Embed Size (px)
Citation preview

Systematic Review: Outpatient Management of Acute
Uncomplicated Diverticulitis (Int J Colorectal Dis (2014)29:775-781)
Mr John JacksonMr Nigel Noor
Mr Toby Hammond

Presentation Contents
• Background
• Methods
• Results
• Discussion
• Conclusions

Background
• Diverticular disease is common.
• Most frequent complication is acute diverticulitis.
• Acute diverticulitis is classified as either complicated or uncomplicated.
• The majority of patients present with uncomplicated disease.

Acute Uncomplicated Diverticulitis (AUD) Current Practice
• 87,202 acute admissions in England annually (HES data 2011-12)
• Traditional management involves Bowel Rest, IV fluids, IV antibiotics
• Significant clinical and financial implications
• Expert opinion - no evidence

Systematic Review: Methods• PRISMA guidelines
• Two researchers independently searched Medline, Embase and Cochrane Library databases
• Eligible studies: – Peer-reviewed articles investigating suitability of
ambulatory treatment protocols for AUD
– Search terms ‘Diverticulitis’, ‘Outpatient’, ‘Out-patient’, ‘Home’

Methods continued
Methods continued
The data sought from each study included:
• Type of study
• Selection criteria of Patients
• Imaging modality
• Nature of intervention
• Success rates
• Methods and duration of follow-up.
Results
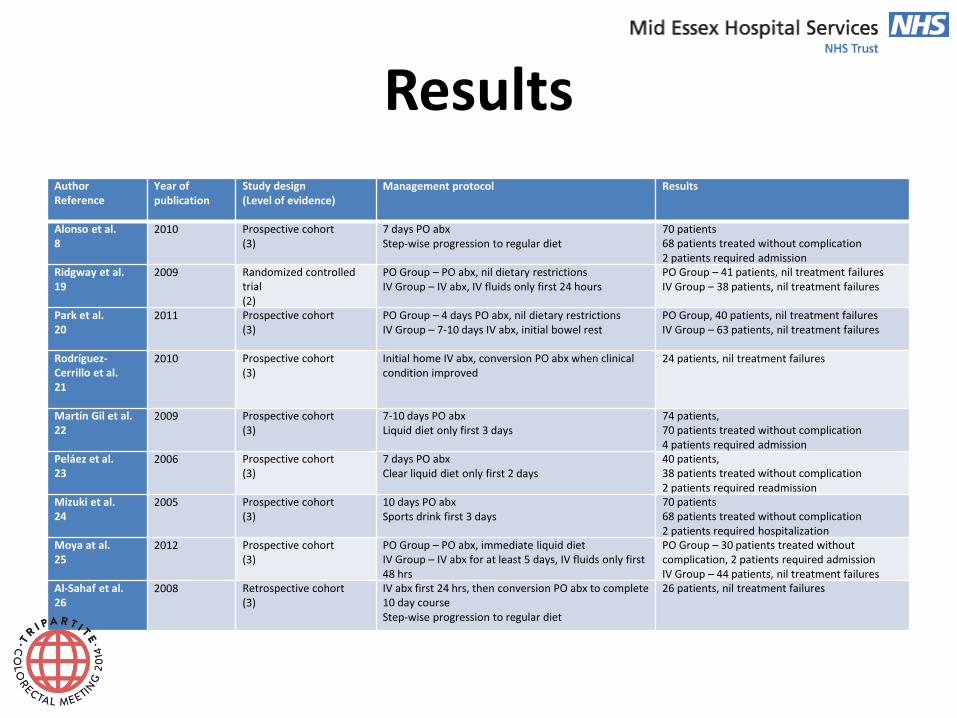
• 9 studies identified
– 1 RCT, 7 Prospective cohort, 1 Retrospective cohort
AuthorReference
Year of publication
Study design(Level of evidence)
Management protocol Results
Alonso et al.8
2010 Prospective cohort(3)
7 days PO abxStep-wise progression to regular diet
70 patients68 patients treated without complication2 patients required admission
Ridgway et al.19
2009 Randomized controlled trial(2)
PO Group – PO abx, nil dietary restrictionsIV Group – IV abx, IV fluids only first 24 hours
PO Group – 41 patients, nil treatment failuresIV Group – 38 patients, nil treatment failures
Park et al.20
2011 Prospective cohort(3)
PO Group – 4 days PO abx, nil dietary restrictionsIV Group – 7-10 days IV abx, initial bowel rest
PO Group, 40 patients, nil treatment failuresIV Group – 63 patients, nil treatment failures
Rodríguez-Cerrillo et al.21
2010 Prospective cohort(3)
Initial home IV abx, conversion PO abx when clinical condition improved
24 patients, nil treatment failures
Martín Gil et al.22
2009 Prospective cohort(3)
7-10 days PO abxLiquid diet only first 3 days
74 patients,70 patients treated without complication4 patients required admission
Peláez et al.23
2006 Prospective cohort(3)
7 days PO abxClear liquid diet only first 2 days
40 patients,38 patients treated without complication2 patients required readmission
Mizuki et al.24
2005 Prospective cohort(3)
10 days PO abxSports drink first 3 days
70 patients68 patients treated without complication2 patients required hospitalization
Moya at al.25
2012 Prospective cohort(3)
PO Group – PO abx, immediate liquid dietIV Group – IV abx for at least 5 days, IV fluids only first 48 hrs
PO Group – 30 patients treated without complication, 2 patients required admissionIV Group – 44 patients, nil treatment failures
Al-Sahaf et al.26
2008 Retrospective cohort(3)
IV abx first 24 hrs, then conversion PO abx to complete 10 day courseStep-wise progression to regular diet
26 patients, nil treatment failures

Results
Diagnosis and Severity Staging:• 7 utilized CT• 1 utilized USS• 1 utilized clinical judgment alone.
Radiological Exclusion Criteria:• Free Perforation• Colonic obstruction• Abscess/Phlegmon ≥3cm
Results
Non Radiological Exclusion Criteria:• Age >80 or >90• Vomiting or Not tolerating Oral intake • Severe Sepsis• Medical Comorbidities• Immunocompromised• Lack of Understanding• Lack of social support• Patient preference
Results
AUD established• Immediate discharge on oral antibiotics/ 24 hours
IV abx & fluids• Analgesia and laxatives• Normal diet
Commonest Antibiotic Regimen• Metronidazole + Cephalosporin• Co-Amoxiclav

Results
1 RCT: IV abx & bowel rest vs oral abx & no dietary restrictions (Ridgway 2009 Colorectal Dis 11:941–946 )
1o outcome: resolution of symptoms
No advantage to former

Results
Follow up 4-10 days post discharge in the majority of studies.
To exclude bowel cancer, 1 month after acute episode
• Colonoscopy
• CT colonography,
• Barium Enema

Results
403/415 (97%) AUD patients successfully managed as outpatients.
Reasons for failure:• persistent abdominal tenderness• vomiting• fever• acopia
4 studies addressed cost benefit• savings 35 – 83%

Discussion
• AUD can be safely and effectively managed in the community.
• Economic benefits of such an approach were also demonstrated.
• Limitations
– high Risk of Bias across all the studies
– level II and III evidence.
Discussion
DIVER study - RCT:
98% patients successfully managed as outpatients
cost savings €1124.70/ patient
(Biondo, Ann Surg 2004)
AVOD study – RCT abx vs no abx for AUD:
no benefit for abx
(Chabok, Br J Surg. 2012)
Conclusion
• Current evidence shows ambulatory based approach for the majority of AUD patients is justified.
• Developed outpatient treatment algorithm based on these findings
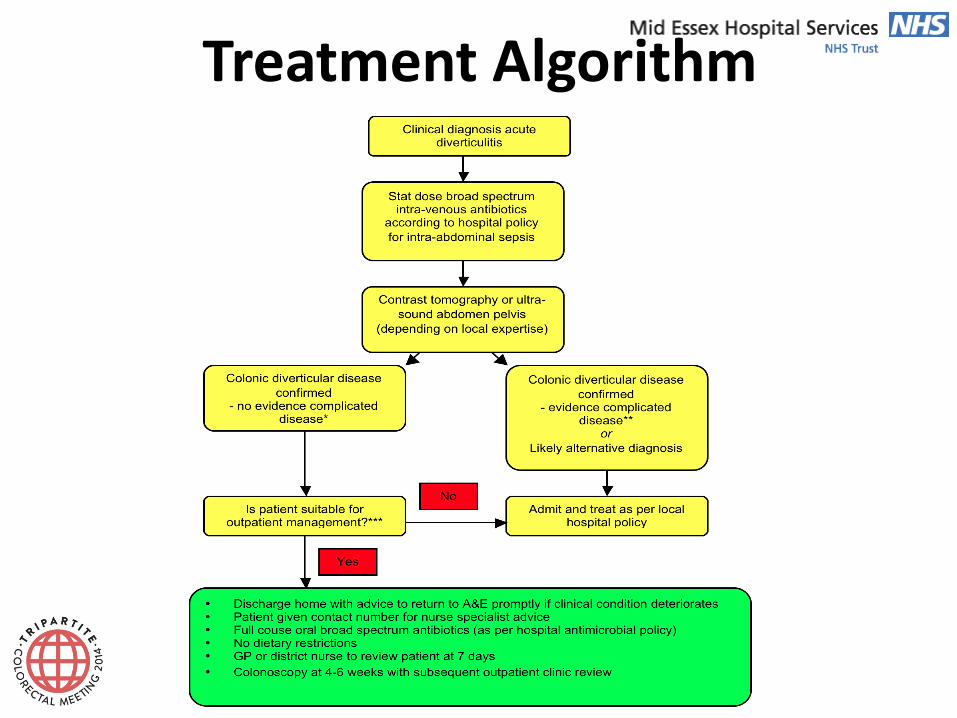
Treatment Algorithm



![The current management of acute uncomplicated appendicitishub.hku.hk/bitstream/10722/251485/1/content.pdf · of acute uncomplicated appendicitis with promising re-sults [6–8]. Appendectomy,](https://img.pdfslide.us/doc/110x75/5c9dec6588c993d8368bb27a/the-current-management-of-acute-uncomplicated-of-acute-uncomplicated-appendicitis.jpg)