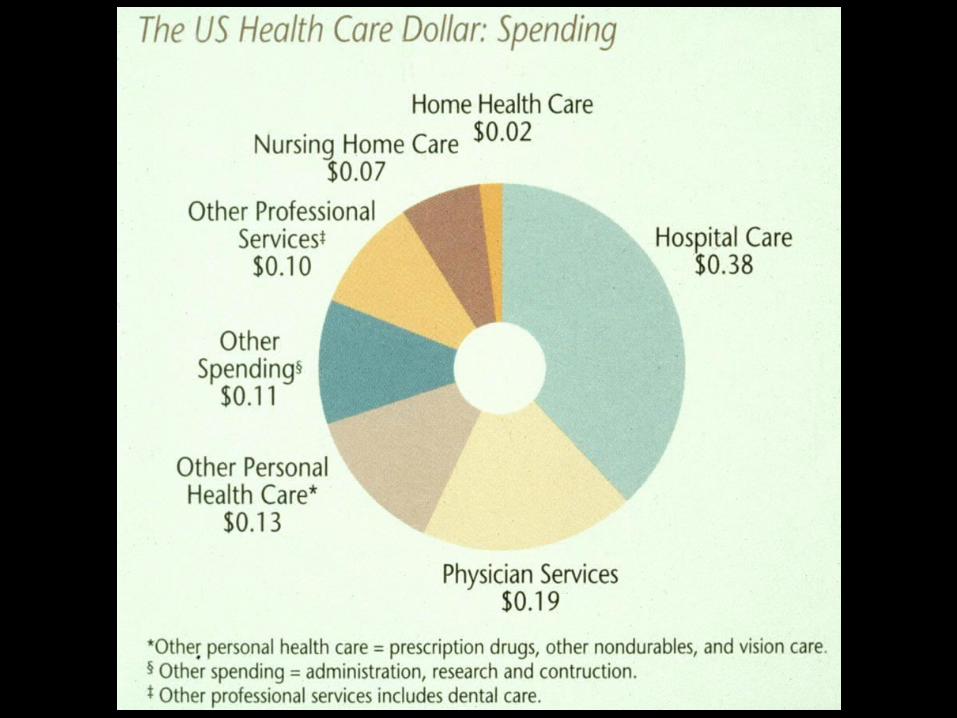
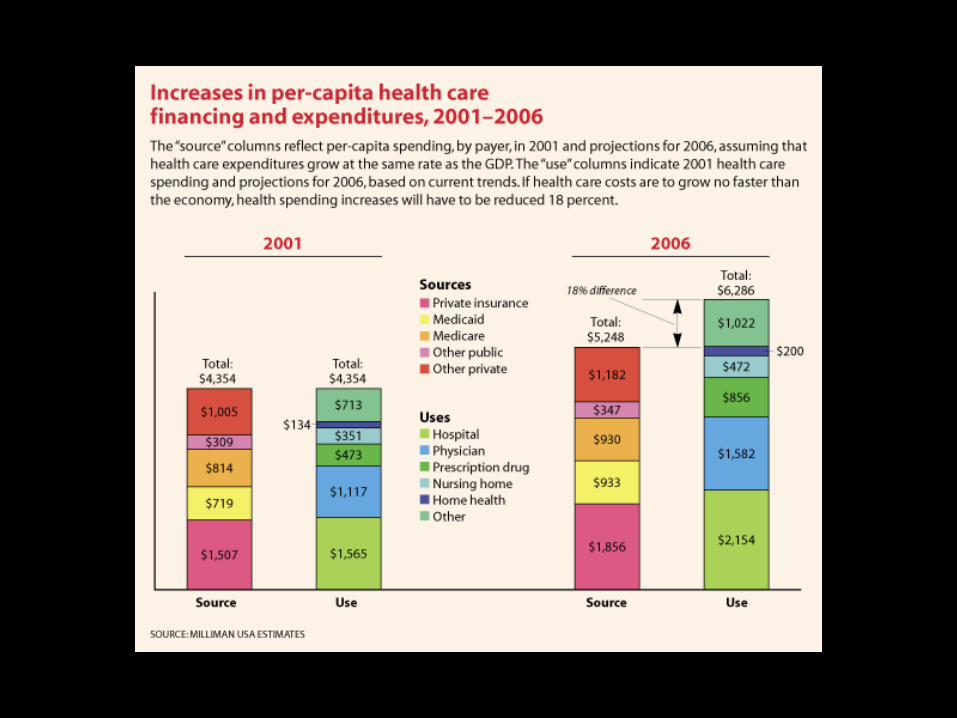
Annual Cost of Medical Care in USAAnnual Cost of Medical Care in USA
(NEMJ,2003, 349,8,768-775)(NEMJ,2003, 349,8,768-775)
• $ 949.4 Billion/Year$ 949.4 Billion/Year• 50% has minimal or no value50% has minimal or no value
• 31% for administrative costs31% for administrative costs• 25% of medical disability due to behavior 25% of medical disability due to behavior
or environmentor environment• SmokingSmoking• DietDiet• AlcoholAlcohol• StressStress• NoncomplianceNoncompliance



HealthCareHealthCare
Privilege versus RightPrivilege versus Right
Insurance versus CoverageInsurance versus Coverage

• MANAGED CARE is the process of the MANAGED CARE is the process of the
application of standard business practices application of standard business practices
to the delivery of health care in the to the delivery of health care in the
traditions of the American free enterprise traditions of the American free enterprise
system.system.

Funding StreamsFunding Streams
• IndividualIndividual
• EmployerEmployer
• GovernmentGovernment

Medical ProfessionMedical Profession
GovernmentGovernment CapitalistsCapitalistsEmployers/Wall Street/Employers/Wall Street/
InsuranceInsurance
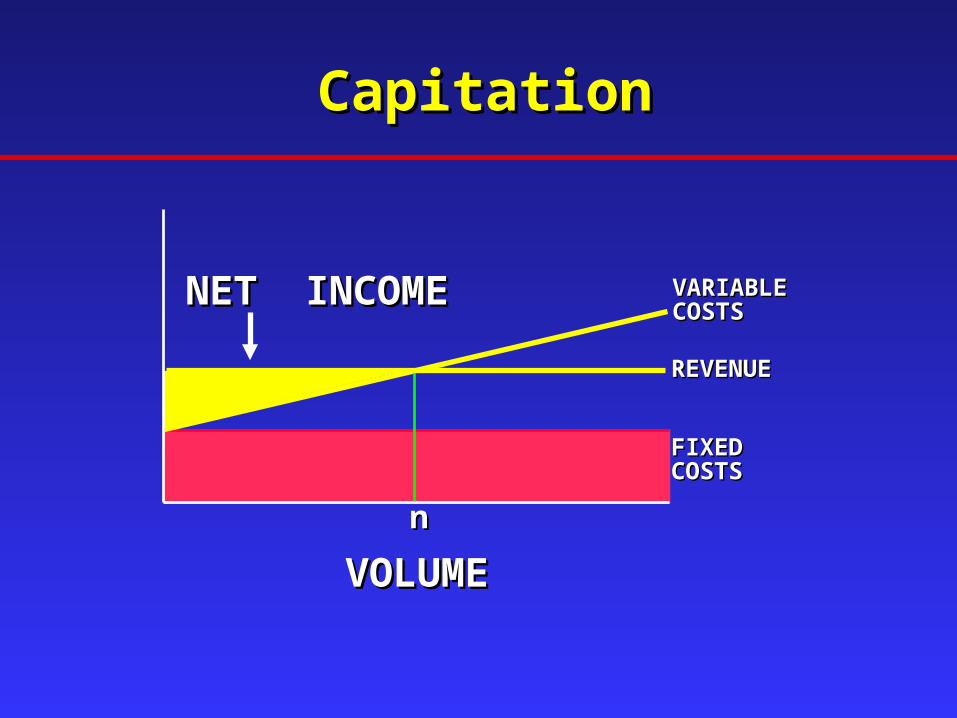
CapitationCapitation
REVENUEREVENUE
VARIABLEVARIABLECOSTSCOSTS
FIXEDFIXEDCOSTSCOSTS
nn
NET INCOMENET INCOME
VOLUMEVOLUME

PMPMPMPM
• Per Patient Per MonthPer Patient Per Month• Used to calculate required capitation Used to calculate required capitation
rates, based upon utilization and cost rates, based upon utilization and cost per unit for specified items. per unit for specified items.


Treat sicknessTreat sickness
Fee-for-serviceFee-for-service
Solo practiceSolo practice
Indemnity insuranceIndemnity insurance
Super specialistsSuper specialists
Traditional FocusTraditional Focus Managed Care FocusManaged Care Focus
Maintain wellnessMaintain wellness
CapitationCapitation
Group practiceGroup practice
Managed careManaged care
Primary carePrimary care
Paradigm ShiftsParadigm Shifts
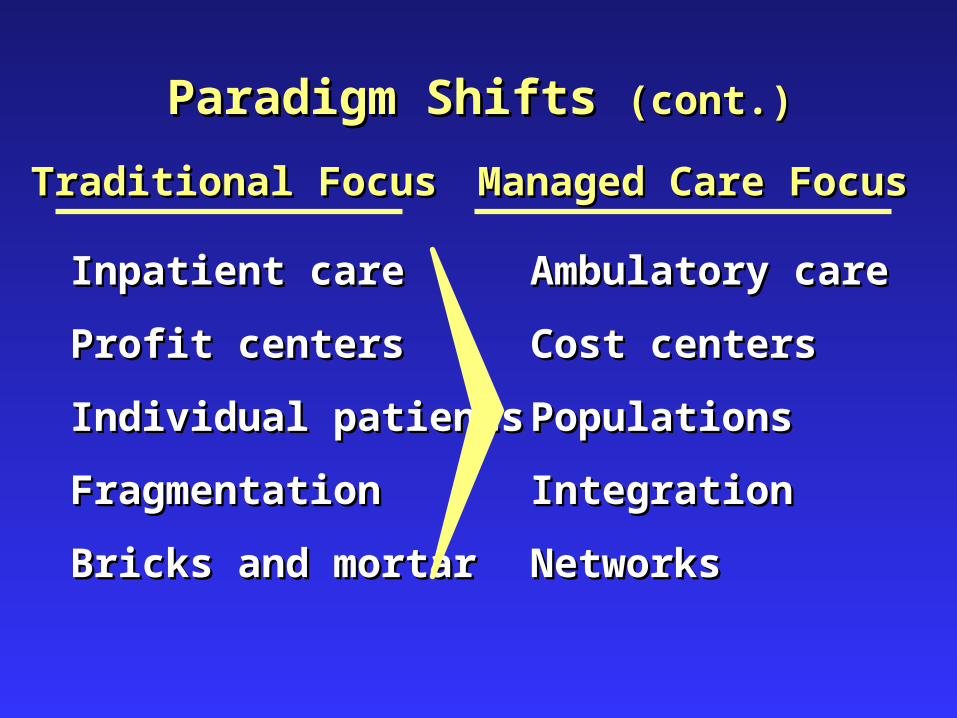
Inpatient careInpatient care
Profit centersProfit centers
Individual patientsIndividual patients
FragmentationFragmentation
Bricks and mortarBricks and mortar
Ambulatory careAmbulatory care
Cost centersCost centers
PopulationsPopulations
IntegrationIntegration
NetworksNetworks
Traditional FocusTraditional Focus Managed Care FocusManaged Care Focus
Paradigm Shifts Paradigm Shifts (cont.)(cont.)

IPAsIPAs((Independent Practice AssociationIndependent Practice Association))
• Set up to accept risk, manage and Set up to accept risk, manage and distribute share of premiumdistribute share of premium
• Either "professional risk only", or "global Either "professional risk only", or "global risk"risk"
• Global risk IPAs often partnered with Global risk IPAs often partnered with hospitalshospitals
Humana/PCA Health Plans 1997Humana/PCA Health Plans 1997

PPO PPO (Preferred Provider Organization )(Preferred Provider Organization )
• Network of MDs and Hospitals who agree to Network of MDs and Hospitals who agree to "discount" in return for prompt payment and "discount" in return for prompt payment and steeragesteerage
• Individuals choose to use or not useIndividuals choose to use or not use• Individuals choose to use or not use the Individuals choose to use or not use the
network at each incident of carenetwork at each incident of care• Financial incentives to use the networkFinancial incentives to use the network
• Lower deductiblesLower deductibles• Lower co-insuranceLower co-insurance
Humana/PCA Health Plans 1997Humana/PCA Health Plans 1997


CapitationCapitation
REVENUE
VARIABLECOSTS
FIXEDCOSTS
n
NET INCOME
VOLUME


-80%
-60%
-40%
-20%
0%
Sigmoidoscopy
DiagnosticUpper GI
Endoscopy
Colonoscopywith Lesion
RemovalDiagnostic
Caths Angioplasty
-12%
-37%
-70%-77%
-62%
Utilization Rates among California Utilization Rates among California Cardiologists and Gastroenterologists Cardiologists and Gastroenterologists
Following CapitationFollowing Capitation
(The Health Care Advisory Board Company, 1995)(The Health Care Advisory Board Company, 1995)





Managed Care Managed Care
Reduces CostsReduces Costs



LegislatureLegislature
• Unfunded mandatesUnfunded mandates
• Impact of premium increasesImpact of premium increases
• Rise of uninsuredRise of uninsured

Examples of Examples of Legislative MandatesLegislative Mandates
• Newborn hearing screeningNewborn hearing screening• Mastectomy reconstructionMastectomy reconstruction• Prostate cancer screeningProstate cancer screening• Maternity length of stayMaternity length of stay• Serious medical illness coverageSerious medical illness coverage• TMJ coverageTMJ coverage• Craniofacial abnormality treatment coverageCraniofacial abnormality treatment coverage

Market Forces: The Economic DriversMarket Forces: The Economic DriversEmployers seek less Employers seek less expensive health careexpensive health care
Result: Providers lose control of medical enterpriseResult: Providers lose control of medical enterprise
Predators discover Predators discover profits in medicineprofits in medicine
Non-Profits Non-Profits become alarmedbecome alarmed
Providers affiliate to Providers affiliate to increase bargaining increase bargaining power and protect power and protect
patientspatients
Collaborations/Mergers/Collaborations/Mergers/Acquisitions escalate to Acquisitions escalate to
enhance power and enhance power and efficiencyefficiency
Develop purchasing Develop purchasing consortiaconsortia
Reimbursement Reimbursement decreasesdecreases

Factors Driving Up CostsFactors Driving Up Costs
• Growth in pharmaceutical expensesGrowth in pharmaceutical expenses• Expensive new technologies, Expensive new technologies, • Aging of the population, and Aging of the population, and • Increased consumer demandIncreased consumer demand
Utilization ManagementUtilization Management
• PrescriptivePrescriptive
• CapitationCapitation
• Integrated Healthcare SystemIntegrated Healthcare System

• Preauthorization for:Preauthorization for:
• ReferralsReferrals
• Expensive TestsExpensive Tests
• Hospital AdmissionsHospital Admissions
• Length of stay guidelines (concurrent review)Length of stay guidelines (concurrent review)
• Definition of benefitsDefinition of benefits
Utilization ManagementUtilization Management
PrescriptivePrescriptive
Utilization ReviewUtilization Review
• Formal assessment of the medical Formal assessment of the medical
necessity, efficiency, and/or necessity, efficiency, and/or
appropriateness of health care services appropriateness of health care services
and treatment plans on a prospective, and treatment plans on a prospective,
concurrent or retrospective basis.concurrent or retrospective basis.
Medically NecessaryMedically Necessary
Health care services that areHealth care services that are
1) essential to preserve the health of the member1) essential to preserve the health of the member
2) consistent with the symptoms or diagnosis and 2) consistent with the symptoms or diagnosis and treatment of the member’s condition, disease, treatment of the member’s condition, disease, ailment or injuryailment or injury
3) appropriate with regard to standards of good medical 3) appropriate with regard to standards of good medical practice in the communitypractice in the community
4) not solely for the convenience of the member, 4) not solely for the convenience of the member, physician or providerphysician or provider
5) the most appropriate supply or level of service which 5) the most appropriate supply or level of service which can be safely provided to the membercan be safely provided to the member

Prior AuthorizationPrior Authorization
• Process of obtaining prior approval to the Process of obtaining prior approval to the
appropriateness of a service or medication. appropriateness of a service or medication.
Prior authorization does not guarantee Prior authorization does not guarantee
coverage.coverage.

Case ManagementCase Management
• Process whereby covered persons with Process whereby covered persons with
specific health care needs are identified specific health care needs are identified
and a plan designed to efficiently utilize and a plan designed to efficiently utilize
health care resources is formulated and health care resources is formulated and
implemented to achieve the optimum implemented to achieve the optimum
patient outcome in the most cost-effective patient outcome in the most cost-effective
manner.manner.
Financial ConsiderationsFinancial ConsiderationsStrategies to Control CostsStrategies to Control Costs
• Shift to ambulatory careShift to ambulatory care
• Streamline all careStreamline all care
• Limit unnecessary careLimit unnecessary care• One third of primary care visits are One third of primary care visits are
unnecessaryunnecessary• Half of the surgeries performed are Half of the surgeries performed are
inappropriateinappropriate

Financial Considerations Financial Considerations Strategies to Control CostsStrategies to Control Costs
• Use Urgent careUse Urgent care
• Use of the emergency facilities for non-urgent Use of the emergency facilities for non-urgent
care is estimated to comprise 40% of all care is estimated to comprise 40% of all
visits,and such visits are 2 to 3 times more visits,and such visits are 2 to 3 times more
costly than a primary care office visitcostly than a primary care office visit
• Manage chronic diseaseManage chronic diseaseOver half of chronic illness is preventable.Over half of chronic illness is preventable.
AHRQ User Liason Program 2001AHRQ User Liason Program 2001

Payment MechanismsPayment Mechanisms
For HospitalsFor Hospitals
• Per DiemPer Diem
• DRGDRG
• CapitationCapitation

Payment MechanismsPayment Mechanisms
For PhysiciansFor Physicians
• Discounted fee for serviceDiscounted fee for service
• Discounted fee scheduleDiscounted fee schedule
• CapitationCapitation

Value-Based Value-Based SelectionSelection
Marketplace “Drivers”Marketplace “Drivers”
Purchaser DemandsPurchaser Demands
TraditionalTraditional TransitionalTransitional MatureMature
Discounted Discounted FFSFFS
Capitation & Capitation & Case RatesCase Rates
60%60%
40%40%
20%20%
0%0%

QualityQuality
CostCostValue =Value =
Ways Others Are Reducing Ways Others Are Reducing Resource UtilizationResource Utilization
• Develop practice guidelines to reduce Develop practice guidelines to reduce
variationvariation
• Shift care to alternate, less costly Shift care to alternate, less costly
providersproviders
• Reduce numbers of proceduresReduce numbers of procedures
• Limit hospital costsLimit hospital costs

Managing the Cost of Primary Care…Managing the Cost of Primary Care…
Health Care Shifting LeftHealth Care Shifting Left
Cost of Routing Care Episode (e.g., cold, flu)Cost of Routing Care Episode (e.g., cold, flu)
$1$1 $5$5
$40$40$50$50
Patient Patient Self-CareSelf-Care
Telephone Telephone Triage NurseTriage Nurse
PhysicianPhysicianExtendersExtenders
Primary Care Primary Care PhysicianPhysician
(The Health Care Advisory Board Company, 1995)(The Health Care Advisory Board Company, 1995)

Cost to HMOCost to HMOER versus ClinicER versus Clinic
•An average visit to an emergency room costs $383 –without physician fees. (2001 www.appleton.org)
•The average physician's office visit costs $60. (American Medical Association, "Physician Socioeconomic Statistics," 2001.)



High Cost Encourages High Cost Encourages Adverse SelectionAdverse Selection
Cost/QualityCost/Quality Enrollment Enrollment
LowLow Healthy, Younger, Healthy, Younger, Less ConcernedLess Concerned
HighHigh Older, Sicker, Older, Sicker, More ConcernedMore Concerned

Uninsured 14.3% PopulationUninsured 14.3% Population
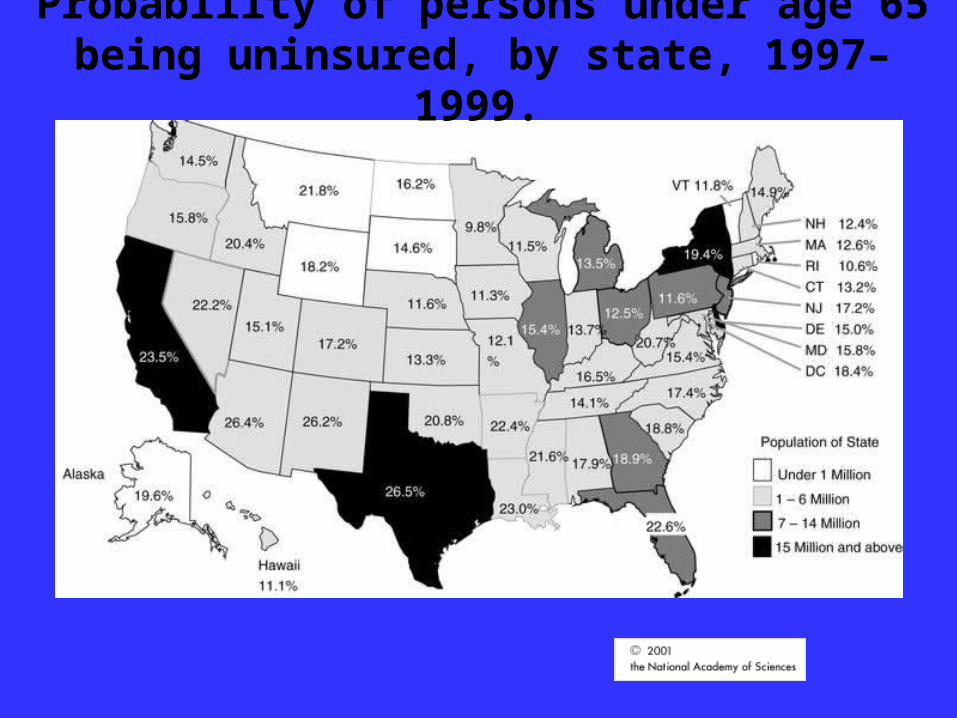
Probability of persons under age 65 being uninsured, by state, 1997–1999.

Texas Leads Nation in Texas Leads Nation in Uninsured ChildrenUninsured ChildrenCenter Public Policy Priorities, 2002Center Public Policy Priorities, 2002

Hispanics in TexasHispanics in Texas
According to the 2000 Census, Hispanics now comprise 32 percent (6.7 million), while white non-Hispanics constitute 53 percent. The rate of growth for Hispanics in the 10-year period was 55 percent. Although most Hispanics are of Mexican descent, the numbers and percentage that are Puerto Rican, Cuban, and Central American are increasing throughout Texas.

Health coverage for TexansHealth coverage for Texans


Who Pays – You DoWho Pays – You Do
Consumers Want:Consumers Want:
• ChoiceChoice
• ControlControl
• Customer serviceCustomer service
• BrandsBrands
• InformationInformation

Future Funding ProblemsFuture Funding Problems
• Spreading riskSpreading risk
• Individual responsibilityIndividual responsibility
• GenomicsGenomics
• How to say NOHow to say NO

Future DirectionsFuture Directions
Reduce CostsReduce Costs
EnhanceEnhanceServiceService
ImproveImproveQualityQuality

CompassionCompassion(advocacy)(advocacy)
BalanceBalance(tension)(tension)
EfficiencyEfficiency(stewardship)(stewardship)
ExcellenceExcellence(quality)(quality)
Part I
The End
Post Test IPost Test IPlease print page, take exam, send hard copy to Please print page, take exam, send hard copy to
Dr. Sandra Oliver OMEDr. Sandra Oliver OME
1. 1. When a physician orders a test that is When a physician orders a test that is unnecessary to make a diagnosis or unnecessary to make a diagnosis or treatment plan, all the following occur treatment plan, all the following occur EXCEPT:EXCEPT:
A.A. increases the premium for health insurance the increases the premium for health insurance the following yearfollowing year
B.B. may result in more tests ordered based on may result in more tests ordered based on resultsresults
C.C. increases financial reimbursement under increases financial reimbursement under capitationcapitation
D.D. may decrease liability riskmay decrease liability risk

Question 2Question 2
2. Which funding source for medical 2. Which funding source for medical care is most impacted by political care is most impacted by political influence?influence?
A.A. individual fee for serviceindividual fee for service
B.B. private Insurance private Insurance
C.C. employer self insuredemployer self insured
D.D. governmentgovernment

Question 3Question 3
3. Which of the following does not 3. Which of the following does not reduce resource utilization? reduce resource utilization?
AA. Develop practice guidelines to reduce variation. Develop practice guidelines to reduce variation
BB. Shift care to alternate, less costly providers. Shift care to alternate, less costly providers
C.C. Increase numbers of procedures Increase numbers of procedures
D.D. Limit hospital costs Limit hospital costs
Question 4Question 4
4. Which method of controlling 4. Which method of controlling medical costs is being abandoned medical costs is being abandoned by some insurance by some insurance companies?companies?
A.A. co-paysco-pays
B.B. gatekeeper for specialty referralsgatekeeper for specialty referrals
C.C. chronic disease managementchronic disease management
D.D. practice guidelinespractice guidelines

Question 5Question 5
5. Which of the following medical 5. Which of the following medical delivery systems is at greatest risk delivery systems is at greatest risk for ethical for ethical problems of performing problems of performing unnecessary tests?unnecessary tests?
A.A. health maintenance organizationshealth maintenance organizationsB.B. fee for servicefee for serviceC.C. medicaid medicaid D.D. primary care case managementprimary care case management

Question 6Question 6
6. Which of the following medical delivery 6. Which of the following medical delivery systems would have the least likelihood systems would have the least likelihood of a of a common electronic medical record?common electronic medical record?
A.A. Independent Practice Association (IPA)Independent Practice Association (IPA)
B.B. Preferred Provider Organization (PPO)Preferred Provider Organization (PPO)
C.C. Physician-Hospital Organization (PHO)Physician-Hospital Organization (PHO)
D.D. Integrated Medical Delivery System (IMS)Integrated Medical Delivery System (IMS)

Question 7Question 7
7. Which mechanism is most likely to 7. Which mechanism is most likely to influence your physician practice?influence your physician practice?
A.A. discussion of a new treatment by a discussion of a new treatment by a colleaguecolleague
B.B. practice guideline described by a practice guideline described by a national physician organizationnational physician organization
C.C. practice guideline placed on a electronic practice guideline placed on a electronic physician order entry systemphysician order entry system
D.D. elimination of reimbursement for a test elimination of reimbursement for a test by a payorby a payor

Question 8Question 8
8.8. Which of the following is false Which of the following is false about Texas ?about Texas ?
A.A. Highest number uninsured childrenHighest number uninsured childrenB.B. Highest percentage of elderlyHighest percentage of elderlyC.C. Physicians subsidize 26% of Physicians subsidize 26% of
uninsured health careuninsured health careD.D. Lower insured rate than nationLower insured rate than nation

SYSTEMS BASED PRACTICE
PART II
Dr. James Rohack

Systems-Based PracticeSystems-Based Practice as manifested as manifested by actions that demonstrate an by actions that demonstrate an
awareness of and responsiveness to the awareness of and responsiveness to the larger context and system of health care larger context and system of health care
and the ability to effectively call on and the ability to effectively call on system resources to provide care that is system resources to provide care that is
of optimal value.of optimal value.

CapitalistCapitalistEmployers/Wall Street/ Employers/Wall Street/
InsuranceInsurance
Medical ProfessionMedical Profession
GovernmentGovernment



ProfessionalismProfessionalism
• Subordinate self-interest to the interests Subordinate self-interest to the interests of othersof others
• Adhere to high moral and ethical Adhere to high moral and ethical standardsstandards
• Respond to societal needs, reflect a Respond to societal needs, reflect a social contractsocial contract
• Commitment to scholarship and Commitment to scholarship and advance-ment of one’s fieldadvance-ment of one’s field

QualityQuality
Scientific Scientific ApproachApproach
All One All One TeamTeam

QualityQuality
CostCostValue =Value =

There's another wayThere's another way
to measure quality.to measure quality.
It's health care qualityIt's health care quality
from thefrom the
patient's point of view.patient's point of view.

QualityQuality
HEDIS HEDIS JCAHOJCAHO
TQM TQM Report CardsReport Cards
NCQA NCQA FACCTFACCT

ProfessionProfession
StateState CapitalistsCapitalists

HEDIS DataHEDIS Data
Quality of CareQuality of Care
• Childhood immunization rateChildhood immunization rate
• Cholesterol screening rate (age 40-64)Cholesterol screening rate (age 40-64)
• Cervical cancer screening rate (age 21-64)Cervical cancer screening rate (age 21-64)
• Percent patients receiving prenatal visit, Percent patients receiving prenatal visit, first trimesterfirst trimester
• Percent infants below birth ratePercent infants below birth rate

Acute Acute Care Care
Costs Costs SoaringSoaring

Reduction in process Reduction in process variation and multi system variation and multi system interactions reduces Risk interactions reduces Risk
for failurefor failure

Physicians Control Two-Thirds Physicians Control Two-Thirds of Inpatient Costsof Inpatient Costs
(Health Care Advisory Board, 1995)(Health Care Advisory Board, 1995)
Controlled Controlled by Hospitalsby Hospitals
Controlled by Controlled by PhysiciansPhysicians
30-35%65-70%

"80% of future cost savings will come "80% of future cost savings will come from modified physician conduct - not from modified physician conduct - not
hospital efficiency, etc."hospital efficiency, etc."
(Advisory Board, Washington, D.C., 1993)(Advisory Board, Washington, D.C., 1993)

Resource UtilizationResource Utilization
• Waste occursWaste occurs
• Eliminate unnecessary and Eliminate unnecessary and
duplicative servicesduplicative services

Primary Care PhysiciansPrimary Care Physicians
“Population” Managers“Population” Managers

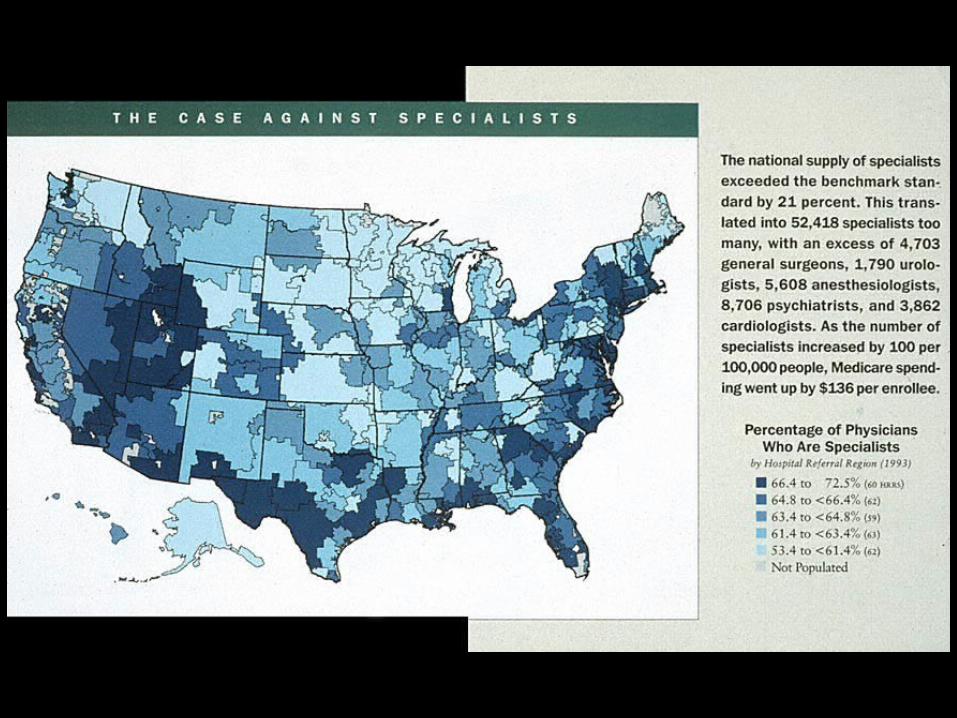
SpecialistsSpecialists
“Event” Managers“Event” Managers
0 1000
Slater
Frisman
Riley
Chu
Philips
Cohen
Carter
Brown
Rosenberg
Albertman
Klein
Fargoe
Bixby
Wells
Snyder
Pierce
Schmidt
Harrington
O'Reilly
Donahue
Adamson
Levitt
Lincoln
Starkman
Reaves
Smith
Dalton
Jones
943
859
643
635
555
552
550
497
449
435
434
432
417
415
391
372
369
350
346
345
329
323
322
319
314
305
297
280
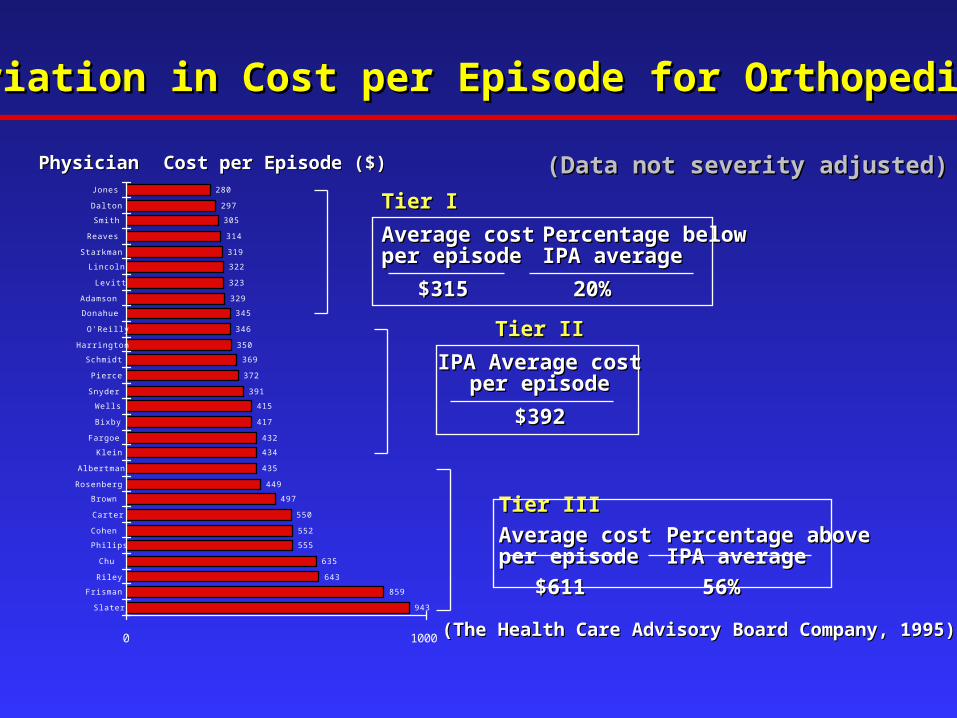
Variation in Cost per Episode for OrthopedicsVariation in Cost per Episode for Orthopedics
Tier IIITier III
Average costAverage cost Percentage abovePercentage aboveper episodeper episode IPA averageIPA average
$611$611 56%56%
Tier ITier I
Average costAverage cost Percentage belowPercentage belowper episodeper episode IPA averageIPA average
$315$315 20%20%
Tier IITier II
IPA Average costIPA Average costper episodeper episode
$392$392
PhysicianPhysician Cost per Episode ($)Cost per Episode ($)
(The Health Care Advisory Board Company, 1995)(The Health Care Advisory Board Company, 1995)
(Data not severity adjusted)(Data not severity adjusted)

Inpatient Costs Controlled Inpatient Costs Controlled by Physiciansby Physicians
• Admissions/Location Within HospitalAdmissions/Location Within Hospital• Length of Hospital StayLength of Hospital Stay• Utilization of Supplies and ServicesUtilization of Supplies and Services
• Lab/RadiologyLab/Radiology• PharmacyPharmacy• ConsultsConsults

You cannot improve what You cannot improve what you do not measureyou do not measure

Patient Safety

Principles for Patient Principles for Patient Safety ReportingSafety Reporting
1. Create an Environment for Safety1. Create an Environment for Safety
2. Data Analysis2. Data Analysis
3. Confidentiality3. Confidentiality
4. Information Sharing4. Information Sharing
Culture -Culture - the set of shared attitudes, the set of shared attitudes, values, goals and practices values, goals and practices that characterizes a that characterizes a company or corporationcompany or corporation

Culture of SafetyCulture of Safety
• Highly reliable organizationHighly reliable organization
• Key componentsKey components
• Non punitive reportingNon punitive reporting

Error -Error - the failure of a planned action the failure of a planned action to be completed as intended, to be completed as intended, or the use of a wrong plan to or the use of a wrong plan to achieve an aimachieve an aim
No one admits an error if No one admits an error if you punish them for ityou punish them for it

Big Errors ResultBig Errors Resultfromfrom
Little ErrorsLittle Errors

Root Causes of ErrorsRoot Causes of Errors
• Insufficient information available to Insufficient information available to
those who need itthose who need it
• Insufficient or inadequate Insufficient or inadequate
communicationcommunication
• Insufficient or inadequate monitoringInsufficient or inadequate monitoring

Humans are the adaptable Humans are the adaptable element of complex systemselement of complex systems

Normal Human Error RatesNormal Human Error Rates
ProbabilityProbability
• Error of commissionError of commission 0.0030.003
• Error of omissionError of omission 0.010.01
• Error in high stress Error in high stress
with rapid activitieswith rapid activities 0.250.25
““Man- a creature made at the Man- a creature made at the end of the week, when God end of the week, when God
was tired.”was tired.”
Mark TwainMark Twain

Safety is made and broken in Safety is made and broken in systems, not individualssystems, not individuals

Culture of Safety does NOT Culture of Safety does NOT Mean:Mean:
• Abandonment of professional accountabilityAbandonment of professional accountability• AnonymityAnonymity• DisregardingDisregarding
• gross incompetencegross incompetence• gross procedural violationsgross procedural violations• gross insubordinationsgross insubordinations• illegal activityillegal activity• practicing under the influencepracticing under the influence

ActAct
PlanPlan
DoDo
CheckCheck

QualityQuality
CostCostValue =Value =

Patient SatisfactionPatient Satisfaction
• Trust is keyTrust is key
• Patient satisfaction at individual Patient satisfaction at individual
physician level now being trackedphysician level now being tracked
High Quality PracticeHigh Quality Practice
• MeasurementMeasurement
• Outcomes cannot be measured Outcomes cannot be measured easily or accuratelyeasily or accurately
• Current strategy is to measure Current strategy is to measure processprocess



Future DirectionsFuture Directions



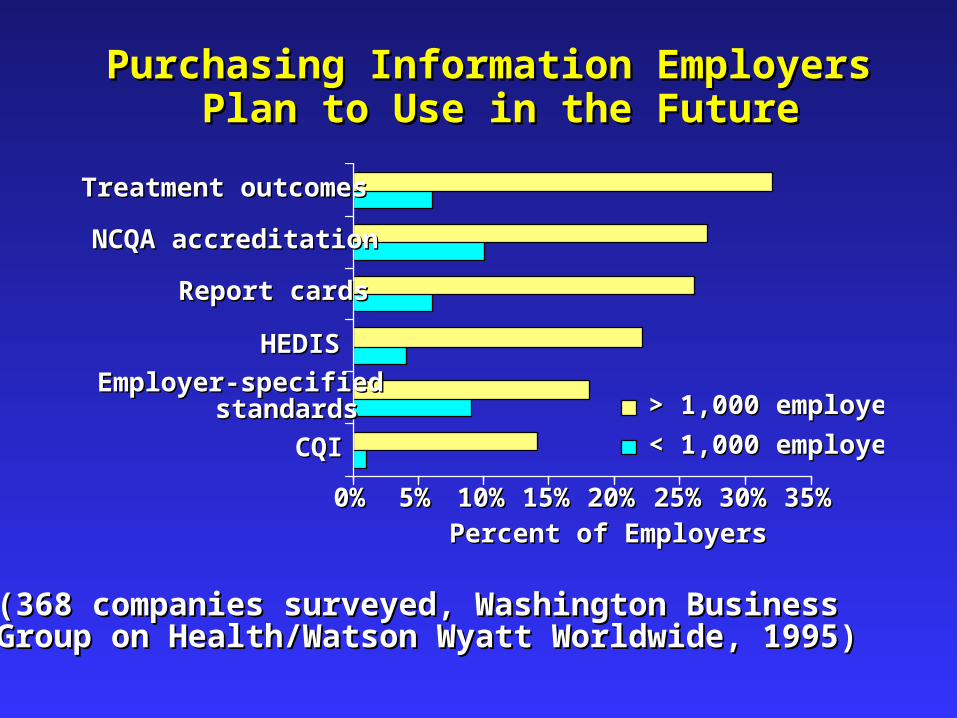
Purchasing Information Employers Purchasing Information Employers Plan to Use in the FuturePlan to Use in the Future
(368 companies surveyed, Washington Business (368 companies surveyed, Washington Business Group on Health/Watson Wyatt Worldwide, 1995)Group on Health/Watson Wyatt Worldwide, 1995)
CQICQI
Employer-specifiedstandards
Employer-specifiedstandards
HEDISHEDIS
Report cardsReport cards
NCQA accreditationNCQA accreditation
Treatment outcomesTreatment outcomes
0%0% 5%5% 10%10% 15%15% 20%20% 25%25% 30%30% 35%35%
Percent of EmployersPercent of Employers
< 1,000 employees< 1,000 employees
> 1,000 employees> 1,000 employees

Vertical Integration of Hospitals and PhysiciansVertical Integration of Hospitals and Physicians
PHYSICIANSPHYSICIANS
INSURERINSURER
HOSPITALHOSPITAL
Capitation Joint Venture OwnershipCapitation Joint Venture Ownership
SoloSolo
Office ShareOffice Share
IPAIPA
CWWCWWGroupGroup Physician-ownedPhysician-owned
Service BureauService Bureau
Open PHOOpen PHO
Closed PHOClosed PHO
MSOMSOFoundationFoundation StaffStaff

Success and Failure Flow Success and Failure Flow from Same Sourcesfrom Same Sources
• Understand technical workUnderstand technical work• Dynamic processDynamic process

• Design tasks and processes that Design tasks and processes that minimize dependency on weak minimize dependency on weak cognitive functionscognitive functions
eg: hurry, fatigue, anger, anxiety, eg: hurry, fatigue, anger, anxiety, boredom, fear, interruptionsboredom, fear, interruptions

Change introduces new Change introduces new forms of failureforms of failure

U.S. Public Opinion - U.S. Public Opinion - Definition of a Good DoctorDefinition of a Good Doctor
• Taken for granted was medical Taken for granted was medical
knowledge and experienceknowledge and experience
• Quality defined as doctors who care, Quality defined as doctors who care,
communicate and take time to listencommunicate and take time to listen

• Treat patients as customersTreat patients as customers
• Recover from mistakes quicklyRecover from mistakes quickly
• Communicate genuine interestCommunicate genuine interest
• Provide recognition and understandingProvide recognition and understanding
• Show compassionShow compassion
Quo Vadis?Quo Vadis?

The Art of Caring for Patients The Art of Caring for Patients
is Caring for Patientsis Caring for Patients


Post Test IIPost Test IIPlease print test pages, take exam, send hard copy to Please print test pages, take exam, send hard copy to
Dr. Sandra Oliver OMEDr. Sandra Oliver OME
1. 1. When you find the medical care your When you find the medical care your
patients receive is not of high quality, patients receive is not of high quality, the following are the following are actions of advocacy actions of advocacy you can take EXCEPT:you can take EXCEPT:
A.A. create a practice guidelinecreate a practice guidelineB.B. lobby for passing a lawlobby for passing a lawC.C. ask your patients for their expectations ask your patients for their expectations DD. refer to a different physician group. refer to a different physician group

Question 2Question 2
2.2. How Is Value defined? How Is Value defined?
A. Quality/ CostA. Quality/ Cost
B. Cost x QualityB. Cost x Quality
C. Quantity/CostC. Quantity/Cost
D. Cost x DesirabilityD. Cost x Desirability

Question 3Question 3
3. When one of your patients requires a medication 3. When one of your patients requires a medication to treat a disease that they cannot afford, all of to treat a disease that they cannot afford, all of the following are reasonable actions you can the following are reasonable actions you can take take EXCEPTEXCEPT::
A.A. write a letter to their insurance company for an write a letter to their insurance company for an individual case review for coverageindividual case review for coverage
B.B. write the pharmaceutical company for help write the pharmaceutical company for help through an indigent programthrough an indigent program
C.C. lobby for the state to mandate as a benefitlobby for the state to mandate as a benefitD.D. encourage the patient to take a family member’s encourage the patient to take a family member’s
unused medicationsunused medications

Question 4Question 4
4. The way to improve patient care is by 4. The way to improve patient care is by improving the safety of the medical delivery improving the safety of the medical delivery system. system. The following are ways that that The following are ways that that can be accomplished EXCEPT:can be accomplished EXCEPT:
A.A. measure process of caremeasure process of care
B.B. measure outcome of caremeasure outcome of care
C.C. increase variation of careincrease variation of care
D.D. decrease variation of caredecrease variation of care

Question 5Question 5
1.1. The most common reason for system The most common reason for system error when dealing with humans is:error when dealing with humans is:
A.A. fatiguefatigue
B.B. complexity of taskcomplexity of task
C.C. number of individuals involvednumber of individuals involved
D.D. number of times a computer is usednumber of times a computer is used

Question 6Question 6
6. One percent of individuals consume 25 6. One percent of individuals consume 25 percent of medical costs. All the following percent of medical costs. All the following are are potential partners to improve care while potential partners to improve care while decreasing costs in the short tem EXCEPT:decreasing costs in the short tem EXCEPT:
A.A. social workerssocial workers
B.B. insurance companiesinsurance companies
C.C. funeral directorsfuneral directors
D.D. governmentgovernment
Question 7Question 7
7. In a medical system that is owned by a 7. In a medical system that is owned by a investor based for-profit system, investor based for-profit system, decreasing medical decreasing medical costs will result in:costs will result in:
A.A. decrease in stock valuedecrease in stock valueB.B. increase in stock valueincrease in stock valueC.C. decrease in quality of care decrease in quality of care D.D. increase in equitable distribution of increase in equitable distribution of
services services

Question 8Question 8
8. Big changes in medical systems can be 8. Big changes in medical systems can be made by which of the followingmade by which of the following
A.A. Small changes in physician processes of Small changes in physician processes of carecare
B.B. Changes in public opinion of medical careChanges in public opinion of medical care
C.C. Changes in legislative reimbursement of Changes in legislative reimbursement of medical caremedical care
D.D. All of the aboveAll of the above





























