Embed Size (px)
Citation preview

236 de Takats, de Takats, Iqbal, et al
Symptomatic cardiomyopathy as a presentation inWhipple's disease
PG de Takats, DLP de Takats, TH Iqbal, RDS Watson, MN Sheppard, BT Cooper
City Hospital, DudleyRoad, BirminghamB18 7QH,UKDepartment ofCardiologyPG de TakatsRDS WilsonGastroenterology UnitDLP de TakatsTH IqbalBT Cooper
Department ofHistopathology, RoyalBrompton NationalHeart and LungHospital, Sydney St,London SW3 6NP, UKMN Sheppard
Correspondence toDr PG de Takats, SeniorRegistrar in MedicalOncology, Department ofClinical Oncology, QueenElizabeth Hospital,Birmingham B15 2TH, UK
Accepted 27 October 1994
SummaryA patient presenting with congestive car-diac failure and anaemia underwent in-vestigation which led to the diagnosis ofWhipple's disease, associated with dilatedcardiomyopathy. Conventional antibiotictherapy for Whipple's disease resulted inresolution of the traditional features ofWhipple's disease and a marked improve-ment in the patient's heart failure.
Keywords: Whipple's disease, dilated cardiomyo-pathy, endomyocardial biopsy
Introduction
First described in 1907,' valid cases ofWhipple's disease reported in the worldliterature to date number around 800. Asoriginally suspected by Whipple, the conditionis now considered to be of infective aetiology,2although the nature of the infecting organismremains undefined. This rare multisystemdisorder has a number of characteristics (seebox). Cardiac involvement is unusual.Although a rarity, diagnosis of Whipple'sdisease carries great significance since effectivetreatment can prevent progression of an other-wise fatal outcome and instead result in cure.
Cardiological changes associated withWhipple's were first described by Upton in1952.3 Previously, gross deformities of heartvalves and the pericardium observed in postmortem cases were ascribed to co-existentrheumatic heart disease. However, more recenthistological studies have shown periodic acidSchiff(PAS)-positive macrophages in the hearttissue of patients with untreated Whipple'sdisease, suggesting a direct relationshipbetween the two entities. A variety of cardiacabnormalities are now recognised to occur in
Whipple's disease: features
* migratory polyarthritis* fever* malabsorption with weight loss* abdominal pain* anaemia* diarrhoea* lymphadenopathy* central nervous system disturbancee male preponderance* skin pigmentation
Whipple's disease, although cardiac involve-ment rarely gives rise to clinical manifestationsand is usually an incidental post mortem finding.We describe a patient with clinical evidence ofmyocardial disease as a presenting feature ofWhipple's disease, whose cardiac dysfunctionresponded to antibiotic therapy.
Case history
A 65-year old retired caucasian man was ad-mitted to hospital with a six-week history ofbreathlessness and cough productive of whitesputum, which had been getting progressivelyworse, despite digoxin and diuretic therapyfrom his general practitioner. No orthopnoeaor ankle oedema was reported, but the patientfelt non-specifically unwell, with arthralgiaaffecting small joints symmetrically, princi-pally in the hands. His bowel habit was normal.Two years previously, he had lost one stone inweight over a period of months, which he hadnever regained. He was a retired engineer,married with no pets, having always lived inEngland and with no history of recent travelabroad. A life-long non-smoker, taking onlymodest quantities of alcohol, he had no othersignificant past medical history. His medica-tion on admission comprised digoxin, co-amilofruse, and ibuprofen.On examination, he had a tanned complexion
and was pyrexial, 37.50C. He had no jaundice,cyanosis, clubbing, or lymphadenopathy andwas not obviously anaemic. He had a regulartachycardia of 120 beats/min with a galloprhythm, but no murmurs were heard. Hisjugular venous pressure was not elevated andhis chest was clear.An electrocardiogram (ECG) showed atrial
tachycardia with right bundle branch block andhis chest radiograph was consistent with mildleft ventricular failure. Initial blood resultswere as follows: haemoglobin 10.8 g/dl, meancorpuscular volume 66 fl, mean corpuscularhaemoglobin 20.8 pg, white blood cell count17.05 x 199/1 (80% neutrophils), serumalbumin 29 g/l. Platelet count, plasma vis-cosity, serum B12, folate, biochemical profileand thyroid function tests were all normal.Faecal occult blood tests were negative, as wereblood and sputum cultures.Upper gastrointestinal endoscopy was per-
formed to investigate the anaemia and revealedmild gastritis only. A small bowel biopsyshowed normal villus architecture, but thelamina propria was infiltrated with PAS-
on 30 August 2018 by guest. P
rotected by copyright.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.71.834.236 on 1 April 1995. D
ownloaded from
Symptomatic cardiomyopathy and Whipple's disease 237
positive macrophages diagnostic of Whipple'sdisease (figure 1). Antibiotic therapy wasinitiated and within 48 hours his fever andneutrophilia settled. He was discharged ondaily tetracycline, iron supplements, and co-amilofruse.When reviewed in clinic three weeks later,
the patient had developed exertional dyspnoea,orthopnoea, paroxysmal nocturnal dyspnoea,and ankle oedema, despite diuretic therapy. Onexamination, he was tachycardic, with a galloprhythm and an ejection systolic murmur. Hisjugular venous pressure was now grosslyelevated, with tender hepatomegaly andbilateral pitting oedema to his knees. A chestradiograph was consistent with worsening leftventricular failure, including a new small right-sided pleural effusion, while his ECG wasunchanged. An echocardiogram showed dila-tation of all four chambers of the heart, withgeneralised poor systolic function (figure 2A)and left ventricular ejection fraction (LVEF)estimated at 42%.The patient was treated for congestive car-
diac failure with digoxin, diuretics, anangiotensin-converting enzyme (ACE)inhibitor, nitrates and hydralazine. On thistreatment, he reverted to controlled atrialfibrillation and was therefore also anti-coagulated with warfarin. He made a gradualimprovement and when stable, coronary angio-graphy and endomyocardial biopsy were per-formed. The coronary arteries were entirelynormal and the LVEF was consistent withprevious echocardiographic findings. Biopsies
A
rU .i,, .....; :...d
B
*.. ..........................
Figure 1 Small bowel biopsies confirming initialdiagnosis of Whipple's disease The extent of villusshortening and PAS stain uptake by macrophages isdemonstrated in A (x 100), while at higher power, B(x 200), numerous foamy macrophages with granularcytoplasm are visible within the villus
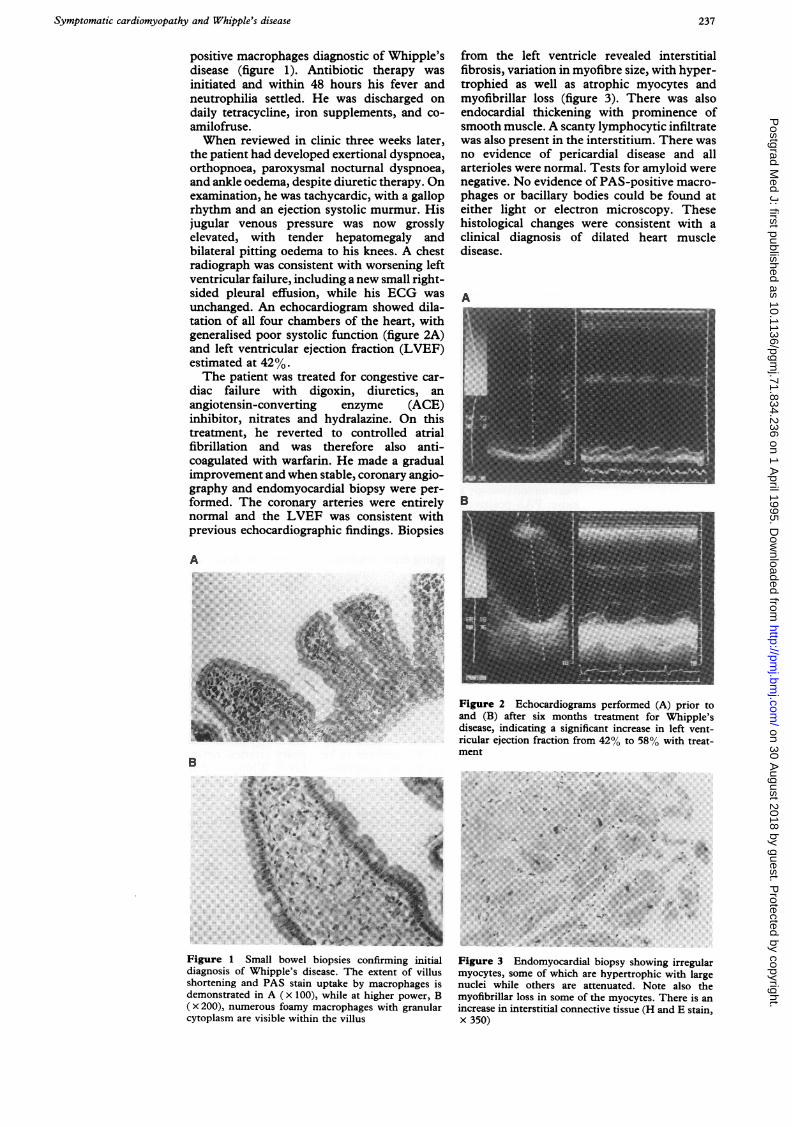
from the left ventricle revealed interstitialfibrosis, variation in myofibre size, with hyper-trophied as well as atrophic myocytes andmyofibrillar loss (figure 3). There was alsoendocardial thickening with prominence ofsmooth muscle. A scanty lymphocytic infiltratewas also present in the interstitium. There wasno evidence of pericardial disease and allarterioles were normal. Tests for amyloid werenegative. No evidence of PAS-positive macro-phages or bacillary bodies could be found ateither light or electron microscopy. Thesehistological changes were consistent with aclinical diagnosis of dilated heart muscledisease.
AI.B _~~~~~~~~~~~~~~~~~~~~~~~~~..........
.~~ ~ ~ ~ ~ ~~~~~~~~ .....X.....~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. ... ........B
Figure 2 Echocardiograms performed (A) prior toand (B) after six months treatment for Whipple'sdisease, indicating a significant increase in left vent-ricular ejection fraction from 42% to 58% with treat-ment
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.. .. .. ...~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. .. ..l_ _|~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.. .. . _ .. . .~~~~~~~~~~~~~~~~~~~~~~~~~~~~~__.03Er714> E
Figr 3 Enoycada bipysoin_ reuamycts som of whc aryetohcwtagnuliwieohr r teutd oeas hmyfbra los insmftemoye hr sainceasinitrttacnetv _iseHadEsanx.350)
on 30 August 2018 by guest. P
rotected by copyright.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.71.834.236 on 1 April 1995. D
ownloaded from

238 de Takats, de Takats, Iqbal, et al
Six months after starting antibiotic treat-ment, the patient's heart failure was wellcontrolled, having discontinued nitrate andhydralazine therapy. His anaemia resolved,with replenished iron stores and his serumalbumin normalised. Repeat small bowelbiopsy failed to show any PAS-positive macro-phages in an otherwise normal-looking speci-men. At that time, he remained in controlledatrial fibrillation, and repeat echocardiographyshowed considerable resolution of cardiachypertrophy, with significant improvement inLVEF, estimated at 58% (figure 2B).The patient is now two years from commenc-
ing antibiotic therapy and has reverted back tosinus rhythm. He remains on tetracycline,digoxin, and lisinopril, currently with noclinical manifestations of Whipple's disease.
Discussion
In the patient presented here, the close tem-poral association of the rapid development ofheart failure with clinical and histologicalevidence of dilated cardiomyopathy and addi-tional clinical manifestations of Whipple'sdisease strongly implies that the myocardialdisorder was due to Whipple's disease. Thisview is supported by his response to therapyand subsequent recovery of cardiac function.At the time of heart muscle biopsy, light and
electron microscopy failed to show evidence ofeither PAS-positive macrophages or bacillarybodies in biopsy specimens. However, thepatient had been on antibiotic treatment for sixweeks prior to the biopsy. In addition, there isalso the likelihood of sampling error, while it isrecognised that histological evidence ofWhipple's disease may be sparse, even in postmortem hearts of untreated patients.4Three weeks after initiating antimicrobial
therapy, the patient was admitted to hospitalwith florid signs of cardiac failure. This is notaltogether surprising, since clearance of PAS-positive macrophages from the gut is known tobe tremendously variable, requiring severalweeks to many years5 in some instances. Thus,while features such as fever and neutrophiliamay settle rapidly following introduction ofantibiotics, more severe manifestations such ascardiac dysfunction would be expected to bemore sustained. In favour of the associationbetween the myocardial disease and Whipple'sin this case is that, despite a reduction in drugtreatment (notably, nitrates and hydralazine),there was a major improvement in cardiacfunctional capacity, which has persisted overtime. In idiopathic dilated cardiomyopathy,changes in ejection fraction over time areusually small and the significant increase from42% to 58% over six months in this patientcould not be attributed to ACE inhibitortherapy alone.
In post mortem studies on hearts of patients
dying from Whipple's disease, the pathologicalchanges observed are consistent with that of achronic inflammatory process. The pericar-dium is most commonly involved, with pericar-ditis, pericardial adhesions and/or pericardialeffusions occuring in up to 60% of patients." 6'7Endocardial disease is a frequent finding, withincidental cardiac murmurs documented in upto 30% of patients during life, while postmortem reports describe valvular vegetations inat least 50% of cases.8 Myocardial involvement,however, is rare. There are only a few cases inthe literature which describe myocarditis aspart of a pancarditis, in an otherwise grosslynormal heart, diagnosed usually at postmortem,7'9 but, on one occasion, during life.4Myocarditis in the face of normal heart valves,chambers, and coronary vasculature has onlyonce been previously documented and was anunexpected post mortem finding in a patientdying of Whipple's disease.'0 Chronic damageto the pericardium, endocardium and, lessfrequently, the myocardium resulting from thepolyserositis characteristic of Whipple'sdisease is probably the cause of death in mostpatients with end-stage disease."'
Congestive cardiac failure appears to charac-terise the terminal stages ofuntreated Whipple'sdisease. In addition, it is estimated that thefrequency ofsudden death in Whipple's diseaseis around 20% 12 and such events are attributedto heart conduction defects and arrhythmias.Conduction tissue defects9 and various ECGchanges including bundle branch block,""4complete heart block'0 and non-specific ST/Twave changes4 have been documented.
Intrinsic heart muscle disease has neverpreviously been described in Whipple'sdisease, although focal myocardial fibrosis hasbeen observed in post mortem heart speci-mens." Moreover, heart failure as a presentingclinical feature, in the absence of significantvalvular or pericardial disease, has not beenpreviously documented. We have presented aunique case of Whipple's disease who devel-oped florid cardiac failure in association with anatrial tachycardia and bundle branch block.Echocardiography showed four chamber dila-tation and endomyocardial biopsy confirmeddilated heart muscle disease, with normal cor-onary arteries, never previously diagnosed inlife in Whipple's disease.This case acts as a reminder that Whipple's
disease can present without gastrointestinalsymptoms. The diagnosis should also be con-sidered in the differential diagnosis of everycase of dilated cardiomyopathy where there areassociated features such as malabsorption,polyarthralgia, pigmentation, or neuropsychia-tric disturbance.
We thank Dr S Singh for performing the endomyocar-dial biopsy and Dr J Gearty for assistance in interpreta-tion of the small bowel histopathology.
1 Whipple GH. A hitherto undescribed disease characterisedanatomically by deposits of fat and fatty acids in theintestinal and mesenteric lymphatic tissues. Johns HopkinsHosp Bull 1907; 18: 382-91.
2 Relman DA, Schmidt TM, MacDermott RP, Falkow S.Identification of the uncultured bacillus of Whipple'sdisease. N Engl Med J 1992; 327: 293-300.
3 Upton AC, Histochemical investigation of mesenchymallesions in Whipple's disease. Am J Clin Pathol 1952; 22:755-64.
4 Pelech T, Fric P, Huslarova A, Jirasek A. Intestinal lym-phocytic myocarditis in Whipple's disease. Lancet 1991; 337:553-4.
on 30 August 2018 by guest. P
rotected by copyright.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.71.834.236 on 1 April 1995. D
ownloaded from
Symptomatic cardiomyopathy and Whipple's disease 239
5 Trier JS, Phelps JC, Eidelman S, Rubin CE. Whipple'sdisease. Gastroenterology 1965; 48: 384-407.
6 Krauntz RF. Whipple's disease with cardiac and renalabnormalities. Arch Intern Med 1969; 123: 701-6.
7 Lie JT, Davis JS. Pancarditis in Whipple's disease: electron-microscopic demonstration of intracardiac bacillary bodies.Am J Clin Pathol 1976; 66: 22-30.
8 Enzinger FM, Helwig EB. Whipple's disease. A review ofthe literature and report of fifteen patients. Virchows Arch(A) 1963; 336: 238-69.
9 James TN, Haubrich WS. Bacterial arteritis in Whipple'sdisease. Circulation 1975; 52: 722-31.
10 Southern JF, Moscicki RA, Magro C, Dickersin GR, Fallon
JT, Bloch KJ. Lyphoedema, lymphocytic myocarditis, andsarcoidlike granulomatosis: manifestations of Whipple'sdisease. JAMA 1989; 261: 1467-70.
11 McAllister HA, Fenoglio JJ. Cardiac involvement inWhipple's disease. Circulation 1975; 52: 152-6.
12 Rose AG. Mital stenosis in Whipple's disease. Thorax 1978;33: 500-3.
13 Fleming JL, Wiesner RH, Shorter RG. Whipple's disease:clinical, biochemical, and histopathological features andassessment oftreatment in 29 patients. Mayo Clin Proc 1988;63: 539-51.
14 Sossai P, DeBoni M, Cielo R. The heart and Whipple'sdisease. Int I Cardiol 1989; 23: 275-6.
Central pontine myelinolysis following orthotopicliver transplant: association with cyclosporinetoxicity
Mustafa H Kabeer, Ronald S Filo, Martin L Milgrom, Mark D Pescovitz,Stephen B Leapman, Lawrence Lumeng, Rahul M Jindal
Department ofSurgery, Dvision ofTransplantation,Department ofMedicine, Division ofGastroenterology/Hepatology, IndianaUniversity MedicalCenter, Indianapolis,Indiana, USAMH KabeerRS FiloML MilgromMD PescovitzSB LeapmanL LumengRM Jindal
Correspondence toDrRM Jindal, Division ofTransplantation (4258),Indiana University MedicalCenter, 550-N UniversityBlvd, Indianapolis,IN 46202, USA
Accepted 26 October 1994
SummaryCentral pontine myelinolysis can occurafter orthotopic liver transplantationleading to high mortality and seriousmorbidity. In our case, central pontinemyelinolysis was associated with widefluctuations in cyclosporine levels duringan episode of hypocholesterolaemia,which may have precipitated central pon-tine myelinolysis.
Keywords: central pontine myelinolysis, liver trans-plantation, cyclosporine
Introduction
Central pontine myelinolysis is a distinctivelesion seen after a variety of conditions (box1).1-' With the widespread application oforthotopic liver transplantation, neurologicalcomplications such as central pontinemyelinolysis has again come into focus.4
Since the introduction of cyclosporine andthe new immunosuppressant FK506,neurological toxicity has been increasinglyrecognised as a complication of both therapies(box 2). Also reported are instances of akineticmutism, severe dyskinesia and pseudo-bulbar
Central pontine myelinolysis:causes
* rapid correction ofsodium and osmolality inpatients who have underlying liver disease
* malnutrition* alcoholism* pneumonia* advanced malignancies* lymphoma* severe burns* haemorrhagic pancreatitis
Box 1
palsies.7 It has been shown that cyclosporineneurotoxicity is specifically aggravated by lowmagnesium and low cholesterol levels.8We report a case of central pontine
myelinolysis after orthotopic liver transplanta-tion in which high cyclosporine levels may haveled to seizure activity, and central routinemyelinolysis subsequently developed due tore-initiation of cyclosporine during an episodeof hypocholesterolaemia.
Case report
A 50-year-old white man with end-stage liverdisease secondary to cryptogenic cirrhosis wastransplanted uneventfully with an ABO-compatible liver. During surgery there was noevidence of haemodynamic disturbances suchas excessive blood loss or re-perfusion synd-rome. Neurologic examination before trans-plantation was normal. His immunosuppres-sive protocol consisted of Imuran (iv 2 mg/kg),methylprednisolone (iv 1 mg/kg) and iv cyclo-sporine (2 mg/kg by continuous infusion) andswitched to po medication when tolerated. Hewas extubated on the second day and was awakeand neurologically stable, as were his othersystems.
Neurological complications ofcyclosporine toxicity
* headache* tremors* convulsions* coma* ataxia* quadriparesis* cerebral blindness
Box 2
on 30 August 2018 by guest. P
rotected by copyright.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.71.834.236 on 1 April 1995. D
ownloaded from





























