Embed Size (px)
Citation preview
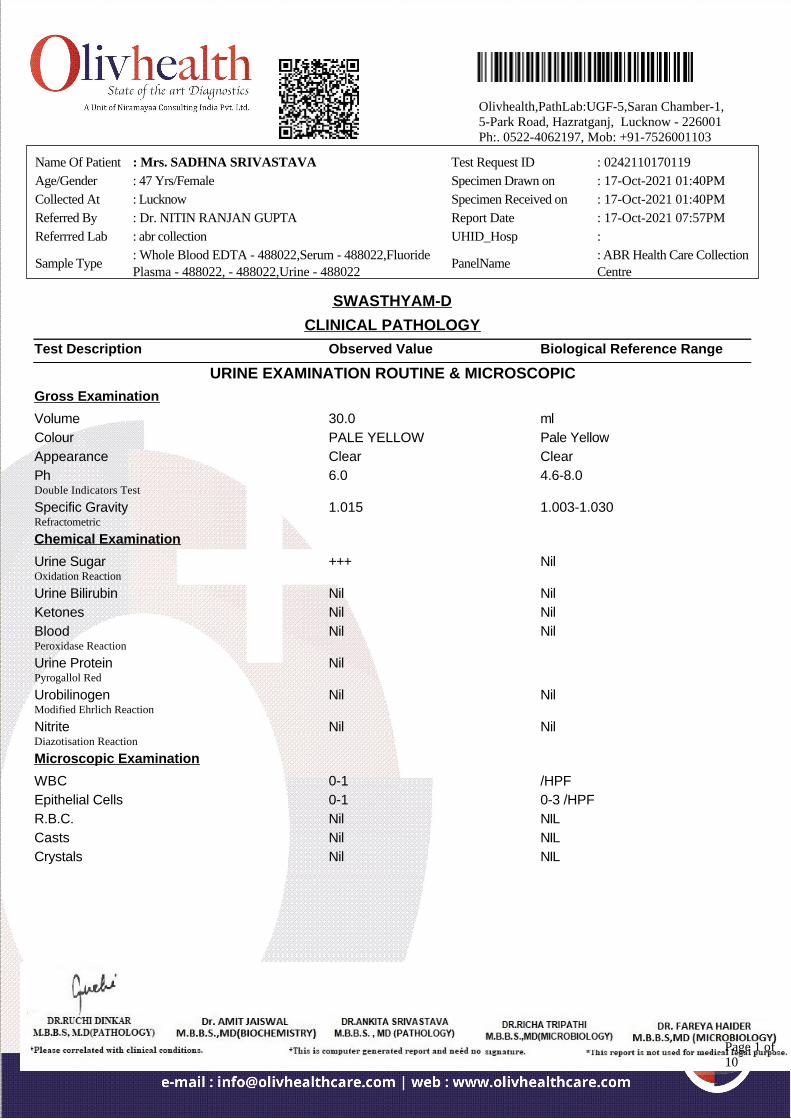
SWASTHYAM-D
CLINICAL PATHOLOGY
Test Description Observed Value Biological Reference Range
URINE EXAMINATION ROUTINE & MICROSCOPIC
Gross Examination
Volume 30.0 ml
Colour PALE YELLOW Pale Yellow
Appearance Clear Clear
PhDouble Indicators Test
6.0 4.6-8.0
Specific GravityRefractometric
1.015 1.003-1.030
Chemical Examination
Urine SugarOxidation Reaction
+++ Nil
Urine Bilirubin Nil Nil
Ketones Nil Nil
BloodPeroxidase Reaction
Nil Nil
Urine ProteinPyrogallol Red
Nil
UrobilinogenModified Ehrlich Reaction
Nil Nil
NitriteDiazotisation Reaction
Nil Nil
Microscopic Examination
WBC 0-1 /HPF
Epithelial Cells 0-1 0-3 /HPF
R.B.C. Nil NIL
Casts Nil NIL
Crystals Nil NIL
Name Of Patient : Mrs. SADHNA SRIVASTAVA Test Request ID : 0242110170119
Age/Gender : 47 Yrs/Female Specimen Drawn on : 17-Oct-2021 01:40PM
Collected At : Lucknow Specimen Received on : 17-Oct-2021 01:40PM
Referred By : Dr. NITIN RANJAN GUPTA Report Date : 17-Oct-2021 07:57PM
Referrred Lab : abr collection UHID_Hosp :
Sample Type: Whole Blood EDTA - 488022,Serum - 488022,FluoridePlasma - 488022, - 488022,Urine - 488022
PanelName: ABR Health Care CollectionCentre
Olivhealth,PathLab:UGF-5,Saran Chamber-1,5-Park Road, Hazratganj, Lucknow - 226001Ph:. 0522-4062197, Mob: +91-7526001103
Page 1 of10
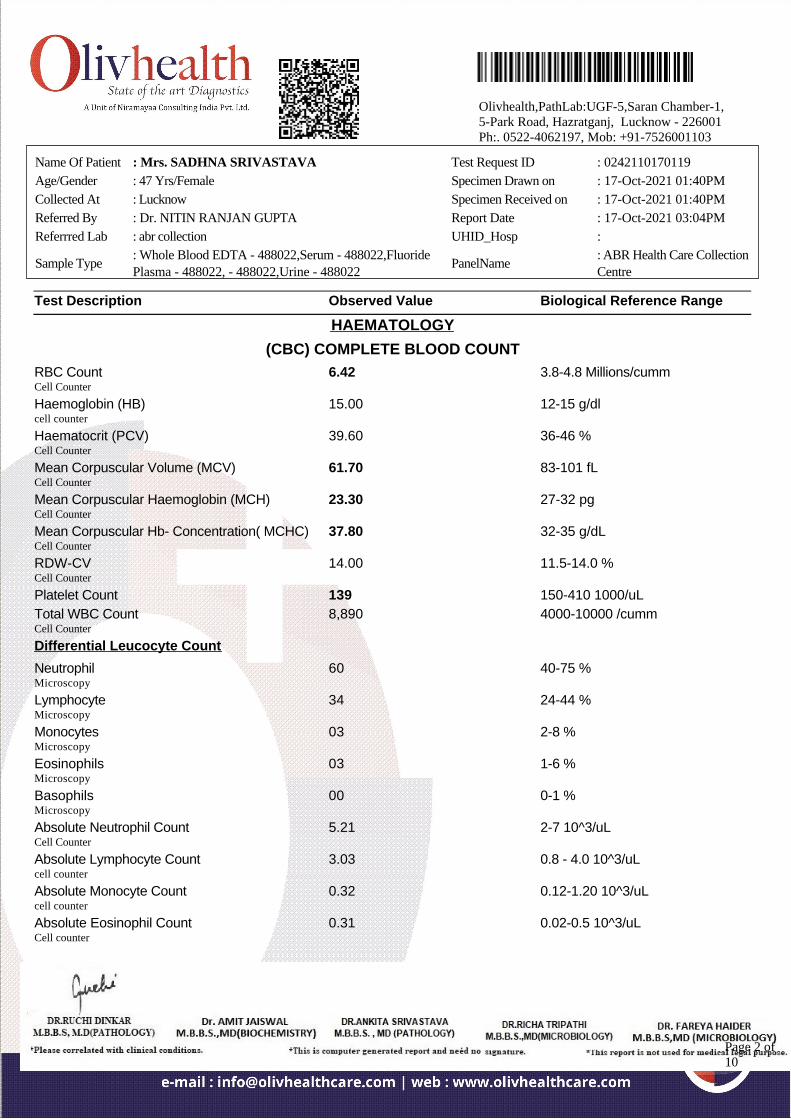
Test Description Observed Value Biological Reference Range
HAEMATOLOGY
(CBC) COMPLETE BLOOD COUNT
RBC CountCell Counter
6.42 3.8-4.8 Millions/cumm
Haemoglobin (HB)cell counter
15.00 12-15 g/dl
Haematocrit (PCV)Cell Counter
39.60 36-46 %
Mean Corpuscular Volume (MCV)Cell Counter
61.70 83-101 fL
Mean Corpuscular Haemoglobin (MCH)Cell Counter
23.30 27-32 pg
Mean Corpuscular Hb- Concentration( MCHC)Cell Counter
37.80 32-35 g/dL
RDW-CVCell Counter
14.00 11.5-14.0 %
Platelet Count 139 150-410 1000/uL
Total WBC CountCell Counter
8,890 4000-10000 /cumm
Differential Leucocyte Count
NeutrophilMicroscopy
60 40-75 %
LymphocyteMicroscopy
34 24-44 %
MonocytesMicroscopy
03 2-8 %
EosinophilsMicroscopy
03 1-6 %
BasophilsMicroscopy
00 0-1 %
Absolute Neutrophil CountCell Counter
5.21 2-7 10^3/uL
Absolute Lymphocyte Countcell counter
3.03 0.8 - 4.0 10^3/uL
Absolute Monocyte Countcell counter
0.32 0.12-1.20 10^3/uL
Absolute Eosinophil CountCell counter
0.31 0.02-0.5 10^3/uL
Name Of Patient : Mrs. SADHNA SRIVASTAVA Test Request ID : 0242110170119
Age/Gender : 47 Yrs/Female Specimen Drawn on : 17-Oct-2021 01:40PM
Collected At : Lucknow Specimen Received on : 17-Oct-2021 01:40PM
Referred By : Dr. NITIN RANJAN GUPTA Report Date : 17-Oct-2021 03:04PM
Referrred Lab : abr collection UHID_Hosp :
Sample Type: Whole Blood EDTA - 488022,Serum - 488022,FluoridePlasma - 488022, - 488022,Urine - 488022
PanelName: ABR Health Care CollectionCentre
Olivhealth,PathLab:UGF-5,Saran Chamber-1,5-Park Road, Hazratganj, Lucknow - 226001Ph:. 0522-4062197, Mob: +91-7526001103
Page 2 of10
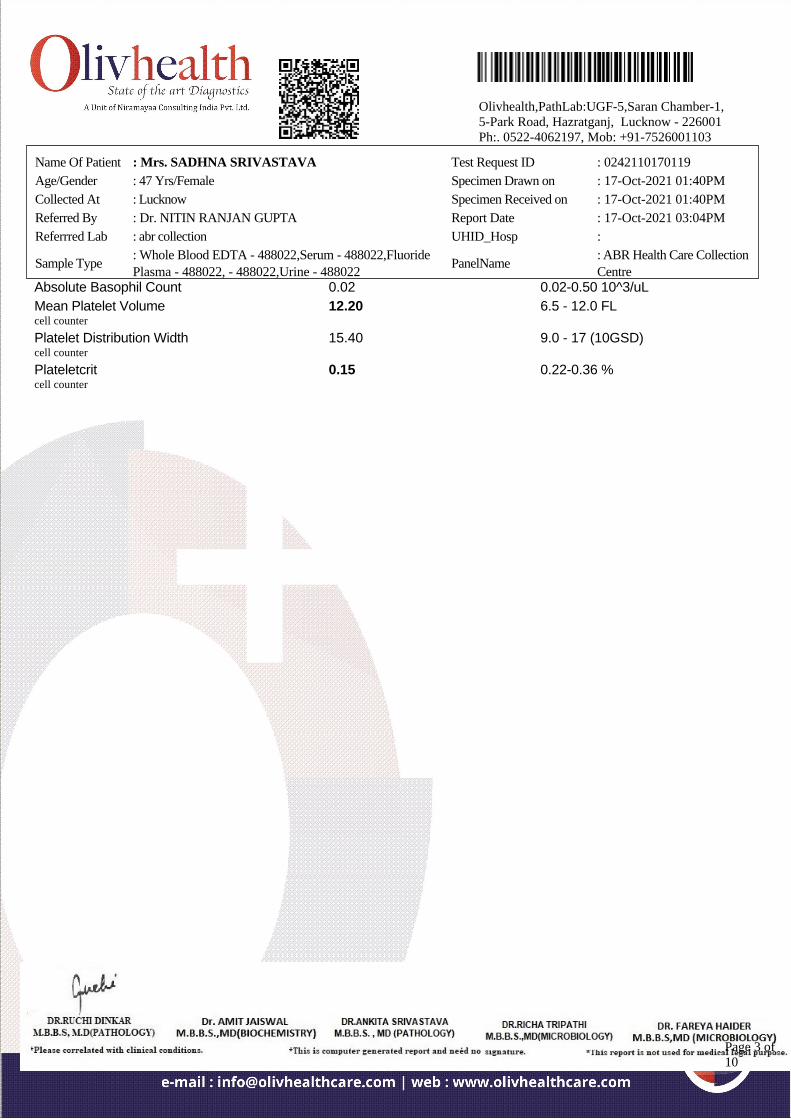
Absolute Basophil Count 0.02 0.02-0.50 10^3/uL
Mean Platelet Volumecell counter
12.20 6.5 - 12.0 FL
Platelet Distribution Widthcell counter
15.40 9.0 - 17 (10GSD)
Plateletcritcell counter
0.15 0.22-0.36 %
Name Of Patient : Mrs. SADHNA SRIVASTAVA Test Request ID : 0242110170119
Age/Gender : 47 Yrs/Female Specimen Drawn on : 17-Oct-2021 01:40PM
Collected At : Lucknow Specimen Received on : 17-Oct-2021 01:40PM
Referred By : Dr. NITIN RANJAN GUPTA Report Date : 17-Oct-2021 03:04PM
Referrred Lab : abr collection UHID_Hosp :
Sample Type: Whole Blood EDTA - 488022,Serum - 488022,FluoridePlasma - 488022, - 488022,Urine - 488022
PanelName: ABR Health Care CollectionCentre
Olivhealth,PathLab:UGF-5,Saran Chamber-1,5-Park Road, Hazratganj, Lucknow - 226001Ph:. 0522-4062197, Mob: +91-7526001103
Page 3 of10
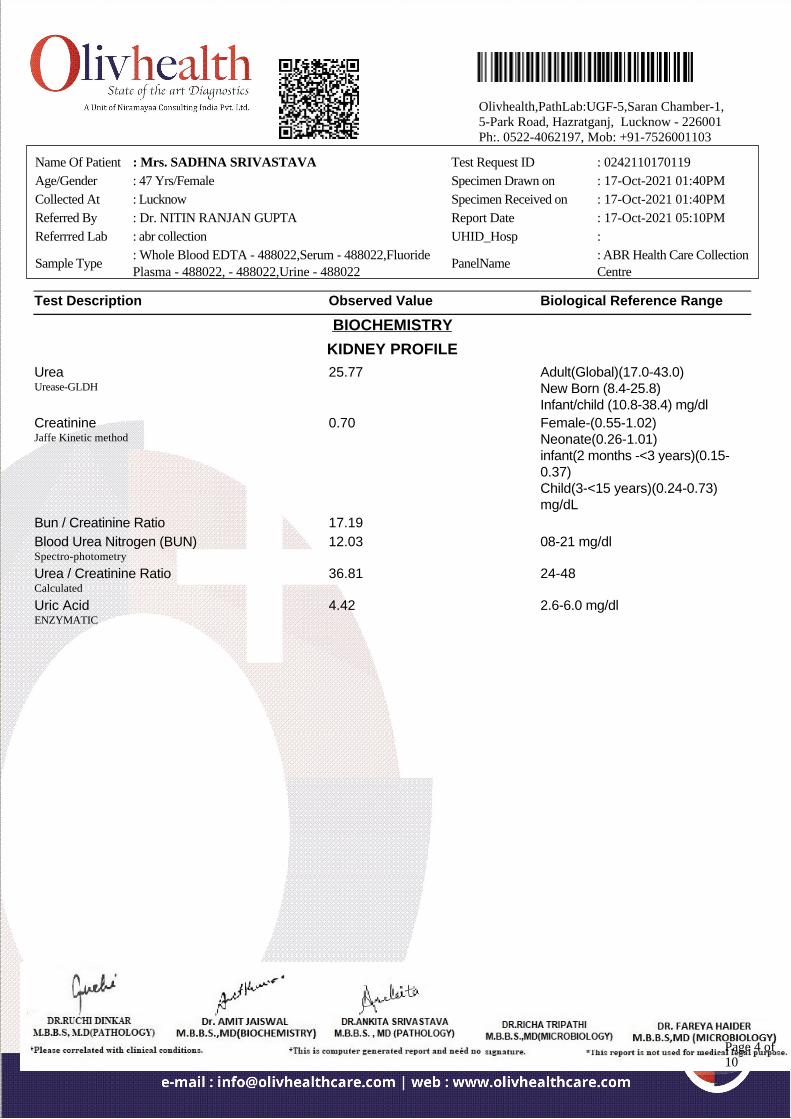
Test Description Observed Value Biological Reference Range
BIOCHEMISTRY
KIDNEY PROFILE
UreaUrease-GLDH
25.77 Adult(Global)(17.0-43.0)New Born (8.4-25.8)Infant/child (10.8-38.4) mg/dl
CreatinineJaffe Kinetic method
0.70 Female-(0.55-1.02)Neonate(0.26-1.01)infant(2 months -<3 years)(0.15-0.37)Child(3-<15 years)(0.24-0.73)mg/dL
Bun / Creatinine Ratio 17.19
Blood Urea Nitrogen (BUN)Spectro-photometry
12.03 08-21 mg/dl
Urea / Creatinine RatioCalculated
36.81 24-48
Uric AcidENZYMATIC
4.42 2.6-6.0 mg/dl
Name Of Patient : Mrs. SADHNA SRIVASTAVA Test Request ID : 0242110170119
Age/Gender : 47 Yrs/Female Specimen Drawn on : 17-Oct-2021 01:40PM
Collected At : Lucknow Specimen Received on : 17-Oct-2021 01:40PM
Referred By : Dr. NITIN RANJAN GUPTA Report Date : 17-Oct-2021 05:10PM
Referrred Lab : abr collection UHID_Hosp :
Sample Type: Whole Blood EDTA - 488022,Serum - 488022,FluoridePlasma - 488022, - 488022,Urine - 488022
PanelName: ABR Health Care CollectionCentre
Olivhealth,PathLab:UGF-5,Saran Chamber-1,5-Park Road, Hazratganj, Lucknow - 226001Ph:. 0522-4062197, Mob: +91-7526001103
Page 4 of10
Test Description Observed Value Biological Reference Range
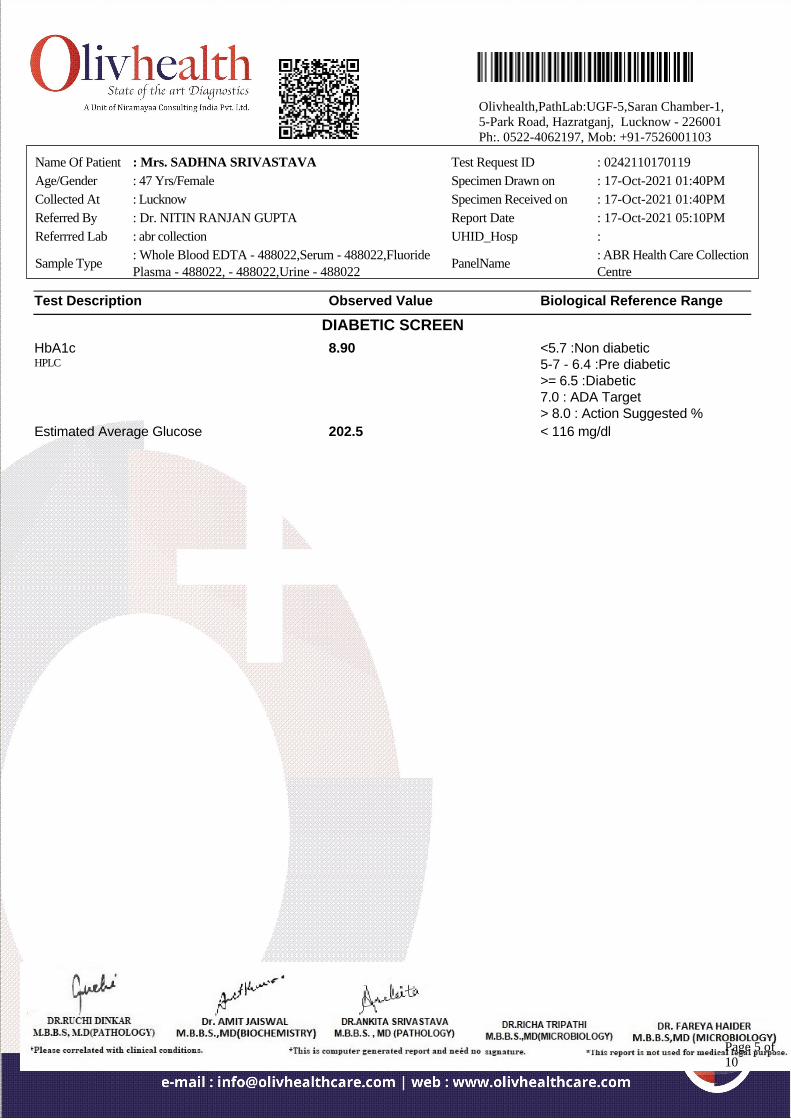
DIABETIC SCREEN
HbA1cHPLC
8.90 <5.7 :Non diabetic5-7 - 6.4 :Pre diabetic>= 6.5 :Diabetic7.0 : ADA Target> 8.0 : Action Suggested %
Estimated Average Glucose 202.5 < 116 mg/dl
Name Of Patient : Mrs. SADHNA SRIVASTAVA Test Request ID : 0242110170119
Age/Gender : 47 Yrs/Female Specimen Drawn on : 17-Oct-2021 01:40PM
Collected At : Lucknow Specimen Received on : 17-Oct-2021 01:40PM
Referred By : Dr. NITIN RANJAN GUPTA Report Date : 17-Oct-2021 05:10PM
Referrred Lab : abr collection UHID_Hosp :
Sample Type: Whole Blood EDTA - 488022,Serum - 488022,FluoridePlasma - 488022, - 488022,Urine - 488022
PanelName: ABR Health Care CollectionCentre
Olivhealth,PathLab:UGF-5,Saran Chamber-1,5-Park Road, Hazratganj, Lucknow - 226001Ph:. 0522-4062197, Mob: +91-7526001103
Page 5 of10
Test Description Observed Value Biological Reference Range
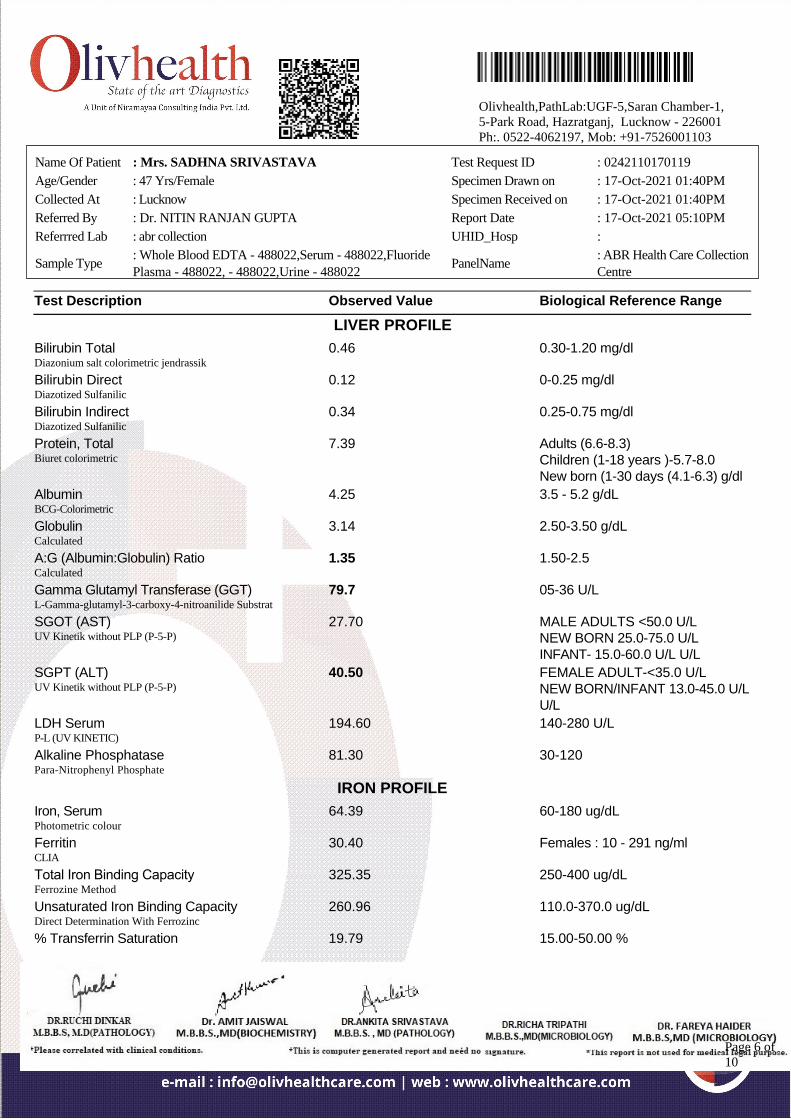
LIVER PROFILE
Bilirubin TotalDiazonium salt colorimetric jendrassik
0.46 0.30-1.20 mg/dl
Bilirubin DirectDiazotized Sulfanilic
0.12 0-0.25 mg/dl
Bilirubin IndirectDiazotized Sulfanilic
0.34 0.25-0.75 mg/dl
Protein, TotalBiuret colorimetric
7.39 Adults (6.6-8.3)Children (1-18 years )-5.7-8.0New born (1-30 days (4.1-6.3) g/dl
AlbuminBCG-Colorimetric
4.25 3.5 - 5.2 g/dL
GlobulinCalculated
3.14 2.50-3.50 g/dL
A:G (Albumin:Globulin) RatioCalculated
1.35 1.50-2.5
Gamma Glutamyl Transferase (GGT)L-Gamma-glutamyl-3-carboxy-4-nitroanilide Substrat
79.7 05-36 U/L
SGOT (AST)UV Kinetik without PLP (P-5-P)
27.70 MALE ADULTS <50.0 U/LNEW BORN 25.0-75.0 U/LINFANT- 15.0-60.0 U/L U/L
SGPT (ALT)UV Kinetik without PLP (P-5-P)
40.50 FEMALE ADULT-<35.0 U/LNEW BORN/INFANT 13.0-45.0 U/LU/L
LDH SerumP-L (UV KINETIC)
194.60 140-280 U/L
Alkaline PhosphatasePara-Nitrophenyl Phosphate
81.30 30-120
IRON PROFILE
Iron, SerumPhotometric colour
64.39 60-180 ug/dL
FerritinCLIA
30.40 Females : 10 - 291 ng/ml
Total Iron Binding CapacityFerrozine Method
325.35 250-400 ug/dL
Unsaturated Iron Binding CapacityDirect Determination With Ferrozinc
260.96 110.0-370.0 ug/dL
% Transferrin Saturation 19.79 15.00-50.00 %
Name Of Patient : Mrs. SADHNA SRIVASTAVA Test Request ID : 0242110170119
Age/Gender : 47 Yrs/Female Specimen Drawn on : 17-Oct-2021 01:40PM
Collected At : Lucknow Specimen Received on : 17-Oct-2021 01:40PM
Referred By : Dr. NITIN RANJAN GUPTA Report Date : 17-Oct-2021 05:10PM
Referrred Lab : abr collection UHID_Hosp :
Sample Type: Whole Blood EDTA - 488022,Serum - 488022,FluoridePlasma - 488022, - 488022,Urine - 488022
PanelName: ABR Health Care CollectionCentre
Olivhealth,PathLab:UGF-5,Saran Chamber-1,5-Park Road, Hazratganj, Lucknow - 226001Ph:. 0522-4062197, Mob: +91-7526001103
Page 6 of10
Spectrophotometry
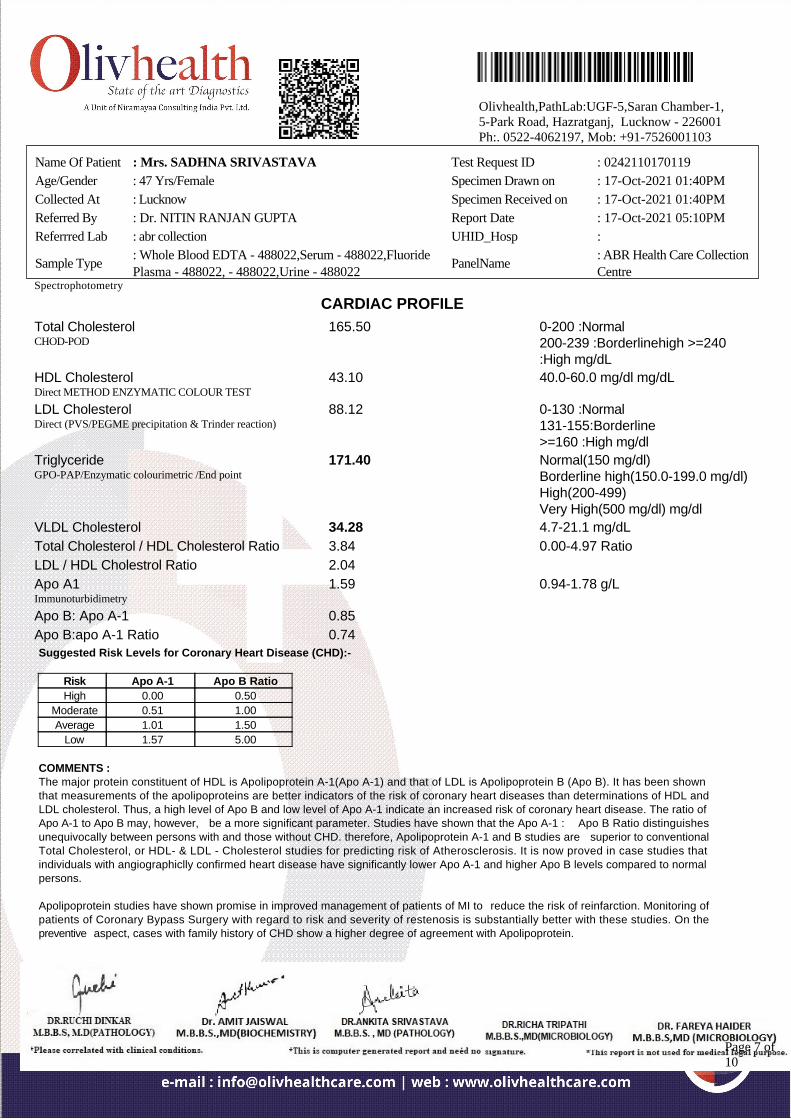
CARDIAC PROFILE
Total CholesterolCHOD-POD
165.50 0-200 :Normal200-239 :Borderlinehigh >=240:High mg/dL
HDL CholesterolDirect METHOD ENZYMATIC COLOUR TEST
43.10 40.0-60.0 mg/dl mg/dL
LDL CholesterolDirect (PVS/PEGME precipitation & Trinder reaction)
88.12 0-130 :Normal131-155:Borderline>=160 :High mg/dl
TriglycerideGPO-PAP/Enzymatic colourimetric /End point
171.40 Normal(150 mg/dl)Borderline high(150.0-199.0 mg/dl)High(200-499)Very High(500 mg/dl) mg/dl
VLDL Cholesterol 34.28 4.7-21.1 mg/dL
Total Cholesterol / HDL Cholesterol Ratio 3.84 0.00-4.97 Ratio
LDL / HDL Cholestrol Ratio 2.04
Apo A1Immunoturbidimetry
1.59 0.94-1.78 g/L
Apo B: Apo A-1 0.85
Apo B:apo A-1 Ratio 0.74
Suggested Risk Levels for Coronary Heart Disease (CHD):-
Risk Apo A-1 Apo B Ratio
High 0.00 0.50
Moderate 0.51 1.00
Average 1.01 1.50
Low 1.57 5.00
COMMENTS :The major protein constituent of HDL is Apolipoprotein A-1(Apo A-1) and that of LDL is Apolipoprotein B (Apo B). It has been shownthat measurements of the apolipoproteins are better indicators of the risk of coronary heart diseases than determinations of HDL andLDL cholesterol. Thus, a high level of Apo B and low level of Apo A-1 indicate an increased risk of coronary heart disease. The ratio ofApo A-1 to Apo B may, however, be a more significant parameter. Studies have shown that the Apo A-1 : Apo B Ratio distinguishesunequivocally between persons with and those without CHD. therefore, Apolipoprotein A-1 and B studies are superior to conventionalTotal Cholesterol, or HDL- & LDL - Cholesterol studies for predicting risk of Atherosclerosis. It is now proved in case studies thatindividuals with angiographiclly confirmed heart disease have significantly lower Apo A-1 and higher Apo B levels compared to normalpersons. Apolipoprotein studies have shown promise in improved management of patients of MI to reduce the risk of reinfarction. Monitoring ofpatients of Coronary Bypass Surgery with regard to risk and severity of restenosis is substantially better with these studies. On thepreventive aspect, cases with family history of CHD show a higher degree of agreement with Apolipoprotein.
Name Of Patient : Mrs. SADHNA SRIVASTAVA Test Request ID : 0242110170119
Age/Gender : 47 Yrs/Female Specimen Drawn on : 17-Oct-2021 01:40PM
Collected At : Lucknow Specimen Received on : 17-Oct-2021 01:40PM
Referred By : Dr. NITIN RANJAN GUPTA Report Date : 17-Oct-2021 05:10PM
Referrred Lab : abr collection UHID_Hosp :
Sample Type: Whole Blood EDTA - 488022,Serum - 488022,FluoridePlasma - 488022, - 488022,Urine - 488022
PanelName: ABR Health Care CollectionCentre
Olivhealth,PathLab:UGF-5,Saran Chamber-1,5-Park Road, Hazratganj, Lucknow - 226001Ph:. 0522-4062197, Mob: +91-7526001103
Page 7 of10
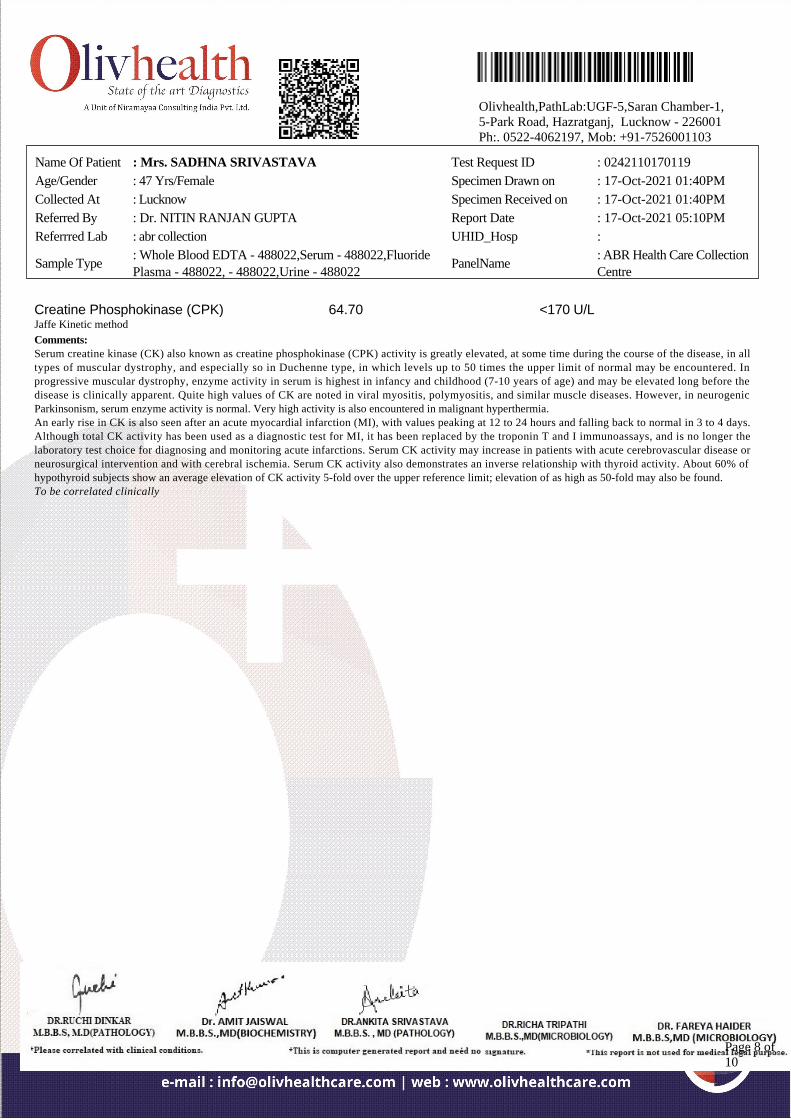
Creatine Phosphokinase (CPK)Jaffe Kinetic method
64.70 <170 U/L
Comments:Serum creatine kinase (CK) also known as creatine phosphokinase (CPK) activity is greatly elevated, at some time during the course of the disease, in alltypes of muscular dystrophy, and especially so in Duchenne type, in which levels up to 50 times the upper limit of normal may be encountered. Inprogressive muscular dystrophy, enzyme activity in serum is highest in infancy and childhood (7-10 years of age) and may be elevated long before thedisease is clinically apparent. Quite high values of CK are noted in viral myositis, polymyositis, and similar muscle diseases. However, in neurogenicParkinsonism, serum enzyme activity is normal. Very high activity is also encountered in malignant hyperthermia.An early rise in CK is also seen after an acute myocardial infarction (MI), with values peaking at 12 to 24 hours and falling back to normal in 3 to 4 days.Although total CK activity has been used as a diagnostic test for MI, it has been replaced by the troponin T and I immunoassays, and is no longer thelaboratory test choice for diagnosing and monitoring acute infarctions. Serum CK activity may increase in patients with acute cerebrovascular disease orneurosurgical intervention and with cerebral ischemia. Serum CK activity also demonstrates an inverse relationship with thyroid activity. About 60% ofhypothyroid subjects show an average elevation of CK activity 5-fold over the upper reference limit; elevation of as high as 50-fold may also be found.To be correlated clinically
Name Of Patient : Mrs. SADHNA SRIVASTAVA Test Request ID : 0242110170119
Age/Gender : 47 Yrs/Female Specimen Drawn on : 17-Oct-2021 01:40PM
Collected At : Lucknow Specimen Received on : 17-Oct-2021 01:40PM
Referred By : Dr. NITIN RANJAN GUPTA Report Date : 17-Oct-2021 05:10PM
Referrred Lab : abr collection UHID_Hosp :
Sample Type: Whole Blood EDTA - 488022,Serum - 488022,FluoridePlasma - 488022, - 488022,Urine - 488022
PanelName: ABR Health Care CollectionCentre
Olivhealth,PathLab:UGF-5,Saran Chamber-1,5-Park Road, Hazratganj, Lucknow - 226001Ph:. 0522-4062197, Mob: +91-7526001103
Page 8 of10
Test Description Observed Value Biological Reference Range
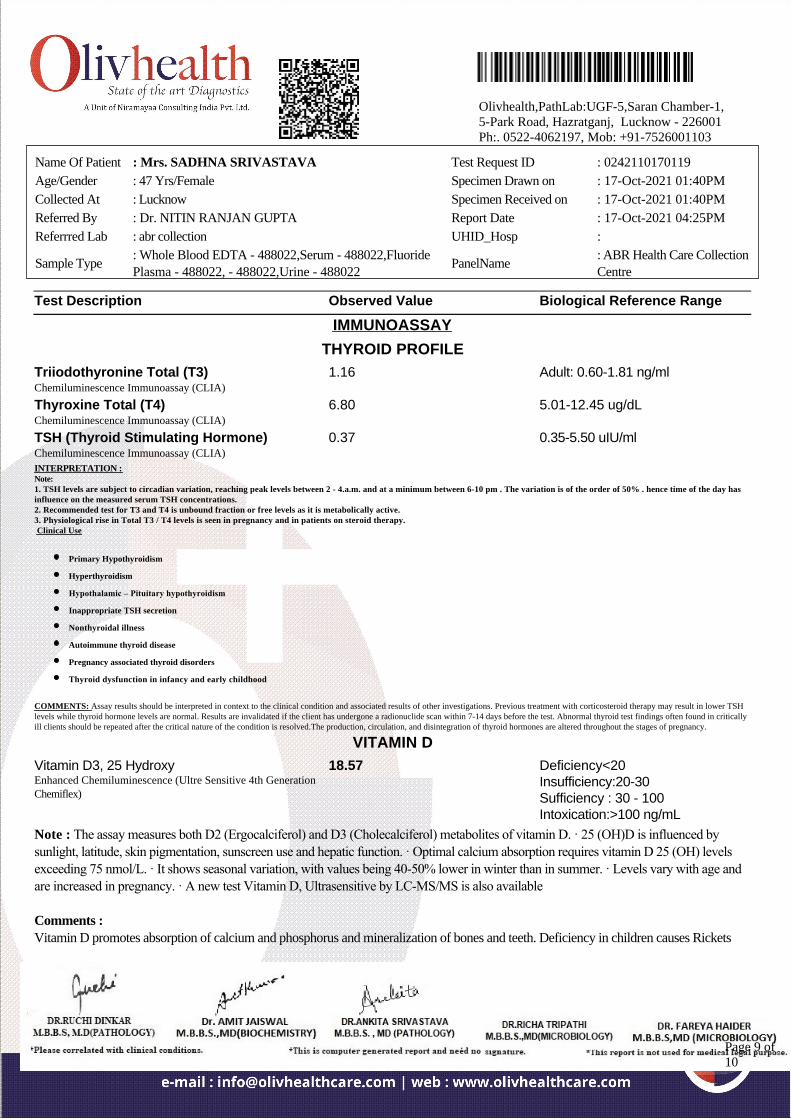
IMMUNOASSAY
THYROID PROFILE
Triiodothyronine Total (T3)Chemiluminescence Immunoassay (CLIA)
1.16 Adult: 0.60-1.81 ng/ml
Thyroxine Total (T4)Chemiluminescence Immunoassay (CLIA)
6.80 5.01-12.45 ug/dL
TSH (Thyroid Stimulating Hormone)Chemiluminescence Immunoassay (CLIA)
0.37 0.35-5.50 uIU/ml
INTERPRETATION :Note:1. TSH levels are subject to circadian variation, reaching peak levels between 2 - 4.a.m. and at a minimum between 6-10 pm . The variation is of the order of 50% . hence time of the day hasinfluence on the measured serum TSH concentrations. 2. Recommended test for T3 and T4 is unbound fraction or free levels as it is metabolically active.3. Physiological rise in Total T3 / T4 levels is seen in pregnancy and in patients on steroid therapy. Clinical Use
Primary Hypothyroidism
Hyperthyroidism
Hypothalamic – Pituitary hypothyroidism
Inappropriate TSH secretion
Nonthyroidal illness
Autoimmune thyroid disease
Pregnancy associated thyroid disorders
Thyroid dysfunction in infancy and early childhood
COMMENTS: Assay results should be interpreted in context to the clinical condition and associated results of other investigations. Previous treatment with corticosteroid therapy may result in lower TSHlevels while thyroid hormone levels are normal. Results are invalidated if the client has undergone a radionuclide scan within 7-14 days before the test. Abnormal thyroid test findings often found in criticallyill clients should be repeated after the critical nature of the condition is resolved.The production, circulation, and disintegration of thyroid hormones are altered throughout the stages of pregnancy.
VITAMIN D
Vitamin D3, 25 HydroxyEnhanced Chemiluminescence (Ultre Sensitive 4th GenerationChemiflex)
18.57 Deficiency<20Insufficiency:20-30Sufficiency : 30 - 100Intoxication:>100 ng/mL
Note : The assay measures both D2 (Ergocalciferol) and D3 (Cholecalciferol) metabolites of vitamin D. · 25 (OH)D is influenced bysunlight, latitude, skin pigmentation, sunscreen use and hepatic function. · Optimal calcium absorption requires vitamin D 25 (OH) levelsexceeding 75 nmol/L. · It shows seasonal variation, with values being 40-50% lower in winter than in summer. · Levels vary with age andare increased in pregnancy. · A new test Vitamin D, Ultrasensitive by LC-MS/MS is also available
Comments :
Vitamin D promotes absorption of calcium and phosphorus and mineralization of bones and teeth. Deficiency in children causes Rickets
Name Of Patient : Mrs. SADHNA SRIVASTAVA Test Request ID : 0242110170119
Age/Gender : 47 Yrs/Female Specimen Drawn on : 17-Oct-2021 01:40PM
Collected At : Lucknow Specimen Received on : 17-Oct-2021 01:40PM
Referred By : Dr. NITIN RANJAN GUPTA Report Date : 17-Oct-2021 04:25PM
Referrred Lab : abr collection UHID_Hosp :
Sample Type: Whole Blood EDTA - 488022,Serum - 488022,FluoridePlasma - 488022, - 488022,Urine - 488022
PanelName: ABR Health Care CollectionCentre
Olivhealth,PathLab:UGF-5,Saran Chamber-1,5-Park Road, Hazratganj, Lucknow - 226001Ph:. 0522-4062197, Mob: +91-7526001103
Page 9 of10
and in adults leads to Osteomalacia. It can also lead to Hypocalcemia and Tetany. Vitamin D status is best determined by measurement of
25 hydroxy vitamin D, as it is the major circulating form and has longer half life (2-3 weeks) than 1,25 Dihydroxy vitamin D (5-8 hrs)
*** End Of Report ***
Name Of Patient : Mrs. SADHNA SRIVASTAVA Test Request ID : 0242110170119
Age/Gender : 47 Yrs/Female Specimen Drawn on : 17-Oct-2021 01:40PM
Collected At : Lucknow Specimen Received on : 17-Oct-2021 01:40PM
Referred By : Dr. NITIN RANJAN GUPTA Report Date : 17-Oct-2021 04:25PM
Referrred Lab : abr collection UHID_Hosp :
Sample Type: Whole Blood EDTA - 488022,Serum - 488022,FluoridePlasma - 488022, - 488022,Urine - 488022
PanelName: ABR Health Care CollectionCentre
Olivhealth,PathLab:UGF-5,Saran Chamber-1,5-Park Road, Hazratganj, Lucknow - 226001Ph:. 0522-4062197, Mob: +91-7526001103
Page 10 of10