Embed Size (px)
Citation preview

Syncope –cardiac causes
James Gnanapragasam
Paediatric cardiologist
Southampton University Hospital
Oxford University Hospital
Syncope
• Commonest cause - Vasovagal syncope• History typical in most
– On rising from seated or supine position– Sometimes in response to sight of blood, pain etc.– Preceding dizziness, blurring of vision– Awareness of impending faint– Rapidly self resolving– More common during intercurrent illness, poor oral
intake
Cardiac causes of syncope – all rare
• Long QT syndrome
• Hypertrophic obstructive cardiomyopathy
• Heart block
• Severe aortic stenosis
• Other arrhythmogenic disorders– Brugada syndrome– Arrhythmogenic right ventricular dysplasia
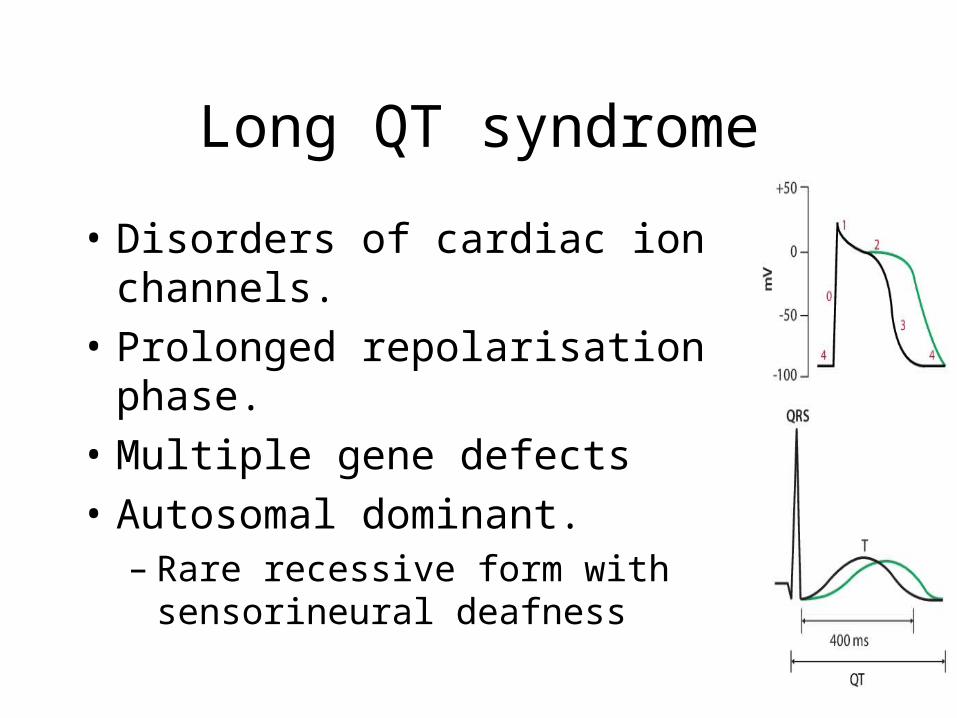
Long QT syndrome
• Disorders of cardiac ion channels.
• Prolonged repolarisation phase.
• Multiple gene defects
• Autosomal dominant. – Rare recessive form with sensorineural
deafness
Consider long QT syndrome if
• Collapse sudden and not related to posture• Collapse during exercise• Collapse during swimming• Collapse after sudden fright eg. loud noise• Family history of unexplained sudden death
– Palpitation not common (sudden collapse)– May have convulsions after collapse
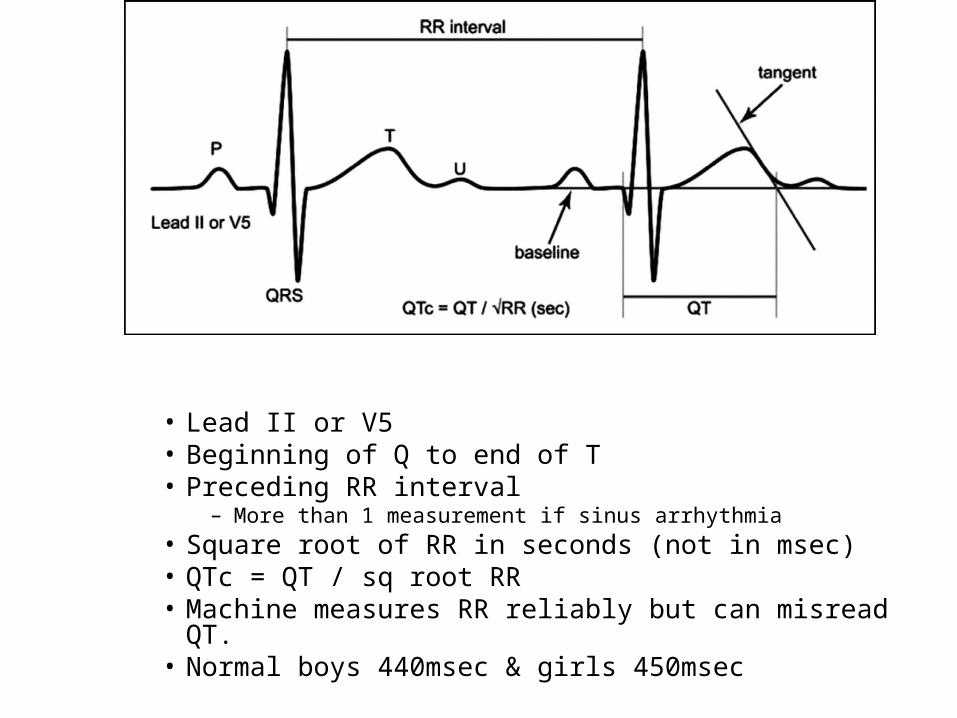
• Lead II or V5• Beginning of Q to end of T• Preceding RR interval
– More than 1 measurement if sinus arrhythmia• Square root of RR in seconds (not in msec)• QTc = QT / sq root RR• Machine measures RR reliably but can misread QT.• Normal boys 440msec & girls 450msec
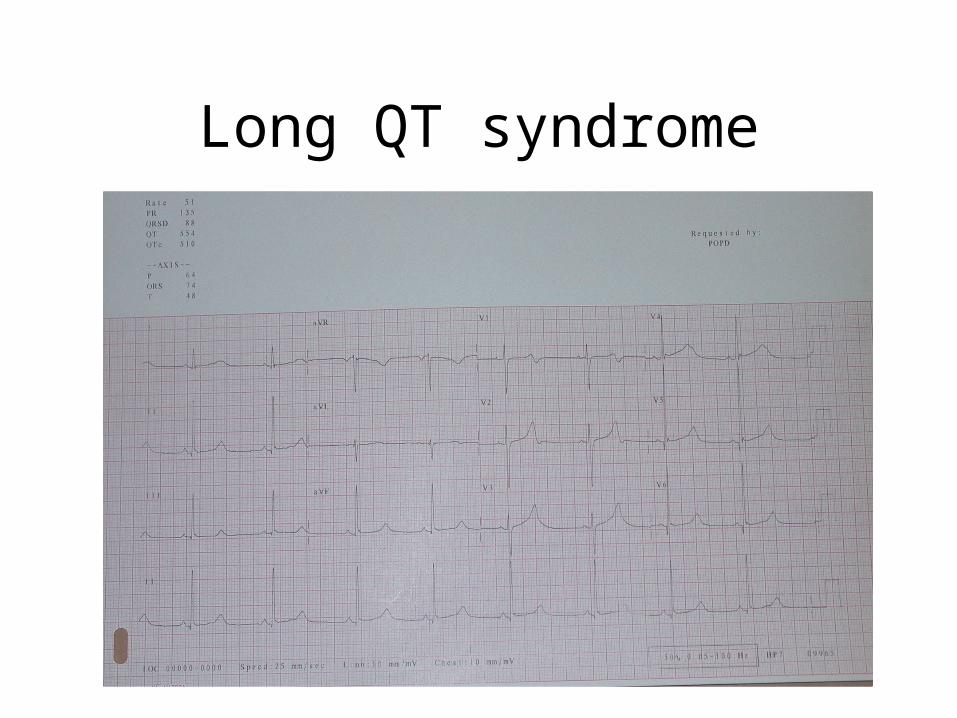
Long QT syndrome
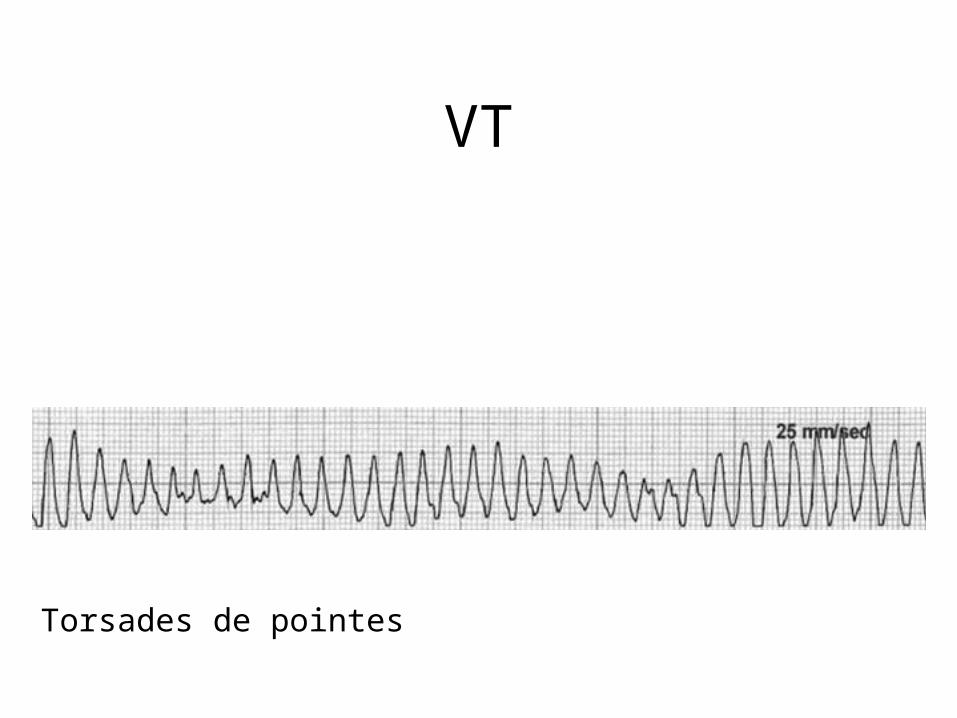
VT
Torsades de pointes
Management of Long QT syndrome
• Beta blocker– reduces risk of sudden death from VT
• Implantable defibrillators– if collapse /VT in spite of beta blockers

Hypertrophic cardiomyopathy• Syncope during exercise
• May not have a significant murmur
• Autosomal dominant / new mutation– Multiple gene defects
• ECG– Q waves
septumaorta
lv
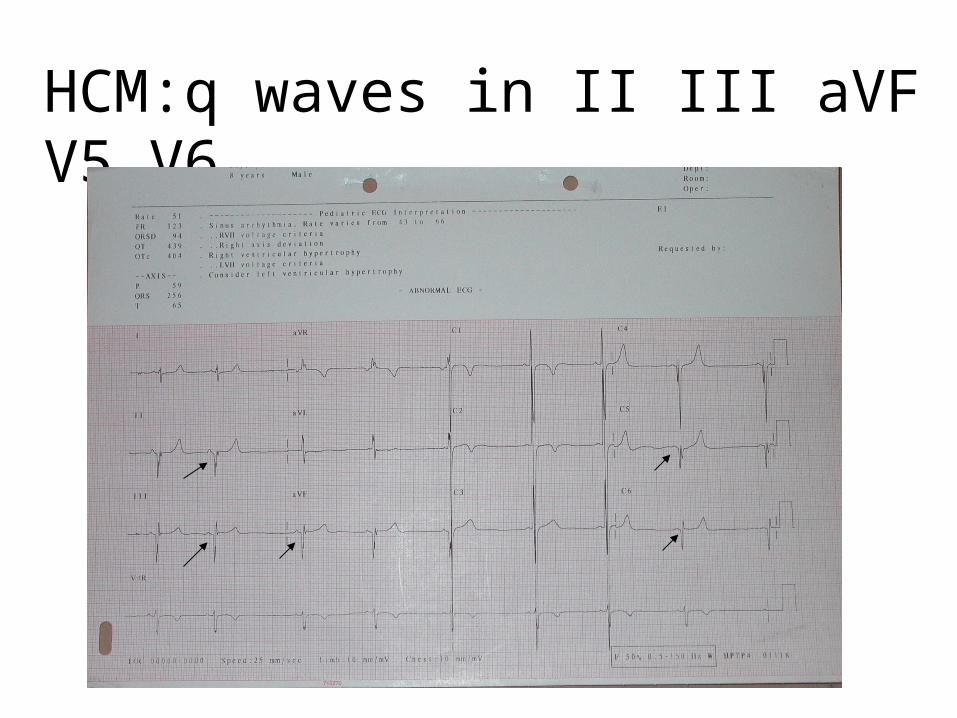
HCM:q waves in II III aVF V5 V6
If history of
– collapse during exercise – collapse very sudden– collapse while supine or seated– collapse in relation to sudden noise
• Refer to cardiologist (even ECG normal)
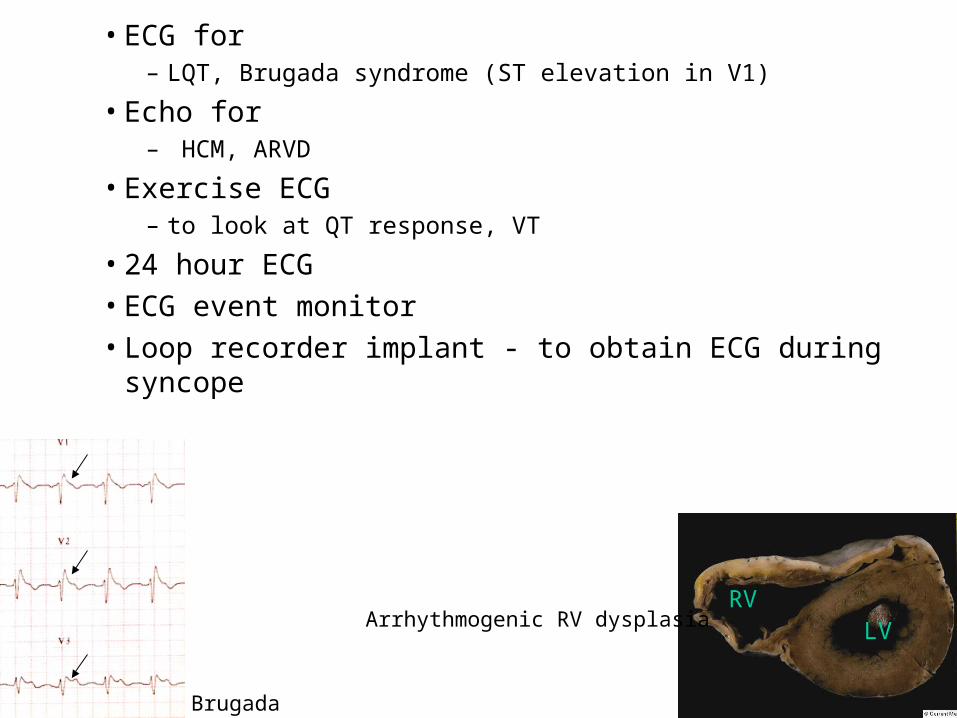
• ECG for – LQT, Brugada syndrome (ST elevation in V1)
• Echo for– HCM, ARVD
• Exercise ECG– to look at QT response, VT
• 24 hour ECG• ECG event monitor• Loop recorder implant - to obtain ECG during syncope
RVLV
Brugada
Arrhythmogenic RV dysplasia

Chest pain in children – when to consider a cardiac cause
James Gnanapragasam
Chest pain in children
• No identifiable cause
• Musculoskeletal
• Respiratory
• Gastrointestinal
• Psychogenic
• Cardiac (very rare)
Cardiac chest pain in children
• Pericarditis
• Coronary ischaemia– Congenital coronary abnormality– Acquired coronary abnormality post
surgery / post Kawasaki– Hypertrophic cardiomyopathy
Is the history suggestive of pericarditis?
– Recent febrile illness. – Pain on inspiration / postural change. – Chest pain co-existing with left
supraclavicular pain.
If history suggestive of pericarditis…
– Look for,• Pericardial rub• CXR
– cardiomegaly
• ECG – low QRS voltages– ST elevation, T inversion– PQ depression
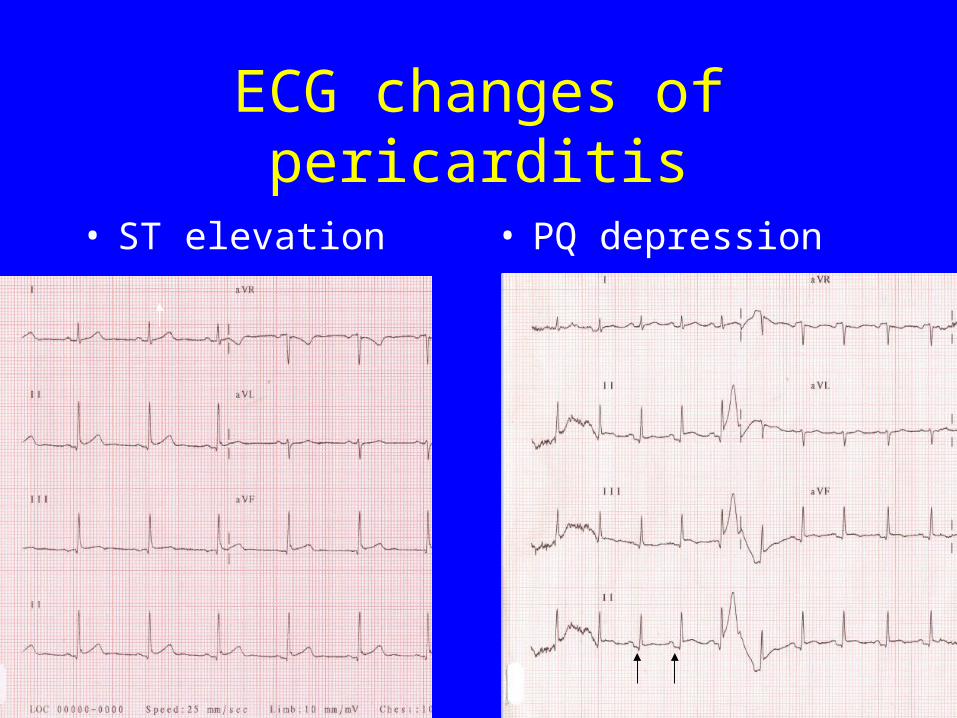
ECG changes of pericarditis
• ST elevation • PQ depression

Is the history suggestive of coronary ischaemia?
– Retrosternal crushing pain– Brought on by exercise– Never at rest
If history suggestive of ischaemic pain…
• ECG– ST segment & T wave changes of
ischaemia– Abnormal Q waves of HCM
• Troponin I assay– More specific and sensitive than CK-MB
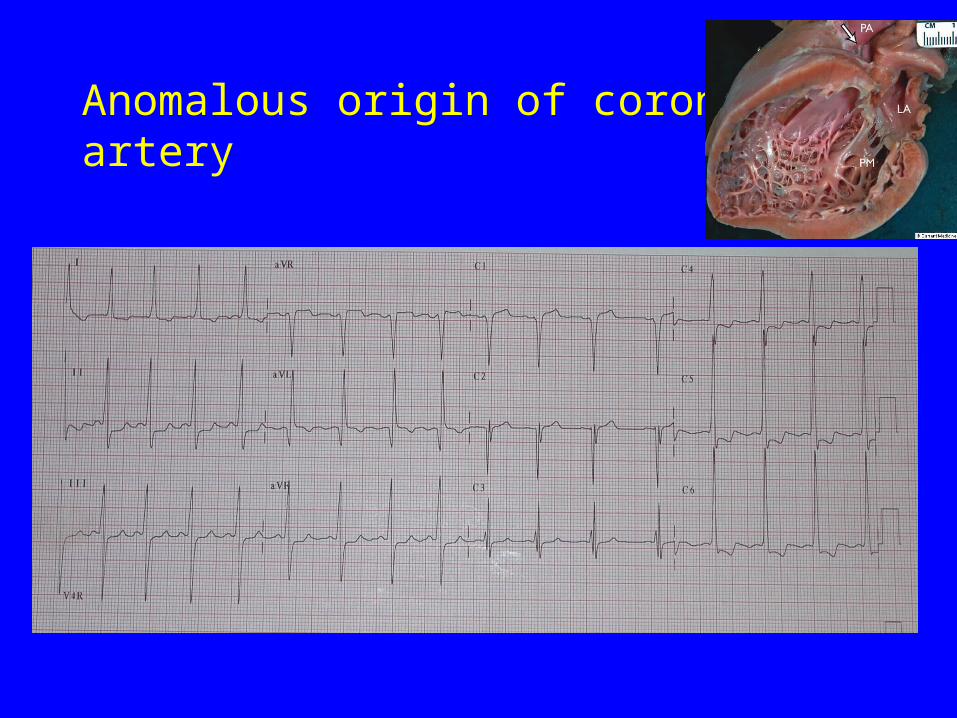
Anomalous origin of coronary artery
Chest pain in children - summary
• Cardiac cause extremely rare.
• History most important.– Suggestive of pericarditis?– Suggestive of ischaemia?
• Cardiac investigations not required if history not suggestive of cardiac cause.
Clinical examination of the heart in children
James Gnanapragasam
Pathological Features on auscultation
– Is the murmur loud & heard widely?– Is it heard over the back?– Does it have a high pitch?– Does it extend into diastole?– Is the second heart sound loud?– Is the second heart sound widely split?– Is there an ejection click?
How do you determine that the S2 is loud?
• Normal Second heart sound – louder than first heart sound at the upper
sternal border
• Loud Second heart sound – louder than first heart sound in all areas.
Loud second heart sound
• Elevated pulmonary artery pressures
• Transposition of great arteries
• Abnormally positioned arteries in complex defects
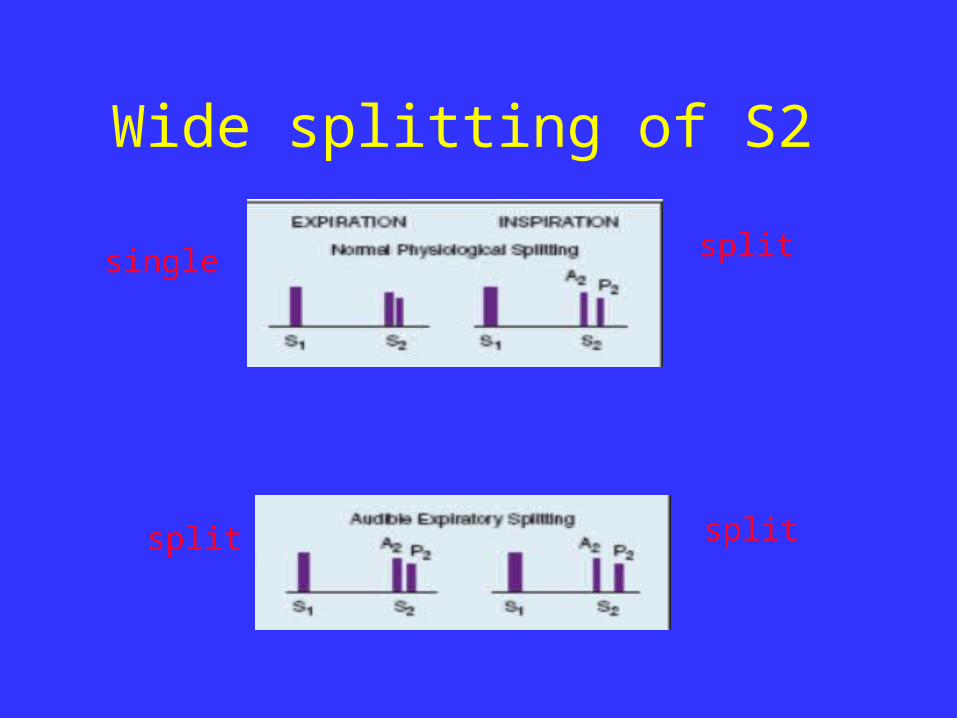
Wide splitting of S2
single split
splitsplit

Wide splitting of S2
single single
splitsingle
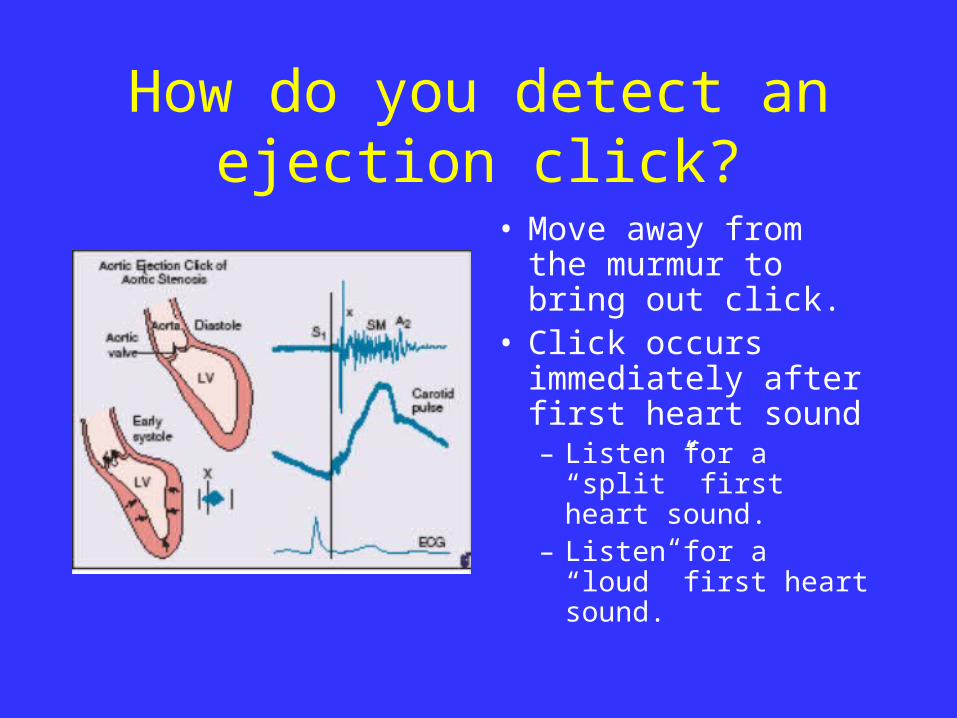
How do you detect an ejection click?
• Move away from the murmur to bring out click.
• Click occurs immediately after first heart sound– Listen for a “split”
first heart sound.– Listen for a “loud”
first heart sound.
• Listen with diaphragm – Vary the pressure on chest to elicit the
qualities of sounds and murmurs
Ejection click
• Aortic stenosis
• Pulmonary stenosis
• Heart defects with dilated aorta / pulmonary artery.
Asymptomatic infant with a murmur
• Is the murmur loud?• Is it heard over the back?• Does it have a high pitch or abnormal quality?• Are there any abnormal sounds?
• Is the cardiac impulse normal?• Is the femoral pulse equal to the brachial?• Is there cyanosis? (pulse oximetry)• Is there tachypnoea, hepatomegaly or FTT?
Palpation of heart in infants
• Most major congenital defects will lead to a right heart impulse. – Palpate at the sternal border and
epigastrium
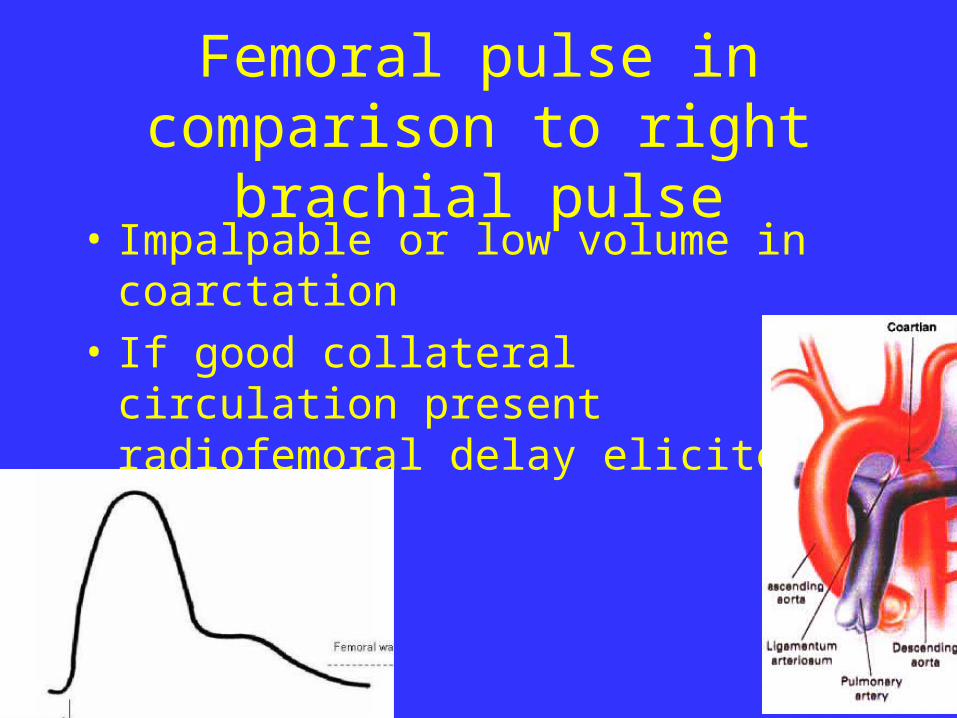
Femoral pulse in comparison to right brachial pulse
• Impalpable or low volume in coarctation
• If good collateral circulation present radiofemoral delay elicited.
Cyanosis
– Mild desaturation (85-93% SaO2) in infants is often clinically undetectable
• Check gums and tongue for duskiness or lack of pinkness
• Check oxygen saturation in all infants with murmurs

Commonest missed diagnosis -presenting in teenage/adult
• ASD• Parasternal impulse• Wide split second sound• Basal soft systolic murmur
• Coarctation• Low volume femorals• Soft murmur over back• Hypertension
ECG in the detection of congenital heart defects
James Gnanapragasam
ECG in children
• Are there signs of RA enlargement?– Tall & pointed p in II and V1
• Are there signs of LA enlargement?– Broad and bifid p in II
– Inverted p in V1• Is the QRS axis normal?
– R lower quadrant in infants. L lower in children.
• Is the QRS progression normal?
– Neonates R>S in V1 and S>R in V6.
– Infants R>S in V1 and in V6.
– Children S>R in V1 and R>S in V6.
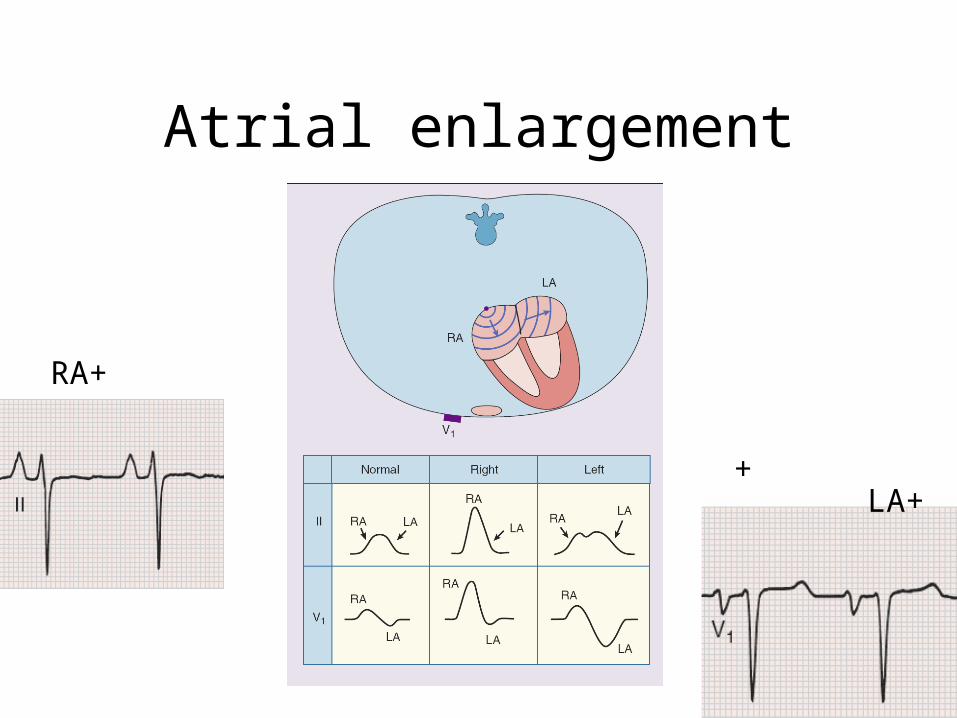
Atrial enlargement
RA+
+LA+
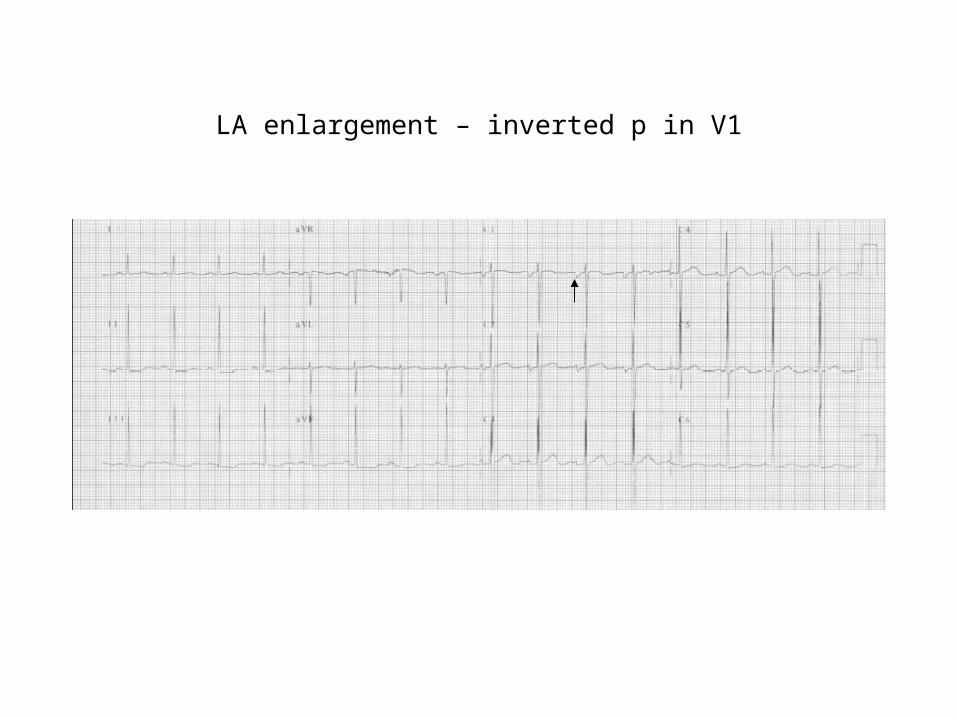
LA enlargement – inverted p in V1
ECG in children
• Are there signs of RA enlargement?
– Pointed p in II or V1
• Are there signs of LA enlargement?
– Broad and bifid p in II. Inversion of p in V1.
• Is the QRS axis normal?– R lower quadrant in infants.
– L lower in children.• Is the QRS progression normal?
– Neonates R>S in V1 and S>R in V6.
– Infants R>S in V1 and in V6.
– Children S>R in V1 and R>S in V6.

QRS axis
Normalinfant
Normalchild
-
-
+

Superior axis
Causes: AVSDTricuspid artesiaEbsteinsHypertrophic cardiomyopathyWPWNoonans syndrome
ECG in children
• Are there signs of RVH?– Lone R in V1.
– Upright T in V1 after 7 days & up to 5 years age
• Are there signs of LVH?
– Abnormally tall R in V6 and deep S in V1.
– Flat or inverted T in V6.• Are there signs of RV dilatation?
– T wave inversion extending to V4. rsR in V1.
• Are there abnormal Q waves?
– Deep q in II III aVf and V5,6.
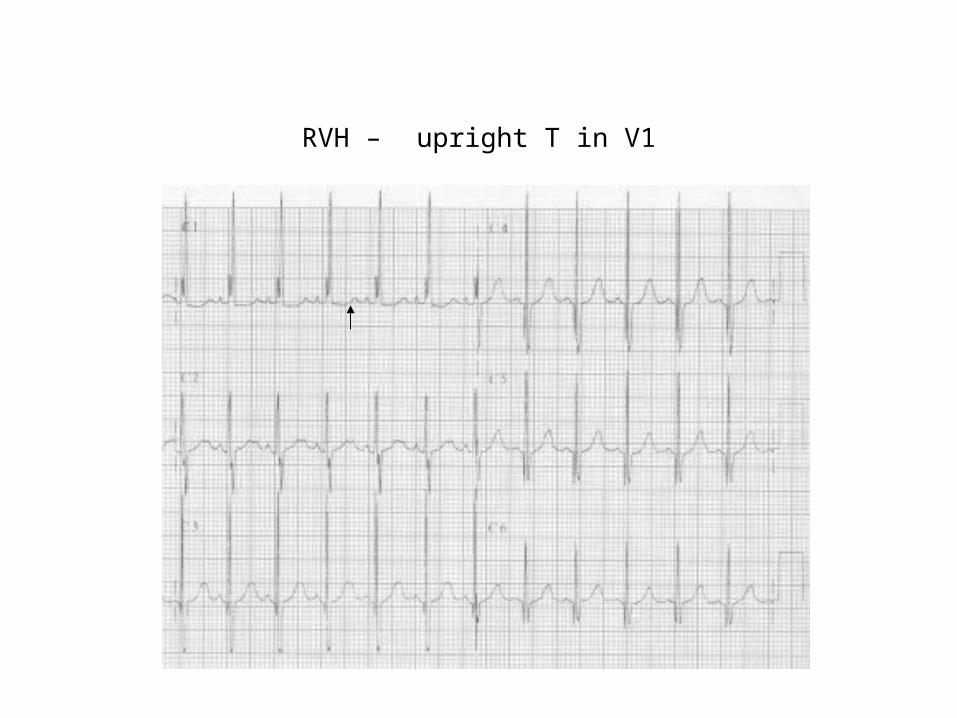
RVH – upright T in V1
ECG in children
• Are there signs of RVH?
– Lone R in V1. Upright T in V1 between 7 days & 5 years
• Are there signs of LVH?
– Abnormally tall R in V6 and deep S in V1. Flat or inverted T in V6.
• Are there signs of RV dilatation?– T wave inversion extending to V4. – rsR in V1.
• Are there abnormal Q waves?
– Deep q in II III aVf and V5,6.
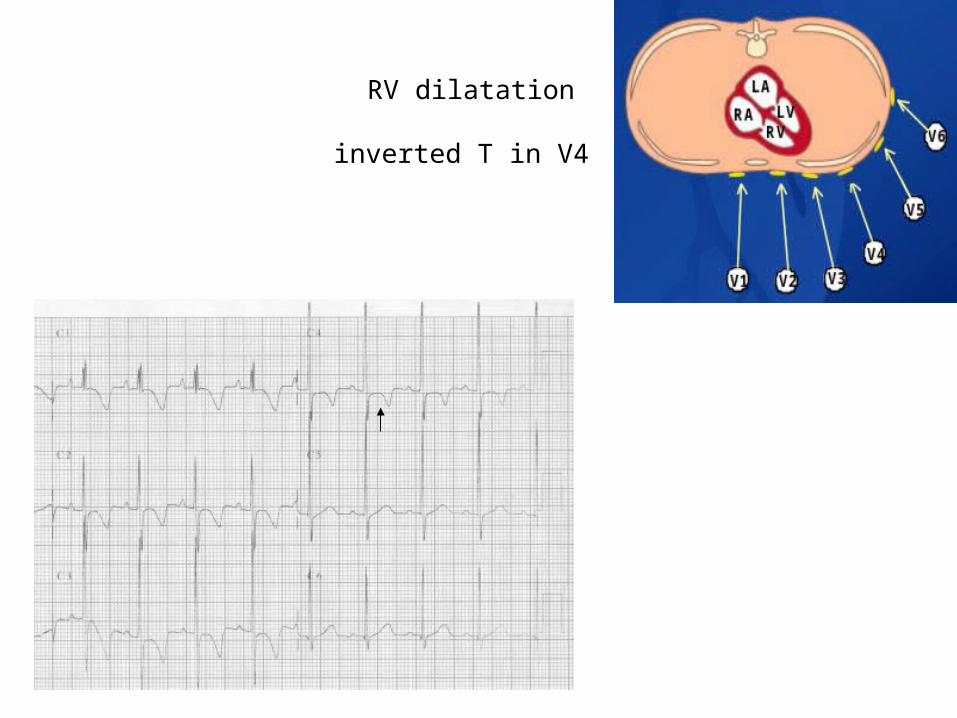
RV dilatation
inverted T in V4
ECG in children
• Are there signs of RVH?– Lone R in V1. Upright T in V1 between 7 days & 5 years
• Are there signs of RV dilatation?– T wave inversion extending to V4. rsR in V1.
• Are there signs of LVH?– Abnormally tall R in V6 and deep S in V1. Flat or
inverted T in V6.
• Are there abnormal Q waves?– Deep q in II III aVf V5 and V6.
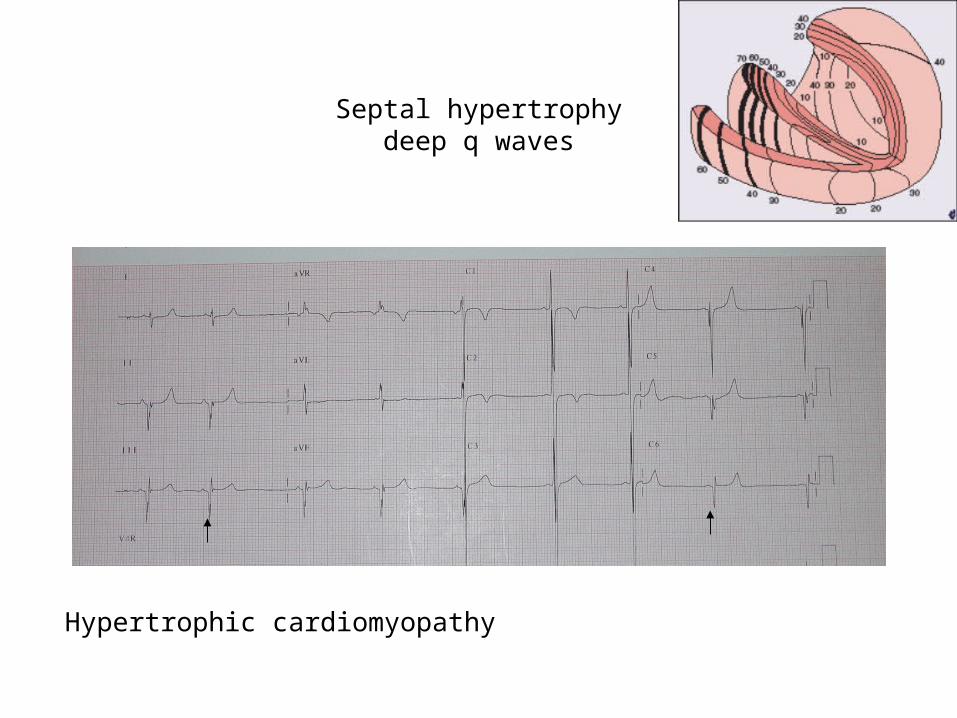
Septal hypertrophydeep q waves
Hypertrophic cardiomyopathy
Surgical outcomes
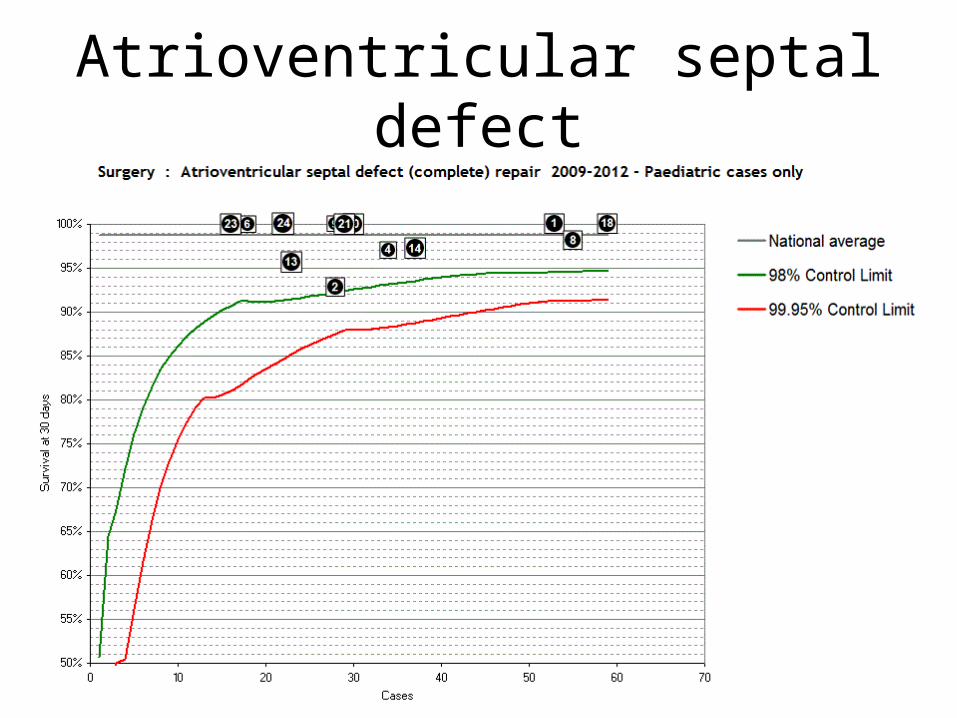
Atrioventricular septal defect
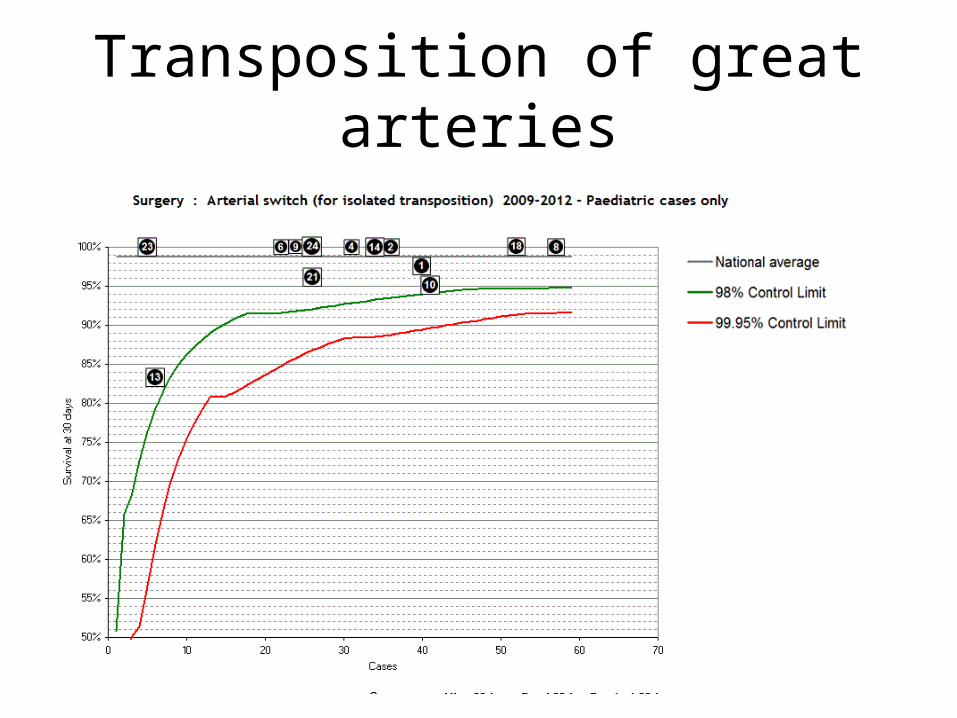
Transposition of great arteries
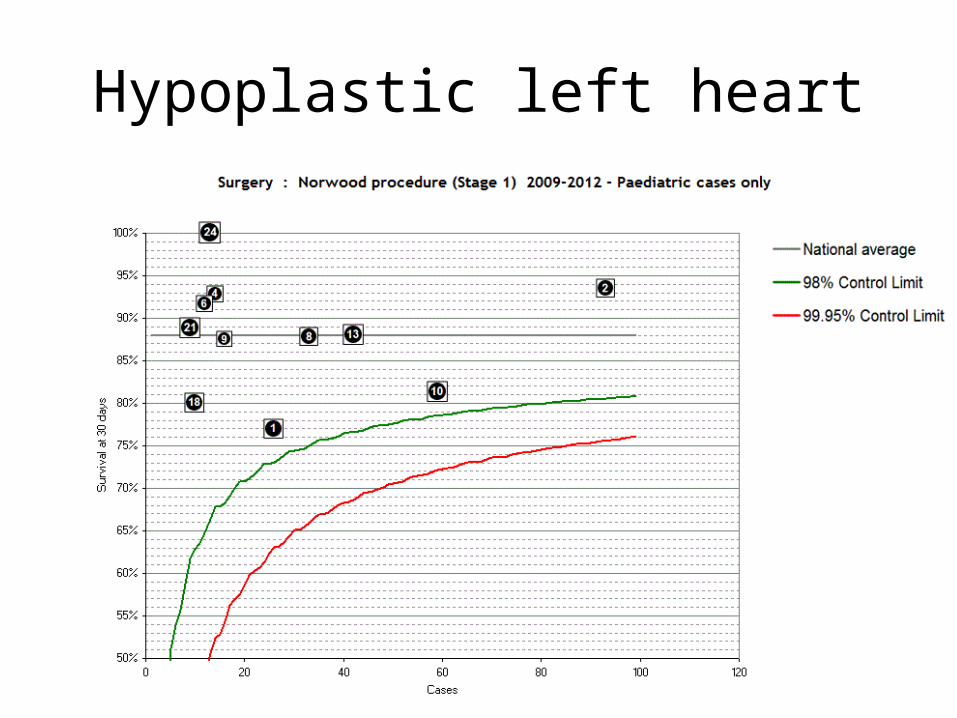
Hypoplastic left heart
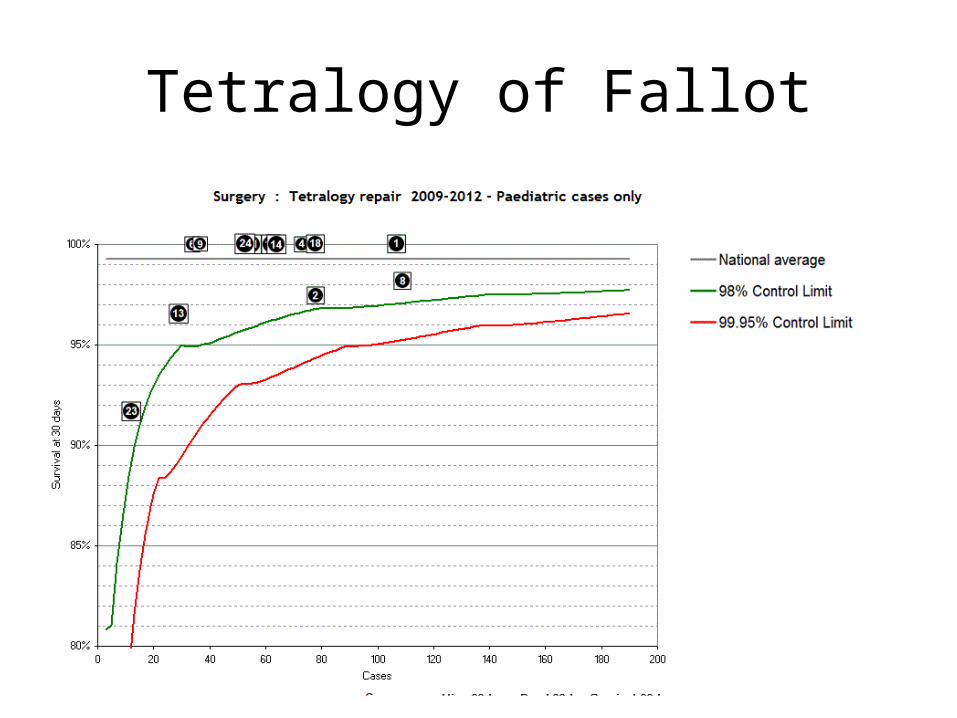
Tetralogy of Fallot












![Syncope AHD[1]](https://img.pdfslide.us/doc/110x75/577d36611a28ab3a6b92ec10/syncope-ahd1.jpg)