Embed Size (px)
DESCRIPTION
4th Annual Scalpel Undergraduate Surgical Conference (20 October 2012)
Citation preview

1

2
© Scalpel Surgical Society, October 2012
“A great day for the surgeons of tomorrow to begin their surgical journey...”
Prof. Averil Mansfield Scalpel Conference 2010

3
Contents
Welcome.....................................4 The Programme..........................5 Map of Rooms.............................6 Our Speakers..............................8 The Workshops ...........................8 Overview of Presentations.........9 Research Abstracts....................11 Audit Abstracts..........................18 Case Report Abstracts ..............23 Poster Abstracts....................... 29 Organising Committee .............38 Notes Pages...............................39
Scalpel Conference 2012

4
Welcome... ...from Grant Coleman, Scalpel president
Dear Colleagues, It is my pleasure to warmly welcome you all to our 4th annual national surgical conference here in Manchester. I hope that the day will have something to offer you all, and you leave our event with fond memories. I have been involved with the surgical society in some form for almost three years now, in which time I have seen the annual conference go from strength to strength, predominantly due to the enthusi-asm, determination and commitment of our delegates, which never ceases to impress me. This year promises to be a truly national event, with delegates coming from all across the UK (and further!). I do hope you will all enjoy getting to know similarly surgically minded students. I am quite excited about the programme we have to offer you this year. We are truly honoured to welcome Prof. Kay, Mr Kiely and Miss Fernandes, whom are all some of the most highly respected and pioneering surgeons in their respective fields. A few weeks ago myself and the rest of the committee had the difficult task of selecting what ab-stracts should be presented at the conference. I can safely say on behalf of the whole committee that we were overwhelmed at the quantity and quality of work submitted to us. Please feel free to sit in on any presentation session you wish, and explore the exciting selection of posters that will be on display in the main foyer. For those of you who are presenting work today, I would like to congratulate you, and I wish you the best of luck. I would like to finish by earnestly thanking our delegates, guest speakers, volunteers, sponsors and the Royal College of Surgeons of England for making this event possible. I would especially like to thank the rest of the Scalpel committee for their hard work and dedication over the last nine months. I hope you enjoy yourself, and I look forward to meeting as many of you as possible. Please do not hesitate to offer us any feedback or suggestions on any aspect of the day. Yours sincerely,
Grant Coleman Scalpel President

5
Our patrons
0800-0900 Registration
0900-0915 Presidential Greetings and Welcome
Grant Coleman (Scalpel President) and Mr Ian Pearce/ Prof McGrouther (Scalpel Patrons)
(Lecture Theatre A, 3rd Floor)
0915-1000 Hand Transplantation
Prof. Simon Kay
(Lecture Theatre A, 3rd Floor)
1000-1045 The Separation of Conjoined Twins
Mr Edward Kiely
(Lecture Theatre A, 3rd Floor)
1045-1100 Coffee (Foyer, Ground Floor)
1100-1200 Research Presentations (Room 4.210, 4th floor)
Audit Presentations (Room 4.212, 4th Floor)
Case Report Presentations (Room 3.205, 3rd Floor)
1200-1300 Practical Workshops —Session A Lunch
W1 W2 W3 W4 (Foyer, Ground Floor)
1300-1400 Lunch Practical Workshops —Session B
(Foyer, Ground Floor) W1 W2 W3 W4
1400-1500 Research Presentations (Room 4.210, 4th floor)
Audit Presentations (Room 4.212, 4th Floor)
Case Report Presentations (Room 3.205, 3rd Floor)
1500-1545 Poster Presentations, Coffee and Networking
(Foyer, Ground Floor)
1545-1645 How to get published
Public Speaking
Women In Surgery Debate:
“This house proposes that those who receive
organs should be or-gan donors them-
selves” Mr A. Raftery
(Lecture theatre A)
How to make a conference poster
Dr Halder Manchester
Orators
Exeter University (Fastbleep)
(4.212, 4th Floor) (4.213, 4.209,
4th Floor)
(4.210, 4th Floor) (4.211, 4th Floor)
1645-1730 Neurosurgery
Ms Helen Fernandes
(Lecture Theatre A, 3rd Floor)
1730-1745 Thanks, prize giving and conference close
Grant Coleman
1800 Conference Dinner
The Programme
Workshops Key: W1—Suturing Skills workshop (3.211, 3rd floor)
W2 – Advanced suturing and plastics Workshop (3.212, 3rd floor) W3 – Chest Drain Workshop (3.214, 3rd floor)
W4 – Laparoscopic Skills Workshop (3.213, 3rd floor)

6
Stairs Stairs
Ground Floor
Main Corridor
Lifts Lifts
Foyer:
Posters, Exhibitors and
Food
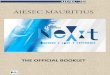
Room guide and Map Please note that the scalpel conference will take place on the ground, third and fourth floors only. Below is a list of what events are occurring in which rooms. All rooms should be clearly signposted as to what event is occurring within. If you have any queries about where to go, please do not hesitate to ask a member of the Scalpel committee. Ground Floor: Registration, Posters, Sponsor Exhibitors and Food 3rd Floor: Lecture Theatre A—Keynote lectures 3.205—Case report presentations 3.214— Chest drains workshops (W3) 3.213— Laparoscopic skills workshop (W4) 3.212—Plastics workshop (W2) 3.211—Suturing (W1) 4th Floor: 4.207—Scalpel committee room 4.209—Public speaking (academic workshop) 4.210—Women in Surgery (academic workshop), Research Presentations 4.211— How to make a conference poster (academic workshop), 4.212—How to get published (academic workshop) , Audit Presentations 4.213—Public speaking (academic workshop)
Canteen (unavailable)

7
Main Corridor
Lifts Lifts
Lecture Theatre A
Lower Entrance
3.211
3.214
3.213
3.212
3.205
3.210
3.209
Stairs Stairs
3rd Floor
Main Corridor
Lifts Lifts
Lecture Theatre A
Upper Entrance
4.212
4.209
4.210
4.211
4.207
4.213
4.214
Stairs Stairs
4th Floor

8
Our Speakers
Mr Edward Kiely, BAO (NUI), FRCSI , FRCS, FRCPCH (Hon) Consultant Paediatric General Surgeon, Great Ormond Street Hospital Mr Kiely has been based at Great Ormond Street Children's Hospital since the mid-1980s, and is considered one of the top surgeons in the world, specialising in the separation of conjoined twins. He has also appeared on the BBC2 documentary "Great Ormond Street". He has kindly agreed to speak today about the unique challenges that conjoined twin surgery can bring.
Professor Simon Kay , FRCS, FRCS (Plas) FRCSE (Hon) Consultant Plastic Surgeon, St James's University Hospital Simon Kay is a Consultant Plastic Surgeon and Professor of Hand Surgery in Leeds. His career lead him to be President of two specialty association, and editor of a major journal, but has remained focused on the human aspects of what are very technical specialties. His main expertise lies in microsurgery and reconstruction, and he will be talking on the whole gamut of upper limb reconstruction culminating in his current interest in hand transplantation .
We are honoured to welcome the following key note speakers to this years programme:
Miss Helen Fernandes, MBBS FRCS (Sn) MD Consultant Neurosurgeon, Addenbrooke's Hospital NHS Trust Helen Fernandes was appointed as Consultant Neurosurgeon at the interna-tionally renowned Addenbrooke's Hospital in Cambridge in 2002, the first female surgeon to be appointed there. She specialises in both the treatment of adult and paediatric patients with brain and spinal problems. Miss Fernandes has kindly agreed to address the conference on her surgical work, and also assist with the women in surgery workshop, a topic she is passionate about.
The Workshops Thanks to a wide range of volunteer professionals, we are delighted to offer so many workshops for your enjoyment. Unfortunately there are limited spaces in each workshop, therefore you may not pick and choose today which ones you attend, like you can do with other parts of the day (such as the presen-tations). Prior to the conference you should have received an email requiring you to sign up to one practical and one academic workshop. These choices should be highlighted on your personal timetable, which should be in the delegate packs. If you are unsure as to what workshops you are going to please don't hesitate to ask a member of the scalpel committee.

9
Abstract guide Overview of presentations
Research Presentations:
Morning Session (11:00-12:00, Room 4.210):
R1 - Benjamin Davies— “Lack of correlation between a histological and a qualitative radiologi-cal grading system of human intervertebral disc degeneration”
R2 - Mitchell Foster – “Cranioplasty: Is Earlier Better?” R3 - Priyanga Balendran – “Endothelial Cell Migration in the Presence of an Electrical Field” R4 - Anam Ashraf – “Pain after Total Knee Replacement. A Randomised Controlled Trial of local
infiltration versus single shot femoral nerve block” R5 - Rafail Angelos Kotronias – “Predictors and impact of prosthesis-patient mismatch after
transcatheter aortic valve replacement with CoreValve and SapienXT valves”
Afternoon Session (14:00-15:00, Room 4.210):
R6 - Ebrahim Mulla – “Myocardial oxidative-nitrosative stress in patients with type 2 diabetes mellitus undergoing coronary artery bypass grafting”
R7 - Michael Brockway –“Anatomical Structures related to Common Peroneal Nerve Entrap-ment”
R8 - Jessica Roth – “Critical Limb Ischaemia: Can we frame a window of opportunity?”
R9 - Aleksandra Szczap –“Renal function after mitral valve surgery performed with minimally invasive vs. conventional sternotomy approach.”
R10 - Jade Whing – “Clinical Significance of Neurovascular Variations Associated with the Short Saphenous Venous System. An Anatomical Study”
Audit Presentations:
Morning Session (11:00-12:00, Room 4.212):
A1 - Emily Decker – “Ruptured Abdominal Aortic Aneurysms: A Single Centre Experience at the Dawn of the IMPROVE Trial”
A2 - Catherine Lunter – “Transsylvian Selective Amygdalohippocampectomy: The Impact of Sur-gery on Memory Functioning in Patients with Medically Refractory Medial Temporal Lobe Epi-lepsy.”
A3 - Tom Robinson – “An audit of paediatric shunt infection and failure rates”
A4 - Robert Ford –“Audit at Bradford Royal Infirmary: Secondary Prevention of Post-Menopausal Osteoporotic Fragility Fractures (The Recommending of Appropriate Patients For DXA Scanning or Commencement of Osteoporosis Treatment)”

10
Afternoon Session (14:00-15:00, Room 4.212):
A5 - Jun Wei Lim –“Effect of Tranexamic Acid (TXA) on Wound Discharge After Primary Total Knee Replacement (TKR)”
A6 - Michael Harrison – “An Audit of Open, Laproscopically assisted and Minimally Invasive Oesophagectomies in a UK Cancer Treatment Centre”
A7 - Nicola Wright – “Lymph Node Harvest as a Marker of Quality in Colon Cancer Resection: A Comparison Between Laparoscopic and Open Resections”
A8 - William Cook – “Adherence to the British Society of Gastroenterology guidelines for man-agement of acute pancreatitis in North Bristol”
Case Report Presentations:
Morning Session (11:00-12:00, Room 3.205):
C1 - Sarah Fendius – “A Giant Thymic Cyst Mimicking a Large Pleural Effusion”
C2 - Carla Harris – “Body Contouring - Is it worth the weight?”
C3 - Seji Angel Jung – “Management of open abdomen following abdominal compartment syn-drome in a child: A case report”
C4 - Vijay Pattni – “An unusual presentation of an infected vallecular cyst presenting as acute supraglottitis.”
C5 - Jun Wei Lim – “Distal Femoral Replacement in Complex Revision of Femoral Component for Peri-prosthetic Fracture: A Case Report”
Afternoon Session (14:00-15:00, Room 3.205):
C6 - John Kan –“ Avascular necrosis of the femoral head following a previous diagnosis of aplas-tic anaemia”
C7 - Iheukwumere Duru – “Coronary Artery Bypass Grafting with Y-type Saphenous Vein: A Case Report highlighting the associated intra-operative benefits.”
C8 - Patrick Robinson - “Tuberculosis a real and present danger: Psoas Abscess presenting as ‘sciatica’.”
C9 - Shabnam Javed – “Recent advances in the management of patients with severe aortic stenosis- A case presentation”
Posters
All posters will be displayed in the foyer on the ground floor, and can be viewed throughout the day. Offi-cial presentation and marking will take place between 15:00-15:45. If you are presenting a poster please be around your board by 15:00.
P1 - John Connelly – “Audit of local recurrence following conventional APER for low rectal can-cer”
P2 - Benjamin Davies - “The changing phenotype of the nucleus pulposus with degeneration”
P3 - Muzzamil Hussain – “Optimisation of Silk Conduits by Degumming and Their Regenerative Potential Following Peripheral Nerve Injury in Adult Rats”

11
P4 - Christina Davies – “Carotid artery dissection in association with a minimally displaced C2 fracture: a case report”
P5 - Clarissa Gurbani – “Lung Transplantation as a Treatment for Idiopathic Pulmonary Hyper-tension: A Case Report”
P6 - Daniel Gibney - “Necrotising Fasciitis: The patient was telling us the diagnosis all along.”
P7 - Tamsyn Clark - “Transcatheter aortic valve implantation: Hope for ‘high risk’ patients.”
P8 - Nyan Su – “C-type Natriuretic Peptide receptors in the Cartilage of Patients with Os-teoarthritis”
P9 - Adrien Yvon – “Laparoscopic Roux-en-Y gastric bypass in an obese patient: a case report. Hospital Clinico San Carlos, Madrid.”
P10 - Rehan Al-Biatty – “Anatomical variation in the inferior pancreaticoduodenal arteries and its relevance to pancreas transplantation”
P11 - Thomas Forshaw - “Can we delay first stoma bag change postoperatively? An observa-tional cohort study”
P12 - Oliver Beaumont – “The quality of operation notes in orthopaedic trauma surgery: An audit in the Bristol Royal Infirmary, 2012”
P13 - Sophia Mahboob – “The Heart-Team Experience in the Management of Patients with Ischaemic Heart Disease”
Abstracts
Research Presentations
R1. Benjamin Davies - University of Manchester
“Lack of correlation between a histological and a qualitative radiological grading system of human in-tervertebral disc degeneration”
B.Davies, University of Manchester, R.Atkinson, SRFT, F.Ludwinski, University of Manchester K.Gnanalingham, SRFT; Prof.T.Freemont University of Manchester; Prof. J.Hoyland University of Manches-ter
Introduction:
Intervertebral disc (IVD) degeneration is a significant cause of back pain. Investigative research relies on comparative observations at different stages of degeneration and there are several qualitative histological and radiological grading systems of IVD degeneration. The relationship between histological and MR grades of human IVD degeneration is poorly understood.
Objective:
To investigate the relationship between the Pfirrmann [2000] radiological system of grading with the Sive et al [2002] histological grades in human cervical and lumbar degenerate discs. Method: Human lumbar (N=104) and cervical (N=112) IVD samples, obtained from patients undergoing discectomy, were assessed using a histological grading system, as per Sive et al [2002]. The corresponding pre-operative MR scans were also assessed as per Pfirrmann et al [2000]. Correlation was assessed using Spearman’s test.
Results:

12
No correlation was identified between the histological and MR grades in cervical (rho = 0.075; P=0.448) or lumbar (rho =0.161; P=0.109) discs.
Conclusions:
In human cervical and lumbar IVD degeneration, qualitative histological and MR grading systems may not be directly comparable, and they may also be measuring differing aspects of IVD degeneration. More quantitative grading systems may be useful in this respect.
R2. Mitchell Foster - University of Manchester
“Cranioplasty: Is Earlier Better?”
M Foster. Supervisor: G Hall, Royal Preston Hospital
The optimum time frame for cranioplasty following decompressive craniectomy has not been established. Early insertion (< 3-months) has been associated with higher infection rates, yet is thought to enhance rehabilitation. This study aimed to assess whether early cranioplasty is both safe, and associated with su-perior functional outcomes compared to late cranioplasty.
The case notes of 69 patients that received cranioplasty between 2006 and 2011 at a single centre were analysed, comparing infection risk with time to cranioplasty. In 51 patients, Glasgow Outcome Scores (GOS), a measure of functional outcome, were derived from clinical notes at intervals of 3, 6 and 12 months following craniectomy and compared against time to cranioplasty
Cranioplasty insertion time was not associated with graft infection rates or functional outcome, regardless of standardising patients by the mechanism of injury or their own relative GOS improvement.
Because too few patients in this centre had cranioplasty within 3-months (early cranioplasty) it was not possible to establish whether infection rate or functional outcome differed with that of late cranioplasty. In isolation, this study is therefore inconclusive. However, results suggest that cranioplasty before 6-months is safe (in contrast to recent advice that it should be delayed until after this point). Furthermore, once the cranioplasty has been delayed by 3-months, earlier insertion has no effect on functional out-come; the beneficial effects of the 3-month ‘early’ window observed in a recent publication may be lost by delaying beyond this point.
R3. Priyanga Balendran - Barts and the London School of Medicine and Dentistry
“Endothelial Cell Migration in the Presence of an Electrical Field”
W. Wang, W.Q. Li, P. Balendran
Cell migration is a several stage process but its functions endogenously are numerous. It is involved in em-bryonic morphogenesis, tissue repair and regeneration as well as driving disease progression in the metas-tasis of cancer. Recent work has implied that angiogenesis, which involves directional cell migration, is closely associated with endogenous electric fields (EF) (Ridley et al., 2003).
The wound healing model protocol involves setting up the electrical chamber, where a voltage is applied. A layer of endothelial cells are wounded by making a scratch, which has the width of approximately 200 micrometres.

13
These cells are treated with an electrical charge of 5 volts over the duration of two hours in the chamber and an image taken every five minutes.
In conclusion, when the cells were placed under an electric field it was noted that that they underwent morphological changes in response to the electrical field as well as being able to move towards the anode. When compared to the control, where the cells had not undergone any electrical stimulation, there was little or random movement. To further reinforce migration under the presence of an electric field, active membrane ruffling was also observed as well as elongation. This arises to the concept of electric fields guiding angiogenesis in endothelial cells.
R4. Anam Ashraf - University of Manchester
“Pain after Total Knee Replacement. A Randomised Controlled Trial of local infiltration versus single shot femoral nerve block”
A. Ashraf, S. Canty, V. Raut, G. J. Mclauchlan Dept. Of Orthopaedics, Lancashire Teaching Hospitals, Pre-ston, United Kingdom
Background:
Pain is a significant factor following Total Knee Replacement (TKR). Multiple modalities can be used to re-duce it. There are no studies of local joint infiltration versus single shot femoral nerve block. Objectives:
We conducted an ethically approved prospective blinded randomised trial. The objective was to identify whether local infiltration gave better postoperative pain relief compared to standard practice of single shot femoral nerve block.
Methods:
40 patients undergoing a primary TKR underwent a standardised spinal anaesthetic and where then ran-domised to the femoral nerve block group or infiltration group. Outcomes measured included post-operative pain scores, pain scores before and after physiotherapy on post-operative day 1, total analgesia used post-operatively, time to achieve physiotherapy goals and length of stay in hospital. Statistical analysis was primarily using a Mann-Whitney test.
Results:
The local infiltration group had significantly lower pain scores at four hours post-operatively (mean [SD] 2.1[2.6] vs 6.8[3.2], p<0.00001) and on post-operative day one prior to physiotherapy (mean [SD] 2.4[2.3] vs 4.4[2.3], p<0.05). Total opiate use was also significantly lower in the local infiltration group (115[50.3] mg vs 176.5[103.5] mg, p<0.01).There was no difference in pain after physiotherapy on day 1 postopera-tively, the achievement of physiotherapy goals or length of hospital stay.
Conclusion:
Intraoperative infiltration gives superior pain relief over the first 24 hours following primary TKR. Further-more, it is also superior in minimising post-operative opiate use. It doesn’t improve time to achieve physiotherapy goals or reduce length of stay compared to single shot femoral nerve block.

14
R5. Rafail Angelos Kotronias - Keele University
“Predictors and impact of prosthesis-patient mismatch after transcatheter aortic valve replacement with CoreValve and SapienXT valves”
R. A. Kotronias, Supervisor: Konstantinos Stathogiannis Clinical Assistant in First Department of Cardiology, Hippokration Hospital, Athens, Greece
Objectives:
To evaluate the significance and impact of prosthesis-patient mismatch after transcatheter aortic valve replacement.
Background:
Prosthesis-patient mismatch (PPM) is an important determinant of morbidity and mortality following sur-gical aortic valve replacement. However, its importance in transcatheter aortic valve replacement (TAVR) is not well defined. The objective of this study was to examine the incidence and predictors of PPM after TAVR with CoreValve (MCV) and SapienXT (EXT) valves.
Methods:
Clinical and echocardiographic parameters were recorded at baseline and prior to discharge in patients undergoing TAVR with the MCV or the EXT valves within a multicenter prospective registry. PPM was de-fined as indexed effective orifice area (EOAi) ≤0.85cm2/m2(severe if ≤0.65cm2/m2).
Results:
A total of 137 patients were evaluated. The EOAi increased from 0.37±0.10cm2/m2 to 0.93±0.28 cm2/m2 (p≤0.001) after TAVR. Fifty-seven patients (42%) had PPM [severe in 6 (7%)]; PPM was observed in 45% of MCV (severe in 8%) and in 37% of EXT (severe in 5%) valves (p=0.21). Predictors of PPM were pre proce-dural EOAi in MCV (OR 0.002, 95% CI 0.001 to 0.688), and pre procedural pulmonary artery systolic pres-sure (OR 0.954, 95% CI 0.913to 0.996) and ejection fraction (OR 0.951, 95% CI: 0.904 to 0.999) in EXT.
Conclusions:
The entity of PPM is frequently seen after TAVR with both available prosthetic valves. The predictors of PPM differ between the MCV and the EXT valve. The clinical significance of PPM following TAVR requires further investigation.
R6. Ebrahim Mulla - University of Birmingham
“Myocardial oxidative-nitrosative stress in patients with type 2 diabetes mellitus undergoing coronary artery bypass grafting”
E. Mulla, The University of Birmingham, A. Menon , University Hospital Birmingham, S Hughes, The Univer-sity of Birmingham. R. Bonser, University Hospital Birmingham, M. J. Stevens, The University of Birming-ham
Introduction:
Type 2 diabetes mellitus (T2DM) is associated with worse mortality and morbidity after coronary artery bypass grafting (CABG). The reasons for this are currently unclear, but it may be a result of oxidative dam-age and autonomic changes in the diabetic heart.

15
Purpose:
The aim of this study was to determine the association between myocardial oxidative stress, autonomic dysfunction and post-CABG outcomes in T2DM.
Method:
In 28 T2DM and 20 non-T2DM, tissue oxidative stress was measured using poly-ADP ribose polymerase (PARP) immunohistochemical staining from right atrial biopsies. Cardiac autonomic neuropathy (CAN) was assessed using heart rate variability tests and plasma oxidative stress was measured using protein carbonyl and nitrotyrosine ELISA. These were all correlated with indirect measures of post-CABG out-comes, specifically peri-operative arrhythmias, troponin and albumin creatinine ratio.
Results:
Mean PARP activation was significantly higher in T2DM compared to non-T2DM (71.0% [95%CI: 65.2-76.86%] vs. 45.2% [95%CI: 38.6-51.8%], (p<0.001, n=48). PARP in T2DM was positively correlated with 6 hr Troponin ([ρ] =0.517, p=0.017, n=21) and 48 hr Troponin ([ρ] =.490, p=0.039, n=18). Plasma protein carbonyl concentration was significantly higher in T2DM compared to non-T2DM at 12, 24 and 48 hours after CABG (p<0.05, n=14). CAN was identified in 69% of diabetics (n=23).
Conclusion:
This data suggests that myocardial oxidative stress is associated with worse post-CABG outcomes in T2DM, but the role of autonomic dysfunction remains to be determined. Interventions which reduce myocardial oxidative stress are likely to be of benefit in this population.
R7. Michael Brockway - University of Leeds
“Anatomical Structures related to Common Peroneal Nerve Entrapment”
M. Brockway, Supervisor S. Nunn, University of Leeds
Background:
Anatomical structures at the fibular neck may cause or contribute to Common Peroneal Nerve (CPN) en-trapment, characterised by pain, muscle weakness, dysesthesias and reduced or absent sensation in the lateral leg and dorsal foot. Insufficient release of these structures during surgical decompression predis-poses to recurrence of symptoms. Previous literature discusses such structures but lacks illustration and clarity to aid surgical understanding.
Purpose:
This study aimed to illustrate and describe anatomical structures which could cause or contribute to CPN entrapment.
Methods:
Three cadaveric lower limbs were finely dissected and an observational study conducted. Relevant struc-tures were photographed, described and compared with previous literature.
Results:

16
Several structures at the fibular neck which may cause or contribute to CPN entrapment were identified: 1. A tight fascial layer, at the fibular head, which the CPN passes deep to and which is continuous with fas-cia overlying biceps femoris and soleus. 2. A fibrous arch surrounding the CPN at the origin of peroneus longus, continuous with soleus and peroneus longus fibres. 3. Peroneus longus muscle fibres taking origin from the fibular shaft around the CPN. 4. An unyielding aperture, through which branches of the CPN passed, present within the intermuscular membrane between the anterior and lateral leg muscle com-partments.
Conclusion:
The narrow openings within these structures, through which the CPN passes, contribute to entrapment. The continuity of all these structures with surrounding muscles may promote dynamic exercise-induced entrapment. Further investigation could identify patient groups at increased risk of CPN entrapment.
R8. Jessica Roth – University of Manchester
“Critical Limb Ischaemia: Can we frame a window of opportunity?”
J. Roth
Background:
University Hospital of South Manchester (UHSM) started the Critical Limb Ischaemia Audit in January 2012, on behalf for Vascular Governance North West (VGNW). The principal aim was to research and audit local standards of service provision. The project developed into research of the relationship between the time taken to initiate treatment and patient outcomes, with limb salvage the principal marker of success. Method:
Data was collected using a proforma approved by VGMW for 74 out of a total of 220 patients submitted for audit by the vascular surgical team. Diagnostic standards, patient demographics, treatment times, types and outcomes were analysed as an interim report.
Results:
77% of patients were known arteriopaths diagnosed during outpatients surveillance appointments; inpa-tient treatment for chronic presentations took up to 6 months. 33% presented to A&E where they were admitted to commence treatment the same day. Time between presentation and commencement of treatment was 9 days for angioplasty, on average 17 days for conservative/lysis/bypass treatments and 23 days for amputation procedures. However, only 50% patients with conservative treatments had limb sal-vage at discharge, compared with 100% lysis patients, 88% angioplasty patients and 67% bypass patients. Conclusion:
Future data collection and NICE guidelines should stratify acceptable treatment times depending on set-ting of presentation and causative factors. Angioplasty with stenting was the most frequently used surgi-cal treatment, also producing the highest rate of limb salvage at discharge. However limb salvage is not a discrete indicator of successful treatment because it does not measure limb functionality.
R9. Aleksandra Szczap - University of Bristol
“Renal function after mitral valve surgery performed with minimally invasive vs. conventional ster-notomy approach.”
A Szczap, F Ciulli, G Asimakopoulos.

17
Background:
Patients undergoing mitral valve surgery frequently sustain renal injury. This study examines the hypothe-sis that minimally invasive mitral valve repair (MIMVR) is associated with lesser degree of renal injury as compared with mitral valve repair through sternotomy (MVR).
Methods:
This study evaluates data from all isolated MVRs performed at our institution. Data were collected using prospective database. There were 27 patients undergoing MIMVR and 170 undergoing MVR. Renal func-tion at day 1,4,7 and pre-operatively was measured. A secondary analysis with the populations divided into normal (eCrCl>50mL/min) and compromised pre-operative renal function (eCrCl<50mL/min) was per-formed.
Results:
The groups were similar with regards to age, gender, BMI, EuroSCORE, angina and dyspnoea, heart rhythm, LVF, previous MIs, PCIs, diabetes, hypertension, smoking, pulmonary disease, hospitalization length, in-hospital death, heamofiltration and re-operation.(P>0.05).
Renal function improved in both groups between pre-operatively and day 4.(P<0.05). There was no signifi-cant difference between groups in terms of plasma creatinine levels pre- and post-operatively (values for MIMVR vs. MVR: 104.0 vs.105.5, 103.8 vs.104.0, 97.6 vs.100.0 and 103.4 vs100.0 umol/L pre-operatively, on day 1, 4 and 7 respectively. P>0.05 for all) and creatinine clearance values (values for MIMVR vs. MVR: 62.7 vs. 64.5, 65.9 vs. 65.9, 70.5 vs. 70.4 and 61.3 vs. 69.0 ml/min pre-operatively, on day 1, 4 and 7 re-spectively. P>0.05 for all). The above observation was also valid for compromised pre-operative renal function group.
Conclusion:
Overall, MVR does not result in significant renal dysfunction. There is no difference in renal function be-tween patients undergoing MIMVR and MVR.
R10. Jade Whing – University of Manchester
“Clinical Significance of Neurovascular Variations Associated with the Short Saphenous Venous System. An Anatomical Study”
J. Whing, Prof Baguneid Department of Vascular Surgery, University Hospital South Manchester
Background:
Nerve damage following varicose vein surgery is the largest cause of medicolegal claims against vascular surgeons in the UK. Surgery on the short saphenous vein (SSV) is particularly associated with this risk, due to its variable anatomy and close relationship to the sural nerve (SN) and common peroneal nerve (CPN).
Aim:
To determine the relationship between the SSV and the surrounding neurological structures, in order to identifying regions potentially prone to damage during venous surgery.
Method:
The posterior aspect of the lower limb was dissected in 17 cadavers. Measurements were taken between the SSV and SN at fifths along the distance between anatomical landmarks; lateral malleolus (LM) to saphenopopliteal junction (SPJ), lateral femoral epicondyle (LFE) and union of SN. The distance from the SPJ to the CPN and LFE was also measured.

18
Results:
Between the LM and SPJ the SN was posterior in 42.9% (6/14) at the level of the LM and in 63.4% (9/14) at the 3/5th’s position. The median lateral distance from the SSV ranged from 1.94mm and 0.9mm at the LM and 1/5th position to 3.3mm to 5.4mm between the 2/5th’s portion and the level of the SPJ. For normal level SPJ terminations the mean horizontal distance to the CPN was 12.4mm. Conclusion: The relationship between the SSV and the surrounding nerves is variable. The SN is at risk of damage at the LM and 3/5th’s position. The CPN is at reduced risk of damage when disconnecting low SPJs, whilst the SN is at increased risk.
Audit Presentations
A1. Emily Decker, University of Leeds
“Ruptured Abdominal Aortic Aneurysms: A Single Centre Experience at the Dawn of the IMPROVE Trial”
E Decker (1), S Winward (1), MA Bailey (2,3), KJ Griffin (2,3), DJA Scott (2,3) 1. Leeds University Medical School, Leeds, UK 2. Division of Cardiovascular & Diabetes Research, LIGHT Laboratories, Leeds, UK 3. Leeds Vascular Institute, Leeds Teaching Hospitals Trust, Leeds UK
Background:
Emergency endovascular repair (eEVAR) of ruptured abdominal aortic aneurysms (rAAA) has been associ-ated with better outcomes than emergency open repair (eOR). In the absence of a randomised control trial, does this reflect a superior technique or patient selection bias?
Objective:
A retrospective single centre study of eEVAR and eOR for rAAA between 2006-2009 was undertaken. Pri-mary outcomes were mortality and hospital stay. Patient selection bias was also analysed. All patients were followed for 2 years post-op, or until death.
Method:
Patients were identified (n=86) retrospectively from a prospectively maintained database and notes ob-tained (EVAR n=20, OR n=29). Data was collected specifically examining patient demographics, cardiovas-cular risk factors, medications, A&E observations, CT findings, procedural details, post-operative hospital stay and mortality. These variables were then compared using non-parametric statistics.
Results:
There were significant differences between the two groups in terms of Glasgow aneurysm score (eOR=87, eEVAR=79.5, p=0.019), pre-operative systolic BP (eOR= 104.5mmHg, eEVAR=116.5mmHg, p=0.038), ICU stay (eOR=3 days, eEVAR=1 day, p<0.001) and HDU stay (eOR=2 days, eEVAR=0 days, p=0.035). Mortality was reduced in the EVAR group (eOR=41.4%, eEVAR=20.0%, p=0.103), as was theatre time (eOR= 202.5 minutes, eEVAR=180 minutes, p=0.37) although statistical significance was not reached.
Conclusion:
eEVAR patients have a shorter critical care stay and possibly reduced mortality compared to eOR, however they were less “complex” aneurysm patients and were more haemodynamically stable on presentation. Optimum management of rAAA remains unclear and we await the IMPROVE trial results.

19
A2. Catherine Lunter – University of Southampton
“Transsylvian Selective Amygdalohippocampectomy: The Impact of Surgery on Memory Functioning in Patients with Medically Refractory Medial Temporal Lobe Epilepsy.”
C. Lunter, W. Gray
Background:
The surgical treatment for Mesial Temporal Lobe Epilepsy (MTLE) is validated as a safe and acceptable method of seizure control in medically refractory individuals. However, the effect that such surgery may have on cognitive functioning has posed a matter of great debate. Declines in verbal and non-verbal mem-ory have been described in previous literature, but these findings are not universal, with recent research purporting that the surgery can also have a beneficial outcome on cognitive performance.
Purpose:
The present audit analyses the impact that transsylvian selective amygdalohippocampectomy (TSA) sur-gery has on verbal and non-verbal memory in patients diagnosed with intractable MTLE.
Methods:
41 patients underwent TSA surgery, 14 left-sided and 27 right-sided operations. Neuropsychological tests were performed prior to the surgery and 6-months post-operatively, assessing verbal and non-verbal memory. Paired samples t-tests compared pre- and post-operative test scores for left and right TSA groups. Independent samples t-tests compared the differences in pre- and post-operative test scores ob-tained by the two groups on each test.
Results:
39 patients were seizure free following the surgery. Analysis of the neuropsychological tests showed a significant improvement in verbal memory performance after right-sided surgery. There was no significant change in memory performance following left-sided surgery.
Conclusion:
The results suggest that TSA is an effective method for MTLE surgery, producing favourable seizure-free outcomes without adversely affecting neuropsychological test performances in any of the domains. Sig-nificant improvements in verbal memory scores were also shown in patients undergoing right-sided TSA surgery.
A3. Tom Robinson – University of Nottingham
“An audit of paediatric shunt infection and failure rates”
T. Robinson, D. Macarthur, Consultant Neurosurgeon - Queens Medical Centre
Introduction:
All patients 16 years and under, at QMC, who had insertion of a ventriculoperitoneal or ventriculoatrial shunt between Jan 2010 – Dec 2011
Method:
A retrospective review 3 months after the end of the study period using theatre records and BPNG activity audit. Failure defined as need for a further shunt. Infection defined as bacterial isolate from CSF or com-ponent of failing shunt.

20
Results: All: 67 patients, 91 shunt insertions
Failure rate at 30 days 15/91 (16.5%)
Infection rate study duration 11/91 (12.1%)
Failure rate study duration 34/91 (37%)
Further analysis of patient age and operating personnel was carried out
Discussion:
Simon et al’s 2009 study reported shunt infection rate per procedure over 24 months of 7.2%. They ex-cluded any patients who had had a previous shunt, previous external drain or reservoir and was limited to “uncomplicated initial” shunt insertion. Our patients were unselected with >50% having had a previous shunt, external drain or reservoir so we might expect higher complication rates. Simons et al had an end of study shunt failure rate of 35% at 24 months and our 37% compares favourably with this.
A4. Robert Ford – University of Leeds
“Audit at Bradford Royal Infirmary: Secondary Prevention of Post-Menopausal Osteoporotic Fragility Fractures (The Recommending of Appropriate Patients For DXA Scanning or Commencement of Osteo-porosis Treatment)”
R. Ford, R. Jeffers
Background:
Osteoporosis is a condition of low bone density so encourages fracture from minimal impact or forces, i.e. fragility fractures. Post-menopausal women have raised incidence of Osteoporosis therefore often initially present with fragility fractures. Patients with fragility fractures should be assessed for osteoporosis to elicit the potential for secondary medical intervention. The assessment is by DXA scan, Duel Energy X-ray Absorptiometry scan. In Bradford, responsibility for requesting DXA scanning lies with the GPs. The Ortho-paedics Department treat fractures then discharge to GP. Good practice would be for discharge letters to include a mention of patient suitability for DXA scanning so reducing oversights.
Purpose:
This audit seeks to assess for improvement potential in Bradford Royal Infirmary Orthopaedic Depart-ment’s practice of recommending postmenopausal patients for DXA scanning following fragility fracture. Scanning determines which patients have osteoporosis and so which would benefit from intervention with treatment, a measure towards secondary prevention of further fractures.
Method:
Retrospective review of May 2012 orthopaedic outpatient clinic letters. The ninety one index group pa-tients were subdivided into: those who had had osteoporosis Ix or Rx recommended in clinic letters Vs those who had not.
Results:
Only 5% were recommended.
Conclusions:
1. Raise departmental emphasis that when appropriate, clinic letters should mention DXA scanning.
2. Collate fragility fracture cases into a book which is followed up monthly and chased to GPs by a ward doctor or sister in charge.

21
A5. Jun Wei Lim – University of Dundee
“Effect of Tranexamic Acid (TXA) on Wound Discharge After Primary Total Knee Replacement (TKR)”
J.W. Lim
Aim:
TKR is a common major joint surgery and bleeding is inevitable during surgery. If bleeding persistent after surgery, it would affect the wound healing process and predispose the joint to infections. TXA is an antifi-brinolytic agent that contributes to haemostasis. The aim of this study is to determine if early haemostasis contributes to better outcome of wound healing after TKR.
Method:
In retrospective cohort study, twenty-five patients received TXA intra-operatively, between 500mg to 1g. In the control group, another twenty-five patients did not received TXA intra-operatively. The risk factors for delayed wound healing such as obesity, smoking and co-morbidities were recorded. The surgical wound cares were recorded from day 0 (immediate post-operation) until the day patients were dis-charged. Based on the wound description, wound care scoring system were created, ranging from score 0 as being discharged to 4 as large ooze. The wound care score for both groups were compared.
Results:
The wound care score of day 0 was 2.12 ± 1.24 for control group whereas the wound care score of day 0 for TXA group was 1.04 ± 0.20. Both were significantly different with p = <0.0001). The wound care scores for the subsequent days until being discharged were not significantly different.
Conclusion:
TXA effectively reduced bleeding immediate post-operation. Only a small dose of TXA was being used and this could explain the non-significant results after day 0. From the meta-analysis, a higher dose of TXA (at least 4000mg) would give better homogenous treatment effects.
A6. Michael Harrison – University of Bristol
“An Audit of Open, Laproscopically assisted and Minimally Invasive Oesophagectomies in a UK Cancer Treatment Centre”
M. Harrison, D. Titcomb, Consultant Upper GI Surgeon at Bristol Royal Infirmary
Background:
Surgical resection is currently the primary method of treating oesophageal cancer. However, the introduc-tion of laparoscopic methods is yet to be a proven improvement from traditional open techniques in im-proving the prognosis of oesophageal cancer. The aim of this study is to retrospectively audit all patients who underwent all elective oesophagectomies from 2005 at the Bristol NHS Cancer centre.
Method:
Surgical statistics, patients’ histopathological data and both short and long term clinical outcomes were collected from patient notes and compared according to the surgical technique. The 3 oesophagectomy techniques used were open, laproscopically-assisted (LAO) and minimally invasive (MIO).

22
Results:
A total of 322 patients (MIO = 69; LAO = 172; Open = 81) underwent oesophagectomies since 2005. Mean blood loss for MIO (222ml) and LAO (359ml) was significantly less (P<0.0001) than open (778ml), con-versely mean duration for open (334mins) surgery was significantly less than MIO (380mins) and LAO (365mins) (P<0.001). The 1-year mortality rate for MIO was 4.3%, significantly less (P<0.02) than LAO (17.4%) and Open (22.2%), however there were no significant differences in the length of hospital stay, Dindo complication classification and 30-day mortality rate.
Conclusion:
The use of new MIO and LAO techniques at this centre has proven that they can produce results that are on par with the traditional open method. It is not yet possible however to stipulate whether or not MIO and LAO improve long-term outcomes. Further research is required to further these short-term findings and provide an accurate long-term prognosis after surgery.
A7. Nicola Wright – University of Birmingham
“Lymph Node Harvest as a Marker of Quality in Colon Cancer Resection: A Comparison Between Laparo-scopic and Open Resections”
Wright, E. Hamilton. New Cross Hospital, Wolverhampton Supervisor- Haney Youssef. Consultant Colorec-tal Surgeon, Good Hope Hospital Birmingham
Background:
Accurate lymph node staging is essential for planning postoperative adjuvant therapy, as well as providing patients with prognostic information. One concern with laparoscopic colonic resection is that complete mesocolic resection is not as thorough as for open surgery. The aim of this study was to compare lymph node harvests and distance to vascular pedicle (DVP) in laparoscopic versus open resections for colon can-cer.
Methods:
Details of all patients having colon cancer resection, from January 2009 to March 2011, were prospec-tively recorded on a database. Data was analysed on primary tumour site, lymph node (LN) yields, positive node ratios, type of surgery, tumour site, DVP and pathological stage.
Results:
242 patients, median age 73 years (range 27–97 years), underwent 188 open or 54 laparoscopic (8 con-verted) colonic resections. Median lymph node harvest for open resection was 18 (range 2-43) compared to 18 (range 6-32) for laparoscopic resection The mean positive node ratio was 12% for open resection vs 10% for laparoscopic resection. The mean DVP was 82cm (median 70cm; range 10-290) for open vs 62cm (median 55cm; range 6-140) for laparoscopic resections. There was a trend to a greater proportion of T4 tumours operated on in the open group than laparoscopic (44% versus 26%,)
Conclusion:
Whilst a greater length of mesentery was removed during open resection of a colonic tumour, lymph node harvest was similar for open and laparoscopic resection suggesting that laparoscopic resection is oncologi-cally similar to open resection

23
A8. William Cook – University of Bristol
“Adherence to the British Society of Gastroenterology guidelines for management of acute pancreatitis in North Bristol”
W. Cook, J. Hewes, Department of Upper GI Surgery, Frenchay Hospital, North Bristol NHS Trust
Audit standard and aim:
The aim of this audit is to assess compliance with the British Society of Gastroenterologists (BSG) guide-lines in the management of acute pancreatitis in our trust.
Methods:
The first 50 patients admitted in 2011 with acute pancreatitis were selected. Audit standards were taken directly from the BSG guidelines and electronic and paper notes were retrospectively reviewed.
Results:
Aetiology
- Aetiology determined in 74% of patients (BSG standard: 80%)
Severity
- 70% of patients were severity scored during the first 48 hours of admission (BSG standard: 100%).
- 8 patients (16%) had severe acute pancreatitis; 2 of these patients were discussed with intensive care and one was admitted to intensive care (BSG standard: all patients scored as severe should be managed in ITU).
Imaging
- 18% had a non-diagnostic CT scan before day 6 of their admission. (BSG standard: no CT before day 6 of admission).
ERCP
- Urgent ERCP indicated in 7 patients, 1 patient underwent ERCP within 72 hours of admission (BSG stan-dard: all patients meeting
pecific criteria should undergo ERCP within 72 hours of admission).
Management
- 3 of 20 patients with gall stone pancreatitis underwent an inpatient laparoscopic cholecystectomy. Seven patients underwent outpatient cholecystectomy (BSG standard: all gall stone pancreatitis patients should undergo definitive management).
Conclusion and Clinical relevance:
This audit demonstrates variability in the adherence to the BSG recommendations in our trust. In order to improve clinical practice and outcomes we have designed a pancreatitis care pathway.
Case Report Presentations
C1. Sarah Fendius – Barts and the London School of Medicine and Dentistry
“A Giant Thymic Cyst Mimicking a Large Pleural Effusion”
S. Fendius, W. Awad, Department of Cardiac Surgery, London Chest Hospital, London, UK
Report:

24
A previously fit and well 24-year-old woman presented with a 3 month history of increasing shortness of breath. On examination she had signs of a right pleural effusion. Chest Xray showed a large right-sided pleural effusion with compression of the lower lobe of lung. An intercostal drain was inserted but no fluid was drained. CT scan of chest confirmed a large cystic mass within the right hemithorax. Following discus-sion at an MDT meeting it was recommended that the patient undergo surgery. Rigid bronchoscopy was normal. A right postero-lateral thoracotomy was performed. A 16cm x 9cm tense cystic lesion was seen firmly adhering to the pericardium with the phrenic nerve stretched over its sur-face. It extended into the anterior mediastinum and encased the superior vena cava. The cyst appeared to be in continuity with the right lobe of the thymus; it was carefully mobilised and excised with both lobes of the thymus. The cyst contained 1.3 litres of clear fluid. The post-operative course was uncomplicated. Histological examination of the resected specimen suggested a benign thymic cyst.
Discussion:
Thymic cysts may be congenital or acquired and account for 2% of mediastinal masses. Patients may be asymptomatic or present with a cough, dyspnoea or chest pain. The cyst in our case was so massive it mimicked a pleural effusion. The differential diagnoses include bronchogenic and pericardial cysts. Thymic cysts can occur in association with thymoma and thymic carcinoma.
Conclusion:
As thymic cysts may be associated with neoplasia, complete surgical resection and careful histopathologic examination is recommended in all patients.
C2. Carla Harris – University of Manchester
“Body Contouring - Is it worth the weight?”
C. Harris, J. Srinivasan, Plastic and Reconstructive Surgeon, Royal Preston Hospital
Background: With the population increasing in number, and in body size, the UK faces a potential obesity epidemic, and the significant medical and social consequences. The surgical options to help reduce their weight are avail-able on the NHS. In the morbidly obese, for whom other treatments have failed, bariatric surgery is an effective treatment. Although it carries with it risks, they are far outweighed by the health benefits of the (often dramatic) weight reduction. Although the aesthetic consequences of bariatric surgery and signifi-cant weight loss ie large amounts of redundant skin, are distressing and psychologically damaging to the patients, funding for corrective aesthetic surgery is rarely available on the NHS due to a lack of funding from local PCTs, and a belief that the surgery is cosmetic, and less of a priority.
Report and discussion:
In my report I described a 33 year old lady who presented to the Plastic Surgery and Burns Unit, with aes-thetically unpleasant redundant skin over her abdomen following massive weight loss after bariatric sur-gery. I reviewed the aesthetic problems that result from massive weight loss and how they affect patients medically. I reviewed the surgical techniques used to correct redundant abdominal skin and the potential post-operative problems. I also reviewed the consequences the patient faces, physically, mentally and emotionally.
Conclusion: As the UK is facing a potential obesity epidemic, it is important for physicians and surgeons to be aware of these problems which are likely to increase in future years.

25
C3. Seji Angel Jung – University of Manchester
“Management of open abdomen following abdominal compartment syndrome in a child: A case re-port”
S.A. Jung
Background:
An abdominal compartment syndrome is an increase in the intra-abdominal pressure. This is one of the causes for an open abdomen where the fascia is left open.
Report:
This case presents a boy born with an anus malformation. Two days after birth, he went for a colostomy operation. An anus was created six months later. He was admitted for a laparotomy for a stoma closure four and a half months later, but a second laparotomy was done due to a distended abdomen which gradually got worse. In the operation, areas of poorly perfused was resected and replaced back into the abdomen. Unfortunately, two days after the second laparotomy, the patient developed abdominal com-partment syndrome. This led to a third laparotomy which resulted in an open abdomen. The patient then formed multiple fistulae as a complication of an open abdomen and went through two further operations. Currently, six months after the last operation, the patient is well, thriving, and has a restricted diet.
Discussion/ Conclusion:
In this child, the abdomen is left open following an abdominal compartment syndrome. Fistulae are pos-sible complication of an open abdomen and this carries a high mortality and morbidity risk. Therefore a cautious management of an open abdomen and its complications are crucial.
C4. Vijay Pattni – University of Bristol
“An unusual presentation of an infected vallecular cyst presenting as acute supraglottitis.”
V. Pattni, G. Porter, University Hospitals Bristol, E. Omakobia, University Hospitals Bristol
Background:
We report an unusual case of a patient with an infected vallecular cyst presenting with acute supraglotti-tis. Vallecular cysts are classified as ductal cysts resulting from the obstruction of mucus in the collecting ducts of submucosal glands, and constitute 5% of benign laryngeal lesions.
Case report:
A 50 year old gentleman presented to the emergency department with a 24 hour history of stridor, dys-phagia, dysphonia and vomiting. On examination, the patient was pyrexial and tachycardic, but there was no palpable cervical lymphadenopathy. Flexible nasendoscopy and lateral neck x-ray revealed soft tissue swelling around the epiglottis. The swelling subsided with conservative management of intravenous anti-biotics and steroids, only to reveal a left sided cyst, which was confirmed on microlaryngoscopy. The cyst was subsequently deroofed and histological examination confirmed an infected, benign vallecular cyst with underlying lymphoid tissue.
Discussion:

26
Although vallecular cysts are asymptomatic in two thirds of adult patients, they can become infected and initiate acute supraglottitis with or without abscess formation, and simulate life-threatening airway dis-ease due to obstruction of the laryngeal inlet; therefore they can be easily misdiagnosed by clinicians. Vallecular cysts may only be visible on flexible nasendoscopy once supraglottic inflammation has subsided, thus early diagnosis and airway management is essential reduce patient morbidity and mortality. Conclusion:
Although rare, vallecular cysts should be considered as a differential diagnosis in life-threatening airway disease. Surgically deroofing vallecular cysts with direct microlaryngoscopy is the recommended treat-ment of choice, and may be followed by histological analysis for further confirmatory diagnostic informa-tion.
C5. Jun Wei Lim – University of Dundee
“Distal Femoral Replacement in Complex Revision of Femoral Component for Peri-prosthetic Fracture: A Case Report”
J.W. Lim
Introduction: Total knee arthroplasty (TKA) is one of the common major joint procedures that provide patients with sat-isfactory functional outcome and pain relief. The number and the rate of TKA have increased steadily in the past decade. Inevitably, this has been followed by an increase in the number of post-operational revi-sion surgeries.
Case Presentation:
An 84-year-old female patient who underwent multiple extensive surgeries for infected TKA and repre-sented with peri-prosthetic fracture after a fall. The patient was in significant pain and unable to mobilise. In this case, distal femoral replacement is mandatory for symptomatic relief and to improve function.
Discussion: The choice of treatment for peri-prosthetic fractures depended on several factors that aimed to achieve a painless and stable knee without significant residual mal-alignment. This patient is at greater risk in rela-tion to the following factors: advanced age, female, osteopenia and multiple previous revisions. Fixation with plates and intra-medullary nails are not feasible in previous rotating-hinge prosthesis and highly os-teopenic bone. This is a difficult case that involved displaced fracture and a loose prothesis coupled with metaphyseal deficient. The distal fracture fragment should be replaced with either distal femoral replace-ment prosthesis or a structural allograft. In low-demand elderly, distal femoral replacement is a better option. However, the complication rates are higher compared to other arthroplasty. Distal femur replace-ment should be reserved for salvage in complex revision cases, as the re-revision or failure of the prosthe-sis is complex and may result in an unsalvage situation.
C6. John Kan – University of Manchester
“ Avascular necrosis of the femoral head following a previous diagnosis of aplastic anaemia”
J. Kan, D. Sochart, Consultant Orthopaedic Surgeon, North Manchester General Hospital

27
Background: Avascular necrosis (AVN) is caused by disruption of the vascular supply to the head of the femur, causing the destruction of bone tissue in the femoral head. The pathophysiology of avascular necrosis is not com-pletely understood and various theories have been put forward.
Report: A 39-year old gentleman presented with pain in his left hip that had progressively worsened over the past 5 months. This started as aching, tremors and fasciculation in his thigh, which then went on to involve the hip joint about 2 months after the initial onset. An MRI scan showed well-established AVN of the left femoral head. His past medical history included a diagnosis of aplastic anaemia 4 years before which was treated with anti-lymphocyte globulin (ALG) and prednisolone. This case of avascular necrosis was treated surgically by drilling and insertion of a rod into the left femoral head. Discussion: It has been postulated that aplastic anaemia in its own right as well as the treatment for it are risk factors for developing AVN, especially if high-dose corticosteroids are used. Management of AVN ranges from conservative management during the early stages to joint replacement for advanced disease. Procedures such as core decompression, osteotomy and bone grafting are available also possible treatment modali-ties. Conclusion: Susceptible patients should be identified, and their risk factors assessed and managed appropriately. Early detection confers a more favourable prognosis and less invasive treatment options are available if the damage is minimal. C7. - Iheukwumere Duru – University of Manchester “Coronary Artery Bypass Grafting with Y-type Saphenous Vein: A Case Report highlighting the associ-ated intra-operative benefits.” I. Duru, B. Krishnamoorthy, W.R. Crichtley, J.E. Fildes, N. Yonan The long saphenous vein (LSV) is the predominant conduit utilised in coronary artery bypass graft (CABG) surgery, and can be retrieved via endoscopic vein harvesting (EVH). Whilst EVH is associated with signifi-cantly greater recovery, wound healing and cosmetic appearance than the traditional open vein harvest-ing technique, the long-term outcome has been questioned. Retrieval of the LSV has been associated with elevated risk of bleeding in the tunnel during harvesting. This complication is even more distinct when a branch of the Y-type, anatomical variant of the LSV is dissected and cauterised, due to the size of the ves-sel being cut. However, we demonstrate a case in which the Y-type variant of the LSV was instead har-vested and successfully utilised as a conduit. We present the benefits associated with our approach. The postoperative results of this case were com-pared to the outcome of 5 other patients, in whom the same anatomical variant of the LSV was dissected and cut by diathermy. Our findings indicate that harvesting, rather than cauterising the Y-type vessel, re-sulted in fewer complications, including intraoperative bleeding. This reduced the operating time and did not necessitate the conversion to either open or bridging techniques in order to extract the vessel.

28
C8. Patrick Robinson—University of Glasgow “Tuberculosis a real and present danger: Psoas Abscess presenting as ‘sciatica’.” P. Robinson, D. Shields, Department of General Surgery, Queen Elizabeth Hospital, Gateshead Mrs X is a 35 year old female of Indian authenticity who has lived in the UK for the last 15 years and occa-sionally visits rural India. She presented with a 1 month history of lower back pain, radiating down the back of her right leg. Soon after, she developed progressive anorexia with weight loss and night sweats. Report Her GP referred her to the spinal clinic querying sciatica but she developed an acute deterioration in her symptomology and presented to A&E. On examination, she was significantly tender at her right sacroiliac joint and had a positive psoas sign. The MRI scan showed a large iliopsoas abscess causing boney destruc-tion in the posterior iliac wing, sacrum and L5 vertebra. Extended culture was positive for Mycobacterium Tuberculosis. 12 days into therapy the patients neurological symptoms completely resolved, but their sac-ral pain still persisted. Discussion An iliopsoas muscle abscess can apply pressure on the femoral nerve, however in this case, it extended posteroinferiorly, irritating the L4-S3 nerve roots and giving her lower back and leg pain which was exacer-bated by osteomyelitic destruction of the sacrum. The patient was diagnosed with sciatica yet she had a positive psoas sign and a painful sacrum which are not consistent of this diagnosis. It is important that pri-mary physicians are aware of the anatomy of the iliopsoas muscle and the potential effect an abscess in this region can have. A sinister underlying cause of a patient’s sciatic distribution of pain should be the excluded before accepting a diagnosis of mechanical back pain. References 1. Wong JG. The psoas signs. Well-described but often forgotten physical examination findings of iliopsoas inflammation. N C Med J1993;54:598–600 2. Hsin-Per Y,Yun-An T, Su-Fen L, Pei-Hisn L, Tien-Yow C. The Challenge of Diagnosing Psoas Abscess. J Chin Med Assoc 2004;67:156-159 3. Ailianou A. Fitsiori A. Syrogiannopoulou A. Toso S. Viallon M. Merlini L. Beaulieu JY. Vargas MI. Review of the principal extra spinal pathologies causing sciatica and new MRI approaches. [Review] British Journal of Radiology. 85(1014):672-81, 2012 Jun. C9. Shabnam Javed – University of Manchester “Recent advances in the management of patients with severe aortic stenosis- A case presentation” S. Javed Background: Aortic stenosis (AS) is the most common valvular disease in the western world with a prevalence of 5-7% in the elderly. However, as many as 30% with severe AS are unable to undergo surgery due to the high surgical risk. The introduction of transcatheter aortic-valve implantation (TAVI) has revolutionised the out-come for these patients by successfully reducing their mortality rates. Report:
A 92 year old female with severe symptomatic aortic stenosis and moderate coronary disease was admit-ted to hospital for an elective transapical TAVI. Her echocardiogram revealed calcified aortic valve and mild mitral regurgitation. During the procedure she had a cardiac arrest and went into ventricular fibrilla-tion. She was cardioverted and was thought to have sick sinus syndrome. Due to the complications, a

29
pacemaker was put in the patient and a chest x-ray revealed that she also had developed a pericardial and pleural effusion. She was sent to cardiac surgery intensive care unit for high dependency care
Conclusion: TAVI is a useful less invasive procedure for patients with severe AS compared to the surgical aortic valve replacement. However, there are many serious complications associated with TAVI such as bleeding (5%), stroke (2-5%), heart attack (<2%), death (7-10%), pericardial effusion (<5%) and infection (<2%). It would be useful to have more data so that we are able to look at the effectiveness of TAVI in patients with se-vere AS who can have surgery and in low risk patients. Posters P1. John Connelly – University of Glasgow “Audit of local recurrence following conventional APER for low rectal cancer” J. Connelly Background: Abdomino-perineal resection (APER) involves resection of the anal canal, rectum and distal colon in pa-tients with low rectal cancer. An extended form involving extra-levator dissection exists and may reduce local recurrence1. Purpose: We aimed to ascertain a 5 year local recurrence rates (5-LRR) in our centre and compare with standards derived from a literature review. Methods: We retrospectively evaluated data from electronic patient records of 38 patients who underwent conven-tional APER performed by a single consultant surgeon between 1993 and 2006. Results: 2 patients with significant co-morbidities died in the early post-operative period and were excluded from analysis. We established a 5-LRR of 8.3% (3/36). This compared favourably with 11.9%1 from a recent sys-tematic review in conventional APER. Further analysis characterised the LRR in specific patient subsets. We found that the 5-LRR was higher in patients with larger tumours and in those who did not receive neoadjuvant chemoradiotherapy. All patients who suffered local recurrence had identifiable risk factors. Conclusion: Although limited by sample size, these data should allow us to provide accurate information when con-senting patients for this radical operation and provide a base-line for subsequent analysis of post-APER local recurrence in the unit. The results support internal decision-making to restrict extra-levator APER to patients with more locally-advanced rectal adenocarcinomas. References: 1. Stelzner S, Koehler C, Stelzner J, Sims A, Witzigmann H. Extended abdominoperineal excision vs. stan-dard abdominoperineal excision in rectal cancer—a systematic overview. Int J Colorectal disease. 2011 Oct;26(10):1227-40

30
P2. Benjamin Davies – University of Manchester
“The changing phenotype of the nucleus pulposus with degeneration”
B.Davies, University of Manchester, R.Atkinson, SRFT, F.Ludwinski, University of Manchester, K. Gnanaling-ham, SRFT, J.Hoyland University of Manchester
Introduction:
Nucleus pulposus [NP] changes may be the initial pathology in a large proportion of back pain. Recently a number of biochemical markers differentially expressed by NP cells have been identified. These are likely to relate to its function.
Objective:
To assess whether the expression of NP markers changes with degeneration.
Method:
Lumbar and cervical human NP samples, provided by patients undergoing discectomy, were tested for NP markers using quantitative real-time PCR. Their pre-operative MR scans were staged for disc degenera-tion. Lumbar and cervical samples were considered separate study groups. Grading reliability was as-sessed. Mean expression per grade of degeneration was compared.
Results:
Grading of lumbar and cervical discs for degeneration (κ of 0.58 and 0.57) showed substantial agreement. 96% of discs were grade III or IV. In lumbar samples significant downregulation of KRT18 and upregulation of TIMP2 and in cervical samples significant downregulation of KRT8 and LSGAL3 was found with grade IV compared to grade III.
Conclusions:
The majority of patients requiring discectomy have degenerate discs. NP markers are expressed during degeneration but significant
P3. Muzzamil Hussain – Barts and the London School of Medicine and Dentistry
“Optimisation of Silk Conduits by Degumming and Their Regenerative Potential Following Peripheral Nerve Injury in Adult Rats”
M. Hussain
INTRODUCTION:
Peripheral nerve injury is a major cause of morbidity. The current ‘gold standard’ to treat such injuries is autologous graft repair. This method risks painful neuroma formation and the incomplete recovery of the resected nerve. Alternative repair strategies such as the use of nerve tubes currently exist. Variable de-grees of success have been achieved with these. A novel fully-degummed ‘silk worm’ fibroin based Spi-derex® nerve tube has been developed.
PURPOSE:
To explore if the novel Spiderex® tube can achieve the same nerve regeneration success as the current ‘gold standard’ and thereby verify if it is a suitable candidate to be used in the clinical setting.

31
METHODS:
12 female Sprague-Dawley rats, Surgical excision of grafts after 8 weeks, Tissue processing, Immuno-histochemistry, Confocal microscopy and Quantitative analysis.
RESULTS:
Axonal regeneration using the Spiderex® tube, in the mid-graft section was comparable to that in the autologous graft (p>0.05) mid-section with greater regeneration in the distal-section of the nerve (p<0.01). Overall Schwan cell support was greater in the Spiderex® nerve tube (p<0.05) as compared to the autologous graft. Macrophage responses were similar at the distal-ends in both the Spiderex® tube and autologous graft treated nerves (p>0.05) but higher at the Spiderex® tube, at mid-graft level com-pared to the autologous graft mid-section (p<0.05).
DISCUSSION:
The novel Spiderex® silk conduit is a suitable alternative for clinical use. Sacrificing animals beyond 8 weeks may demonstrate superior nerve regenerative potential of Spiderex® tubes compared to autolo-gous graft repair. Whether this translates to functional recovery is unknown.
References:
Altman GH, Diaz F, Caroline J et al. (2003) Silk based biomaterials, Biomaterials, 24:401-416 Battiston, B., Geuna, S., Ferrero, M. And Tos, P. (2005). Nerve repair by means of tubulisation: literature review and personal clinical experience comparing biological and synthetic conduits for sensory nerve re-pair. Microsurgery, 25, 258-267
De Ruiter GCW, Spinner RJ, Yaszemski M et al. (2009) Nerve tubes for peripheral nerve repair, Neurosurg Clinic N Am 20:91-105
Huang W, Begum R, Barber T, Ibba V, Tee NC, Hussain M et al.( 2012) Regenerative potential of silk con-duits in repair of peripheral nerve injury in adult rats. Biomaterials. 33(1):59-71 Radtke C, Vogt P, (2009) Peripheral nerve regeneration: A current perspective, J. Plastic Surg., 9:435-442
P4. Christina Davies – University of Manchester
“Carotid artery dissection in association with a minimally displaced C2 fracture: a case report”
C. Davies, A. Baker
Introduction:
It is well known that vertebral artery injury can occur with displaced cervical spine fractures that involve the vertebral foramen. Also, carotid artery dissection has been described in association with cervical spine trauma but its incidence is lower. Some propose that carotid artery dissection results from stretching of the internal carotid artery over the transverse processes of C1 and C2 vertebrae.
Case:
We describe a case of carotid artery dissection in association with a minimally displaced C2 fracture and our attempts at management as well as a review of the literature. Initial treatment of the minimally dis-placed high energy cervical fracture was with halo vest immobilisation. Subsequent assessment was with CT angiography and treatment systemic thrombolysis with moderate improvement in symptoms.
Conclusion:

32
Early diagnosis of carotid artery dissection can improve treatment by informing decisions about anticoagu-lation therapy. New imaging modalities, such as CT Angiography and MR Angiography are providing in-creased opportunity for early diagnosis and advances in interventional radiology may increase the treat-ment options and improve progress.
P5. Clarissa Gurbani – University of Manchester
“Lung Transplantation as a Treatment for Idiopathic Pulmonary Hypertension: A Case Report”
C. Gurbani
Idiopathic pulmonary arterial hypertension (IPAH) is defined as a mean pulmonary arterial pressure (mPAP) of greater than 25 mmHg at rest or 30 mmHg during exertion, with a pulmonary capillary wedge pressure (PCWP) of below 15 mmHg. The progression of the disease is generally grim, invariably leading to right ventricular dysfunction and subsequent right heart failure and death. This is a case report of a 25-year old woman with IPAH, in which we describe her history, diagnosis and management. She initially pre-sented with a six-month history of progressive exertional dyspnoea and generalized fatigue, with late-onset syncope. She was referred for assessment and showed evidence of pulmonary congestion on chest radiography and right ventricular dysfunction on echocardiography, with her diagnosis eventually con-firmed by right heart catheterization. Our patient then began pharmacological therapy but due to the pro-gressive nature of IPAH, began to deteriorate rapidly approximately 3 years after starting treatment until a lung transplant was necessitated. This case aims to outline our patient’s journey to transplantation, with a view to ultimately showcase lung transplantation as the gold standard of management for patients with an adverse prognosis despite medical therapy.
P6. Daniel Gibney – University of Manchester
“Necrotising Fasciitis: The patient was telling us the diagnosis all along.”
D. Gibney, J. Cheesbrough, Consultant Microbiologist, Lancashire Teaching Hospitals NHS Foundation Trust
Necrotising fasciitis is a rare yet infamous disease due to invasive group A streptococcal (GAS) infection causing necrosis and damage to skin and fascia, although it can also infect muscle. This case report looks at a woman who presented 3 times in 24 hours with severe arm pain needing morphine, ketamine and pregabalin, with no skin signs. She was transferred to ITU with septic shock before having urgent debride-ment by the plastic surgeons. GAS was isolated from tissue samples. GAS has re-emerged since the 1980s and has increased in virulence; the discovery of “superantigens” is indeed worrying, and it is able to cause an array of other infections. Necrotising fasciitis has an unusual and vague presentation, which normally involves severe pain in an area such as the arm, but there will be little to see or find on examination and other pathologies will be presumed, such as septic arthritis in this case. A flu-like prodrome may precede the events that follow; which can be cytokine mediated streptococcal toxic shock syndrome that leads to multi organ dysfunction, DIC and ARDS. By the time it is recognised, the disease process will probably be advanced and early surgical debridement is often necessary to remove necrotic tissue and toxins. How-ever with large sections of skin often being removed, open wounds and skin grafting can hinder the recov-ery. Clindamycin, a beta lactam and IV immunoglobulin, with rapid diagnosis and surgical debridement offer a reasonable chance of recovery. The pathophysiology, microbiology and surgery will be discussed…

33
P7. Tamsyn Clark – University of Bristol
“Transcatheter aortic valve implantation: Hope for ‘high risk’ patients.”
T. Clark
Aortic stenosis (AS) is the most common valve disease in Europe(1). Prognosis is poor if left untreated af-ter development of symptoms, with an average survival of 2-3 years(2). Symptomatic or severe AS (defined as valve area 0.6-0.8cm(1), mean pressure gradient 40-50mmHg(2)) indicates aortic valve re-placement (AVR)(3). However, the procedure involves cardioplegic arrest, cardiopulmonary bypass and a sternotomy(4), ruling out many elderly patients.
A 90 year old female presented with sudden onset anginal pain brought on at rest, following a 2 year his-tory of stable angina. She had known severe stenosis of the aortic valve and a history of cardiovascular and cerebrovascular disease, classifying her as too ‘high risk’(5) for open valve replacement. Echocardi-ography confirmed the severe AS and showed normal systolic contractility of the left ventricle. The patient was therefore considered for transcatheter aortic valve implantation (TAVI). This minimally invasive proce-dure involves balloon valvuloplasty of the stenotic valve under rapid ventricular pacing(6) and subsequent bioprosthetic valve implantation from either a femoral approach(7) or a subclavian approach(8). The pro-cedure results in significant haemodynamic improvement in high risk indicated patients(4). Yet the risk of complications such as stroke is high(9) and therefore a trans-apical approach has been developed(10). Further research is required to determine the best approach on a patient specific basis(11). However, it is evident that TAVI has future potential since it allows AVR in ‘high risk’ patients with severe, symptomatic AS for whom open AVR is contraindicated.
References: (1) Iung B, Messika-Zeitoun D, Cachier A, Delahaye F, Baron G, Tornos P, Gohlke-Ba¨rwolf C, Boersma E, Ravaud P, Vahanian A. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. European Heart Journal 2003;24: 1231– 43. (2) Brown J, Morgan-Hughes NJ. Aortic stenosis and non-cardiac surgery. Continuing Education in Anaesthesia, Critical Care & Pain 2005;5: 1-4. (3) Shipton B, Wahba, H. Valvular heart disease: Review and update. American Family Physician 2001;63: 2201-08. (4) Thielman M, Wendt D, Eggbrecht H, Kahlert P, Massoudy P, Kamler M, Erbel R, Jakob H, Sack S. Transcatheter aortic valve implantation in patients with very high risk for conven-tional aortic valve replacement. Annals of Throracic Surgery 2009;88: 1468 –75. (5) Tony Goldstone. Euro-pean System for Cardiac Operative Risk Evaluation. http://www.euroscore.org/euroscore_scoring.htm (accessed 10 September 2012). (6) Leon MB, Smith CR, Mack M, Miller C, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontanna GP, Makkar RR, Brown DL, Block PC, Guyton RA, Pichard AD, Bavaria JE, Hermann HC, Douglas PS, Petersen JL, Akin JJ, Anderson WN, Wang D, Pocock S. Transcatheter aortic valve implan-tation for aortic stenosis in patients who cannot undergo surgery. New England Journal of Medicine 2010; 363: 1597-1607. (7) Cribier A, Eltchaninoff H, Bash A, Borenstein N, Tron C, Bauer F, Derumeaux G, Anselme F, Laborde F, Leon MB. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: First human case description. Circulation 2002;106: 3006-8. (8) Petronio AS, De Carlo M, Bedogni F, Marzocchi A, Klugmann S, Maisano F, Ramondo A, Ussia GP, Ettori F, Poli A, Brambilla N, Saia F, De Marco F, Colombo A. Safety and efficacy of the subclavian approach for transcatheter aortic valve implantation with the CoreValve Revalving System. Circulation Cardiovascular Inventions 2010;3: 359-366. (9) Cribier AG, Zajarias A. Outcomes and safety of percutaneous aortic valve replacement. Jour-nal of American College of Cardiology 2009;53: 1829-36. (10) Walther T, Dewey T, Borger MA, Kempfert J, Linke A, Becht R, Falk V, Schuler G, Mohr FW, Mack M. Transapical aortic valve implantation: step by step. Annals of Thoracic Surgery 2009;87: 276-83. (11) Osswald BR, Gegouskov V, Badowski-Zyla D, Tochter-mann U, Thomas G, Hagl, S, Blackstone EH. Overestimation of aortic valve replacement risk by EuroSCORE: implications for percutaneous valve replacement. European Heart Journal 2009;30: 74-80.

34
P8. Nyan Su – Barts and the London School of Medicine and Dentistry
“C-type Natriuretic Peptide receptors in the Cartilage of Patients with Osteoarthritis”
N. Su. Supervisor: T. Chowdhury, Queen Mary, School of Engineering and Material Sciences
Objective:
CNP signalling pathways play a crucial role in the process of endochondral ossification and growth plate chondrogenesis. However, CNP expression in healthy, adult articular cartilage and disease processes, such as Osteoarthritis has yet to be investigated. The present study was undertaken to investigate NPR-B and NPR-C expression in normal and OA articular cartilage.
Methods:
Human articular cartilage was isolated from the femoral condyles of 10 patients (aged 55 to 84). Samples were fixed in 4% PFA and paraffin embedded, before being sectioned into 5µ sagittal sections. Histological analysis of specimens was conducted using safranin O and haematoxylin and eosin staining. Immunofluo-rescence studies were conducted to identify NPR-B and NPR-C expression.
Results:
NPR-B and NPR-C are expressed in articular cartilage and markedly up-regulated during the progression of OA.
Conclusion:
This is the first study to demonstrate the expression of NPR-B and NPR-C in human articular cartilage, in vivo. CNP pathways play an important function in the regulation of articular cartilage. The activities of these pathways are dramatically increased in the diseased state of Osteoarthritis. The CNP pathways may prove to be the site for a novel therapeutic agent to slow down the progression of OA.
P9. Adrien Yvon – University of Manchester
“Laparoscopic Roux-en-Y gastric bypass in an obese patient: a case report. Hospital Clinico San Carlos, Madrid”
A. Yvon
Background:
Obesity has become a worldwide epidemic, affecting more adults year by year. Medical treatment which includes diets, exercise, and drugs fails in more than 95% of obese patients. This has led to the expansion of bariatric surgery as a popular and efficient treatment option, with the best long term results.
Report:
A 50 year old male patient with obesity and metabolic syndrome is presented. He was operated with the gold standard technique in bariatric surgery: the gastric bypass. The patient suffered two classic complica-tions of the intervention: an anastomotic leakage, and a gastrointestinal bleeding. Patient symptoms in-cluded epigastric pain, maelena, pallor, and the abdominal drain revealed purulent fluid. In addition to his normal postoperative treatment the patient was managed with metoclopramide and IV Tazocin.
Discussion:

35
This presentation highlights the principles of the gastric bypass technique as well as the most frequent and serious complications: pulmonary embolism, anastomotic leakage, gastrointestinal haemorrhage, in-ternal abdominal hernia, anastomotic stricture, marginal ulcer, cholelithiasis, and “dumping” syndrome.
Conclusion:
Though gastric bypasses are becoming more common, awareness of its complications in the postoperative phase needs to be stressed and adequate management is highly important.
P10. Rehan Al-Biatty – University of Leeds
“Anatomical variation in the inferior pancreaticoduodenal arteries and its relevance to pancreas trans-plantation”
R. Al-Biatty
Aims:
To investigate the variation in the patterns of origin of the inferior pancreaticoduodenal arteries (IPDaa.), and the variation in the level at which the IPDaa arise from the superior mesenteric artery (SMA). Knowl-edge of the variation in anatomy of the IPDaa is important in pancreas transplantation as it can potentially complicate procurement and revascularization of the pancreas.
Methods:
The abdomens of 20 cadavers (10 males; 10 females) were dissected to demonstrate the range of varia-tion in patterns of origin of the IPDaa. The incidence and diversity of the variations were recorded. The distance from the aorta to the level of origin of the IPDaa as they arise from the SMA was measured.
Results:
9 different patterns of origin were found for the anterior IPD artery (IPDa), and 10 different patterns of origin were found for the posterior IPDa. The results of measuring the distance from the aorta to the ori-gin of the IPDaa ranged from 24-57mm.
Conclusions:
The pattern of origin of the IPDaa is extremely variable with clinical relevance in pancreas transplantation. It has been reported that in some cases, the head of the pancreas does not reperfuse during the reperfu-sion stage of transplantation. This arises when ligation of the SMA occurs above the origin of the IPDaa. The IPDaa are the only arterial supply to the head of the donor pancreas. Thus, knowledge of the variation in anatomy of the IPDaa will obviate extensive dissection to identify vessels, and avert vascular damage.
P11. Thomas Forshaw – University of Glasgow
“Can we delay first stoma bag change postoperatively? An observational cohort study”
T. Forshaw, S. Panteleimonitis, I. Robertson, C. McNulty, L. Drummond, A. Macdonald, Monklands Hospi-tal, Airdrie, Lanarkshire, Scotland
Background:
Stoma companies recommend changing the appliance one to two days postoperatively. We challenge this in a cohort study where first ostomy change occurred at four days.

36
Methods:
We carried out a retrospective review of a prospectively collected data set. Each patient had a numerical stoma complication score 0 - 22 (leakage, soiling, excoriation), with points added for frequency and sever-ity. Data on elective/emergency status and stoma type were collected. New policy patients (ostomy change at 4 days, Consultant A) were compared with those whose bags were changed after two days (consultants B+C+D+E). Additionally, new policy patients were compared to an historical cohort (Consultant A) where ostomies were previously changed routinely at 48 hours. Results are presented as a median(inter-quartile range)
Results:
There was no obvious difference between the scores of Consultant A and consultants B, C, D and E for emergency or elective surgery. 56 ostomists in the new policy group (consultant A) had a complication score of 0(0-0-0-1-16) compared with 1(0-0-1-4-14) in 113 ostomists (consultants B, C, D and E) in the original policy group (p< 0.209). 448 ostomists under the care of consultant A prior to the policy change had similar stoma scores 0(0-0-0-2-17) when compared to those post policy change (p< 0.435).
Conclusion:
There was no rise of ostomy complications associated with changing appliances beyond 48 hours and up to 96 hours. Planned ostomy change at 96 hours benefits nursing practice by saving: time; money; and inconvenience to postoperative stoma patients.
P12. Oliver Beaumont – University of Bristol
“The quality of operation notes in orthopaedic trauma surgery: An audit in the Bristol Royal Infirmary, 2012”
R. Miller, Bristol University, D. Adams, Bristol Royal Infirmary, M. Jackson, Bristol Royal Infirmary.
Both the Royal College of Surgeons of England (RCSE) and British Orthopaedic Association (BOA) recognise that good medical records are a fundamental and basic prerequisite to a patient’s clinical care. They im-pact upon medico-legal cases, coding and subsequent management of patients. It is vital that the impor-tance of adequate record keeping is recognised by surgical consultants, trainees and medical students alike. Although focused on orthopaedics, issues raised from this audit and methods for change are trans-ferable to all surgical specialties.
This audit compares the quality of orthopaedic post-operative notes to the gold standard set out by RCSE and additional BOA recommendations. A cohort of thirty trauma orthopaedic patient notes were ran-domly selected and compared to these standards.
Full compliance to recommended standards was never observed. Furthermore, compliance with the eleven RCSE criteria was as low as 50% and only three of these were met 100% of the time. These results were deemed unacceptable, demonstrating an essential need for quality improvement in orthopaedic post-operative note documentation.
Methods for improvement include the use of a computer-generated proforma, a switch to dictated notes or an aide-memoire in orthopaedic theatres. An aide-memoir is now in place within orthopaedic theatres as the first step in the quality improvement cycle. The full impact of this intervention is being assessed. These results will be crucial in establishing the most effective methods for implementing change.

37
P13. - Sophia Mahboob – University of Birmingham
“The Heart-Team Experience in the Management of Patients with Ischaemic Heart Disease”
S. Mahboob, J. Thekkudan, M. Norell
Background:
There is growing interest in “Heart-Team” (HT) approach for managing patients with ischaemic heart dis-ease (IHD).
Aim:
This study assessed the function of HT: its composition, decisions, “actioning” of decisions (if not, why not) and reproducibility of decision-making.
Methods:
Data from consecutive patients (n = 943) discussed at HT meeting were reviewed from HT database. Pa-tient’s records were reviewed to assess whether the HT decision was carried out. Reasons for aberration were documented. 65 patients were randomly selected for re-presentation to HT meeting assessing con-sistency of decisions.
Results:
At least one cardiac surgeon, interventional and non-interventional cardiologists were present for each of the twice weekly HT meeting. Data presented included patient demographics, symptoms, known co-morbidities, coronary angiography, LV function and other investigations (e.g. echocardiograms). Decisions included continued medical treatment (19%), PCI (33%), CABG (29%) or further investigations such as pressure wire studies, dobutamine stress echo (DSE) or cardiac MRI in 19%. HT decisions were fully un-dertaken in 96% of patients. Reasons for aberration included patient’s refusal (15%), previously unrecog-nised co-morbidities (42%), emergency primary PCI (13%) and other (30%). On re-discussion of the same patient data (n = 65), 23% of decisions (n=15) differed from the original HT recommendations. This appar-ent aberration in decision-making reflected the fact that the evidence to treat some coronary artery dis-ease pattern with PCI, medical therapy or CABG, is not very strong.
Conclusion:
A Heart-Team approach to decision making provides transparency for decision making in the treatment of patients with coronary artery disease.

38
2012 Organising Committee:
Charlotte May, Conference Director
Grant Coleman, President
Rebecca Hill, Vice President
Zainab Sherazi, Secretary
Jins Johny Kallampallil, Treasurer
Hasan Mohammad, Lectures Director
Edwin Ong, Workshops Lead
Natasha Westbrook, Communications and Publicity
Lauren Bolton, Membership and IT
Amar Patel, Salford Hospital Rep
Neil Devlin, South Manchester Rep
Laura Lake, Phase 1 Rep
James Ashcroft, Phase 1 Rep
Je Song Shin, Alumni Liaison

39
Notes ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

40
Notes ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

41
Notes ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

42
Notes ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

43
© Scalpel Surgical Society, October 2012
Keep up to date with our future events:
www.scalpelmanchester.com Facebook: /scalpel.manchester
Twitter: @scalpel_mcr

44
With thanks to our sponsors:
In partnership with: