Embed Size (px)
Citation preview
514-
THE DIAGNOSIS AND MANAGEMENT OFHAEMOPHILIA AND CHRISTMAS DISEASEBjy M. C. G. ISRAELS, M.Sc., M.D., F.R.C.P., F. NOUR-ELDIN, Ph.D., M.B., L.S.A.,
and JOHN F. WILKINSON, M.Sc., Ph.D., M.D., F.R.C.P., F.R.I.C.From the Department of Haematology, Royal Infirmary and University of Manchester
The diagnosis of the clinically similar bleedingdiseases Haemophilia and Christmas diseasedepends on the clinical history and the clinicalpicture, the family history and the special labora-tory tests. With the technical methods nowavailable, the diagnosis can be made positively inall cases. The clinical history can vary from a lifeof chronic or recurring invalidism since infancyto an affection so mild that only a tooth extractionor minor injuries cause trouble. Points that arediagnostically suggestive are: spontaneous haemar-throses, spontaneous bruising in childhood orbruises out of all proportion to trauma and bleedingfor more than 48 hours after tooth extraction;less commonly spontaneous haematuria, melaenaand epistaxis may occur. Excessive bleeding aftercircumcision in infancy is frequently said to be thefirst haemorrhagic incident. The patients arenearly always males but females may have thesediseases, although extremely rarely.Family HistoryOwing to the sex-linked transmission of
haemophilia and of Christmas disease by femaleswho remain unaffected, one or more ' silent'generations are common and then the familyhistory is lost or not observed. A typical familyhistory is very valuable when obtained, but in ourseries of nearly 300 patients we only found it inabout 6o per cent. of them. There is no doubtthat new mutations explain some of the other40 per cent.
Laboratory Diagnostic TestsThe whole blood clotting time is characteris-
tically prolonged, often grossly, but in 32 per cent.of our cases the clotting time was normal.The prothrombin consumption index is based
on the fact that in these diseases little prothrombinis converted to thrombin and remains in the serum;whereas in the normal person no more than a traceof prothrombin remains in the serum afterclotting. Normal values for this index are less
than 40 per cent.; over 40 per cent., provided thatthe platelet count is normal, is diagnostic ofhaemophilia and of Christmas disease. But hereagain, in 28 per cent. of our cases, this test gave anormal result.The thromboplastin generation test as originally
described by Biggs and Douglas (I953) makes itpossible to distinguish between deficiency ofantihaemophilic globulin and Christmas factor.In order to confirm the presence of true haemo-philia or Christmas disease the inhibitory actionof the plasma must be demonstrated by themethod of Nour-Eldin and Wilkinson (1958a, b,1959) in addition to the deficiency in AHG orChristmas factor respectively. Wilkinson, Nour-Eldin and Israels (1958) have demonstrated theabsence of this blood-clotting inhibitor termedBridge anticoagulant in three patients with vonWillebrand's syndrome; this has since beenverified in another three cases.
Christmas disease occurs with a frequency ofabout I5 per cent. of all patients having theclinical features seen in association withhaemophilia.
ManagementMost minor incidents can be dealt with in an
out-patient clinic, but if any likelihood of trans-fusion arises, it is better to admit the patient, evenif the danger seems to have passed. Minoroperations and tooth extractions must not beattempted in an out-patient clinic or surgery.
Blood transfusion for the replacement of lost redcells and for giving the patient temporarily someantihaemophilic globulin or Christmas factor is anessential part of treatment. For red-cell replace-ment only, packed stored red cells can be used;for the supply of the antihaemophilic globulinfactor, fresh blood-i.e. used within four hours ofwithdrawal-is essential. If the Christmas factoris required fresh blood is best in an emergency,but plasma from blood not more than five days oldcan also be used (Nour-Eldin and Wilkinson
Protected by copyright.
on 15 May 2018 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.407.514 on 1 S
eptember 1959. D
ownloaded from
September I959 ISRAELS, NOUR-ELDIN and WILKINSON: Haemophilia and Chlristmas Disease 515
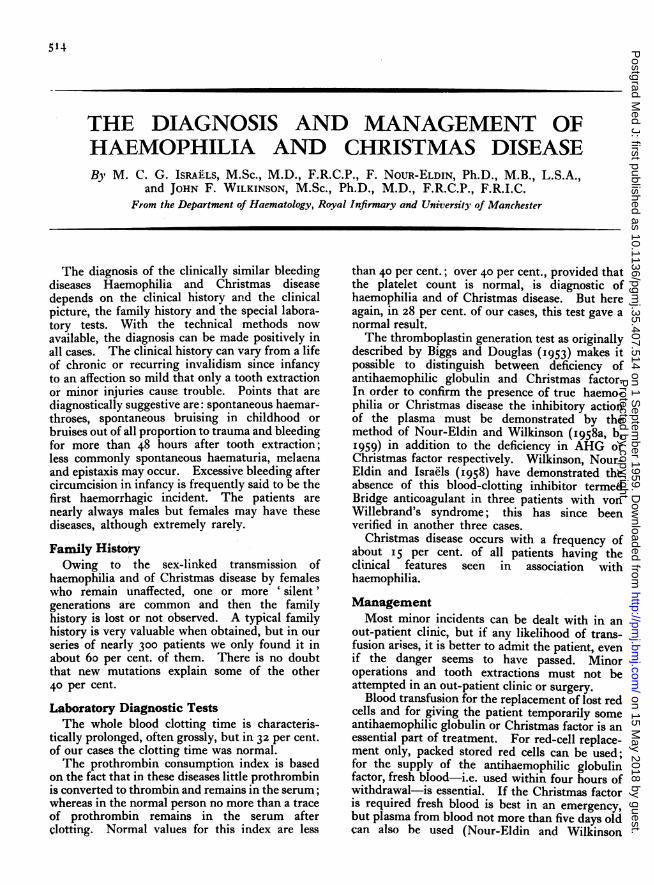
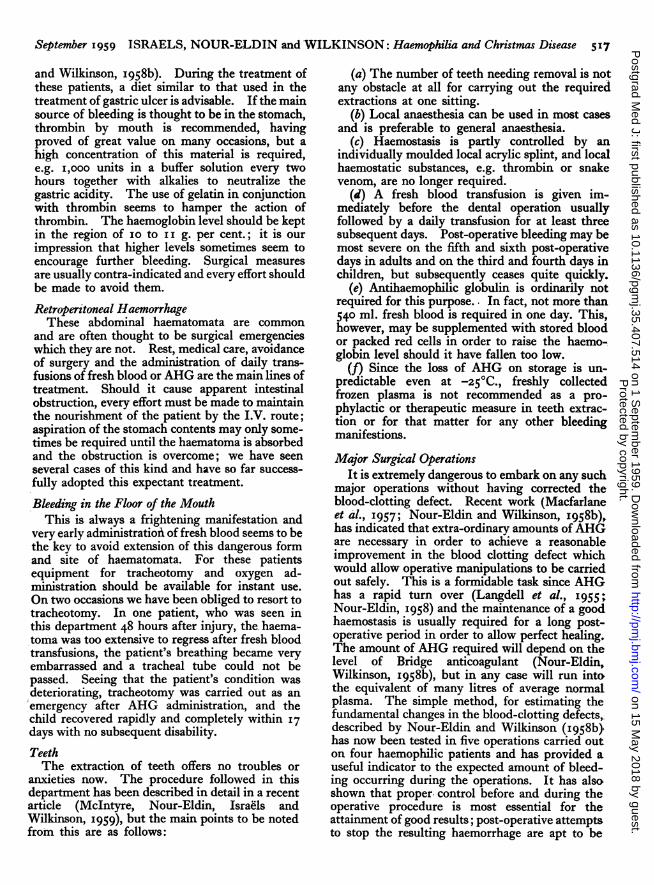
FIG. I.-X-ray of knee joints showing gross arthritic changes with considerablenarrowing of joint spaces and deformity of patello-femoral joints.Juxta-articular cysts are seen in the tibia.
1958c). Human antihaemophilic globulin hasbeen prepared in concentrated form by Kekwickand Wolf (I957) but only strictly limited quantitiesare available and it is valuable when the AHGconcentration must be raised quickly. Animalantihaemophilic globulin (Bidwell, 1955) has beenmade from pig and ox blood, which contain muchgreater quantities than human blood and havebeen extensively tested and also found to be veryvaluable in emergency; their use, however, islimited somewhat by the rapid development ofantibodie3 after the first course of treatment.
HaematomataSubcutaneous bruises are common occurrences
developing either spontanecusly or as a result ofminor traumata; apart from care in order to avoidfurther sources of injury in the latter case, theseneed no special treatment. Large haematomatainvolving the muscles and specially those reducingthe haemoglobin concentration necessitate bloodtransfusions, and early treatment is often followedby extra-ordinarily rapid disappearance of thehaematomata. As an example, the following caseis described.The patient (T.H.) was admitted on a Monday
with an extensive bleeding irto the lower thirdof the abdominal wall, the upper two-thirds of theleft thigh and the whole of the gluteal regions,reducing his haemoglobin to 5.0 g. per cent. Hewas given 540 ml. of fresh blood and 250 ml. ofpacked cells. After five days, apart from yellowskin discolouration, there were hardly any signsof the haematoma. During this period no furtherfresh blood was administered; the haemoglobin
level was raised bv 500 ml. packed cells on the thirdday and i,ooo ml. stored blood on the fifth day.The patient was discharged on the eighth daywith a haemoglobin level of 10.7 g.
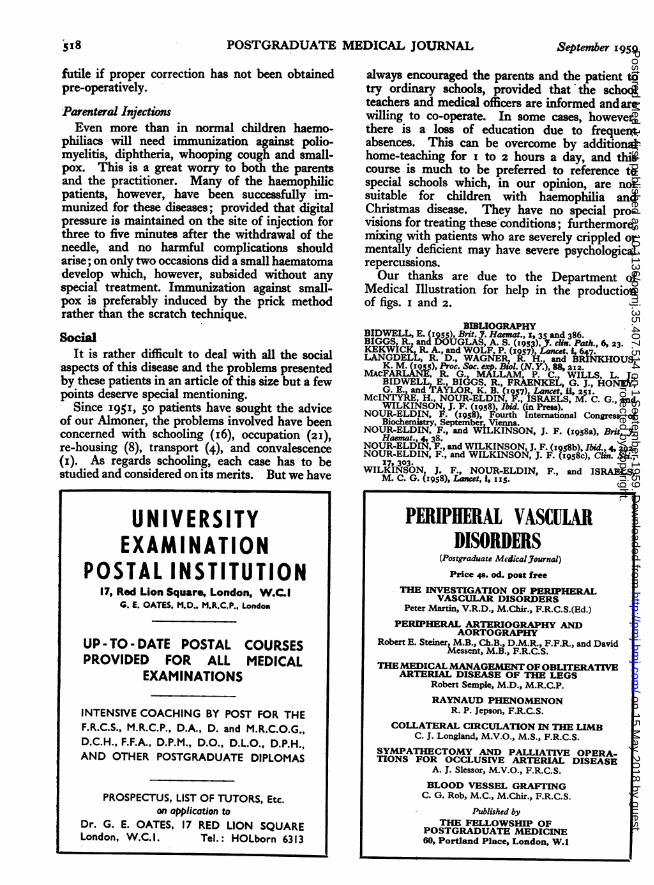
HaemarthrosisTable i shows the distribution of joints affected
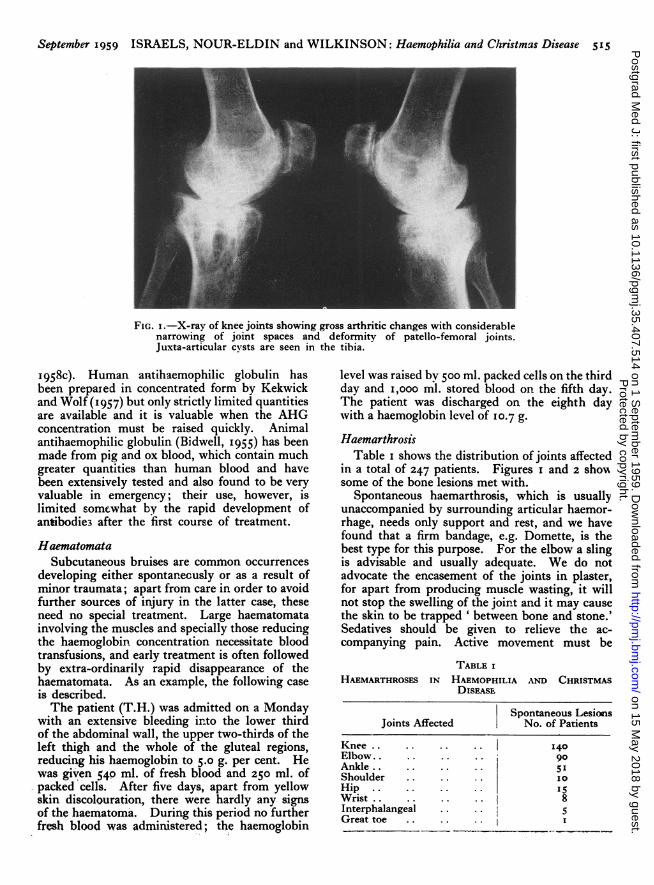
in a total of 247 patients. Figures i and 2 showsome of the bone lesions met with.
Spontaneous haemarthrosis, which is usuallyunaccompanied by surrounding articular haemor-rhage, needs only support and rest, and we havefound that a firm bandage, e.g. Domette, is thebest type for this purpose. For the elbow a slingis advisable and usually adequate. We do notadvocate the encasement of the joints in plaster,for apart from producing muscle wasting, it willnot stop the swelling of the joint and it may causethe skin to be trapped ' between bone and stone.'Sedatives should be given to relieve the ac-companying pain. Active movement must be
TABLE IHAEMARTHROSES IN HAEMOPHILIA AND CHRISTMAS
DISEASE
Spontaneous LesionsJoints Affected No. of Patients
Knee .. ... ... . 140Elbow.. .. .. .. goAnkle .. .. .. .. 5'IShoulder .. .. .. I0HiP .. . . ISWrist.. .. .. .. I 8Interphalangeal .. .. 5Great toe .. .. .
Protected by copyright.
on 15 May 2018 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.407.514 on 1 S
eptember 1959. D
ownloaded from
516 POS'TGRADUATE MEDICAL JOURNAI, September I959
AlIM
FIG. 2.-X-ray of left hip showing flattened head offemur simulating Perthe's disease. This is a rarefinding in haemophilic joints.
started as soon as the pain is relieved. Physio-therapy is very helpful in restoring the movementsof the joints and developing the weak muscles.The traumatic haemarthrosis or that ac-
companied by bleeding in surrounding musclesnecessitates more active treatment. Fresh bloodtransfusions are used to help to stop the bleedingand usually a daily volume of 540 ml. is required.A back splint for the lower limbs may be required,but this should be of the lightest weight and re-moved as soon as possible in order that physio-therapy treatment can be started.
WoundsThe following three principles underly the basic
procedure adopted for dealing with these lesions:
Pow,dered thrombin is locally applied in its drystate to the wound on sterile petroleum-jellygauze; ordinary gauze has two disadvantages,namely, absorption of the thrombin and adherenceto any clot which may form.
Suturing must be avoided; a pressure bandageis all that is required, and this should be left un-disturbed for at least five days so that any clot isnot dislodged.
Prophylaxis against sepsis by suitable oral anti-biotics is advisable; we usually use tetracycline.
Epistaxes are frequent symptoms. Havingmade sure that there is no local abnormality, anasal pack is inserted after local application ofthrombin. The pack, which is preferably left un-disturbed for 48 hours is gradually removed bycutting off a few inches at a time. In a few cases,however, fresh blood transfusions will be neededin order to control the bleeding and to raise thehaemoglobin level.
Nerve PalsiesWhere these occur, the important point is to
persist with treatment indefinitely, giving physio-therapy and muscle re-education for as long asmay be required. In peripheral nerve palsies,fresh blood or antihaemophilic globulin trans-fusions are often required; in one case of bleedinginto the cauda equina we were able to re-habilitatethe patient by intensive AHG administrationfollowed by a prolonged physiotherapy course.
Similarly several cases of median and ulnarnerve palsies have been successfully treated usingfresh blood transfusions and local support.
HaematuriaExperience has shown that haematuria is the
least troublesome form of bleeding, howeveralarming it-may be for the patient and it rarelywarrants any specific treatment. In most cases itclears up within two weeks or less causing nosignificant drop in the haemoglobin level. Never-theless, it is advisable to make X-ray and otherexaminations to exclude the presence of a urinarystone or other possible lesions. Treatment con-sists of sedatives with belladonna.
MelaenaIn contrast to haematuria, melaena is the most
troublesome symptom and must be investigatedand treated in hospital. Apart from bleedingfrom the mucous membrane, peptic ulcerationsometimes may be a contributing factor. Althoughimmediate transfusions of fresh blood or AHGfractions are usually required, the total amountrequired for controlling this haemorrhage varieseven for the same patient on different occasions;this has varied between l to 20 litres (Nour-Eldin
Protected by copyright.
on 15 May 2018 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.407.514 on 1 S
eptember 1959. D
ownloaded from
September I959 ISRAELS, NOUR-ELDIN and-WILKINSON: Haemophiia and Christmas Disease 517
and Wilkinson, I958b). During the treatment ofthese patients, a diet similar to that used in thetteatment of gastric ulcer is advisable. If the mainsource of bleeding is thought to be in the stomach,thrombin by mouth is recommended, havingproved of great value on many occasions, but ahigh concentration of this material is required,e.g. i,ooo units in a buffer solution every twohours together with alkalies to neutralize thegastric acidity. The use of gelatin in conjunctionwith thrombin seems to hamper the action ofthrombin. The haemoglobin level should be keptin the region of io to i i g. per cent.; it is ourimpression that higher levels sometimes seem toencourage further bleeding. Surgical measuresare usually contra-indicated and every effort shouldbe made to avoid them.
Retroperitoneal HaemorrhageThese abdominal haematomata are common
and are often thought to be surgical emergencieswhich they are not. Rest, medical care, avoidanceof surgery and the administration of daily trans-fusions of fresh blood or AHG are the main lines oftreatment. Should it cause apparent intestinalobstruction, every effort must be made to maintainthe nourishment of the patient by the I.V. route;aspiration of the stomach contents may only some-times be required until the haematoma is absorbedand the obstruction is overcome; we have seenseveral cases of this kind and have so far success-fully adopted this expectant treatment.
Bleeding in the Floor of the MouthThis is always a frightening manifestation and
very early administratioA of fresh blood seems to bethe key to avoid extension of this dangerous formand site of haematomata. For these patientsequipment for tracheotomy and oxygen ad-ministration should be available for instant use.On two occasions we have been obliged to resort totracheotomy. In one patient, who was seen inthis department 48 hours after injury, the haema-toma was too extensive to regress after fresh bloodtransfusions, the patient's breathing became veryembarrassed and a tracheal tube could not bepassed. Seeing that the patient's condition wasdeteriorating, tracheotomy was carried out as anemergency after AHG administration, and thechild recovered rapidly and completely within I7days with no subsequent disability.TeethThe extraction of teeth offers no troubles or
anxieties now. The procedure followed in thisdepartment has been described in detail in a recentarticle (McIntyre, Nour-Eldin, Israels andWilkinson, I959), but the main points to be notedfrom this are as follows:
(a) The number of teeth needing removal is notany obstacle at all for carrying out the requiredextractions at one sitting.
(b) Local anaesthesia can be used in most casesand is preferable to general anaesthesia.
(c) Haemostasis is partly controlled by anindividually moulded local acrylic splint, and localhaemostatic substances, e.g. thrombin or snakevenom, are no longer required.
(d) A fresh blood transfusion is given im-mediately before the dental operation usuallyfollowed by a daily transfusion for at least threesubsequent days. Post-operative bleeding may bemost severe on the fifth and sixth post-operativedays in adults and on the third and fourth days inchildren, but subsequently ceases quite quickly.
(e) Antihaemophilic globulin is ordinarily notrequired for this purpose.. In fact, not more than540 ml. fresh blood is required in one day. This,however, may be supplemented with stored bloodor packed red cells in order to raise the haemo-globin level should it have fallen too low.
(f) Since the loss of AHG on storage is un-predictable even at -250C., freshly collectedfrozen plasma is not recommended as a pro-phylactic or therapeutic measure in teeth extrac-tion or for that matter for any other bleedingmanifestions.
Major Surgical OperationsIt is extremely dangerous to embark on any such
major operations without having corrected theblood-clotting defect. Recent work (Macfarlaneet al., I957; Nour-Eldin and Wilkinson, 1958b),has indicated that extra-ordinary amounts ofAHGare necessary in order to achieve a reasonableimprovement in the blood clotting defect whichwould allow operative manipulations to be carriedout safely. This is a formidable task since AHGhas a rapid turn over (Langdell et al., I955;Nour-Eldin, I958) and the maintenance of a goodhaemostasis is usually required for a long post-operative period in order to allow perfect healing.The amount of AHG required will depend on thelevel of Bridge anticoagulant (Nour-Eldin,Wilkinson, I958b), but in any case will run intothe equivalent of many litres of average normalplasma. The simple method, for estimating thefundamental changes in the blood-clotting defects,.described by Nour-Eldin and Wilkinson (958b)jhas now been tested in five operations carried outon four haemophilic patients and has provided auseful indicator to the expected amount of bleed-ing occurring during the operations. It has alsoshown that proper. control before and during theoperative procedure is most essential for theattainment of good results; post-operative attemptsto stop the resulting haemorrhage are apt to be
Protected by copyright.
on 15 May 2018 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.407.514 on 1 S
eptember 1959. D
ownloaded from
518 POSTGRADUATE MEDICAL JOURNAL September I959
futile if proper correction has not been obtainedpre-operatively.
Parenteral InjectionsEven more than in normal children haemo-
philiacs will need immunization against polio-myelitis, diphtheria, whooping cough and small-pox. This is a great worry to both the parentrsand the practitioner. Many of the haemophilicpatients, however, have been successfully im-munized for these diseases; provided that digitalpressure is maintained on the site of injection forthree to five minutes after the withdrawal of theneedle, and no harmful complications shouldarise; on only two occasions did a small haematomadevelop which, however, subsided without anyspecial treatment. Immunization against small-pOX is preferably induced by the prick methodrather than the scratch technique.Soci
It is rather difficult to deal with all the socialaspects of this disease and the problems presentedby these patients in an article of this size but a fewpoints deserve special mentioning.
Since 195I, 50 patients have sought the adviceof our Almoner, the problems involved have beenconcerned with schooling (I6), occupation (2I),re-housing (8), transport (4), and convalescence(i). As regards schooling, each case has to bestudied and considered on its merits. But we have
always encouraged the parents and the patient totry ordinary schools, provided that the schoolteachers and medical officers are informed andarewilling to co-operate. In some cases, however,there is a loss of education due to frequentabsences. This can be overcome by additionalhome-teaching for I to 2 hours a day, and thiscourse is much to be preferred to reference tospecial schools which, in our opinion, are notsuitable for children with haemophilia andChristmas disease. They have no special pro-visions for treating these conditions; furthermore,mixing with patients who are severely crippled ormentally deficient may have severe psychologicalrepercussions.Our thanks are due to the Department of
Medical Illustration for help in the productionof figs. I and 2.
BIBLIOGRAPHYBIDWELL, E. (rQ5), Bnit. J. Haemat., x,35 and 386.BIGGS R and DOUGLAS, A. S. (z9s;), Y. cii. Path., 6, 23.KEKWiCI, R. A., and WOLF P. (97 Lancet. 1 647.LANGDELL, R. D., WAG_ER, R. h., and B NKHOUS,K. M. (I955), Proc. Soc. exp. BEol. (N.Y.), 88, 212.WCFARLANL R. G MALLAM, P. C. WILLS, L.
BIDVELL E. BI6GS, R., FRAENKEL, G. J., HONEG. E., and 6AYLOR, K. B. (I7) Lame, , 251.McINTYRE, H., NOUR-ELDIN '., iSRAELS, M. C. G., andWILKINSON, J. F. (I958), i. (in Press).
NOUR-ELDIN, F. (I958), Fourth International Congress ofBiochemistry, September, Vienna.NOUR-ELDIN, F., and WILKINSON, J. F. (19s8a), Brt. JT.Haemat., 4 38.NOUR-ELDIN F., and WILKINSON, J. F. (r958b), Ibid., 4, 292.NOUR-ELDIN F., and WILKINSON, J. F. (I958c), Clin. Sc.,
17, 303.WILKINSON, J. F., NOUR-ELDIN, F., and ISRAELS,M. C. G. (1958), Lancet, 1, IIS.
UNIVERSITYEXAMINATION
POSTAL INSTITUTION17, Red Lion Square, London, W.C.l
G. i. OATES. M.D.. M.R.C.P., London
UP - TO - DATE POSTAL COURSESPROVIDED FOR ALL MEDICAL
EXAMINATIONS
INTENSIVE COACHING BY POST FOR THEF.R.C.S., M.R.C.P., D.A., D. and M.R.C.O.G.,D.C.H., F.F.A., D.P.M., D.O., D.L.O., D.P.H.,AND OTHER POSTGRADUATE DIPLOMAS
PROSPECTUS, LIST OF TUTORS, Etc.on application to
Dr. G. E. OATES, 17 RED LION SQUARELondon, W.C. 1. Tel.: HOLborn 6313
PERIPHERAL VASCULARDISORDERS
(Postgraduate Medical.Journal)Price 4s. od. post free
THE INVESTIGATION OF PERIPHERALVASCULAR DISORDERS
Peter Martin, V.R.D., M.Chir., F.R.C.S.(Ed.)PERIPHERAL ARTERIOGRAPHY AND
AORTOGRAPHYRobert E. Steiner, M.B., Ch.B., D.M.R., F.F.R., and David
Messent, M.B., F.R.C.S.THEMEDICALMANAGEMENT OF OBLITERATIVEARTERIAL DISEASE OF THE LEGS
Robert Semple, M.D., M.R.C.P.RAYNAUD PHENOMENON
R. P. Jepson, F.R.C.S.COLLATERAL CIRCULATION IN THE LIMB
C. J. Longland, M.V.O., M.S., F.R.C.S.SYMPATHECTOMY AND PALLIATIVE OPERA-TIONS FOR OCCLUSIVE ARTERIAL DISEASE
A. J. Slessor, M.V.0., F.R.C.S.BLOOD VESSEL GRAFTING
C. G. Rob, M.C., M.Chir., F.R.C.S.Published by
THE FELLOWSHIP OFPOSTGRADUATE MEDICINE60, Portland Place, London, W.1
Protected by copyright.
on 15 May 2018 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.35.407.514 on 1 S
eptember 1959. D
ownloaded from