Embed Size (px)
Citation preview

Heart 1996;75:134-140
Salt supplement increases plasma volume andorthostatic tolerance in patients with unexplainedsyncope
H El-Sayed, R Hainsworth
AbstractObjective-To determine whether inpatients presenting with posturallyrelated syncope administration of saltincreases plasma volume and improvesorthostatic tolerance. Patients with poortolerance of orthostatic stress tend tohave lower than average plasma andblood volumes.Design-A double blind placebo con-trolled study in 20 patients and an openstudy in 11 of the effects of giving 120mmoUday of sodium chloride.Patients-31 patients presenting withepisodes of syncope who had no apparentcardiac or neurological disease. Plasmavolume was determined by Evans bluedye dilution, orthostatic tolerance by timeto presyncope in a test of combined head-up tilt and lower body suction, andbaroreceptor sensitivity by the effect ofneck- suction on pulse interval.Results-8 weeks after treatment, 15(70%) of the 21 patients given salt andthree (30%) of the placebo group showedincreases in plasma and blood volumesand in orthostatic tolerance, anddecreases in baroreceptor sensitivity.Improvement was related to initial saltexcretion in that patients who respondedto salt had a daily excretion below 170mmol. The patients in the placebo groupwho improved also showed increases insalt excretion.Conclusions-In patients with unex-plained syncope who had a relatively lowsalt intake administration of saltincreased plasma volume and orthostatictolerance, and in the absence of contra-indications, salt is suggested as a first lineof treatment.
(Heart 1996;75:134-140)
Keywords: orthostatic; syncope; baroreceptors; bloodvolume; salt
Institute forCardiovascularResearch, Universityof Leeds, LeedsH El-SayedR HainsworthCorrespondence to:Prof R Hainsworth, Institutefor Cardiovascular Research,University of Leeds, LeedsLS2 9JT.Accepted for publication17 October 1995
Syncope for no apparent cause in otherwisehealthy people is a relatively common clinicalproblem.' Frequently, patients are subjectedto an array of neurological and cardiovascularinvestigations and, if these are negative andthe patient gives a history suggestive oforthostatic hypotension, a diagnosis is madeof vasovagal, or neurocardiogenic, syncope.Sometimes the diagnosis can be confirmed byreproducing the hypotension during tilt-table
testing though this test is often negative.2Syncope may be provoked by combining tilt-ing with administration of isoprenaline.3 This,however, also induces syncope in manyasymptomatic volunteers.4 We have recentlyintroduced a test that combines head-up tilt-ing with lower body suction.5 We believe thatthis test, which causes progressive reduction invenous return and cardiac output, has a soundphysiological basis and we have shown that astage of the test can be defined which provokespresyncope in only 20% of asymptomatic vol-unteers but 85% of patients with historiesstrongly suggestive of posturally related syn-cope.6 Furthermore, because this test is repro-ducible, it should be useful in detectingresponses in individual patients to therapeuticinterventions. Indeed we have already exam-ined the effects of cardiac pacemakers usingthis test and shown that the time to presyn-cope was almost identical irrespective ofwhether or not the heart was being paced.7
Treatment of attacks of unexplained syn-cope is generally unsatisfactory and reports ofbenefits are often contradictory. For example,treatment with f,-adrenoceptor blocking agentshas been claimed by some8-'0 to relieve symp-toms, but others have found no benefit or evenan exacerbation of symptoms."1-'3 The benefitsof other agents also seem uncertain. 14 Oneform of treatment which has sometimes beenrecommended to prevent syncope is givingdietary salt supplements.15 The rationale forthis is that the body's sodium content deter-mines the volume of the extracellular fluid,including that of the plasma. Lately, we foundthat a subject's orthostatic tolerance is highlysignificantly correlated with his plasma vol-ume.'6 It is likely, therefore, that an increase inplasma volume would lead to an increase inorthostatic tolerance. The question remainswhether in patients with unexplained syncopean increase in dietary salt intake does increaseplasma volume. Reports based on animal stud-ies'7 or human studies'8 indicate that salt load-ing is likely to increase plasma volume.However, there have been no objective studiesof the effects of salt in patients with poororthostatic tolerance and the aim of the pre-sent work was to examine, using a doubleblind protocol, whether salt loading increasedboth plasma volume and orthostatic tolerance.
Patients and methodsWe studied a total of 31 patients complainingof attacks of syncope for which no cause hadbeen detected. These attacks were defined as a
134
on 3 August 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Heart: first published as 10.1136/hrt.75.2.134 on 1 F
ebruary 1996. Dow
nloaded from

Salt supplement increases plasma volume and orthostatic tolerance in patients with unexplained syncope
transient loss of consciousness and posturaltone, with spontaneous prompt and completerecovery. The attacks varied in frequency fromonly once ever to several attacks per day. Thenumber of attacks ranged from one to 30(median three) and the period over which theyoccurred ranged from three to 48 (median 12)months. Clinical examinations in all cases
were normal. The patients had been investi-gated as deemed appropriate by their physi-cians. All had blood cell counts, electrolyteanalyses, resting electrocardiography, 24 or 48hour Holter monitoring, and cardiac echocar-diography. Exercise electrocardiography was
undertaken in 25 patients, electroencephalog-raphy in eight, computed tomography scan ofthe head in six, and coronary angiography infive. All results were regarded as normal. Nopatient was receiving any medical treatment.
This paper is a report of two studies of theeffects of salt. The first was a double-blindplacebo controlled trial and the second was an
open study in which only salt treatment was
given. In both studies assessments were made,before and after eight weeks of taking salt or a
placebo, of plasma volume, haematocrit, meancorpuscular volume, orthostatic tolerance,baroreceptor sensitivity, and 24 hour urinarysodium excretion. In premenopausal women,the second study was undertaken on the same
day of the menstrual cycle as in the initialstudy and nearest to eight weeks. Between thetwo assessments, the patients took either saltor placebo. In the double blind study, theytook capsules containing 10 mmol sodiumchloride or placebo (12 per day). In the openstudy, they took slow sodium (Ciba) (10mmol, 12 per day). Patients were informedthat the trial was of "a mineral dietary supple-ment". Salt was not mentioned in the hopethat the patients would not modify their owndiets.
All patients were instructed to fast, exceptfor water, from midnight before the studies,and to report to the laboratory at 9-00 am.
The tests were then carried out in the same
sequence: plasma volume, baroreceptor sensi-tivity, orthostatic tolerance.The studies were approved by the United
Leeds Teaching Hospitals Research EthicsCommittee and all patients gave informedwritten consent.
PLASMA VOLUME AND HAEMATOLOGICALVARIABLES
Plasma volume was estimated by the Evans
blue dilution method.'9 Patients rested supinefor 30 minutes, then a venous catheterattached to a plastic tap was inserted into an
antecubital vein. After blood was withdrawnfor calibration of the spectrophotometer, 15mg of Evans blue dye (New World TradingCorporation) was injected and thoroughlywashed in with isotonic saline. Blood sampleswere withdrawn 10 min after injection andevery five minutes thereafter to 35 min. Thesamples were allowed to clot. Then they were
centrifuged and the concentration of dye inthe serum was determined using a spectropho-tometer (Pye Unicam, Cambridge) and com-
pared with known concentrations of dye madein undiluted serum from the same patient.The theoretical concentration of dye in theplasma at the time of injection was calculatedby reverse extrapolation of the log concentra-tion decay curve. The total quantity of bloodremoved from each patient was about 30 mland this was replaced by an equal volume ofsaline. The repeatability (95% tolerance lim-its) of the plasma volume estimates was ± 62ml. 19
The haematocrit was determined by themicrohaematocrit method from blood with-drawn immediately before the dye injection.20Blood volume was calculated as: plasma vol-ume/(1 - hematocrit). Mean corpuscular vol-ume was estimated from the initial bloodsample using a Coulter counter.
BARORECEPTOR SENSITIVITY
Subjects reclined supine and were fitted withfour standard electrocardiogram leads. After20 minutes' rest a neck chamber, constructedfrom thermoplastic,21 was fitted round the sub-ject's neck. The subject held his breath inexpiration and, after five seconds, a pressure of0, - 20, or - 40 mm Hg was applied for a fur-ther five seconds, on two occasions at eachpressure. Baroreflex sensitivity was taken as
the slope of the maximal prolongation of RRinterval of the electrocardiogram againstapplied chamber pressure. The repeatability ofthese estimates (95% tolerance limits) was± 0 5 ms/mm Hg (± 8-5% of mean values).
ORTHOSTATIC TOLERANCE
We used the method recently developed andevaluated in our laboratory.5 6 Subjects restedsupine for 20 minutes on a specially con-
structed tilt table with built-on lower bodychamber. The subject was then tilted head-upby 60° for 20 minutes after which, while they
Baseline data (mean (SE)) and responses to salt or placeboSalt (n = 10) Placebo (n = 10)
Variable Baseline Change Baseline Change
Weight (kg) 77-1 (5-5) +1-7 (0 3)* 67-4 (2 5) +0 7 (0 4)Plasma volume (ml) 2930 (193) +185 (43)**t 2727 (163) +97 (83)Blood volume (ml) 4912 (370) +291 (56)**t 4391 (302) +110 (108)Haematocrit 0 40 (0 01) -0-01 (0-005) 0 39 (0-01) -0 004 (0 005)Mean corpuscular volume (fl) 90 3 (0-8) +0-6 (0-3) 88-3 (1-2) +0-2 (0-5)Time to syncope (min) 20-6 (1-6) +8-7 (1-4)**t 18-0 (2-2) +4-0 (2 4)Baroreceptor sensitivity (ms/mm Hg) 5-9 (0 8) -2-0 (0 4)**t 6-0 (1-4) +0-6 (0 4)UrinaryNa (mmol/day) 128 (13) +95 (14)**t 129 (18) +21 (18)Values after treatment which were significantly different from those before treatment (Wilcoxon signed-rank test): *P < 0-02, **P< 0-002. Changes after salt treatment which were significantly different from corresponding changes after placebo (Mann-Whitney U test): tP < 0-01, t P < 0 005.
135
on 3 August 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Heart: first published as 10.1136/hrt.75.2.134 on 1 F
ebruary 1996. Dow
nloaded from

El-Sayed, Hainsworth
Salt Placebo3800
3600
3400
a) 3200E:f 3000
> 2800E 2600
a 2400
2200
+UX=e +~~~~~4
_--O-0Baseline study Second study
Salt
S~~ ~~~~~~~~~~~~~~~~*°
6500
6000
E0
0
Fo
5500
5000
4500
4000
3500
3000Baseline study Second study
Baseline study Second s
Placebo
t s"IBaseline study Second f
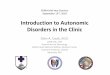
Figure 1 Plasma volume (top) and blood volume (bottom) in patients before and atreatment with salt or placebo. Open circles denote patients in whom the change in plvolume after treatment was greater than the 95% tolerance limits of the estimates.
Salt Placebo40
an
a)
0.+-
cn
E0
a)0.0
a)
E
Baseline study Second study
SaltcoI
EEE
.5
Co
a)
o~~~~~~~~~~~~~~~~~~C
0.
oa0
0
Baseline study Second study
14
12
10
8
6
4
2
Baseline study Second s
Placebo
Baseline study Second s
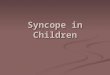
Figure 2 Values of orthostatic tolerance (time to presyncope) and baroreceptor sensitispatients before and after salt orplacebo treatment. Open and closed circles identify thepatients in whom there was and was not a significant increase in plasma volume as shefig 1. Note that in top plots, at the time to syncope of20 min, lower body negative preswas applied at 20 mm Hg and at 30 min it was increased to 40 mm Hg. This figureemphasises that all patients in whom plasma volume increased (both salt and placebo galso showed increases in orthostatic tolerance and decreases in baroreceptor sensitivity.
were still tilted, lower body suction wasapplied to below the iliac crests at - 20 andthen - 40 mm Hg for 10 minutes at each pres-sure. Blood pressure was recorded throughoutthe test from the brachial artery by an auto-matic sphygmomanometer (Infrasonde,Puritan-Bennett, California) and in a fingermaintained at heart level by a Finapres monitor(Ohmeda, Wisconsin). Heart rate was deter-mined from the electrocardiogram. The endpoint of the test and the measure of orthostatictolerance was the onset of imminent syncope,seen as a fall in systolic blood pressure to 80
study mm Hg or less. The repeatability of this test
(95% tolerance limits) is ± 2-5 min.
ResultsDOUBLE BLIND STUDYTwenty patients who had been shown to havepoor orthostatic tolerance6 were randomlyallocated to the salt and placebo groups (10 toeach). The ages and heights of the patients inthe salt and placebo groups (means (SD))were 41-2 (4.1) and 46-1 (5-8) years and171-4 (3-1) and 169-8 (2 8) cm. Other dataare listed in the table. There were no signifi-cant differences between the groups in any of
study the baseline data (Mann-Whitney U test, P >0 05).
fter At the second assessment the group taking~asma salt showed significant increases in body
weight, plasma and blood volumes, orthostatictolerance (assessed as the time to onset ofsyncope), and urinary sodium excretion (P <0-05, Wilcoxon signed-rank test). They alsoshowed a significant decrease in baroreceptorsensitivity. None of these variables changedsignificantly in the placebo group and all vari-ables in the salt group that changed signifi-cantly from the baseline data showed changes
------------ that were also significantly different fromthe corresponding changes in the placebogroup (Mann-Whitney test, P < 0 05). Theresponses are compared in the table.
Responses in individual patients wereregarded as significant if they changed beyondthe 95% tolerance limits of the repeatability of
i measurements. On this basis eight of the 10;tudy patients taking salt but only three of the 10
taking placebo showed significant increases inplasma and blood volumes; the other patientsshowed no significant responses (fig 1). All thepatients from both groups who showedincreases in plasma and blood volumes alsoshowed improved tolerance to the orthostaticstress test and decreases in baroreceptor sensi-tivity (fig 2). The patients in whom the plasmaand blood volumes did not change did notshow changes in either orthostatic tolerance orbaroreceptor sensitivity. The only differenceseen between patients who did not respond tosalt and those who did was that their baselinesalt excretion was higher. The mean 24 hour
;tudy urinary salt excretion in the responding.. . patients was 105 (range 66-152) mmol and in
v?tyzn those who failed to respond it was 219 andown in 226 mmol. The three patients in the placebo,sure group who had increases in plasma volume
7,ups) and orthostatic tolerance and decreases inbaroreceptor sensitivity all showed larger
4000
3800
= 3600E 3400a)E 32005 3000m 2800Ec 2600FL 2400
2200
7000
6500-
6000
a) 5500E- 5000
V 450000m 4000
3500
3000
Ra)
0.4-Qc
0
Q
CL
o0.
El=
m 12IEE 10
E> 6
C. 6cna)
0
&- 4Qa)
moam c
136
I
sm 0
41
C"", -lo01-1...
on 3 August 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Heart: first published as 10.1136/hrt.75.2.134 on 1 F
ebruary 1996. Dow
nloaded from

Salt supplement increases plasma volume and orthostatic tolerance in patients with unexplained syncope
140
120
.C
-a 100 -
I 6040
6 10 2b 3D 40
140
120 w . ;100_.,
E 80 -
X 60
40
20
0 10 20 30 4CTime to presyncope (minutes)
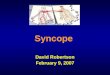
Figure 3 Time course of changes in heart rate and systolic and diastolic blood pressuresduring the orthostatic stress test in the 21 patients who received salt. Results (means(SEM)) are of tests before (-) and after (O) treatment. HUT, head up tilt, LBNP,lower body negative pressure.
increases in urinary sodium excretion at thesecond studies than were seen in the placebopatients who did not show changes (+115,+83, and +39 compared with a range of-36-+7 mmol/24 h).
OPEN STUDYEleven patients were openly given sodiumchloride tablets (slow sodium (Ciba) 120mmol/day) and were studied before and aftereight weeks of treatment as in the double blindstudy. There was no significant difference inany of the baseline values in comparison witheither group of the double blind study.Of the 1 1 patients openly receiving salt,
seven showed increases in plasma and bloodvolumes. These patients also showedincreased orthostatic tolerance and decreasedbaroreceptor sensitivity. As in the double blindstudy, the only difference in the patients whodid not respond to salt was that their baselinesodium excretion was high (192-262 mmol/24 h compared with 45-166 mmol/24 hour inpatients who did respond).
RESPONSES OF BLOOD PRESSURE AND HEARTRATESalt administration had no significant effect onthe supine values of blood pressure or heartrate in either of the two groups of patients whowere given salt. The mean values and SD inthe 21 patients given salt, before and after 8weeks of treatment were systolic pressure110-6(106) and 113-1 (9-5)mmHg, dias-tolic pressure 60-8 (9 7) and 61-5 (7 5) mmHg, heart rate 63-4 (11-8) and 63-7 (9 6)beats/min. Values of blood pressures in thehead-up tilt position were significantly (P <0-01) higher after salt administration but wereunchanged by placebo. Figure 3 shows the val-ues of heart rate and blood pressure through-out the test, before and after saltadministration.
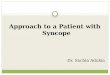
RELATIONS BETWEEN VARIABLESFigure 4 shows the relations between thechanges in orthostatic tolerance and thechange in baroreceptor sensitivity, with thechange in plasma volume. This figure, whichpresents data from all groups of patientsincluding the placebo group shows that allpatients in whom plasma volume increased byover 90 ml had significant increases in ortho-static tolerance and significant decreases inbaroreceptor sensitivity. Only one of the 13patients in whom plasma volume changed byless than 90 ml showed an increase in ortho-static tolerance and a decrease in baroreceptorsensitivity.
Figure 5 shows the influence of the baselinesalt excretion on the responses of plasma vol-ume and orthostatic tolerance in the 21patients given salt. The patients in whom thebaseline excretion was less than 170 mmol/24 hall showed increases in plasma volume andorthostatic tolerance. Those excreting morethan 190 mmol/day did not show significantincreases.
SYMPTOMATIC EFFECTSMost of the patients who took the salt capsulesin the double blind study initially experiencedsome nausea. In all but one this persisted forless than two weeks, and in no subject did itnecessitate withdrawal from the trial. Nopatient experienced any problems in taking theslow release sodium chloride tablets that wereused in the open study. All patients, from bothstudies in whom increases in plasma volumeand orthostatic tolerance were observed,including the three patients taking placebowho also showed changes, claimed to beentirely free from symptoms at the time of thesecond study. On the other hand, all thepatients in whom the test results wereunchanged claimed to be unchanged sympto-matically.
DiscussionThe principal finding from this study was thatadministration of salt supplements to patientssuffering from attacks of unexplained syncopesignificantly increased plasma and bloodvolumes, improved orthostatic tolerance,
137
on 3 August 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Heart: first published as 10.1136/hrt.75.2.134 on 1 F
ebruary 1996. Dow
nloaded from

El-Sayed, Hainsworth
30 To reduce the likelihood of patients chang-ing their diets spontaneously, we were careful
0 ~~~~~~~~~~~notto mention salt to any of our patients and25 ~~~~~~~~~~~~~~~~~referred to the treatment only as a "mineral
dietary supplement". The lack of dietary con-
20 ~~~~~~~~~~~~~~~~~trolin these patients is clearly a limitation to
20-
the study. However, our purpose was not tomake a detailed study of sodium balance, but
15-rather to determine whether a large dietary saltsupplement on top of the normal intake couldincrease the plasma and blood volumes and
10 improve orthostatic tolerance. The fact thatothree patients spontaneously increased salt
intake and that this was accompanied byp- increases in the blood volume and orthostatic
.-............................ di"'l""'ll'll"I'l""'ll,,'l""'ll""Itolerance adds further support to our conclu-0 _ tMD t e nsions.
the results showed that six (30%) of thepatients taking salt did not show any signifi-
-200-100 0upemn1onseso0.The lack of response was-200-1000100 200 300 400 500 600 700 800 900related to their initial salt intake as reflected inthe 24 hour urinary excretion. Those patients
2 - who already took a large quantity of salt intheir diets did not show increases in volume to
5_, in~~~~~~~~~~~~~uthkersl loadigMayothettiwa acopatient who
0 o0 El p did show good responses volunteered that they
..................[P :......... 0
ehad avoided salt withl their meals and often0 also in cooking. The relation that we observed
-2 0 between salt and plasma volume is actuallyo0 entirely compatible with the results of earlier
thsalt balance studies x that showed that low24 - co dietary sodium was associated with low extra-
cellular fluid volumes and that after anincrease in sodium intake there was someretention of salt and water before a new bal-ance was achieved when the input wasexcreted. The relation between input and vol-ume change, however, is not linear and at highsalt loads little extra volume is retained.7l24These observations explain our findings that
iI salt loading hadaneffectonlyonrelativelysalt
41 - * depetary indivium als.ascae ihlweta
-200 -100 0 100 200 300 400 500 600 700 800 90 deltdiivuasceBlood volume was calculated from plasma
Change of plasma volume (ml) volume using the haematocrit. There was nokure 4 Data from all patients showing the relations between the changes in plasma significant change in the haematocrit in theseume and the changes in orthostatic tolerance (top) and the changes in plasma volume nts aftereitaid the changes in baroreceptor sensitivity (BRS) (bottom). Closed circles are from the ptegtweso attetet
-~~ ~~~ ~o theeedopensaltio betweenanpusqurefimol-plce
-Uble blind salt group, open circles fr which implies that the red cell volume mustup. Note that changes in plasma volume of over 90 ml, in all groups ofpatients, are also have increased. Reticulocytes werevariably associated with increases in orthostatic tolerance and decreases in barorecepwr counted before and after treatment to test for-?sitivity haemopoiesis and, though some patients
showed increases, overall the change was notand decreased baroreceptor sensitivity, significant. This may have been because theImprovements occurred in eight out of 10 haemopoiesis was almost complete after eightpatients given salt and three out of 10 given weeks and also because reticulocytosis is saidplacebo in the double blind study and seven to occur in burstS25 and we may have missedout of1t1 given salt openly. Overall, in the 21 the peaks in many patients.patients given salt, 70% imnproved, whereas in The striking and consistent findings fromthose taking placebo 30% improved, this work were the associations between theInterestingly, the patient who showed the responses of plasma and blood volumes andlargest change in the entire study was actually the changes in both orthostatic tolerance andone who was given placebo. However, it tran- baroreceptor sensitivity. These associationsspired that this patient had changed her diet were seen in all groups of patients includingspontaneously and had had a large increase in the three patients taking placebo who showedbody weight as well as in plasma and blood increases in their volumes. This finding isvolumes. She, and the other two patients in entirely compatible with our recent reportwhom plasma volume increased on placebo, showing a highly significant positive correla-also showed increases in urinary sodium excre- tion in a large group of patients betweention at the second assessment and this indi- orthostatic tolerance and plasma volume and acates that all three had increased their salt negative correlation with baroreceptor sensi-intakes. tivity.'6
c
E0)UC
-
0
0-c
0
0
0
0)C
0)
0
C
Cu
-CC-
Filvoandoigrziseseh
138
on 3 August 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Heart: first published as 10.1136/hrt.75.2.134 on 1 F
ebruary 1996. Dow
nloaded from

Salt supplement increases plasma volume and orthostatic tolerance in patients with unexplained syncope
600
500
E 400
a)
E
300
0
coE 200
0Q
100
a)cm
c
0
-100
0
0
0
*
0 0
0
0
25 50 75 100
30r
c
EC
4L-a)
o0
a)
C.2
0
0
0)
%-C0
25
0
125 150 175 2
0
20;
150
*e
0
lo k-
5
0
525
0 0
0
50 75
0 0
101~~~~~~~~~
100 125 150 175 2
Baseline excretion (mmol/24
Figure 5 Relation between the pretreatment 24 hour urinary exresponse ofplasma volume (top) and orthostatic tolerance (bottoClosed circles give data from the double blind salt group andopelstudy group. Note that only patients in whom the initial salt exc?mmol/24 hours showed significant improvement after salt admin
The effect of plasma v
tolerance is not unexpeorthostasis is effectively atory volume due partlyand partly to capillaryeven with just upright tilcause a loss of about 15°/c15 minutes.26 It is therethat, if it is possible to e,plasma volume, this s:increase in his orthostatthe first report of changand orthostatic toleranceing of attacks of synccresults are consistent wthat, in normal subjectsinactivity there were dec:ume and this was associaorthostatic tolerance.27 28
The negative associations between thechanges in baroreceptor sensitivity and plasmavolume and orthostatic tolerance are harder tounderstand. It must first be emphasised that,in this study, baroreceptor sensitivity refersonly to the prolongation of cardiac interval inresponse to carotid sinus distension. Theimportant factor in resisting orthostatichypotension is really the increase in vascularresistance to baroreceptor unloading and thiswas not actually studied. Nevertheless, theseresults are quite compatible with our earlier
-- .................--- work showing negative correlations in a differ-0 ent group of subjects between baroreceptor
sensitivity and bothplasma volume and ortho-static tolerance.16 Furthermore there havebeen some studies in animals2930 which have
0 shown similar associations. Clearly, muchmore work is needed to establish the role of
!00225 250 275 the baroreceptor reflex in guarding against!00 225 250 275 orthostatic hypotension.
Although this study has shown thatincreased salt intake is associated withincreases in plasma volume and orthostatictolerance, this does not prove that theincreased orthostatic tolerance is necessarilythe result of the expanded plasma volume.Syncope occurs when vasoconstrictionabruptly fails,3" and it is conceivable that saltloading may alter reflex activity in some waywhich has the effect of delaying the onset ofsympathetic inhibition. Such an effect mightbe related to the observed changes in barore-flex sensitivity.
In assessing patients, with unexplained syn-cope, we feel that objective measurements, asmade in this study, are more reliable than sub-jective assessments. Clearly, relief of the
0* patients' symptoms is the primary concern and0 0 0 all of our patients who responded to salt
---- ----- ---- claimed to be improved symptomatically.II I I However, postural syncope is sporadic. In this
200 225 250 275 study the median number of attacks was three
h) over a median period of 12 months. Thismeans that, for subjective changes to be reli-
mcretion ofsodiumandthe able, a larger and longer study would betm) to salt administration.circles from the open needed.
retion was less than 170 We believe that the results of this study havetistration important implications for the management of
patients with unexplained syncope. It isimportant to emphasise again that the patients
,olume on orthostatic studied for this report were apparently healthy.,cted. The stress in They had no evidence of cardiovascular, neu-decrease in circula- rological, or renal disease and, apart from
to venous distension occasional attacks of syncope or near syncope,transudation which, were indistinguishable from the rest of the
Iting or standing, can population. In managing these patients, we
Dof plasma volume in advocate first excluding all known organic-fore to be expected causes of syncope. Then the patient's urinaryKpand an individual's excretion of sodium and his tolerance to
,hould result in an orthostatic stress should be determined and,ic tolerance. This is unless the sodium excretion is high (> 170;es in plasma volume mmol/day), oral salt administration should bein patients complain- given. The advantages of this simple treatment)pe. However, these are, firstly, that it is effective in people secretingAith previous reports low levels of salt and secondly, it is safe; wefollowing prolonged did not observe any adverse reactions. There
:reases in plasma vol- was even no effect on supine blood pressureted with decreases in although it would be advisable, particularly in
elderly subjects, to review patients at intervals
139
on 3 August 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Heart: first published as 10.1136/hrt.75.2.134 on 1 F
ebruary 1996. Dow
nloaded from

El-Sayed, Hainsworth
to ensure that supine blood pressure does notsubsequently increase. We do not yet knowwhether it is necessary to give as much as 120mmol of salt per day. However, until we knowotherwise it is reasonable to start with thisdose and possibly to reduce it later to a lowermaintenance level.This work was supported by the British Heart Foundation.
1 Day SC, Cook EF, Funchenstein H, Goldman L.Evaluation and outcome of emergency room patientswith transient loss of consciousness. Am J Med1982;73:15-23.
2 Wahbha MMAE, Morley CA, Al-Shamma YMH,Hainsworth R. Cardiovascular reflex responses inpatients with unexplained syncope. Clin Sci 1989;77:547-53.
3 Waxman MB, Yao L, Cameron DA, Wald RW, RosemanJ. Isoproterenol induction of vasodepressor-type reactionin vasodepressor-prone persons. Am J Cardiol 1989;63:58-65.
4 Fitzpatrick AP, Theodorakis G, Vardas P, Sutton R.Methodology of head-up tilt testing in patients withunexplained syncope. JAm Coll Cardiol 1991;17:125-30.
5 El-Bedawi KM, Hainsworth R. Combined head-up tilt andlower body suction: a test of orthostatic tolerance. ClinAuton Res 1994;4:41-7.
6 Hainsworth R, El-Bedawi KM. Orthostatic tolerance inpatients with unexplained syncope. Clin Auton Res1994;4:239-44.
7 El-Bedawi KM, Hainsworth R. Cardiac pacing does notimprove patients with vasovagal syncope. Clin Auton Res1994;4:233-37.
8 Goldenberg IF, Almquist A, Dunbar DN, Milstein S,Pritzker MR, Benditt DG. Prevention of neurally-medi-ated syncope by selective f,-adrenoreceptor blockade.Circulation 1987;76 Suppl IV:133.
9 Grubb BP, Temesy-Armos P, Hahn H, Elliot L. Utility ofupright tilt table testing in evaluation and management ofsyncope of unknown origin. AmJMed 1991;90:6-10.
10 Asso A, Milstein S, Dunnigan A, Remole S, Bailin S,Benditt DG. Prognostic significance of parenteral meto-prolol during head-up tilt-table testing: follow-up after 3years. Circulation 1991;84 Suppl II:409P.
11 Chan WL, Kong CW, Chang MS, Chiang BN. Exacer-bation of vasodepressor syncope by beta-adrenergicblockade (letter). N Engl Med 1991 ;324: 1219-20.
12 Frietas J, Puig J, Campos J, Garcia JM, Cunha DL,Carvalho MJ, et al. Malignant vasovagal syncope: a caseof prolonged asystole induced by "tilt" test and aggra-vated by therapy with beta-blockers (a clinical case anddiagnostic, physiopathologic and therapeutic review).Rev Portug Cardiol 1993;12:745-51.
13 Rashtian MY, Bhandari AK. Worsening of neurocardio-genic syncope by beta-blockers. Ann Intern Med 1993;119:955-6.
14 Sneddon JF, Camm AJ. Vasovagal syncope: classification,investigation and treatment. Br J Hosp Med 1993;49:329-34.
15 Edmonds ME, Watkins PJ. Clinical presentation of dia-betic autonomic failure. In: Bannister R, Mathias CJ,eds. Autonomic failure. A textbook of clinical disorders of theautonomic nervous system. Oxford: Oxford UniversityPress, 1992:698-720.
16 El-Sayed H, Hainsworth R. Relationship between plasmavolume, carotid baroreceptor sensitivity and orthostatictolerance. Clin Sci 1995;88:463-70.
17 Gupta BN, Linden RJ, Mary DASG, Weatherill D. Theinfluence of high and low sodium intake on blood volumein dogs. QJExp Physiol 1981;66:117-28.
18 Brown WI, Brown FK, Krishan I. Exchangeable sodiumand blood volume in normotensive and hypertensivehumans on high and low sodium intake. Circulation1971;43:508-19.
19 El-Sayed H, Goodall S, Hainsworth R. Reevaluation ofEvans blue dye dilution method of measurement ofplasma volume. Clin Lab Haematol 1995;17: 189-94.
20 International Committee for Standardization in Haem-atology. Standard techniques for the measurement of redcell and plasma volume: panel on diagnostic applicationof radioisotopes in haematology. Br _' Haematol 1973;25:801-14.
21 Al-Timman JKA, Hainsworth R, Vukasovic JL. A modifiedneck chamber for the study of carotid baroreceptors inhumans. Y Physiol 1988;399:14P.
22 Lyons RH, Jacobson SD, Avery NL. Increases in theplasma volume following the administration of sodiumsalts. Am J Med Sci 1944;208: 148-54.
23 Romero JC, Staneloni RJ, Dufau JL, Dohmen R, Binia A,Kliman B, et al. Changes in fluid compartments, renalhaemodynamics, plasma renin and aldosterone secretioninduced by low sodium intake. Metabolism 1968;17:10-9.
24 O'Connor WJ. Normal renal function. London: CroomHelm, 1982;299-328.
25 Lange RD, Jones JB. Erythropoiesis in dogs and humanswith cyclic haemotapoiesis. In: Dunn CDR, ed. Currentconcepts in erythropoiesis. Chichester: John Wiley 143-65.
26 Hagan RD, Diaz FJ, Horvath SM. Plasma volume changeswith movement to supine and standing position. J ApplPhysiol 1978;45:414-8.
27 Bungo MW, Charles JB, Johnson PC. Cardiovasculardeconditioning during spaceflight and the use of saline asa counter measure to orthostatic intolerance. Aviat SpaceEnviron Med 1985;56:985-90.
28 Ludwig D, Convertino VA. Predicting orthostatic intoler-ance: physics or physiology? Aviat Space Environ Med1994;65:404-1 1.
29 Vatner SF, Boettcher DH, Hayndrickx GR, McRitchie RJ.Reduced baroreflex sensitivity with volume loading inconscious dogs. Circ Res 1975;37:236-42.
30 Billman GE, Dickey DT, Teho KK, Stone HL. Effects ofcentral venous blood volume shifts on arterial baroreflexcontrol of heart rate. AmY Physiol 1982;241:H571-5.
31 Barcroft H, Edholm OG. On the vasodilatation in humanskeletal muscle during post-haemorrhagic fainting. JPhysiol 1945;104:161-75.
140
on 3 August 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Heart: first published as 10.1136/hrt.75.2.134 on 1 F
ebruary 1996. Dow
nloaded from