Embed Size (px)
Citation preview

Sympathomimetics

Overview
• Review of Autonomic Nervous System• Common ways of manipulating ANS• Parasympathetic agent• Sympathetic agents• Review by purpose of drugs• Non-autonomic uses

Autonomic Nervous System
“Rest and Digest”• Parasympathetic• Activities that serve body
maintenance needs- digestion, elimination, urination, relaxation
“Fight or Flight”• Sympathetic• Activities that deal with
facing threats (historically)- breathe, move, see far

Autonomic Nervous System
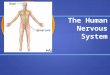
Autonomic NS
Common Drug targets of autonomic agents
• Heart (CV system)-chronotropic, inotropic, dromotrophic effects
• Vessels- vasoconstrict/dilate• Lungs- bronchodilate• Gut- increase or decrease motility• Bladder/GU- decrease tone, increase passage• Eye- Mydriatics/Miotics• CNS- Tune up/Tune down• MSK- affect neuromuscular blockade• CNS- sedation, excitation, fear response
Remember discrete effects possible
• Whole variety of receptors• Cholinergic– Nicotinic– Muscarinic (M1 vs. M2 )
• Adrenergic– α1, α2, β1, and β2
• Targeting on type allows greater specificity of action
• Variety of secondary Messengers

Second Messengers
DAG PKC
Parasympathetic Agents
• Cholinergic agonists– Direct- ACh, Bethanecol, Carbachol, Pilocarpine– Indirect (Anticholinesterases)- Neostigmine,
Edrophonium, Physostigmine
• Cholinergic antagonists– Direct’ish- Atropine, benzatropine, scopalmine,
ipratroprium, oxybutin, glycopyrrolate
• Others- Hexamethonium, Pralidoxime

Direct Cholinergic Agonists
• Systemic rarely used- Bethanecol– Gut- Ileus – Urinary – urinary retention
• Topical- more common (Bethanecol, Carbachol)– Glaucoma- • Open angle- Contracts ciliary muscle – alters trabecular
meshwork &helps drainage• Closed angle- Contracts pupil- pulls away from ciliary
body
Indirect Cholinergic Agonists
• All are reversible acetylcholinesterase inhibitors• Mainly vary in T1/2 and pharmokinetics
• Uses– Gut- reverse ileus (rarely used)– Glaucoma- Echothiphate, Physostigmine– Reverse neuromuscular blockade (Neostigmine,
edrophonium)– Myasthenia gravis- edrophonium for diagnosis,
neostig, pyridostig, or neostig for tx
Cholinergic Antagonists
• Gut- – antispasmodics (IBS)- hyoscyamine and atropine– Reduced secretions- glycopyrrolate and
scopolamine
• GU- reduce detrussor tone- oxybutin• Eye- atropine will dilate (mydriasis and
cycloplegia)- can precipitate angle closure glaucoma- BAD!!!

Cholinergic antagonists
• CNS- – Sedation- Scopalmine is used for motion sickness – Reverse Parkinsonism- Benzotropine (particularly
useful for drug induced parkinsonism or acute dystonia)
• Respiratory- Ipratroprium (or more rarely tiatroprium) is a bronchodilator
• CV- Atropine will increase heart rate (often used in OR)

Weird Cholinergic Drugs
• Hexamethonium- Nicotinic ACh receptor blocker= blocks ganglion– No real clinical indications
• Pralidoxime– Dephosphorylates and reactivates
acetylcholinesterase (after inactivation by organophosphates)
Cholinergic Poison= too much parasympathetic

Cholinergic Overdoses=too much parasympathetic
• Irreversible inhibitors of acetylcholinesterase• Symptoms- Diarrhea, Urination, Miosis,
Bronchospasm, Bradycardia, Excitation skeletal muscle and CNS, Lacrimation, Sweating, and Salivation (DUMBBELSS)
• Treatment– Atropine– Pralidoxime

Anticholinergic Toxicity

Anticholinergic Toxicity• Often our fault• Dirty drugs aimed at other receptors- TCA’s,
Antihistamines, Antipsychotics• Also plants- nightshade family (Jimson weed)• Mnemonics– Blind as a bat, mad as a hatter, red as a beet, hot as
hell, dry as a bone, the bowel and bladder lose their tone, and the heart runs alone
– Can't see, can't spit, can't pee, can't shit• Physostigmine or neostigmine common
treatments
Sympathetic drugs
Sympathomimetics• Alpha Blockers– α1, - Prazosin, Doxasosin, Terazosin, Phenoxybenzamine,
Phentolamine• Beta blockers– TONS: labetalol, metoprolol, propanolol, nadololol,
esmolol, etc…• Sympathetic agonists– α2 agonists– Clonidine and Guanfacine– Direct β agonists- albuterol, salmeterol, etc..– Pressors- ephedrine, norepinephrine, dobutamine,
dopamine, Ephinephrine• Indirect SNS drugs
Receptor type is important
• α1 – Gq, Ca =contracts smooth muscle (vascular smooth muscle, eye)
• α2- Gi, decreased cAMP= tunes down NE release (presynapic terminal)
• β1- Gs, increased cAMP= increased rate and contractility (heart)
• β2- Gs, increased cAMP= vasodilation, bronchodilation, insulin release

Alpha antagonists
• Mixed α1 and α2 (Almost never used)– Phenoxybenzamine, Phentolamine
• α1 specific– Prazosin, Doxasosin, (Cardura), Terasozin
(Hytrin), Tamsulosin (Floxax)
• α2 specific– Mirtazapine (Remeron)

Indications
• 4th or 5th line anti-HTN– Except in pheocromocytoma or cocaine- need
alpha
• BPH- huge market• ? PTSD• Depression- mirtazapine (particularly in old
people)
Side effects
• Orthostatic Hypotension• Reflex Tachycardia• Dizziness• Headache• Sedation and increased appetite with
mirtazapine

Beta blockers
• HUGE NUMBERS• Vary in specificity for β1 vs β2
• More β1 (CV) specific include (begin with a-m)– Metoprolol, carvedilol, atenolol , esmolol
• Less specific agents less commonly used– Propanolol, nadolol
• Except labetalol- has alpha activity too
Indications
• CV – Hypertension (1st or 2nd line)– Fast IV agents include esmolol and labetalol– CHF (if symptoms definitely)– Prevention death in CAD, MI– Rate control
• Glaucoma- decrease secretion of aqueous humor (open angle)- topical timolol

Side Effects
• Worsen asthma • Bradycardia or AV block• Decompensation in CHF exacerbation• Hypoglycemia unawareness• Problems if anaphylaxis- use Glucagon• CNS effects?- depression, impotence

Alpha 2 agonists
• Unlike other agonists actually tones down parasymphathetic (α2 is feedback inhibition)
• Clonidine, a- methyldopa and Guanfacine– Rarely used in HTN– Children w/ ADD (particularly if sleep problems
due to amphetamine)– Sometimes for impulsive behaviors– Methydopa- HTN in pregnancy

Beta 2 agonists
• Short acting- rescue inhalers– Albuterol, terbutaline (rarely used)– Also used for hyperkalemia (increases K uptake
into cell)• Long acting-– Salmeterol, Formoterol– Always combined with corticosteroids– Increased mortality when used alone?
• Toxicities – tachycardia, arrythmia, tremor

“Pressors”
• IV drugs used to support circulation• Usually in ICU with close monitoring• Almost all act on sympathetic nervous system• All tried to use short periods (dangerous)

Direct “Pressors”
• Epinephrine- direct agonist of everything– Uses- anaphylaxis, open angle glaucoma, asthma,
hypotension• NE- primarily alpha-1 (vasoconstriction)– Septic shock, distributive shock
• Isoproterenol= Beta agonist– Cardiac arrest, av block, asthma
• Dobutamine- β1>β2 – Increases cardiac contractility- cardiogenic shock,
heart failure
Pressor Side Effects
• Most side effects can be figured out physicologically– i.e. Vasocontriction can cause reflex tachycardia
• Any beta agonist can cause arrythmias• Concern of decreased renal perfusion w/ pure
NE
Indirect Pressors
• Ephedrine- Releases stored catecholamines– Hypotension and nasal decongestant
• Dopamine- D1= D2>B>a– Increasing doses different effects– First increases renal blood flow– Then increases heart rate and contraction– Then finally acts like NE
Indirect Sympathetic drugs• Reserpine- Blocks NE incorporation into
presynaptic vesicles– Old anti-HTN, causes depression
• Amphetamines- increased release stored catecholamines– Narcolepsy, ADD, ADHD, depression– Can cause HTN, arrythmia
• Methylxanthines- i.e. theophylline– Decrease cAMP degradation and bronchodilate– Dangers w/ lots of interactions, beta agonist effects
outside the lungs, etc…
Agents by purpose
• CV– Increase rate- Beta agonists and cholinergic
blockers= dobutamine, isopreternol, atropine– Slow rate/antiarrythmic= Beta antagonists and
cholinergic agents (not used clinically)- metoprolol, labetalol, etc..
• Respiratory– Bronchodilators = Beta 2 agonists and anti-
cholinergics- albuterol, ipratroprium, etc..

Agents by system
• GI– Anticholinergics decrease motility- hyocyamine, atropine– Cholinergics- Bethanecol can increase motility (though
rarely used)• GU– Alpha antagonists increase urination- Doxasosin, Terasozin– Anti-cholinergics decrease urgency- oxybutinin
• Eye- Glaucoma– Cholinergics contract pupil allow drainage– B blockers decrease fluid production