Embed Size (px)
Citation preview
9/18/2018
1
Beth A. Steele, OD, FAAO
Disclosures: Member of Optos Advisory Board
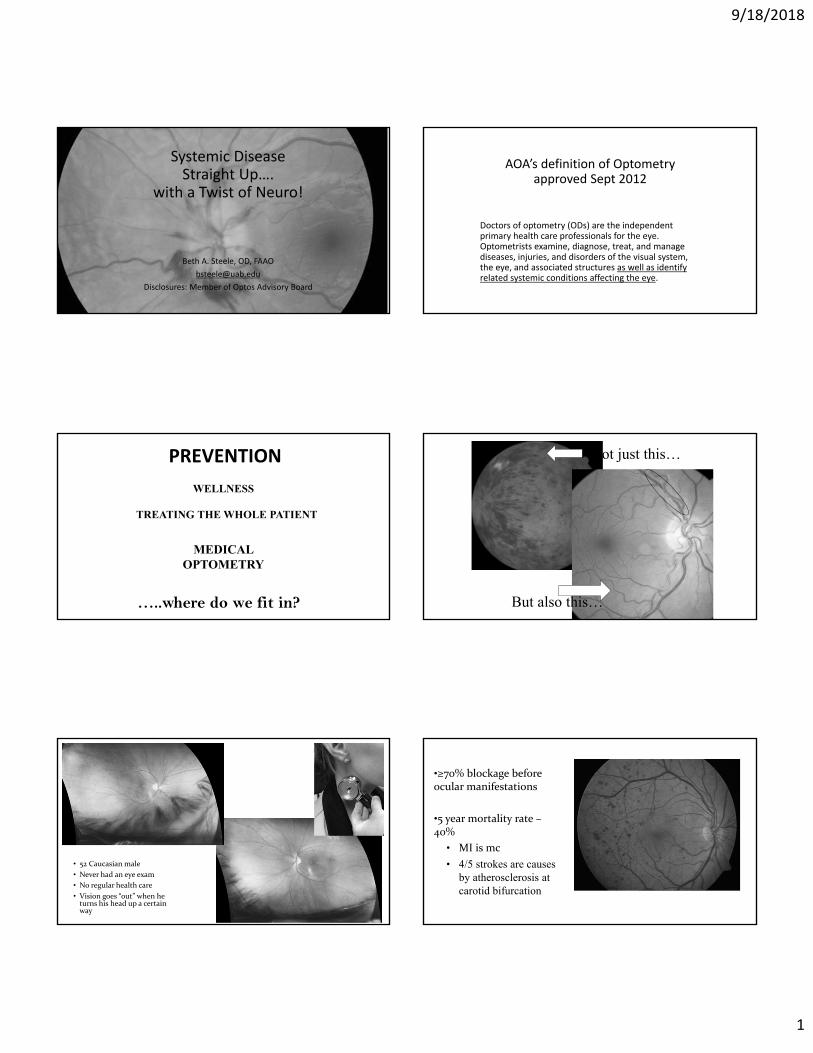
Systemic Disease Straight Up….
with a Twist of Neuro!
AOA’s definition of Optometryapproved Sept 2012
Doctors of optometry (ODs) are the independent primary health care professionals for the eye. Optometrists examine, diagnose, treat, and manage diseases, injuries, and disorders of the visual system, the eye, and associated structures as well as identify related systemic conditions affecting the eye.
PREVENTION
…..where do we fit in?
WELLNESS
TREATING THE WHOLE PATIENT
MEDICAL OPTOMETRY
Not just this…
But also this…
• 52 Caucasian male
• Never had an eye exam
• No regular health care
• Vision goes “out” when he turns his head up a certain way
•≥70% blockage before ocular manifestations
•5 year mortality rate –40%
• MI is mc
• 4/5 strokes are causes by atherosclerosis atcarotid bifurcation
9/18/2018
2
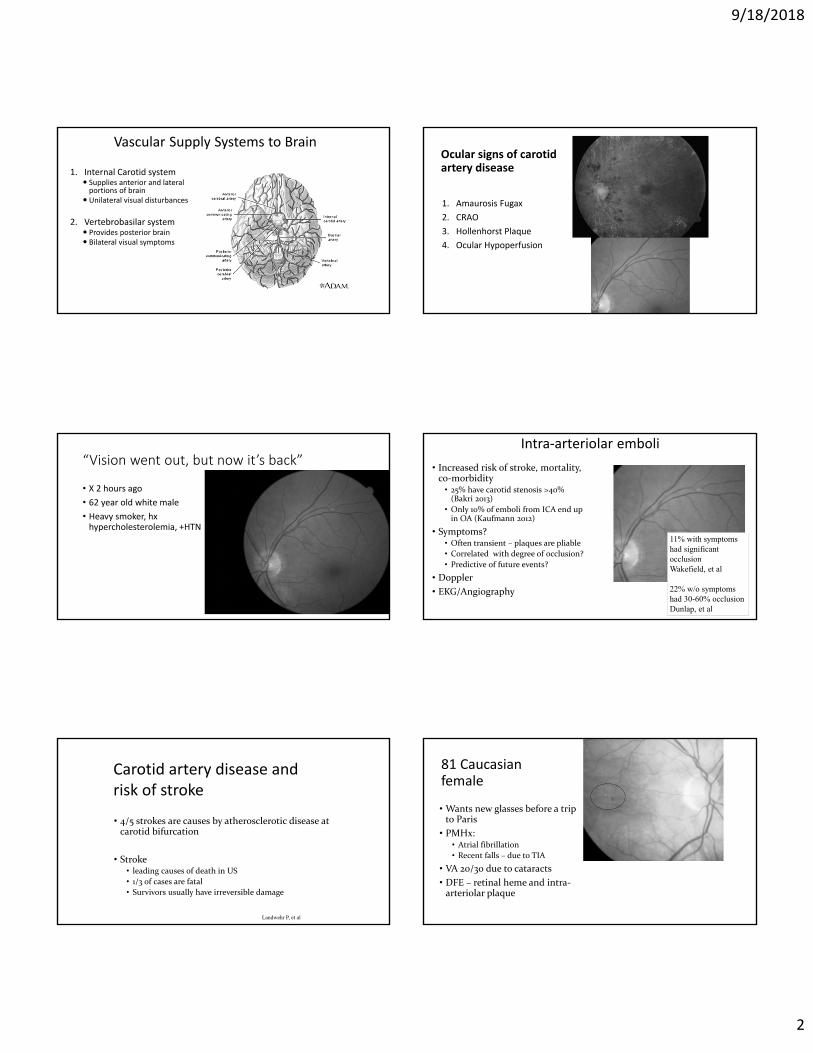
Vascular Supply Systems to Brain
1. Internal Carotid system Supplies anterior and lateral portions of brain
Unilateral visual disturbances
2. Vertebrobasilar system Provides posterior brain Bilateral visual symptoms
Ocular signs of carotid artery disease
1. Amaurosis Fugax
2. CRAO
3. Hollenhorst Plaque
4. Ocular Hypoperfusion
“Vision went out, but now it’s back”
• X 2 hours ago
• 62 year old white male
• Heavy smoker, hxhypercholesterolemia, +HTN
Intra‐arteriolar emboli
• Increased risk of stroke, mortality, co‐morbidity
• 25% have carotid stenosis >40% (Bakri 2013)
• Only 10% of emboli from ICA end up in OA (Kaufmann 2012)
• Symptoms?• Often transient – plaques are pliable
• Correlated with degree of occlusion?
• Predictive of future events?
• Doppler
• EKG/Angiography
11% with symptoms had significant occlusion Wakefield, et al
22% w/o symptoms had 30-60% occlusion Dunlap, et al
• 4/5 strokes are causes by atherosclerotic disease at carotid bifurcation
• Stroke• leading causes of death in US
• 1/3 of cases are fatal
• Survivors usually have irreversible damage
Carotid artery disease and risk of stroke
Landwehr P, et al
81 Caucasian female
• Wants new glasses before a trip to Paris
• PMHx: • Atrial fibrillation
• Recent falls – due to TIA
• VA 20/30 due to cataracts
• DFE – retinal heme and intra‐arteriolar plaque
9/18/2018
3
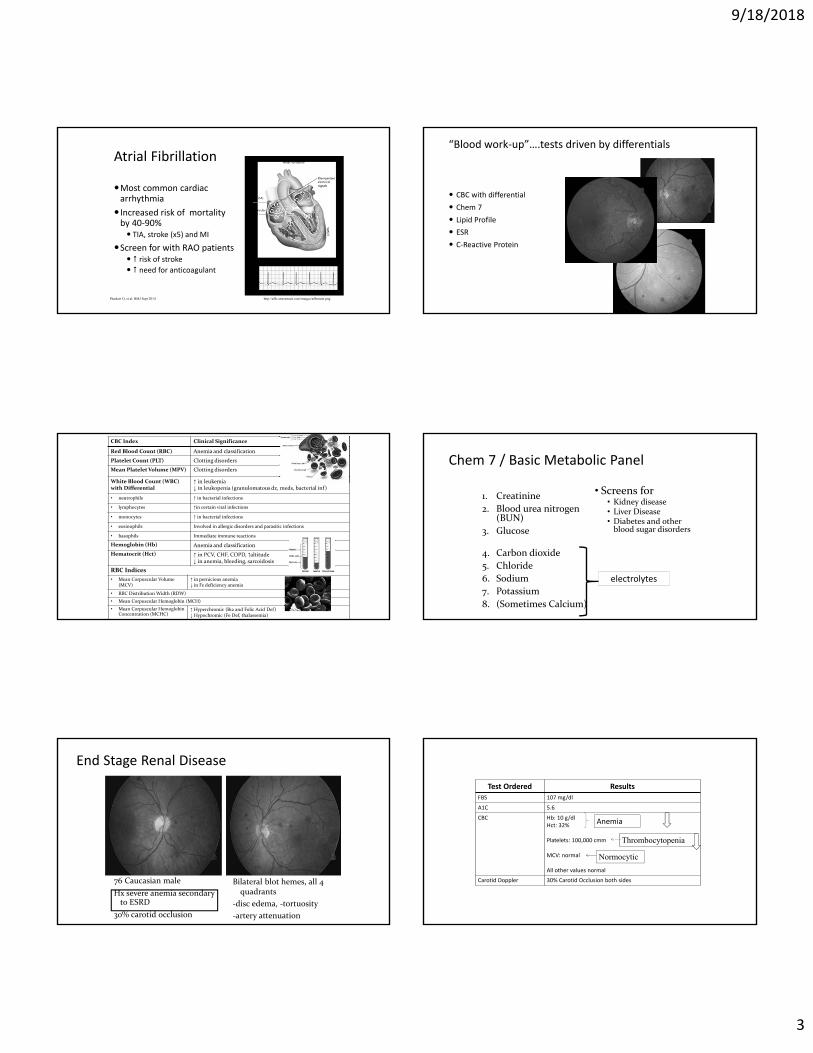
Atrial Fibrillation
Most common cardiac arrhythmia
Increased risk of mortality by 40‐90% TIA, stroke (x5) and MI
Screen for with RAO patients risk of stroke need for anticoagulant
http://afib.utorontoeit.com/images/afibmain.pngPlunkett O, et al. BMJ Sept 2014
“Blood work‐up”….tests driven by differentials
CBC with differential
Chem 7
Lipid Profile
ESR
C‐Reactive Protein
CBC Index Clinical Significance
Red Blood Count (RBC) Anemia and classification
Platelet Count (PLT) Clotting disorders
Mean Platelet Volume (MPV) Clotting disorders
White Blood Count (WBC) with Differential
↑ in leukemia ↓ in leukopenia (granulomatous dz, meds, bacterial inf)
• neutrophils ↑ in bacterial infections
• lymphocytes ↑in certain viral infections
• monocytes ↑ in bacterial infections
• eosinophils Involved in allergic disorders and parasitic infections
• basophils Immediate immune reactions
Hemoglobin (Hb) Anemia and classification
Hematocrit (Hct) ↑ in PCV, CHF, COPD, ↑altitude↓ in anemia, bleeding, sarcoidosis
RBC Indices
• Mean Corpuscular Volume (MCV)
↑ in pernicious anemia ↓ in Fe deficiency anemia
• RBC Distribution Width (RDW)
• Mean Corpuscular Hemoglobin (MCH)
• Mean Corpuscular Hemoglobin Concentration (MCHC)
↑ Hyperchromic (B12 and Folic Acid Def)↓ Hypochromic (Fe Def, thalassemia)
Chem 7 / Basic Metabolic Panel
1. Creatinine
2. Blood urea nitrogen (BUN)
3. Glucose
4. Carbon dioxide
5. Chloride
6. Sodium
7. Potassium
8. (Sometimes Calcium)
• Screens for• Kidney disease • Liver Disease • Diabetes and other blood sugar disorders
electrolytes
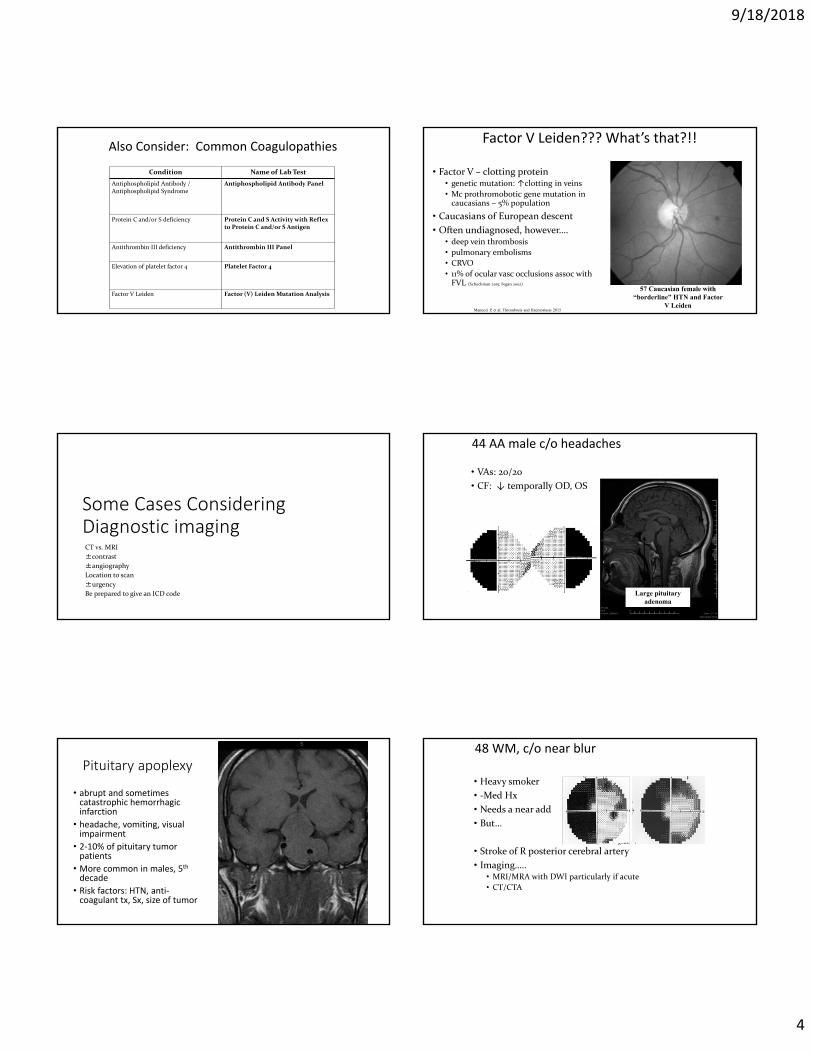
End Stage Renal Disease
76 Caucasian male
Hx severe anemia secondary to ESRD
30% carotid occlusion
Bilateral blot hemes, all 4 quadrants
‐disc edema, ‐tortuosity
‐artery attenuation
Test Ordered Results
FBS 107 mg/dl
A1C 5.6
CBC Hb: 10 g/dlHct: 32%
Platelets: 100,000 cmm
MCV: normal
All other values normal
Carotid Doppler 30% Carotid Occlusion both sides
Anemia
Thrombocytopenia
Normocytic
9/18/2018
4
Also Consider: Common Coagulopathies
Condition Name of Lab Test
Antiphospholipid Antibody / Antiphospholipid Syndrome
Antiphospholipid Antibody Panel
Protein C and/or S deficiency Protein C and S Activity with Reflex to Protein C and/or S Antigen
Antithrombin III deficiency Antithrombin III Panel
Elevation of platelet factor 4 Platelet Factor 4
Factor V Leiden Factor (V) Leiden Mutation Analysis
Factor V Leiden??? What’s that?!!
• Factor V – clotting protein• genetic mutation: ↑clotting in veins
• Mc prothromobotic gene mutation in caucasians – 5% population
• Caucasians of European descent
• Often undiagnosed, however….• deep vein thrombosis
• pulmonary embolisms
• CRVO
• 11% of ocular vasc occlusions assoc with FVL (Schockman 2015; Fegan 2002)
57 Caucasian female with “borderline” HTN and Factor
V LeidenManucci P, et al. Thrombosis and Haemostasis 2015
Some Cases Considering Diagnostic imagingCT vs. MRI
±contrast
±angiography
Location to scan
±urgency
Be prepared to give an ICD code
44 AA male c/o headaches
• VAs: 20/20
• CF: ↓ temporally OD, OS
Large pituitary adenoma
Pituitary apoplexy
• abrupt and sometimes catastrophic hemorrhagic infarction
• headache, vomiting, visual impairment
• 2‐10% of pituitary tumor patients
• More common in males, 5th
decade
• Risk factors: HTN, anti‐coagulant tx, Sx, size of tumor
48 WM, c/o near blur
• Heavy smoker
• ‐Med Hx
• Needs a near add
• But…
• Stroke of R posterior cerebral artery
• Imaging…..• MRI/MRA with DWI particularly if acute
• CT/CTA
9/18/2018
5
57 WM
Patient complaining of Reduced visionWorsening headaches last 2 mos
Hx: Successful triple bypass 2 months prior, 20/20 VA
VA: 20/70 OD, OS
26 27
• Imaging…..• MRI of brain with and without contrast
28
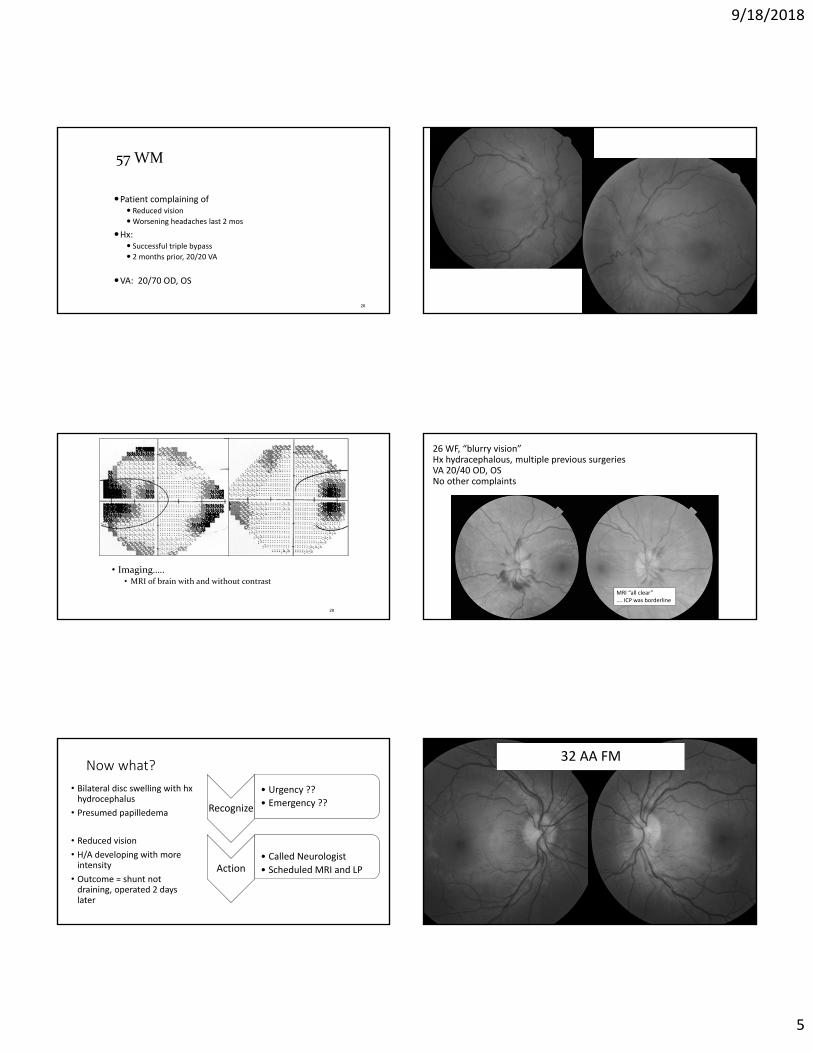
26 WF, “blurry vision”Hx hydracephalous, multiple previous surgeriesVA 20/40 OD, OSNo other complaints
MRI “all clear”…. ICP was borderline
Now what?
• Bilateral disc swelling with hxhydrocephalus
• Presumed papilledema
• Reduced vision
• H/A developing with more intensity
• Outcome = shunt not draining, operated 2 days later
Recognize
• Urgency ??
• Emergency ??
Action • Called Neurologist
• Scheduled MRI and LP
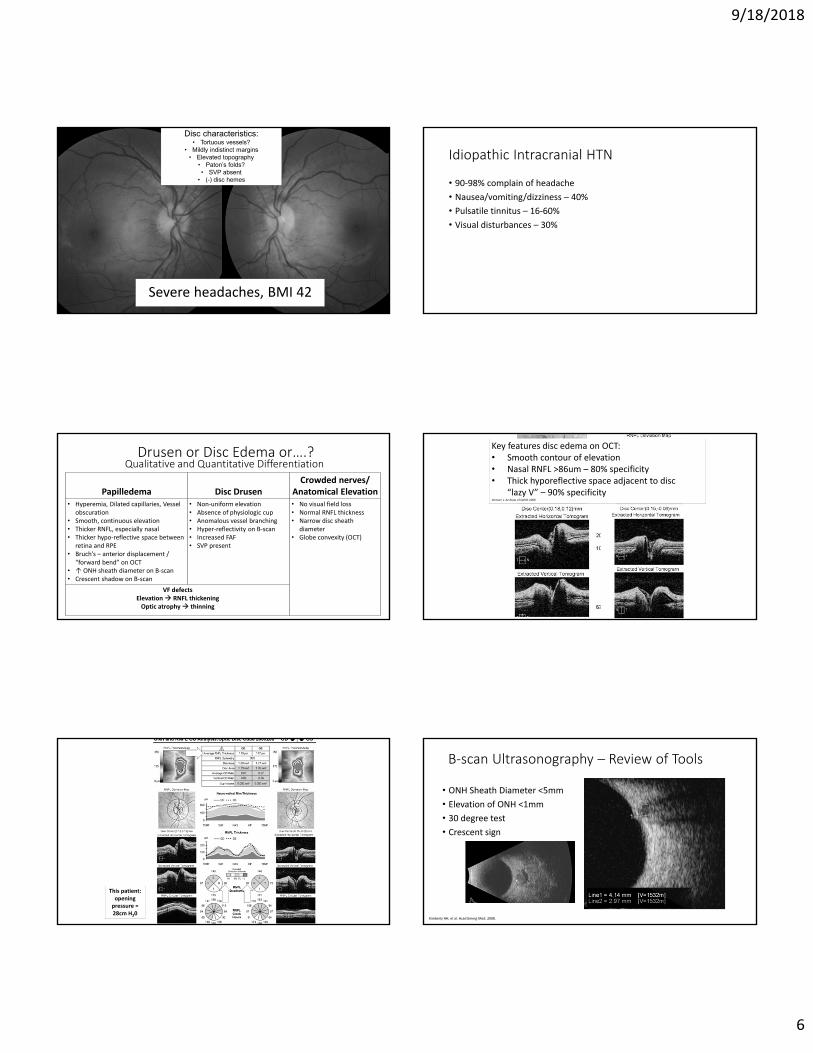
32 AA FM
9/18/2018
6
Disc characteristics: • Tortuous vessels?
• Mildly indistinct margins• Elevated topography
• Paton’s folds? • SVP absent
• (-) disc hemes
Severe headaches, BMI 42
Idiopathic Intracranial HTN
• 90‐98% complain of headache
• Nausea/vomiting/dizziness – 40%
• Pulsatile tinnitus – 16‐60%
• Visual disturbances – 30%
Papilledema Disc DrusenCrowded nerves/
Anatomical Elevation• Hyperemia, Dilated capillaries, Vessel
obscuration• Smooth, continuous elevation• Thicker RNFL, especially nasal• Thicker hypo‐reflective space between
retina and RPE• Bruch’s – anterior displacement /
“forward bend” on OCT• ↑ ONH sheath diameter on B‐scan• Crescent shadow on B‐scan
• Non‐uniform elevation• Absence of physiologic cup• Anomalous vessel branching• Hyper‐reflectivity on B‐scan• Increased FAF• SVP present
• No visual field loss• Normal RNFL thickness • Narrow disc sheath
diameter• Globe convexity (OCT)
VF defectsElevation RNFL thickeningOptic atrophy thinning
Drusen or Disc Edema or….? Qualitative and Quantitative Differentiation
Key features disc edema on OCT:• Smooth contour of elevation• Nasal RNFL >86um – 80% specificity• Thick hyporeflective space adjacent to disc
“lazy V” – 90% specificity Johnson L. Archives of Ophth 2009.
This patient: opening pressure = 28cm H20
B‐scan Ultrasonography – Review of Tools
• ONH Sheath Diameter <5mm
• Elevation of ONH <1mm
• 30 degree test
• Crescent sign
Kimberly HH, et al. Acad Emerg Med. 2008.
9/18/2018
7
Those tools can miss subtle elevation….. 3 years earlier, the was consistent with anatomical elevation; then lost to f/u x 3 years
…3 years later patient decides to come back
• 21 AAF
• High BMI
• MRI clear
• Initial opening pressure of 52
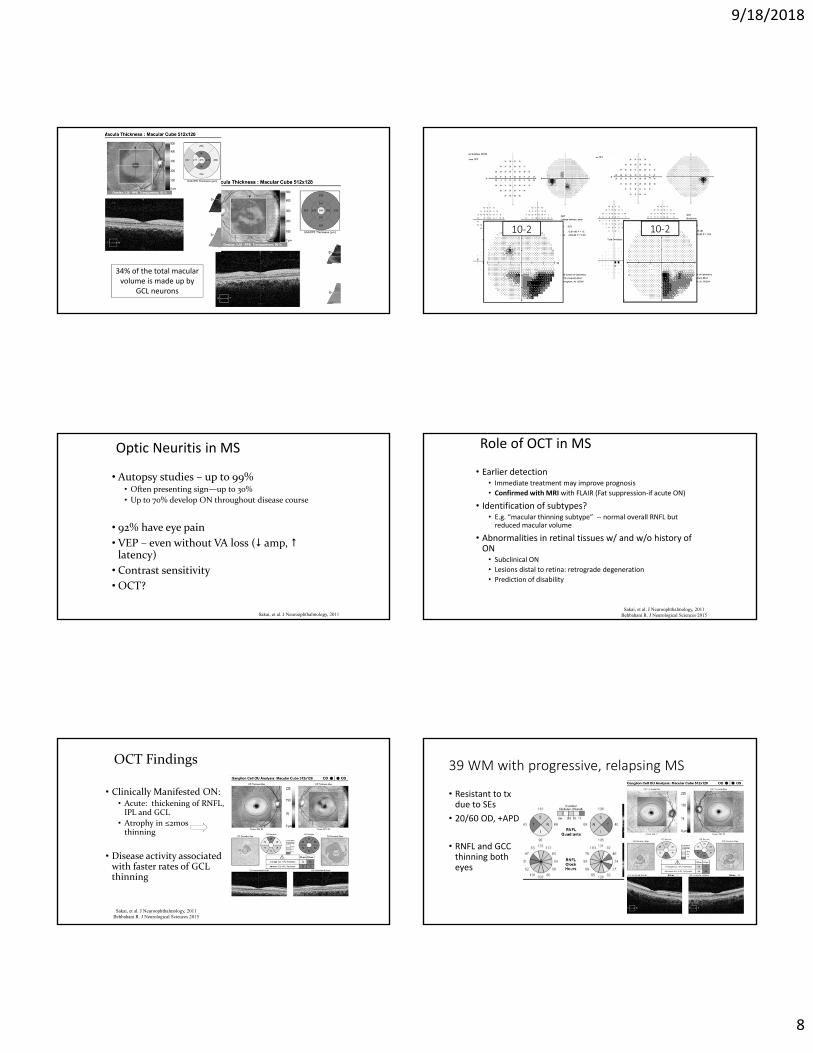
IIH Treatment Trial – JAMA, April 2014
• In patients with IIH and mild visual loss, the use of acetazolamide with a low‐sodium weight‐reduction diet compared with diet alone resulted in modest improvement in visual field function.
• Papilledema Outcomes from the Optical Coherence Tomography Substudy of the Idiopathic Intracranial Hypertension Treatment Trial. Ophthalmology, Sept 2015.
• Acetazolamide and weight loss effectively improve RNFL thickness, TRT, and ONH volume swelling measurements resulting from papilledema
• RNFL and Total Retinal Thickness (TRT) useful in following and monitoring response to treatment
Acetazolamide + Low Sodium/Wt Loss Diet
The Idiopathic Intracranial Hypertension Treatment Trial. JAMA 2014
• 42 AA female
• R/v: headache
• Father has glaucoma
• ROS: arm weakness
• BVA 20/20 after corrected significant cylinder
• Pupils normal
• Color (HRR) normal OD, OS
• IOP 21, 20
9/18/2018
8
34% of the total macular volume is made up by
GCL neurons
10‐2 10‐2
Optic Neuritis in MS
• Autopsy studies – up to 99%• Often presenting sign—up to 30%
• Up to 70% develop ON throughout disease course
• 92% have eye pain
• VEP – even without VA loss ( amp, latency)
• Contrast sensitivity• OCT?
Sakai, et al. J Neuroophthalmology, 2011
Role of OCT in MS
• Earlier detection • Immediate treatment may improve prognosis
• Confirmed with MRI with FLAIR (Fat suppression‐if acute ON)
• Identification of subtypes?• E.g. “macular thinning subtype” ‐‐ normal overall RNFL but reduced macular volume
• Abnormalities in retinal tissues w/ and w/o history of ON
• Subclinical ON
• Lesions distal to retina: retrograde degeneration
• Prediction of disability
Sakai, et al. J Neuroophthalmology, 2011Behbahani R. J Neurological Sciences 2015
OCT Findings
• Clinically Manifested ON:• Acute: thickening of RNFL, IPL and GCL
• Atrophy in ≤2mosthinning
• Disease activity associated with faster rates of GCLthinning
Sakai, et al. J Neuroophthalmology, 2011Behbahani R. J Neurological Sciences 2015
39 WM with progressive, relapsing MS
• Resistant to txdue to SEs
• 20/60 OD, +APD
• RNFL and GCC thinning both eyes
9/18/2018
9
Optic Neuritis Treatment Trial, circa 1992
• IV steroids over oral • 1000mg IV methylpred x 3 days • Speeds recovery of vision; reduces recurrences
• Alternative? Considerations?• Bioequivalent Oral Steroid–
• oral prednisone (1250‐mg over 3 days ) vs. high dose IV over 3 days • No significant differences in VA, Contrast Sensitivity, VEP at 1 month or 6 months Morrow et al. JAMA Neurology 2018.
• Steroid “Smoothie”
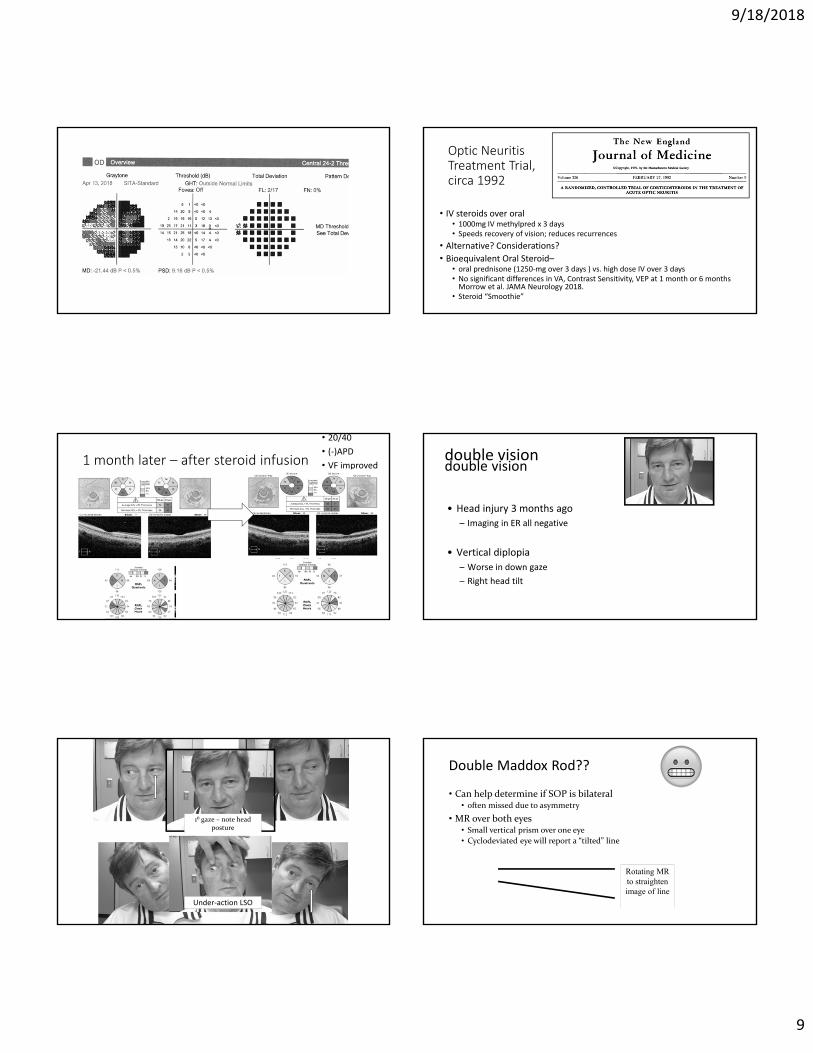
1 month later – after steroid infusion
• 20/40
• (‐)APD
• VF improved double vision
• Head injury 3 months ago
– Imaging in ER all negative
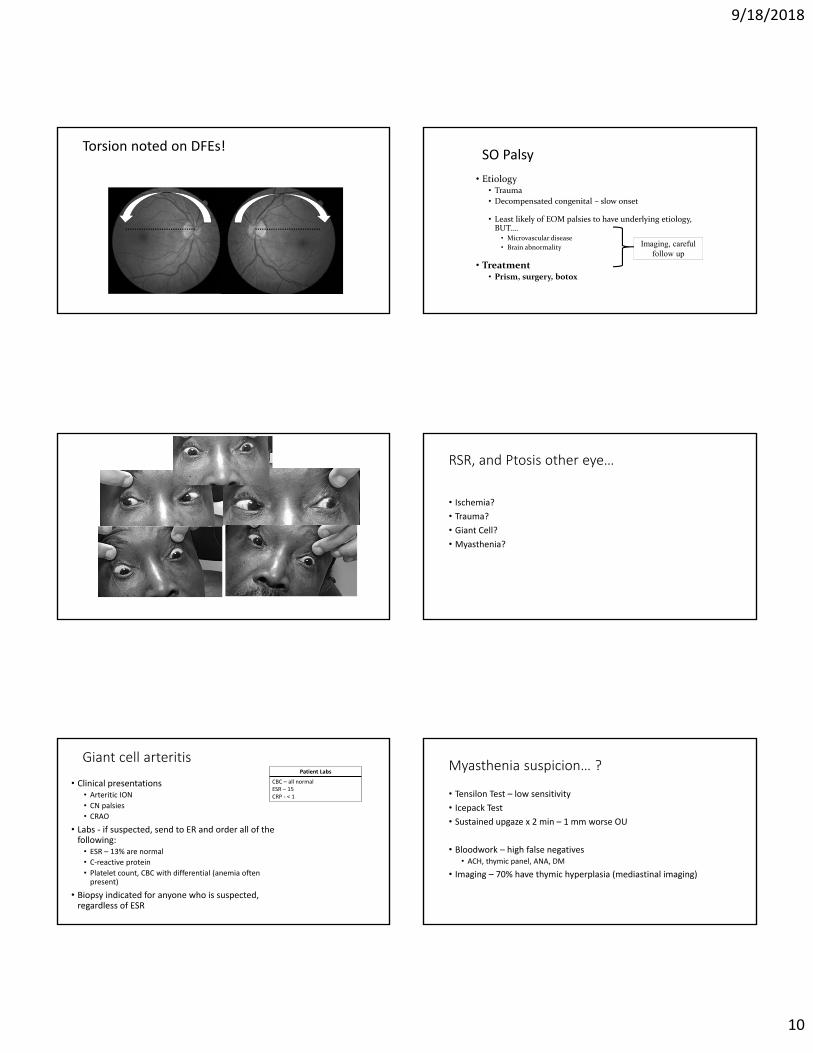
• Vertical diplopia
– Worse in down gaze
– Right head tilt
double vision
Under‐action LSO
1⁰ gaze – note head posture
Double Maddox Rod??
• Can help determine if SOP is bilateral• often missed due to asymmetry
• MR over both eyes• Small vertical prism over one eye
• Cyclodeviated eye will report a “tilted” line
Rotating MR to straighten image of line
9/18/2018
10
Torsion noted on DFEs!SO Palsy
• Etiology• Trauma
• Decompensated congenital – slow onset
• Least likely of EOM palsies to have underlying etiology, BUT….
• Microvascular disease
• Brain abnormality
• Treatment • Prism, surgery, botox
Imaging, careful follow up
RSR, and Ptosis other eye…
• Ischemia?
• Trauma?
• Giant Cell?
• Myasthenia?
Giant cell arteritis
• Clinical presentations• Arteritic ION
• CN palsies
• CRAO
• Labs ‐ if suspected, send to ER and order all of the following:
• ESR – 13% are normal
• C‐reactive protein
• Platelet count, CBC with differential (anemia often present)
• Biopsy indicated for anyone who is suspected, regardless of ESR
Patient Labs
CBC – all normal ESR – 15CRP ‐ < 1
Myasthenia suspicion… ?
• Tensilon Test – low sensitivity
• Icepack Test
• Sustained upgaze x 2 min – 1 mm worse OU
• Bloodwork – high false negatives • ACH, thymic panel, ANA, DM
• Imaging – 70% have thymic hyperplasia (mediastinal imaging)
9/18/2018
11
VI Palsy – Pearls
• Children• Frequently acquired and transient
• Trauma, tumor, hydrocephalus
• Adults • Trauma
• Neoplasm
• Microvascular disease
Significant risk of morbidity – imaging
even if other risk factors present
Rutsein, Daum. Anomalies of Binocular Vision
http://cim.ucdavis.edu/EyeRelease/Interface/TopFrame.htm
EOM palsies: Do not assume……
1. Vasculopathic 16.5% thought to be ischemic had another cause (neoplasm, MS, GCA)
Tamhankar, et al. Ophthalmology Nov 2013
2. True isolation
Caro d Artery Dissec on → Painful Horner’s
• 48 year old male presents with a big pupil in the left eye.
• ROS: right‐sided neck pain, headache
• Exam• Right eye – miosis, ptosis
• Dilates with 0.5% apraclonidine
• Horner’s – 3rd order neuron defect along sympathetic pathway
http://www.cmaj.ca
Carotid Artery Dissection
Lu A, et al. Emerg Radiol Feb 2015
Carotid Artery Dissection
• Presentation• Headache – up to 69%‐ most common presenting symptom• Unilateral neck pain – up to 49%• Ipsilateral Horner’s – up to 50% • Visual manifestations associated with artery dissections
• Photopsia• VF defect
• Cause of 2.5% of strokes• 10‐25% of ischemic events in patients <45Rao, J Vasc Surg 2011
• Mgmnt• Immediate Imaging: CT/CTA, MRI/A, T1W with contrast and fat suppression
• Doppler
Kwak JH, et al. Neurointervention, 2011.
Big pupil problem think 3rd N
• Parasympathetic pupillary fibers are located superficially along 3rd CN
• Likely to be affected early with compressive lesion
• Anatomically at risk• 85% are within anterior Circle of Willis
• 30‐35% are adjacent to 3rd CN
• Imaging Considerations
Kanski. Clinical Ophthalmology, 4th Ed
9/18/2018
12
3rd Nerve –a nice overview
Presentation bilateral in 11% complete in 33% isolated in 36%
Etiology trauma (26%) tumor (12%) diabetes (11%) aneurysm (10%) surgery (10%) stroke (8%) infection (5%)
Of 234 patients with diabetes 2/3 due to microvascular ischemia
53% had pupillary involvement-often bilateral 5 had aneurysms
Only 2% of aneurysms spared the pupil.
Painful onset 94% of aneurysm 69% of diabetic cases.
Keane JR, Can J Neuro Sci. 2010 Sep;37(5):662-70.
1400 personally examined patients – 37 years
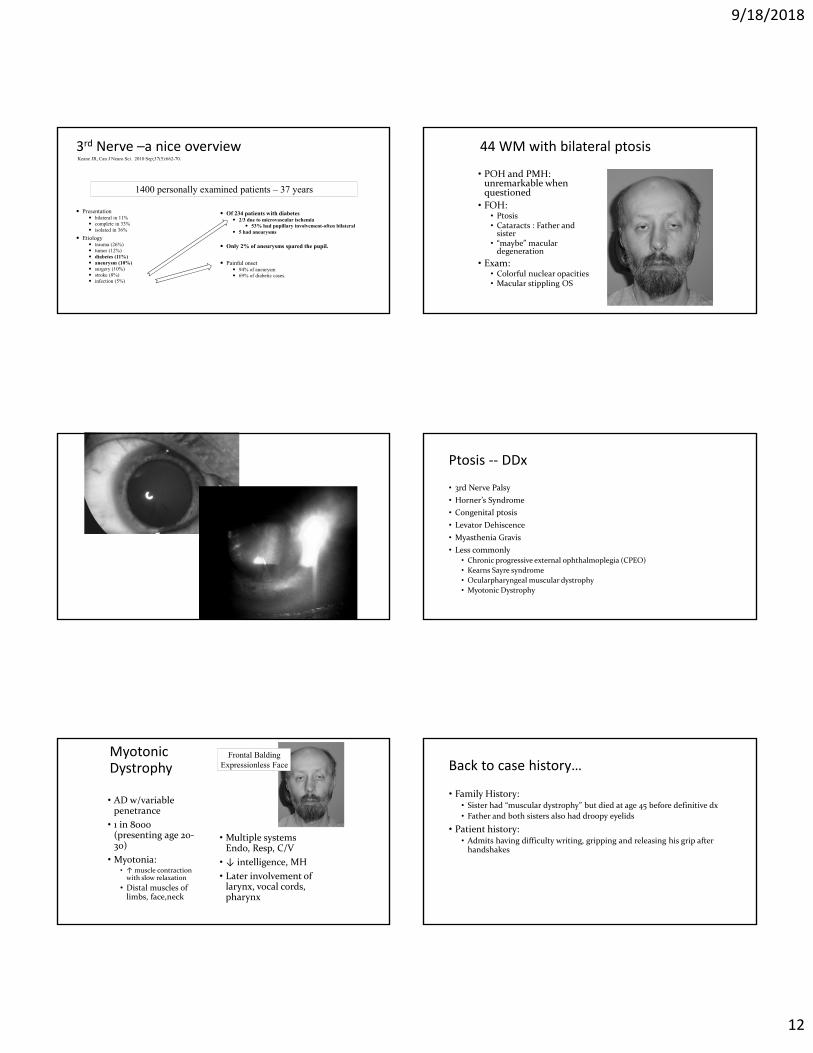
44 WM with bilateral ptosis
• POH and PMH: unremarkable when questioned
• FOH: • Ptosis• Cataracts : Father and sister
• “maybe” macular degeneration
• Exam: • Colorful nuclear opacities• Macular stippling OS
Ptosis ‐‐ DDx
• 3rd Nerve Palsy
• Horner’s Syndrome
• Congenital ptosis
• Levator Dehiscence
• Myasthenia Gravis
• Less commonly• Chronic progressive external ophthalmoplegia (CPEO)
• Kearns Sayre syndrome
• Ocularpharyngeal muscular dystrophy
• Myotonic Dystrophy
Myotonic Dystrophy
• AD w/variable penetrance
• 1 in 8000 (presenting age 20‐30)
• Myotonia: • ↑ muscle contraction with slow relaxation
• Distal muscles of limbs, face,neck
• Multiple systems Endo, Resp, C/V
• ↓ intelligence, MH
• Later involvement of larynx, vocal cords, pharynx
Frontal BaldingExpressionless Face Back to case history…
• Family History:• Sister had “muscular dystrophy” but died at age 45 before definitive dx
• Father and both sisters also had droopy eyelids
• Patient history:• Admits having difficulty writing, gripping and releasing his grip after handshakes
9/18/2018
13
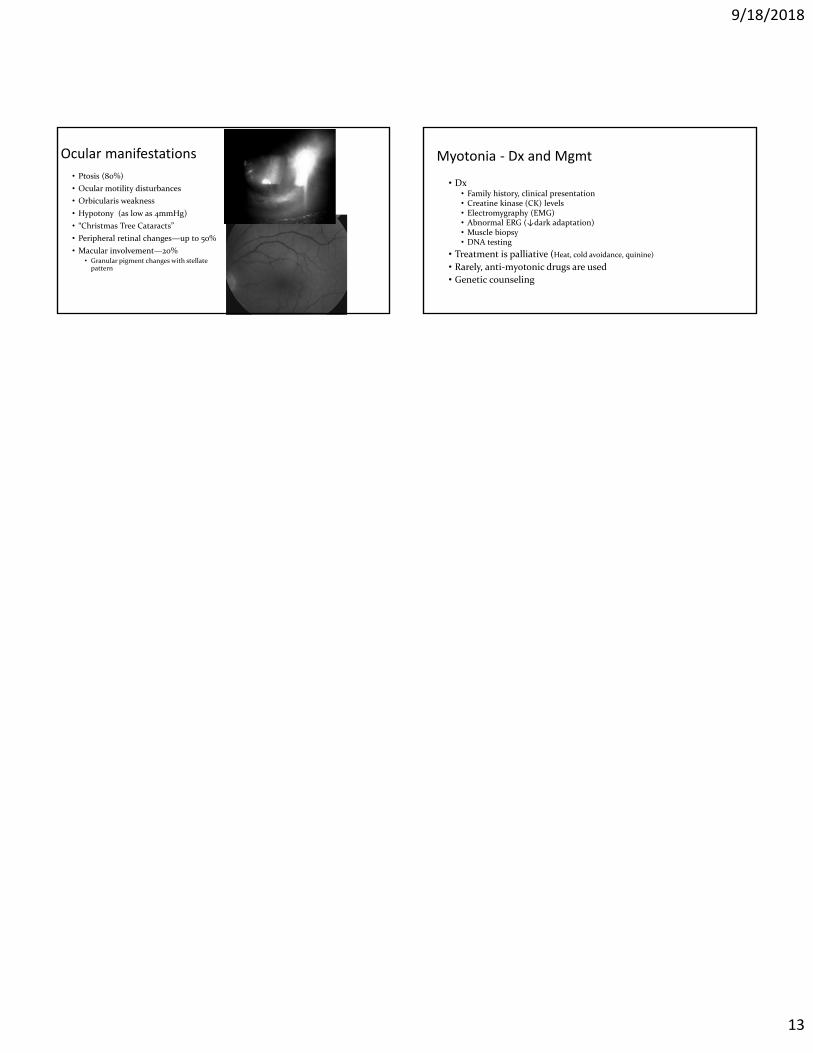
Ocular manifestations
• Ptosis (80%)
• Ocular motility disturbances
• Orbicularis weakness
• Hypotony (as low as 4mmHg)
• “Christmas Tree Cataracts”
• Peripheral retinal changes—up to 50%
• Macular involvement—20%• Granular pigment changes with stellate pattern
Myotonia ‐ Dx and Mgmt
• Dx• Family history, clinical presentation• Creatine kinase (CK) levels• Electromygraphy (EMG)• Abnormal ERG (↓dark adaptation)• Muscle biopsy• DNA testing
• Treatment is palliative (Heat, cold avoidance, quinine)
• Rarely, anti‐myotonic drugs are used
• Genetic counseling