Embed Size (px)
Citation preview

Annals of the Rheumatic Diseases 1991; 50: 8-13
SCIENTIFIC PAPERS
Study of 500 patients with limb joint osteoarthritis.I. Analysis by age, sex, and distribution ofsymptomatic joint sites
Janet Cushnaghan, Paul Dieppe
AbstractFive hundred subjects with symptomatic limbjoint osteoarthritis, who had been referred toa rheumatologist, were enrolled into a con-tinuing study. They comprised 342 women(mean age 65.3) and 158 men (mean age 59.7),with a mean symptom duration of 15-4 yearsat entry. Only 31 patients (6%) had sympto-matic osteoarthritis of one joint alone; how-ever, in a further 205 (41%) the disease waslimited to one site. One hundred and eightytwo (36-4%) had two sites affected and 82(16-4%) three or more sites of symptomaticosteoarthritis. Of 847 affected joints the mostcommonly involved were 349 (41-2%) knees,254 (30%) hands, and 161 (19%) hips. Hipdisease stood out as a separate entity, oftenoccurring alone, and having a stronger malepreponderance and different associationsthan osteoarthritis at other joint sites. Kneeand hand disease were significantly associatedin women. Obesity, hypertension, andHeberden's nodes were common. Thenumber of sites affected, as well as thedistribution, was strongly related to age aswell as sex, suggesting that polyarticularosteoarthritis arises from slow acquisition ofnew joint sites in a non-random distribution.'Generalised' osteoarthritis did not emerge asa distinct entity.
Rheumatology Unit,Bristol Royal Inirmar,
Bristol BS2 8HWJ CushnaghanP DieppeCorrespondence to:Dr JCnaghan.
Accepted for publication29 January 1990
Osteoarthritis is the commonest form of jointdisease.' It is related to age, and an increasinglyimportant health problem in an older, generallyfitter, more health conscious society. Excludingthe spine, the three joint sites most oftenaffected are the hip, knee, and hand.2
Surprisingly little is known about osteo-arthritis, which remains difficult to define,characterise, or assess. Epidemiological studiesimplicate six main risk factors: age, inheritance,obesity, trauma, abnormal biomechanics, andalterations in joint shape.3 4 Probably, however,differences exist in the relative importance ofthese factors in the two sexes, and at differentjoint sites.5 Clinical studies of osteoarthritishave largely been concerned with a single jointsite, such as hip or knee disease, generallydivided into two main categories-primary (noobvious cause) or secondary (an apparentpredisposing factor identified). The cause ofosteoarthritis is clearly multifactorial, however,and the distinction between primary and
secondary disease is blurred.6 Most of theavailable clinical and epidemiological data arecross sectional, little being known about thenatural history of this condition.
In 1985 we embarked on a prospective studyof symptomatic osteoarthritis of the limb joints.This paper reports on cross-sectional dataobtained at the time of patient recruitment,analysed by age, sex, and the distribution ofsymptomatic joint sites.
Patients and methodsFive hundred consecutive patients with limbjoint osteoarthritis were recruited into the study.All had been referred to the rheumatology unitof the Bristol Royal Infirmary by local generalpractitioners or consultant colleagues. Thediagnosis of osteoarthritis was made by one ofthe authors (PD) before study entry and wasbased on a combination of typical radiographicfeatures (including joint space narrowing) plussymptoms and signs compatible with osteo-arthritis (including pain related to use) in atleast one limb joint. In all cases the osteoarthritiswas considered to be the primary rheumato-logical problem, though those with other dis-orders were not excluded.One observer (JC) interviewed all the patients
according to a set protocol. Historical detailsincluded the age, sex, and occupation of allpatients, the duration of joint symptoms andsymptomatic joint sites at the time of theinterview. The joint(s) considered by thepatient to be the major or worst sites werenoted. Details of symptoms (pain, stiffness, anddisability) were collected and the Steinbrockerfunctional class recorded. Any previous traumaor surgery which might have predisposed toosteoarthritis, as well as the presence of anyintercurrent disease, was noted. Current drugsused and any treatment, including use of aidsand appliances, were recorded.The same observer also examined all patients.
Their height and weight were recorded and thebody mass index (wt(kg)/ht(m2)) derived as ameasure of obesity. The blood pressure wasmeasured, and patients who were either receiv-ing drugs for hypertension or had a restingdiastolic blood pressure of >90 mmHg, or both,were recorded as hypertensive. The distal inter-phalangeal joints were palpated and nodesrecorded as present or absent. A full examinationof all limb joints was carried out; joint disease
8

9Study of500 paients with Imbjoitostrts
was noted as present or absent on a joint chart,and more detailed information recorded fromthe three principal sites-the hips (range ofmovement), knee (swelling, range ofmovement,instability, and tenderness), and hands (swell-ing, deformity, and tenderness of each joint).
Blood was taken for determination of rheu-matoid factor, full blood count, viscosity, and Creactive protein at the time of examination.
Further aliquots of serum were stored at - 70°C,and synovial fluid was obtained from the kneejoints of some patients. Standard radiographswere taken of the knees (anteroposterior stand-ing and lateral views) and hands (posteroanterior)in all cases, as well as other symptomatic jointsites.
0)ICL
0..
Ez
Age (years)
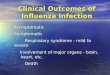
Figure I Age-sex dutributin ofaUpaients entered into the study.
Each case record was then reviewed by thetwo authors, with the radiographs available.Painful joint sites accompanied by typical radio-graphic changes of osteoarthritis-that is, bothjoint space narrowing and subchondral bonereaction in any part of the site, were coded asthe index joint sites. Data were only collectedfor limb joints-hips, knees, ankles, feet,shoulders, elbows, wrists, hands. Disease of thefirst metatarsophalangeal joint was not studiedbecause of the difficulty in establishing, record-ing, and interpreting the presence of halluxvalgus, halux rigidus, and other changes. Backdisease was not included in the analysis.
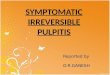
ResultsAGE, SEX, DISEASE DURATIONThe study group comprised 342 women and 158men aged 24 to 88, with a mean of 65 3 years forwomen and 59-7 for men. Figure 1 shows theage-sex distribution by decade, and illustratesthe peaks for men in the 55-64 age group andwomen in the 65-74 age group. Most patientsreported that symptoms had been present in theindex joint sites for a long time before referral;the mean symptom duration was 15-4 years witha range of 0-65 years. Figure 2 shows therelation between age at examination and diseaseduration. It suggests that older patients had thelongest disease duration. In many cases, how-ever, it was difficult to establish the time ofonset of symptoms in the joint sites of interest,and true symptomatic disease duration wasoften uncertain.
50 +
40 + ++±
++-0+ ±+±±4 +
±+*w I 1 E.~20 -t 1
10
20 ~40 60' 80 lOC
Age at entry to study (years)Fgure 2 Disease duration plotted against age ofentry, shoing a weak correlation betweensymptom duratwn and increasing age.
JOINT DISTRIBUTIONA total of847 painful, radiographically abnormaljoint sites were recorded, of which 349 (41-2%)were knees, 254 (30%) hands, and 161 (19%)hips. The other 83 (9-8%) symptomatic sitesaffected included, in order of frequency, ankles/subtalar joints, shoulders, elbows, wrists, andmidtarsal joints.Two hundred and thirty six (47-2%) patients
had only one symptomatic joint site, of whomonly 31 (6%) had unilateral (monoarticular)disease. Single site disease was commoner in
men (97/158 (61%)) than in women (139/342(40 6%)) and decreased in prevalence withincreasing age, as shown in table 1 and figs 3Aand B. The chief sites of lone osteoarthritiswere, in order of prevalence, the knee, hand,and hip. Hand disease showed a strong femalepreponderance (4-2: 1) and hip disease a malebias (2-4: 1), whereas knee disease had a roughlyequal sex distribution (F:M 1-3:1). Only 17patients had other joints affected as the only
Tabk I Number of sites affected by ostearthitis in men and women at different agesWomen MenTotal -44 45-54 55-4 65-74 275 Total <44 45-54 55-64 65-74 275No (%) No (%)
Total numbers 342 15 49 91 111 76 158 19 30 54 36 19
1 Joint siteunilateral j0(2-9) 2 4 2 2 0 21(13) 7 5 7 2 01 Joint site bilateral 129(38) 10 28 44 31 16 76(48) 10 17 27 11 112 jointsites 141(41) 3 12 37 56 33 41(26) 2 6 13 15 53 joint sites 49(14) 0 4 6 17 22 15 (9) 0 2 4 7 24+ Jont sites 13 (3 8) 0 1 2 5 5 5 (3) 0 0 3 1 1

Cushnaghan, Dieppe
0 40
a30
h 20nEz 10
Age of patients
.44 45-54 55-64 65-74Age of patients
>75
Ca)
Ez
.44 45-54 55-4 65-74 .75Age of patients
50-2 Joint sites, Men
40(- ) Knee/hand-o - Knee / hip
30 - Hip/hand
20-
10
O.44 45-54 5544 65-74
Age of patients
275
Figure 3 Number ofpatients with one or two majorjoint sites affected at different ages.
symptomatic sites; 11 were men, and the jointsaffected were ankles (eight), shoulders (five),elbows (two), wrists and midtarsal joints (oneeach).
Disease of joints at two different sites was
recorded in 182 patients (36-4%), of whom 141were women. This group was dominated bywomen with a combination of knee and handdisease (108 patients, 21-6% of all patients) (figs3C and D). Analysis of the correlations betweenosteoarthritis at the three major joint sites(knees, hands, hips) in this group showed a
statistically significant association between handand knee disease in women but no relationbetween hand and hip or knee and hip disease ineither sex or in the whole group (table 2). Sixtyfour patients (12-8%) had three symptomaticjoint sites, of whom 49 were women; only 13women and five men had four or more sitesaffected. Table 1 shows the strong correlationbetween increasing age, female sex, andincreasing numbers of affected joints.
Table 2women
Associations between two joint sites in men and
Women Men
Hip Hand Hip Hand
+Knee 7 108 (p<0 001) 9 15 (NS)-Knee 7 13 5 3
Knee Hand Knee Hand+Hip 7 7 (NS) 8 2 (NS)-Hip 121 114 25 16
p Values for x2 statistic for one degree of freedom with Yates'scorrection.
Table 3 Age, sex, and incidence of other affected sites inpatients with osoarthniis involving each of the major linbjoints
Joint site % Of total F:M rano Mean age % Occwrnngas only site
F M
Knees 41-2 1-3:1 62-6 59-8 39Hands 30-0 4-3:1 59-3 61-5 36Hips 19 0 0-4:1 54-3 51-3 58Ankles 4-4 0-8:1 57-7 51-4 38Shoulders 3-2 3:1 69-7 61-5 31Elbows 1-6 0-25:1 62-8 54-5 20Wrists 0-6 1:1 75-5 77-0 25
Table 3 shows the prevalence of disease ofeach major joint site together with the sex ratio,mean age of men and women with each siteaffected, and incidence of coexisting osteo-arthritis at other sites. The overall femalepreponderance of hand and shoulder diseasecontrasted with the male bias for hip and elbowdisease. The hip was clearly the earliest siteaffected in both sexes, whereas shoulder diseasein women was a later manifestation. Wristdisease was largely seen in elderly patients withchondrocalcinosis, but the number of peoplewith symptoms at this site was very small.
ASSOCIATIONSAssociations between any apparent predispos-ing causes, intercurrent rheumatic diseases,obesity, hypertension, Heberden's nodes, andthe patterns of osteoarthritis described weresought (table 4).An obvious predisposing cause was only
apparent in 46 cases-28 (18%) men and 18(5%) women. They included severe trauma,menisectomy, epiphysial dysplasia, and in-stability. 'Secondary' osteoarthritis was com-monest in men, younger patients, and thosewith one large joint site affected. It was recordedin 200/o of hips, 27-5% of knees and 37 5% ofthose with the less common sites (ankles,shoulders etc) as their only symptomatic joints.
Seventy two patients (14-4%) had some otherdisorder of the musculoskeletal system inaddition to their osteoarthritis. There was awide spectrum of such conditions, of which thecommonest was gout (12 men, 2-4%). In eachcase it was thought they were associated con-ditions rather than causes of the osteoarthritis,and they were commonest in the older patients.Eleven patients (2-2%) with definite or classicalrheumatoid arthritis (American RheumatismAssociation criteria7) were entered into thestudy. In each case the rheumatoid arthritis haddeveloped after the onset of symptomatic osteo-arthritis, and the latter was still considered to bethe principal problem.The most common extra-articular associations
were hypertension and obesity (table 4). Hyper-
2 joint sites, Women
-S
Ez
:50.
10
,0D
- -- .0-

11Study of500 patients with limb joint osteoarthritis
Table 4 Association betwveen apparent predisposing causes, intercurrent rheumatic diseases, obesity, hypertension, Heberden's nodes, and the patterns ofosteoarthritis
n Obvious Knee Erosions Heberden's Obesity Hypertension Steinbrockersecondary chondrocalciwosis () nodes (Q~-30)' %cause (% M% (%M% Class 1-2 Class 3-4
Total 500 9 18 5 48 13 37 66 31Total women 342 5 17 6 56 13 37 63 35
-<64 years 155 7 6 11 53 17 32 81 17>-65 years 187 4 26 3 59 10 42 48 50
Total men 158 18 22 1 30 15 37 72 23,<64 years 103 21 21 2 28 14 38 78 16>,65 years 55 11 24 0 33 16 36 62 34
One joint site:Knee 105 15 27 0 19 16 38 73 24Hip 37 19 5 0 5 22 22 73 27Hand 78 0 8 15 70 11 33 74 17Other 16 31 37 0 37 6 25 69 31
Two joint sites:Knee/hand 123 3 13 6 71 16 41 63 32Knee/hip 16 31 25 0 6 37 19 44 50Hip/hand 9 22 22 0 78 0 44 67 33
tension, as defined, was recorded in 128 women(37%) and 59 men (37%). There was noapparent association with the patterns of osteo-arthritis. Subjects with a body mass index of>25 were considered to be overweight, thoseover 30 obese. A total of 172 women (50%) and96 men (6O0%/) were overweight, of whom 52women and 26 men were obese (15 5%). Thisfeature was commoner in the younger womenrather than the older women (table 4). Thosewith obesity tended to have only one or two sitesaffected, the commonest joints being knees(17), hands (nine), hips (eight), knees+hands(21), and knees+hips (13). Six of 16 patients(37%) with the combination of hip and kneedisease had a body mass index of >30, and 71%were overweight. Those with lone hand diseasetended to have a lower than average incidence ofobesity (11-5%).
Heberden's nodes were found in 193 women(56%) and 47 men (30%/). There was noapparent association between this finding andage. Nodes were not uncommon in thosewithout symptomatic hand disease, occurring in28 of 158 patients (18%) with lone involvementof one large joint site. They were found in only5-5% of those with hip disease, 190/o of thosewith knee joint disease, and 37'5% of thosewith other symptomatic large joints.
INVESIGATIONSHaematological investigations were unremark-able. A slightly raised plasma viscosity wascommon, but the C reactive protein was abovethe upper limit of normal of 10 mg/l in only 50women (15%) and 23 men (15%). Thirty fivepatients had a rheumatoid factor titre of >1/40,including the 11I with known rheumatoidarthritis. Raised C reactive protein and rheuma-toid factor titres correlated with age, female sex,and the presence of an intercurrent inflam-matory disorder, but showed no correlationswith patterns of osteoarthritis.Two specifilc radiological features were
recorded as present or absent and related to theknown osteoarthritis: they were knee chondro-calcinosis and interphalangeal joint erosions.Erosions, defined as breaks in the cortex of
subchondral bone, were seen in the inter-phalangeal joints in only 24 cases (22 women,mean age 57'S years). Chondrocalcinosis waspresent in 57 women (17%) and 35 men (22%).It correlated with increasing age and thepresence of knee osteoarthritis; 28/105 (27%) ofthose with lone knee disease had chondro-calcinosis, compared with only 13/13 1 (10%)with isolated disease of other joint sites.
FUNCTIONThe Steinbrocker functional class was used as acrude measure of disability.8 As shown in table4 functional classes 3 or 4 were recorded mostoften in elderly women. As might be expected,poor function also correlated with lower limbdisease and multiple joint sites affected. Onehundred and fifty five (3 1%) of all patients werein functional classes 3 or 4, and a further 262(52-5%) were in functional class 2, giving someindication of the severity of osteoarthritis beingstudied. A total of 165 patients (33%) wererecorded as using aids and appliances, usually awalking aid. Three hundred and seventy four(74-8%) were taking non-steroidal anti-inflammatory drugs or analgesics, or both, fortheir osteoarthritis at the time of assessment.
DiscussionIt is widely recognised that osteoarthritis is themost important form ofjoint disease contributingto the overall health burden of the community.1There has been less clinical research intoosteoarthritis than into many other, much rarerforms of rheumatic disease, however. This maybe explained in part by the relative lack ofseverity of osteoarthritis in comparison withsystemic inflammatory arthropathies, andbecause a minority of patients with osteoarthritisare referred to specialist rheumatologists.9 As aresult we still lack definitive data on manysimple facets of osteoarthritis, such as itspatterns of joint distribution, possible diseasesubsets, and natural history. Two main subsetsare recognised, monoarticular secondary osteo-arthritis, resulting from congenital or acquired

12
abnormalities of joint shape, and generalised'nodal' osteoarthritis, characterised by poly-articular disease affecting the hand.10 Thevalidity of even these subsets is arguable,6 11however, and the definition, classification, anddiagnostic criteria of the disease also remaincontroversial. 12
This paper reports the cross-sectional dataobtained from 500 patients diagnosed as havingperipheral joint osteoarthritis in a hospital basedrheumatology unit. The purpose of this reportis to examine the hypothesis that subsets ofosteoarthritis can be defined by demographyand joint distribution, and to examine thevalidity of the concept of a generalised form ofosteoarthritis. To that end the associations andinterrelations of osteoarthritis at each of themajor peripheral joint sites have been recorded.The patient group is unlikely to be represen-
tative of osteoarthritis in the community. Thepatients were all referred to consultant rheuma-tologists in Bristol or Bath, and then channelledto the one local unit with a special interest in thedisease. They may well have more severeosteoarthritis, or be more demanding people,than most; they may exclude an importantgroup referred directly to orthopaedic surgeons.If a large number are examined, however, someexamples of most of the important manifesta-tions of the condition should be included.Furthermore, the age and sex distribution ofour patients is not inconsistent with that ofother hospital surveys,'3 and similar to that seenin community based studies of osteoarthritis,3suggesting that our patients are not entirelyunrepresentative of the problem as a whole. Anoverall female preponderance and a wide rangeof age of onset with a mean around the sixth orseventh decade has been described in otherstudies.4 5 The data reported here provide acomparison of patients of different age, sex, orjoint complaints. This was facilitated by carefuldata collection. Entry to the study was controlledby one of the authors (PD), and the historicaland examination data were all collected by theother (JC). As a result, any apparent differencesin associations between patient groups shouldbe of value, though the absolute numbers with aparticular feature cannot be regarded asmeaningful.
For the purposes of this study osteoarthritiswas diagnosed if the patient complained of painrelated to joint usage, if the radiographs of thatjoint(s) showed evidence of osteoarthritis (in-cluding joint space narrowing), and if there wasno other apparent cause of symptoms. In theabsence of established diagnostic criteria'2 thereare few alternatives. Spinal disease was excludedbecause of the difficulty in defining spinalosteoarthritis and of relating radiographs tosymptoms,'4 and the first metatarsophalangealjoint was omitted from the analysis for similarreasons. This limits the study and makes itdifficult to relate it to published data which, forexample, stress spinal disease in generalisedosteoarthritis. '5The data collected weredesignedto maximise information on the major joint sitessaid to be affected in osteoarthritis (knees,hands, and hips), and some of the main riskfactors and associations previously reported.3 4
It is apparent that the group as a whole hadsignificant disease, as shown by the high rates ofdrug use, dependence on aids and appliances,and the number of patients with a Steinbrockerindex of 3 or 4. Not surprisingly, age and lowerlimb disease correlated strongly with thegreater degrees of disability.The joint disease seen in our patients was
much as we expected, being dominated byknee, hand, and hip problems, in that order.Hip disease may well be underrepresented,because of the tendency among local prac-titioners to refer this condition directly tosurgeons. The interrelations between thesethree sites show a strong association betweenhand and knee disease, but not between hipsand hands, or hips and knees. The hip standsout as a site with quite different associations,being more likely to occur as a lone problem inyounger, non-obese men than disease at otherjoint sites. Elbow disease also emerged ashaving a male preponderance, as recentlydescribed elsewhere.'6 In contrast, problems atthe shoulder tended to occur in older women.The other strong trend to emerge is of moresites of disease, more severely affected, as ageadvances. The association of numbers of jointsites with age might be explained by slowaddition of new sites, as suggested in anotherstudy in a similar population,'7 or by oldersubjects having a greater predisposition toosteoarthritis at unusual sites. The prospectivedata on this group should help resolve thisfurther, but if, as seems likely, it is due to slowaddition of new sites, then it is important torecognise that the diagnosis of 'generalised'osteoarthritis would depend on the time point inthe disease evolution at which a particularpatient was seen. The absence of older men inthe group might be due to earlier death, or be anascertainment artefact-that is, we might nothave seen a representative selection of patientsas we recruited only patients referred to arheumatologist. Prospective data should showwhether osteoarthritis develops differently inmen and women with time.The disease associations included a signifi-
cant number with another rheumatic disease,which probably represents an ascertainmentartefact. In contrast, few had a clear cut 'cause'for their osteoarthritis. This low incidence of'secondary' osteoarthritis is at variance withsome studies, though patient series not domi-nated by hip osteoarthritis rarely report a highincidence of an obvious cause.'0 3 18 19 Ourdata support the idea that secondary osteo-arthritis is an uncommon form of the condition,principally seen in younger men with hip, knee,or ankle/subtalar disease related to abnormalitiesof joint shape or previous trauma. A combinationof hip and knee disease was unusual, but oftenassociated with a predisposing cause or obesity,or both, in our series. The high incidence ofsubjects with osteoarthritis who were over-weight or obese accords with other data3 4; thefindings that this was not associated with age orrelated to numbers of sites affected or disabilitysuggests that it is a genuine risk factor orassociation, and not a result of osteoarthritis.20Although we have no control data, the incidence
Cueshnaghan, Dieppe

Study of500 patents wih limbjoitosteoartkrits3
of obesity in our series is much higher than thatfound in a recent United Kingdom communitysurvey.21
Heberden's nodes are often used as amarker of so called generalised or nodal osteo-arthritis.1 22 Population surveys suggest, how-ever, that they become extremely common inolder women, with a far higher incidence thanthat of symptomatic osteoarthritis.23 In thisseries they were usually, but not always, seen inthose with hand disease. They were also com-monly present in those with osteoarthritic kneesand other symptomatic joint sites (except thehips and ankles) who did not have handproblems. This strengthens the data indicatingthat hip osteoarthritis behaves differently fromthat of other sites, but it undermines theconcept of a distinct subset of nodal osteo-arthritis. The high incidence of multisite diseaseassociated with being overweight, hypertensive,and having Heberden's nodes suggests thatmost subjects with osteoarthritis have a back-ground systemic predisposition to their disease,resulting in localisation to a limited number ofjoint sites which is associated with age. Age wasalso the main association of chondrocalcinosisand abnormalities of blood tests, none of whichshowed any clear relation with disease at aparticular joint site(s). Previous reports ofdistinctive forms of inflammatory, erosive, orgeneralised osteoarthritis may reflect diseaseseverity rather than specific subsets.24The most significant finding is the strong
statistical association between knee and handdisease in women. This indicates that thedistribution of osteoarthritis, although depen-dent on age and sex, is not random. It is alsostrong evidence for a major generalised orsystemic component in the aetiology of manycases of osteoarthritis.
This work is supported by the Arthritis and RheumnatismCouncil. We would like to thank Mrs Sara Browning fororganisational and secretarial help, and consultant colleagues forallowing us to study their patients.
1 Lawrence R C, HochbergM C, Kelsey J L, et al. Estimates ofthe prevalence of selected arthritic and musculoskeletaldiseases in the United States. J Rhewnatol 1989; 16:427-41.
2 Wood P H N, Badley E M. Epidemiology of individualrheumatic disorders. In: Scott J T, ed. Copeman's textbookof the rheumatic disases. 6th ed. Edinburgh and London:Churchill Livingstone, 1986: 59-142.
3 Felson D T. Epidemiology of hip and knee osteoarthritis.Epidmiol Rev 1988; 10: 1-28.
4 Scott J C, Hochberg M C. Osteoarthritis: 1. Epidemiology.Maryland State Medical Journal 1984; 33: 712-6.
5 PeyronJ G. Theepidemiologyofosteoarthritis. In: MoskowitzR W, Howell D S, Goldberg V M, Mankin H S, eds.Osteoarthritis: diagnosis and management. Saunders: Phila-delphia and London, 1984: 9-27.
6 Doherty M, Watt I, Dieppe P. Influence of primarygeneraiised osteoarthitis on development of secondaryosteoarthitis. Lancet 1983; ii: 8-11.
7 Arnett F C, Edworthy S M, Bloch D A, et al. The AmericanRheumatism Association 1987 revised criteria for theclassification of rheumatoid arthritis. Arthitis Rhewn 1988;31: 315-24.
8 Steinbrocker 0, Traeger C H, Batterman R C. Therapeuticcriteria in rheumatoid arthritis. JAMA 1949; 140: 659-62.
9 Hadler N M. Osteoarthritis as a public health problem. ClinRhewn Dis 1985; 11: 175-85.
10 Mitchell N S, Cruess R L. Classification of degenerativearthritis. Can Med AssocJ 1977; 117: 763-5.
11 Wood P H N. Osteoarthitis in the community. Clin RhenDis 1976; 2: 495-507.
12 McAlindon T, Dieppe P. Osteoarthritis: definitions andcriteria. Ann Rheum Dis 1989; 48: 531-2.
13 Huskisson E C, Dieppe P A, Tucker A K, Cassell B. Anotherlook at osteoartritis. Ann Rhewn Dis 1979; 38: 423-8.
14 Lawrence J S, Bremner J M, Bier F. Osteoarthritis:prevalence in the population and relationship betweensymptoms and x-ray changes. Ann Rhewn Dis 1966; 25:1-24.
15 Kellgren J H, Moore R. Generalised osteoarthritis andHeberden's nodes. Br Med J 1952; i: 181-4.
16 Doherty M, Preston B. Primary osteoarthritis of the elbow.Ann Rhewn Dis 1989- 48: 743-7.
17 Massardo L, Watt I, Cushnaghan J, Dieppe P. An eight yearprospective study of osteoarthritis of the knee joint. AnnRheum Dis 1989; 48: 893-7.
18 Meachim G, Whitehouse G H, Pedley R B, Nichol F E,Owen R. An investigation of radiological, clinical andpathological correlations in osteoarthritis of the hip. ClinRadiol 1980; 31: 565-74.
19 Harris W. Etiology of osteoarthritis of the hip. Clin Ortp1986; 213: 20-33.
20 Van Saase J L C M, Vandenbroucke J P, van Romande L,Valkenburg H A. Osteoarthritis and obesity in the generalpopulation. A relationship calling for an explanation.Rhewnatol 1988; 15: 1152-8.
21 Royal College of Physicians. Obesity. J R Coil PhysiciansLond 1983; 17: 5-65.
22 YaziciH,SavillePD,SalvatiEA,etal. Primaryosteoarthritisofthe knee or hip-prevalence of Heberden's nodes inrelation to age and sex. JAMA 1975; 231: 1256-60.
23 Lawrence J S. Rhewmatim in population. London: Heine-mann, 1977.
24 Cobby M, Cushnaghan J, Creamer P, Dieppe P, Watt I.Erosive osteoarthitis: Is it a separate disease entity? ClinRadiol (in press).
13