Embed Size (px)
Citation preview

Dr AMIT KUMAR MALLIK
DEPT. OF PHYSICAL MEDICINE AND REHABILITATION
RIMS,IMPHAL
ORTHOSTATIC HYPOTENSION

Definition
BLOOD PRESSURE
The pressure exerted by flowing column of blood on arterial wall.
Normal BP- Systolic 100-140 mm Hg
Diastolic 60-90 mm Hg

Orthostatic hypotension
• Decrease in systolic BP≥20 mm Hg or decrease in diastolic BP≥10 mm Hg within 3 minutes of standing when compared with BP from sitting or supine position
or
• Similar drop in BP within 3 minutes in a head up position on tilt table test at angle ≥60°

Normal mechanism of BP regulation
There are two basic mechanisms for regulating blood pressure:
(1) short-term mechanisms
(2) long-term mechanisms
Blood Pressure = cardiac output x peripheral resistance

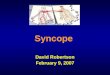
Location of Baroreceptor and Chemoreceptor

Control of Blood pressure
I. Nervous system
II. Chemoreceptor

I. Nervous System
• Control BP by changing blood distribution in the body and by changing blood vessel diameter.
• Sympathetic & Parasympathetic activity
• The vasomotor center – medulla
It sends efferent motor fibers that innervate smooth muscle of blood vessels

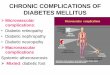
Regulation of Rising Blood Pressure

Baroreceptors
• The best known of nervous mechanisms for arterial pressure control(baroreceptor reflex)
• Baroreceptor are stretch receptors found in the carotid sinus ,aortic sinus
• Respond more to a rapidly changing pressure than stationary

Baroreceptors

Effect of Baroreceptors
EFFECT
VASODILATATION OF THE VEINS AND ARTERIOLES
DECREASED HEART RATE AND STRENGTH OF HEART
CONTRACTION
Therefore, excitation of baroreceptors by high pressure in the arteries reflexly causes arterial pressure to decrease (as decrease in PR and CO)

Increased Parasympathetic Activity
• Reduction of heart rate
• Lower cardiac output
• Lower blood pressure

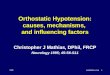
Regulation of Falling Blood PressureBaroreceptors inhibited
Decreased impulses to the brain
Decreased parasympathetic activity, increased sympathetic activity
Effects
Heartincreased heart rate and
increased contractility
Vesselsincreased vasoconstriction
Adrenal glandrelease of epinephrine and
norepinephrine which enhance heart rate
Contractility and vasoconstriction
Increased blood pressure


II. Chemoreceptor

Chemoreceptor
• Chemosensitive cells that respond to changes in pCO2 and pO2 and pH levels (Hydrogen ion).
pCO2 pO2 and pH
Stimulation of vasomotor center
CO HR vasoconstriction
BP (speeding return of blood to the heart and lungs)

Chemoreceptor

• Any interruption in the body's natural process of counteracting low blood pressure

Causes of Postural HypotensionNeurogenic causes
Primary causes-
Autonomic failure due to idiopathic central and peripheral neurodegenerative diseases—the “synucleinopathies”
• Parkinson’s disease
• Lewy body dementia
• Pure autonomic failure
• Multiple system atrophy (Shy-Drager syndrome)

Secondary causes1.Spinal cord injury
2.Secondary autonomic failure • Diabetes
• Hereditary amyloidosis (familial amyloid polyneuropathy)
• Primary amyloidosis (AL amyloidosis; immunoglobulin light chain associated)

• Idiopathic immune-mediated autonomic neuropathy
• Autoimmune autonomic ganglionopathy
• HIV neuropathy

Non-neurogenic Causes of Orthostatic Hypotension
• Age related
Cardiac pump failure
• Myocardial infarction
• Myocarditis
• Constrictive pericarditis
• Aortic stenosis
• Tachy-arrhythmias
• Brady-arrhythmias

Reduced intravascular volume
• Dehydration
• Diarrhea, emesis
• Hemorrhage
• Burns

Metabolic
• Adrenocortical insufficiency
• Hypo-aldosteronism
• Pheo-chromocytoma
• Severe potassium depletion

Venous pooling• Postprandial dilation of splanchnic vessel beds
• Vigorous exercise with dilation of skeletal vessel beds
• Heat: hot environment, hot showers and baths, fever
• Prolonged recumbency or standing

Medications
• Antihypertensives
• Diuretics
• Vasodilators: nitrates, hydralazine
• Alpha- and beta-blocking agents
• CNS sedatives: barbiturates,opiates
• Tricyclic antidepressants
• Phenothiazines

Symptoms
Characteristic symptoms are
• Light-headedness
• Dizziness
• Presyncope (near-faintness)
However, symptoms may be absent or nonspecific like
• Generalized weakness
• Fatigue
• Cognitive slowing
• Headache.

• Visual blurring
• Neck pain—typically in
-suboccipital
-posterior cervical
-shoulder region
( “coat-
hanger headache”)

• Patients may report orthostatic dyspnea
• Symptoms may be exacerbated by exertion, prolonged standing, increased ambient temperature, or meals
• Syncope is usually preceded by warning symptoms, but may occur suddenly, suggesting the possibility of a seizure or cardiac cause

Percentage wise symptoms
• Lightheadedness (dizziness) 88%• Weakness or tiredness 72%• Cognitive difficulty (thinking/concentrating) 47%• Blurred vision 47%• Tremulousness 38%• Vertigo 37%• Pallor 31%• Anxiety 29%• Palpitations 26%• Clammy feeling 19%• Nausea 18%

Diagnosis
• By taking BP in supine and standing
• By comparing both BP

Management
Non pharmacological
• Patient education: mechanisms and stressors of OH
• Compression garments

• The head of the bed of a patient with orthostatic hypotension should be elevated by 10 to 20 degrees or 4 inches (10 cm)

• Move legs while standing
• Get up slowly
• Avoid bending at waist
• FES
• Exercise-Calf muscle exercise, when getting out of bed, sit on edge of bed for a minute before standing

• High-salt diet (1g/d) QID
• High-fluid intake (2 l/d)
• Learn physical counter-maneuvers
• Correct anemia

Medicines(pharmacological)
• Fludrocortisone
• L-dopa-to treat hypotension a/w Parkinson ds.
• Midodrine or Ephedrine
• Erythropoitin
• Pyridostigmine


Thank You