Embed Size (px)
Citation preview

CCIPITAL lobe epilepsy accounts for a small percent-age of extratemporal epilepsies. Depending on se-lection and inclusion criteria, the frequency of OLE
varies between 2 and 13% of symptomatic partial epilep-sies.5,6,23,40 Few large series of patients with OLE have beenreported so far.2,10,25,36 Moreover, some patient series covertime periods before the introduction of MR imaging.5,8,30,31,36
In one of the largest patient series, 42 occipital resectionswere performed between 1930 and 1991 at the MontrealNeurological Institute.31 In the modern era, however, preop-erative diagnostic findings, surgical strategies, histopatho-
logical bases, and postoperative outcomes for OLE remainto be further elucidated.
Compared with results of surgical treatment for TLE,success rates after epilepsy surgery in the occipital regionhave been less promising. Seizure-free outcomes have beenreported in 30–60% of patients; however, due to diversi-ty of disease, inclusion criteria, and outcome classificationscales, evaluation among these studies is difficult.2,8,31 Themost recent OLE series described 61.5% of patients whobecame seizure free after surgeries for OLE performed be-tween 1994 and 2001.22
Occipital lobe epilepsy constitutes a challenge for diag-nosis. Visual auras and/or elementary visual hallucinationsare typical in OLE, and ictal blindness, contralateral eyeand head deviation, eye movement sensations, blinking,and eyelid flutter have all been described. Nevertheless, di-agnosis remains difficult because of rather nonspecific pat-terns in the later course of a seizure, due to fast ictal spreadto distinct brain areas, resulting in temporal or frontal mo-tor seizures in as many as 50% of cases.31,36 A separate syn-
J. Neurosurg. / Volume 109 / July 2008
J Neurosurg 109:57–69, 2008
Surgical treatment of occipital lobe epilepsy
DEVIN K. BINDER, M.D., PH.D.,1,2 MAREC VON LEHE, M.D.,2 THOMAS KRAL, M.D.,2
CHRISTIAN G. BIEN, M.D.,3 HORST URBACH, M.D.,4 JOHANNES SCHRAMM, M.D.,2
AND HANS CLUSMANN, M.D.2
1Department of Neurological Surgery, University of California, Irvine, California; andDepartments of 2Neurosurgery, 3Epileptology, and 4Neuroradiology, University of BonnMedical Center, Bonn, Germany
Object. Occipital lobe epilepsy (OLE) accounts for a small percentage of extratemporal epilepsies and only few andmostly small patient series have been reported. Preoperative findings, surgical strategies, histopathological bases, andpostoperative outcomes for OLE remain to be elucidated.
Methods. A group of 54 patients with occipital lobe involvement were identified from a prospective epilepsy surgerydatabase established in 1989. Medical charts, surgical reports, MR imaging, and histopathology data were reviewed,and patients with additional temporal and/or parietal involvement were categorized separately. Seizure outcome wasclassified according to the Engel classification scheme (Classes I–IV). Two patients were excluded due to incompletedata sets. Fifty-two patients with intractable epilepsy involving predominantly the occipital lobe were included in thestudy, comprising 17.8% of 292 patients undergoing operations for extratemporal epilepsies.
Results. In nearly all cases (50 [96.2%] of 52), a structural lesion was visible on preoperative MR imaging. Of thesecases, 29 (55.8%) had “pure” OLE with no temporal or parietal lobe involvement. Most patients (83%) had complexpartial seizures, and 60% also had generalized seizures. All patients underwent occipital lesionectomies or topectomies;9 patients (17.3%) underwent additional multiple subpial transections. Histopathology results revealed 9 cortical dys-plasias (17.3%), 9 gangliogliomas (17.3%), 6 other tumors (11.5%), 13 vascular malformations (25%), and 15 glialscars (28.8%). Visual field deficits were present in 36.4% of patients preoperatively, and 42.4% had new or aggravat-ed visual field deficits after surgery. After a mean follow-up of 80 months, 36 patients were seizure free (69.2% EngelClass I), 4 rarely had seizures (7.7% Engel Class II), 8 improved more than 75% (15.4% Engel Class III), and 4 had nosignificant improvement (7.7% Engel Class IV). Multifactorial logistic regression analysis revealed that early age atepilepsy manifestation (p = 0.031) and shorter epilepsy duration (p = 0.004) were predictive of better seizure control.All other clinical and surgical factors were not significant in predicting outcome.
Conclusions. Occipital lobe epilepsy is an infrequent but significant cause of extratemporal epilepsy. Satisfactory re-sults (Engel Class I or II) were obtained in 77% of patients in our series. Postoperative visual field deficits occurred ina significant proportion of patients. In the modern MR imaging era, lesions should be investigated in patients with OLEand lesionectomies should be performed early for a better outcome. (DOI: 10.3171/JNS/2008/109/7/0057)
KEY WORDS • dysplasia • epilepsy • ganglioglioma • gliosis • occipital tumor •visual field
O
57
Abbreviations used in this paper: AVM = arteriovenous mal-formation; CPS = complex partial seizure; ECoG = electrocorti-cography; EEG = electroencephalography; FDG-PET = fluorine-18–labeled fluorodeoxyglucose–PET; IED = interictal epileptiformdischarge; MST = multiple subpial transection; OLE = occipital lobeepilepsy; SPS = simple partial seizure; TLE = temporal lobe epilep-sy; TSE = turbo spin echo; WHO = World Health Organization.

drome of nontumoral occipitotemporal epilepsy has alsobeen defined.3 In addition, visual auras can also occur intemporomesial and temporooccipital seizures.6 Scalp EEGrecordings are often not helpful or even misleading,29,31,36
but clearly lateralizing semiology was found to be predic-tive for satisfactory seizure relief.10 The identification of alesion with high-resolution MR imaging and additional im-aging modalities such as SPECT and FDG-PET play a ma-jor role in the diagnostic workup of patients with presumedOLE.19,22,40 For the definitive discrimination between OLEand TLE, invasive video-EEG monitoring using intracra-nial subdural and/or depth electrodes is often mandato-ry.11,21,29
We describe a large series of consecutive patients whounderwent occipital resections for lesional OLE during theera of modern MR imaging and video-EEG monitoring.We analyzed preoperative findings, surgical strategies, his-topathological bases, and postoperative outcomes in this in-frequent type of extratemporal epilepsy.
Methods
Study Population
From a prospective epilepsy surgery database estab-lished at the University of Bonn in 1989, we identified pa-tients who underwent surgery for OLE between 1990 and2005. Minimal requirements for inclusion in the study wereas follows: 1) clinical history of medically intractable epi-lepsy; 2) preoperative MR imaging or histopathological re-sults positive for occipital lobe involvement; 3) completeclinical and electrophysiological data sets; and 4) follow-upseizure outcome data. Of 292 patients undergoing surgeryfor extratemporal epilepsy in our database, we identified 54patients (18.4%) with occipital lobe involvement. Of these54 patients, 52 had adequate data for analysis. To determinethe localization and extent of the lesion, MR imaging, op-erative reports, and histopathology data were reviewed.This review yielded 29 patients with “pure” OLE (9.9%of the total extratemporal epilepsy population in our series),9 patients with additional temporal lobe involvement (oc-cipitotemporal), 10 patients with additional parietal lobeinvolvement (occipitoparietal), and 4 patients with addi-tional involvement of both temporal and parietal lobes (oc-cipitotemporoparietal). These groups were then analyzedboth separately and together as described below.
Preoperative Evaluation
All patients had suffered chronic medically intractableepilepsy for . 1 year and had undergone adequate trialsof $ 2 antiepileptic drugs before they were referred forpresurgical evaluation. All patients underwent continuousnoninvasive scalp video-EEG monitoring to determine ictaland interictal focal epileptiform abnormalities. The detailsof the preoperative workup for epilepsy surgery candidatesat our institution have been previously described in detail.21
Demographic, Clinical, and Radiological Data
Demographic and clinical data used for this analysis in-cluded the following variables for each patient: 1) sex; 2)age at epilepsy manifestation; 3) age at operation; 4) epi-
lepsy duration; 5) seizure type; 6) seizure frequency; 7)presence or absence of other medical history; 8) preopera-tive neurological status; and 9) preoperative visual fields.For the other medical history variable, we examined wheth-er the patient had a history of trauma, hypoxia, perinatalinsult, or intracranial hemorrhage. For preoperative neuro-logical status, preexisting localizing neurological findings(such as hemiparesis) were documented. Preoperative visu-al fields were categorized on an ordinal scale (0 = no de-fect, 1 = minimal/scotoma, 2 = quadrantanopsia, 3 = in-complete hemianopsia, 4 = hemianopsia).
Magnetic resonance imaging was performed using 1.5-or 3-T systems (Gyroscan ACS-NT, Gyroscan NT-Intera,Gyroscan Intera, Gyroscan 3T Intera, and Gyroscan 3TAchieva; Philips Medical Systems) according to a stan-dardized protocol that has been described previously.35
Briefly, the following sequences were acquired: 1) a sagit-tal 3D T1-weighted gradient echo sequence with a voxelsize of 1 mm3; 2) axial FLAIR TSE and T2-weighted TSEsequences at a slice thickness of 5 mm; and 3) coronal in-version recovery (at a section thickness of 5 mm), FLAIR(at a section thickness of 3 mm), and T2-weighted TSEsequences (at a section thickness of 2 mm). If a lesion wasdetected, T1-weighted spin echo sequences before and af-ter gadolinium/diethylenetriamine pentaacetic acid admin-istration were acquired. Based on the neuroradiologist’soriginal MR imaging examination, radiological data wereclassified into the following categories: dysplasia, tumor,scar/cyst formation, vascular malformation, or other lesion.When FDG-PET (12 [23.1%] of 52 cases) and SPECT (9[17.3%] of 52 cases) studies were performed, results werenoted.
Electrophysiological Data
Preoperative, intraoperative, and postoperative electro-physiological data were reviewed in each case. InterictalEEG studies were separated into the following categories:1) IEDs over the posterior cortex (EEG leads P3/P4, T5/T6,and O1/2) ipsilateral to the resection side; 2) ipsilateralIEDs ipsilaterally over the posterior cortex but also overother brain regions; 3) IEDs ipsilateral to the resection sidebut anterior to the above-named contacts; 4) bilateral IEDsor IEDs contralateral to the resection side; and 5) no IEDs.Ictal EEG studies were categorized as follows: 1) ictal on-set over the posterior cortex EEG leads ipsilateral to the re-section side; 2) ictal onset ipsilateral to the resection sideover the posterior cortex but also over other brain regions;3) ictal onset ipsilateral to the resection side but anterior tothe above-named contacts; 4) bilateral or contralateral ictalonset; or 5) no localizing, regionalizing, or lateralizing ictalonset pattern (for example, because of artifacts).
Preoperative invasive diagnostic monitoring was per-formed in 22 (42.3%) of 52 patients, and included vari-ous combinations of depth, strip, and grid electrodes. Thetype and location of grid and strip electrodes were noted.Whether intraoperative ECoG was performed was alsonoted.
Operative and Histopathological Data
Operative details recorded and analyzed in the databaseincluded the date, side, location, and type of operation. The
D. K. Binder et al.
58 J. Neurosurg. / Volume 109 / July 2008

location of the operation (pure occipital, occipitotempo-ral, occipitoparietal, or occipitotemporoparietal) was scoredbased on the concordance between operation report de-scriptions and MR images. The patients with MR imag-ing–visible lesions received lesionectomies, and 12 patients(23%) received additional MSTs in adjacent epileptogeniceloquent areas. In the MR imaging–negative cases, topecto-mies were performed guided by intracranial EEG record-ings. Two patients (3.8%) with recurrent seizures under-went repeat resections, and the location and type of thesecond operations were noted.
Resected specimens were examined histopathologicallyusing methods previously described.37 Tumors were classi-fied according to the revised WHO classification scheme.20
Different subtypes of cortical developmental malforma-tions were grouped together as “dysplasia.” For purposes ofoverall evaluation and correlations, histopathological diag-noses were categorized into 1 of 5 categories: 1) dysplasia;2) ganglioglioma; 3) other tumor; 4) vascular malforma-tion; or 5) scar/gliosis formation.
Outcome Data
Postoperative visual field outcome was categorized onthe same ordinal scale as preoperative field outcome (seeabove) to detect new visual field deficits in individual pa-tients. Cases with unclear or incomplete pre- and postop-erative visual field testing (19 patients [36.5%]) were ex-cluded from this evaluation. For seizure and neurologicaloutcome, follow-up information was obtained either fromthe last regular annual outpatient visit or from telephoneinterviews. Patients were assigned to 1 of 4 outcome class-es according to the Engel classification scheme14 as fol-lows: Class I, seizure free or auras only since surgery; ClassII, rare seizures (, 2/year or only nondisabling nocturnalseizures); Class III, reduction of seizure frequency . 75%;and Class IV, unchanged (, 75% reduction of seizurefrequency). For further analysis, Engel Classes I and IIoutcomes were grouped as satisfactory seizure control,whereas Classes III and IV were grouped as unsatisfactoryseizure control.
Statistical Analysis
We analyzed multiple potential prognostic factors withrespect to their prediction of good seizure outcome: 1) his-topathology versus outcome; 2) surgical procedure versusoutcome; 3) age of onset and epilepsy duration versus out-come; 4) location versus outcome; 5) seizure type ver-sus outcome; and 6) EEG characteristics versus outcome.In addition, we studied potentially interesting interactionsamong nonoutcome variables in this patient group, such ashistopathology versus seizure characteristics and seizuretype versus age of onset. Each factor was analyzed by chi-square or Fisher exact tests both for Engel Class (I–IV)and satisfactory (Engel Class I or II) versus unsatisfactory(Engel Class III or IV) seizure outcome. Continuous vari-ables were tested with the Student t-test. For nonparametrictesting, the Mann–Whitney U-test was applied. For multi-factorial analysis, a stepwise logistic regression model wasapplied. Backward stepwise logistic regression was per-formed with critical probability levels of 0.05 for inclusionand 0.1 for exclusion of factors from the model.
Results
Demographic and Clinical Findings
Demographic and clinical data are summarized in Table1 for the entire patient population (52 patients) and in Table2 for the subgroup with pure OLE (29 patients) and theextended OLE subgroup (23 patients). The overall popula-tion consisted of 25 males and 27 females. Mean age atoperation was 23.6 years (range 4–58 years), and mean pre-operative epilepsy duration was 13.6 years (range 1–42years). The preoperative seizure history for the pure OLEgroup was 17 years, however, compared with only 9.5years in the extended OLE group (p = 0.008, Student t-test). Eight (89%) of 9 patients with cortical malformationshad their epilepsy manifestation before the age of 10 years,compared with only 40–50% in all other diagnoses. Thir-teen patients (25%) had a medical history notable for trau-ma, hypoxia, intracranial hemorrhage, or previous intra-cranial surgery, whereas 75% had no obvious contributingmedical history. Forty-two patients (80.8%) had a normalpreoperative neurological status (visual fields were catego-rized separately), and 10 patients had preoperative neu-rological deficits (cognitive deficits in 6 patients and hemi-paresis or hemisensory syndrome in 4 patients). These latterdemographic factors were not significantly different be-tween the two OLE subgroups.
Seizure types were quite variable (Tables 1 and 2), butthe majority of patients (43 patients [82.8%]) had CPSswith or without other seizure types. Complex partial sei-zures occurred with similar frequencies in the pure and ex-tended OLE subgroups. Thirty-one patients (59.6%) hadgeneralized seizures. The most common seizure-type com-bination was CPS and occasional secondary generalizedseizures (32.7%). Seizure frequencies varied over a widerange. In the 43 patients with CPSs, these seizures occurredat a median of 15 per month (range 1–600/month). In the23 patients with SPSs, these seizures occurred at a medi-an of 25 per month (range 1–300/month). In the 31 patientswith secondary generalized seizures, these seizures oc-curred at a median of 3.5/year.
Adequate preoperative visual field information wasavailable for 41 patients (78.8%). Of this subset, 26 hadintact preoperative visual fields, 3 had minimal deficit orscotoma, 5 had quadrantanopsia, 3 had incomplete hemi-anopsia, and 4 had complete hemianopsia. Between the 2subgroups, the presence of a visual field defect was signif-icantly more frequent in pure OLE (48.1%) compared withextended OLE (14.3%; p = 0.003, Fisher exact test).
Electrophysiological Findings
Adequate interictal EEG studies were available for re-view in 49 (94.2%) of 52 patients. Twenty (40.8%) of these49 patients had epileptiform activity exclusively over thehemisphere on which the resection was performed; of these,only 3 had IEDs over posterior EEG leads only, and anoth-er 9 had IEDs at ipsilateral posterior plus other electrodecontacts, whereas 8 patients had only nonposterior epilepti-form activity. Sixteen patients had IEDs bilaterally or con-tralaterally to the resection side (32.7%), and in 13 patients(26.5%) no IEDs were recorded.
Ictal surface EEG studies were available in 41 patients(78.8% of the total group). Thirteen (31.7%) of these pa-
J. Neurosurg. / Volume 109 / July 2008
Surgery for occipital lobe epilepsy
59

tients had ictal onsets ipsilateral to the resection site. Ofthose 13, seizures in 3 patients originated exclusively overposterior areas, in 7 additionally over nonposterior areas,and in 3 exclusively over nonposterior brain regions. Bilat-eral or contralateral ictal onset patterns were recorded in 18patients (43.9%). In 10 patients (24.4%), seizure origincould not be localized by surface EEG.
Invasive monitoring using intracranial electrodes wasperformed in a total of 22 patients (42.3%). Fourteen pa-tients received mesial temporal depth electrodes implantedalong the longitudinal hippocampal axis to distinguish hip-pocampal seizures from occipital seizures with fast tem-poral spread. In 18 patients, varying numbers of subduralelectrodes were implanted, including 5 patients with multi-ple interhemispheric strip electrodes. In 13 patients, gridelectrodes were used for preoperative functional mapping.Intraoperative ECoG was used in 21 patients (40.4%) andwas usually used following resection to evaluate neighbor-ing cortical areas for residual spiking activity.
Neuroimaging and Histopathological Findings
In nearly all cases (50 [96.2%] of 52), a structural lesionwas visible on preoperative MR imaging. Preoperative MRimaging interpretations were as follows: 10 developmentaltumors/gangliogliomas, 4 other tumors, 5 dysplasias, 7 vas-cular malformations, 16 cases of scar/cyst formation, 8 MR
imaging–visible lesions not otherwise specified, and 2 cas-es in which no lesion was visible.
In 12 cases (23.1%), FDG-PET was performed. In 10 ofthese cases, FDG-PET revealed decreased glucose utili-zation ipsilateral to the lesion; in the other 2 cases it wasnormal or nonspecific. Single-photon emission CT was per-formed in 9 cases (17.3%). In 6 of these cases, SPECT re-vealed hypoperfusion ipsilateral to the lesion. In 3 cases,ictal SPECT was performed and demonstrated ictal hy-perperfusion ipsilateral to the lesion in each case; in 1 case,SPECT results were discordant with FDG-PET results.
A clear histopathological diagnosis was obtained in all52 cases (Table 3). Nine dysplasias were seen, with 5 focalcortical dysplasias, 2 glioneuronal hamartomas, and 2 casesof tuberous sclerosis (Fig. 1). Nine gangliogliomas wereobserved (Fig. 2). Six other tumors were observed (5 astro-cytomas and 1 ependymoma). Of the astrocytomas, 2 wereWHO Grade I, 2 were Grade II, and 1 was Grade III. Thir-teen vascular malformations were found: 6 AVMs, 5 casesof Sturge–Weber disease, and 2 cavernous malformations(Fig. 3). Fifteen cases of scar/gliosis formation were found,
D. K. Binder et al.
60 J. Neurosurg. / Volume 109 / July 2008
TABLE 1Demographic and clinical characteristics of 52 patients with OLE
Characteristic No. of Patients (%) Mean Yrs (range)
sexmale 25 (48)female 27 (52)
age at op 23.6 (4–58)mean preop epilepsy duration
all patients 52 (100) 13.6 (1–42)dysplasia 9 (17.3) 15.8 (1–34)ganglioglioma 9 (17.3) 9.9 (3–20)other tumor 6 (11.5) 11.3 (2–31)vascular malformation 13 (25) 16.0 (3–42)scar/gliosis 15 (28.8) 13.5 (1–30)
other medical historytrauma 5 (9.6)hypoxia 2 (3.8)intracranial hemorrhage 1 (1.9)previous intracranial op 5 (9.6)none 39 (75)
neurological statusnormal 42 (80.8)impaired 10 (19.2)
seizure typeSPS only 3 (5.8)CPS only 11 (21.2)generalized only 1 (1.9)SPS 1 CPS 7 (13.5)SPS 1 generalized 5 (9.6)CPS 1 generalized 17 (32.7)SPS 1 CPS 1 generalized 8 (15.4)
preop visual fieldsintact 26 (50.0)minimal deficit/scotoma 3 (5.8)quadrantanopsia 5 (9.6)incomplete hemianopsia 3 (5.8)hemianopsia 4 (7.7)unclear 11 (21.2)
TABLE 2Demographic and clinical characteristics of 29 patients
with pure OLE and 23 patients with extended OLE
Pure OLE Extended OLE
No. of Mean No. of MeanPatients No. Patients No.
Characteristic (%) of Yrs (%) of Yrs
sexmale 16 (55) 9 (39)female 13 (45) 14 (61)
age at op 25.3 21.5preop epilepsy duration
all patients 29 (100) 17.0 23 (100) 9.5*dysplasia 5 (17.2) 17.8 4 (17.4) 13.5ganglioglioma 7 (24.1) 10.1 2 (8.7) 9other tumor 1 (3.4) 28 5 (21.7) 8vascular malformation 7 (24.1) 23.6 6 (26.1) 7.2scar/gliosis 9 (31.0) 15.4 6 (26.1) 10.7
other medical historytrauma 2 (6.9) 3 (13)hypoxia 1 (3.4) 1 (4.3)intracranial hemorrhage 1 (3.4) 0 (0)previous intracranial op 4 (13.8) 1 (4.3)none 21 (72.4) 18 (78.3)
neurological statusnormal 24 (82.8) 18 (78.3)impaired 5 (17.2) 5 (21.7)
seizure typeSPS only 2 (6.9) 1 (4.3)CPS only 5 (17.2) 6 (26.1)generalized only 0 (0) 1 (4.3)SPS 1 CPS 2 (6.9) 5 (21.7)SPS 1 generalized 3 (10.3) 2 (8.7)CPS 1 generalized 12 (41.4) 5 (21.7)SPS 1 CPS 1 generalized 5 (17.2) 3 (13)
preop visual fieldsintact 14 (48.3) 12 (52.2)minimal deficit/scotoma 2 (6.9) 1 (4.3)quadrantanopsia 5 (17.2) 0 (0)incomplete hemianopsia 3 (10.3) 0 (0)hemianopsia 3 (10.3) 1 (4.3)unclear 2 (6.9) 9 (39.1)
* p = 0.008.

with variable evidence of other histopathological featuressuch as cortical and subcortical astrocytosis, hemosider-in deposition, microglial activation, and cyst formation(Fig. 4).
The 8 lesions revealed on MR imaging as not otherwisespecified were found to comprise 3 vascular malforma-tions, 2 dysplasias, 2 developmental tumors/ganglioglio-mas, and 1 other tumor (Grade I astrocytoma). The 2 casesof no MR imaging–visible lesion were found to comprise 1case of scar/gliosis and 1 case of cortical dysplasia.
Thus the overall MR imaging sensitivity for detectingdistinct histopathological lesions in this series was 96.2%.The MR imaging specificity was 78.6% for 15 tumors in-cluding gangliogliomas, 33.3% for any type of 9 dyspla-sias, 53.8% for 13 vascular malformations, and 86.7% for15 cortical scars and gliosis.
Procedures and Complications
Forty-one patients underwent lesionectomies (extended,if possible), and 2 MR imaging–negative patients under-went topectomies. Five of these patients had undergoneoperations before, as described below. Twenty-five proce-dures were restricted to the occipital lobe, 8 were occipi-totemporal resections, 7 were occipitoparietal procedures,and 3 resections were carried out in the occipitotemporopa-rietal region. Overall seizure outcome resulted in 30 pa-
J. Neurosurg. / Volume 109 / July 2008
Surgery for occipital lobe epilepsy
61
TABLE 3Histopathological diagnoses in 52 patients with OLE
Histopathological Diagnosis No. of Cases (%)
dysplasia 9 (17.3)focal cortical dysplasia 5glioneuronal hamartoma 2tuberous sclerosis 2
ganglioglioma 9 (17.3)other tumor 6 (11.5)
Grade I astrocytoma 2Grade II astrocytoma 2Grade III astrocytoma 1ependymoma 1
vascular malformation 13 (25)AVM 6Sturge–Weber disease 5cavernous malformation 2
scar/gliosis formation 15 (28.8)
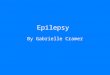
FIG. 1. Example of a patient with an occipital focal cortical dysplasia. Preoperative sagittal (A, B, D, and E), axial (C),and coronal (F) FLAIR TSE images (at 3 T) of a 5-year-old girl with seizure onset at 2 years who experienced both SPSsand CPSs (~ 30/month). An extended occipital lesionectomy with preservation of the basal and mesial occipital cortex wasperformed using intraoperative ECoG. Histopathology revealed focal cortical dysplasia (Type IIb, Palmini and Lüdersclassification). Her preexisting contralateral superior quadrantanopsia was unchanged postoperatively, and she became sei-zure free (Engel Class I).

tients in Engel Class I (69.8%), and 4 patients in EngelClass II (9.3%), resulting in 79.1% satisfactory seizurecontrol. Five 5 patients attained Engel Class III and 4 pa-tients Engel Class IV, thus unsatisfactory seizure controlwas found in 20.9%.
Nine patients underwent lesionectomies together withadditional MSTs of adjacent eloquent cortex. Four MSTswere restricted to the occipital area, 1 was occipitotempo-ral, 3 were occipitoparietal, and 1 was occipitotemporo-parietal. Seizures were fully abolished in 6 patients (66.7%Engel Class I), and seizures were reduced in frequencyby . 75% in 3 patients (33.3% Engel Class III). These re-sults were not statistically significantly worse comparedwith the results of pure lesionectomies (p = 0.415, Fisherexact test).
Seizure control was less frequently achieved in the groupof patients in whom invasive monitoring was required (22patients, 42.3%): with noninvasive monitoring, 73.3% be-came seizure free, whereas the rate was 63.6% after inva-sive monitoring. In 7 patients with electrode implantations,however, results from intracranial monitoring resulted in
the suggestion to perform lesionectomies and MSTs, andall but 1 patient became seizure free (85.7%, Engel ClassI). Only 3 of these cases were occipital only, whereas theothers involved adjacent temporal, parietal, or both lobes.
Five patients had undergone previous operations. Onepatient with a remote history of hypoxia and right frontaland occipital porencephaly with gliotic scar formation hadundergone a right frontal lesionectomy 8 months prior with-out seizure relief; the occipital operation was the secondoperation and led to an Engel Class II outcome. Anotherpatient with an occipital ganglioglioma had undergone anincomplete occipital lesionectomy without sufficient sei-zure control and remnants of the tumor were detectable onMR imaging; this patient underwent a second operation 6months later that led to complete seizure control (EngelClass I). One patient had undergone an operation years be-fore for an AVM, and another underwent an operation for acavernoma. The former operations were only successful forextirpation of the malformations, but did not improve sei-zures, so that both patients underwent occipital reoperationsto resect gliotic scars in the adjacent occipital or occipi-
D. K. Binder et al.
62 J. Neurosurg. / Volume 109 / July 2008
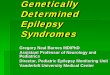
FIG. 2. Example of a patient with an occipital ganglioglioma. Preoperative axial FLAIR (A), sagittal (B), axial (C), andcoronal (D) inversion-recovery sequences (at 1.5 T) of a 14-year-old boy with seizure onset at 6 years of age who experi-enced 2.5 CPSs per month and 1 generalized seizure per year. An extended occipital lesionectomy and MSTs were per-formed using intraoperative ECoG. Histopathology revealed a WHO Grade I ganglioglioma. There was a new postopera-tive contralateral superior quadrantanopsia, and the patient was seizure free at 79 months (Engel Class I).

totemporoparietal area. Both patients became seizure free(Engel Class I). Another patient had undergone an opera-tion elsewhere for “gliosis,” which upon revision 3 yearslater was discovered to be a ganglioglioma, and an extend-ed resection led to complete seizure relief. Thus, of 5 pa-tients with a history of intracranial surgery, all 4 who under-went reoperations in the same area became seizure free.One patient with a distinct previous operation had an EngelClass II outcome.
Complications were noted in 2 patients (3.8%). In 1case, a postoperative epidural hematoma was found that re-quired drainage, without resulting in neurological deficit.In another case, postoperative intracranial hemorrhage ledto hemiparesis and dysphasia. A third patient with a left oc-cipitoparietal lesion had postoperative dyscalculia, whichwas transient and not considered a complication.
Follow-Up and Seizure Outcome
In the overall group of 52 patients, the mean follow-up
period was 6.7 years (range 4 months–14.4 years; Table4). A total of 36 patients (69.2%) were classified as seizurefree (Engel Class I), and 4 patients (7.7%) had rare nondis-abling seizures (Engel Class II). Thus, overall satisfacto-ry seizure outcome was achieved in 40 patients (76.9%).Eight patients (15.4%) were categorized in Engel Class III,and 4 patients (7.7%) experienced no significant improve-ment (Engel Class IV); thus, unsatisfactory seizure out-come was observed in 12 patients (23.1%).
In the subgroup of 29 patients with pure OLE, mean fol-low-up duration was 86.1 months (range 4–170 months).Twenty-three patients (79.3%) had . 24 months of follow-up. A total of 21 patients (72.4%) were seizure free (EngelClass I) and 2 patients (6.9%) had rare nondisabling sei-zures (Engel Class II); thus, satisfactory seizure outcomewas achieved in 79.3% of the pure OLE population. Threepatients (10.3%) were categorized in Engel Class III, and 3patients (10.3%) experienced no significant improvement(Engel Class IV); these patients were grouped together asunsatisfactory seizure outcome (20.7%).
J. Neurosurg. / Volume 109 / July 2008
Surgery for occipital lobe epilepsy
63
FIG. 3. Example of a patient with an occipital vascular malformation. Preoperative CT scans (A–C) and T1-weightedMR images (D–F) with gadolinium enhancement (at 1.5 T) of a 57-year-old man with seizure onset at 16 years of age whoexperienced 30 CPSs per month. Invasive monitoring with grid and subdural strip electrodes was performed, followed byan extended occipitobasal lesionectomy. Histopathology results revealed an AVM with calcification. There was a newpostoperative contralateral hemianopsia, and the patient was not seizure free at 33 months (Engel Class IV) despite com-plete resection as revealed by repeated MR imaging.

Factors analyzed as predictors of seizure outcome in-cluded the location of lesion, sex, age at operation, age atepilepsy onset, duration of epilepsy, seizure characteristics,and histopathological diagnosis. Neither preoperative sei-zure frequency nor presence of specific seizure types (SPSs,CPSs, or generalized seizures) predicted postoperative sei-zure outcome. There was no statistically significant dif-ference in seizure outcome by location of lesion (occipital,occipitoparietal, occipitotemporal, occipitotemporoparietal;Table 4) analyzed according to either Engel class (p =
0.368, Fisher exact test) or to satisfactory versus unsatisfac-tory seizure outcome (p = 0.478, Fisher exact test).
Age at operation did not have a statistically significanteffect on seizure outcome (p = 0.181; Fisher exact test).Similarly, age at epilepsy manifestation was not a statisti-cally significant predictor of seizure outcome according tochi-square analysis and nonparametric analysis (p = 0.168for satisfactory seizure control; Mann–Whitney U-test), butwas later significant in the logistic regression analysis (seebelow). Duration of epilepsy . 20 years was associated
D. K. Binder et al.
64 J. Neurosurg. / Volume 109 / July 2008
TABLE 4Summary of follow-up and seizure outcome
Engel Class* (%)
Group No. of Patients Mean Follow-Up Mos (range) I II III IV
all patients 52 80.3 (4–173) 36 (69.2) 4 (7.7) 8 (15.4) 4 (7.7)occipital only 29 86.1 (4–170) 21 (72.4) 2 (6.9) 3 (10.3) 3 (10.3)occipitoparietal 10 89.9 (12–173) 6 (60) 0 (0) 4 (40) 0 (0)occipitotemporal 9 60.1 (10–102) 5 (55.6) 2 (22.2) 1 (11.1) 1 (11.1)occipitotemporoparietal 4 60.1 (6–123) 4 (100) 0 (0) 0 (0) 0 (0)
* Number of patients in each class.
FIG. 4. Example of a patient with an occipital glial scar. Preoperative axial T2-weighted gradient echo (A–C) and coro-nal FLAIR TSE images (D–G) of a 36-year-old man with seizure onset at 6 years of age who experienced 6 SPSs permonth, 2.5 CPSs per month, and 2 generalized seizures per year. Invasive monitoring with depth electrodes and occipitalinterhemispheric strip electrodes was performed, followed by an extended occipital lesionectomy. Histopathology revealedglial scar/gliosis formation. The preoperative small scotoma enlarged into a postoperative contralateral upper quadrant-anopsia, and seizure outcome was Engel Class III (> 75% reduction in seizure frequency) at 80 months.

with poorer outcome (46.2% satisfactory seizure outcome)compared with , 20 years (p = 0.034, Fisher exact test;Table 5). These findings were confirmed by a nonparamet-ric analysis comparing age and seizure outcome, in whicha younger age at surgery correlated with better seizure con-trol (p = 0.003 for Engel Class I outcome and p = 0.002 forsatisfactory seizure control [Engel Class I or II]; Mann–Whitney U-test).
Seizure characteristics (seizure frequency or seizuretypes) were not associated with outcome. A positive pastmedical history for conditions such as trauma, intracranialhemorrhage, or hypoxia was not associated with alteredoutcome (p = 0.811, Fisher exact test). In addition, the pres-ence or absence and type of intracranial invasive monitor-ing failed to predict outcome.
We next considered whether histopathology results mayhave been associated with outcome. Table 6 demonstratesseizure outcome (Engel Class) according to histopatholog-ical group. The patients with the best seizure outcome werefound in the ganglioglioma group (89% Engel Class I, 11%Engel Class II), and the poorest outcome was seen in pa-tients in the “other tumor” group (50% Engel Class I, 0%Engel Class II). This difference was not statistically signif-icant (p = 0.565, Fisher exact test).
Multifactorial Analysis of Prognostic Factors
To formally analyze multiple clinical and surgical factorssimultaneously in the prediction of outcome, we performeda multifactorial univariate logistic regression analysis. Thedependent variable was satisfactory versus unsatisfactoryseizure outcome. Factors tested in the model were sex,EEG characteristics (including interictal and ictal EEGclassifications as described above and seizure frequencies),type and side of surgery, presence or absence of MST, pres-ence or absence of ECoG, presence or absence of invasivediagnostic monitoring, age at epilepsy manifestation, ageat operation, and epilepsy duration. A backward stepwiselogistic regression analysis was performed with inclusion ata probability value of 0.05 and exclusion at 0.10. Factorsexcluded successively from the model included all but 2factors: early age at epilepsy manifestation (p = 0.031) andshorter epilepsy duration (p = 0.004), which were pre-dictive for satisfactory outcomes. All other clinical factorswere not statistically significant in predicting outcome. Ad-ditional analysis with seizure freedom (Engel Class I) as adependent variable also revealed a shorter epilepsy dura-tion as a prognostic factor (p = 0.023), but not age at epilep-
sy manifestation (p = 0.187). Instead, female sex was foundto be correlated with being seizure free (p = 0.003).
Visual Field Outcome
In 33 cases, both adequate preoperative and postoper-ative visual field data were available for comparison. Ofthese 33 cases, 21 patients (63.6%) started with intact visu-al fields and 12 patients (36.4%) had preoperative visualfield deficits. Of those 21 patients with intact preoperativefields, 10 patients (47.6%) still had intact visual fields post-operatively; therefore, 11 patients (52.4%) had new defi-cits. These deficits consisted of a new scotoma/subquadrantdeficit in 2 cases, new quadrantanopsia in 3 cases, new in-complete hemianopsia in 3 cases, and new hemianopsia in3 cases. Of the 12 patients with preoperative visual fielddeficits, 9 patients (75%) had no worsening of visual fielddeficit and 3 patients (25%) experienced worsened deficitspostoperatively. In summary, new or aggravated visualfield deficits were seen in 14 (42.4%) of the 33 cases inwhich all the information was available.
Discussion
Diagnosis of OLE
Due to the relatively small number of patients who haveundergone operations so far for OLE, experience is stilllimited, for example, compared with TLE. Occipital lobeepilepsy appears to account for ~ 2–13% of extratempo-ral epilepsies.5,6,23,40 The literature indicates that there is astrong selection bias in extratemporal epilepsy patient se-ries, depending on referral, inclusion criteria, and consider-ation of potential surgical candidates.
We found an epilepsy duration of 17 years in the sub-group with pure OLE, whereas the epilepsy duration wasonly 9.5 years in the group with extended OLE (occipito-temporal, occipitoparietal, or occipitotemporoparietal epi-lepsies). This difference in seizure history was statistical-ly significant. In this context, it is interesting to note that alonger duration of epilepsy was 1 of 2 factors predictive ofpoorer outcome after surgery. Long epilepsy duration priorto surgical therapy may be related to several challenges indiagnosing and treating OLE. Many patients developedtheir epilepsies before the introduction of modern MR im-aging and before the reinstitution of epilepsy surgery inGermany in the 1980s. In contrast, more extended forms ofOLE resulted in shorter individual seizure history. One can
J. Neurosurg. / Volume 109 / July 2008
Surgery for occipital lobe epilepsy
65
TABLE 5Seizure outcome according to epilepsy
duration in 52 patients with OLE
Seizure Outcome* (%)
Epilepsy No. of Satisfactory UnsatisfactoryDuration (yrs) Patients (Engel Class I or II) (Engel Class III or IV)
,5 16 13 (81.3) 3 (18.8)5–10 10 9 (90.0) 1 (10.0).10–20 13 12 (92.3) 1 (7.7).20 13 6 (46.2) 7 (53.8)
* Number of patients in each category.
TABLE 6Seizure outcome according to
histopathological group in 52 patients with OLE
Engel Class* (%)Histopathological No. of
Group Patients I II III IV
all patients 52 36 (69.2) 4 (7.7) 8 (15.4) 4 (7.7)dysplasia 9 6 (66.7) 2 (22.2) 1 (11.1) 0 (0)ganglioglioma 9 8 (88.9) 1 (11.1) 0 (0) 0 (0)other tumor 6 3 (50) 0 (0) 2 (33.3) 1 (16.7)vascular malformation 13 10 (76.9) 0 (0) 2 (15.4) 1 (7.7)scar/gliosis formation 15 9 (60.0) 1 (6.7) 3 (20.0) 2 (13.3)
* Number of patients in each class.

assume that although these latter epilepsies are more wide-spread in nature, they may be considered as evolving fromless eloquent areas. The core of pure OLE is the mesial oc-cipital area and the occipital pole, both highly eloquent ar-eas, whereas extended forms of OLE mostly involve morelateral areas in which surgical resections can be performedwith less risk of persistent neurological deficits. This expla-nation is supported by the observation that patients withpure OLE had significantly more preoperative visual fielddeficits compared with the patients with extended OLE (48vs 14%, respectively; p = 0.003). This finding is consistentwith the study of Blume and colleagues9 who found visualfield deficits in 42% of patients with mesial OLE and nonein lateral OLE, whereas other clinical symptoms did not al-low them to distinguish between mesial and lateral OLE.Interestingly, semiological features characteristic of TLEwere found in 78% of the patients in the latter study. Thisis consistent with our finding of 83% CPSs in the pure OLEand the extended OLE subgroups, suggesting that ictal fea-tures do not allow differentiation between mesial or lateralOLE, nor between OLE and TLE.6,9,17
Electrophysiology and OLE
Because neither semiological nor EEG findings providereliably specific findings in OLE, diagnosis and selectionof patients for surgery is difficult. In the present study, allpatients had medically refractory epilepsy; however, MRimaging findings played a major role in nearly all patientsin suggesting occipital seizure localization. This lesion-based hypothesis was then furthered by analysis of clinicaland EEG findings. Thus, our approach was predominant-ly lesion-directed, and the vast majority of patients had le-sions documented in the occipital lobes or additionally inadjacent areas of parietal and/or temporal lobes.
Elementary visual hallucinations have been consistentlyfound as part of OLE semiology; however, TLEs can ex-hibit comparable features.6 Typical visual auras were foundin 61–68% of patients in recent studies of OLE or posteriorepilepsies, but they were not reliably lateralizing.8,22 Sala-nova and colleagues31 described visual auras in 73% of 42patients who underwent operations for OLE over a periodof . 60 years. Williamson et al.36 found only initial ictalsymptoms to provide information on the presumed seizurefocus in 88% of patients with OLE, whereas symptoms inthe later course of seizures were nonspecific: 44% expe-rienced seizures with typical temporal semiology, and thesame amount had multiple types of seizures. Boesebeckand associates10 hypothesized that with precise characteri-zation of auras it should be possible to lateralize the seizurefocus. This characterization had a significant impact onoutcome prediction: lateralizing auras resulted in completeseizure relief in 69%, whereas the rates were 28% onlywithout lateralizing auras, and false lateralization resultedin a 0% rate of seizure control. These findings were most-ly explained by the arbitrary borders of the occipital lobeand strong connections with temporal and parietal lobes,which enable fast propagation of seizure activity.23,33 Thus,if the initial symptoms are not determined, misdiagnosis ofTLE may result.
Interictal and ictal surface EEG recordings may contrib-ute to the generation of an adequate focus hypothesis insome cases insofar as they frequently indicate the hemi-
sphere (40.8% of interictal studies and 31.7% of ictal stud-ies) or even brain region (24.5% of interictal EEG studies,24.4% of ictal EEG studies) that is eventually shown tocontain the ictal onset area. To clarify potentially mis-leading clinical and electrophysiological results, evaluationusing intracranial electrodes may be necessary.29 Invasivemonitoring with implanted electrodes was performed in42% of patients in our study to define the epileptogenic ar-ea and to reliably differentiate seizure spread from occipi-tal origin versus nonoccipital seizure origin.
Imaging of OLE
Only 6 modern studies of OLE included only patientswho had undergone MR imaging prior to surgery.2,10,19,22,24
As in these modern studies, the vast majority of patients inour study (50 [96%] of 52) showed MR-detectable lesions.Thus, we took a lesion-directed approach in this study, butidentification of a lesion alone is not sufficient to offer epi-lepsy surgery to the patient. Magnetic resonance imagingproved to be very sensitive, but MR imaging specificity waslower: 87% for scars and cysts, 79% for tumors, and sur-prisingly only 54% for vascular malformations. The leastspecificity was attained in cortical malformations (33%).Clinically a high sensitivity is most important, however,and clearly in this group of patients MR imaging proved tobe the major adjunct to the diagnostic armamentarium. Thepresence of a lesion on MR imaging is generally acceptedto portend a better prognosis for becoming seizure free.12,40
The introduction of modern MR neuroimaging has facili-tated the identification of occipital lesions.2,3,22 It should benoted that 2 lesions were undetected using MR imaging inour sample, but nevertheless MR sensitivity was 96%. Theclinical impact of the lower specificities may be of less im-portance, because initial treatment planning is not primari-ly dependent on histopathological diagnosis.
In nonlesional cases or cases with ambiguous MR imag-es, FDG-PET and ictal SPECT have been especially help-ful in defining the epileptogenic zone.19,22,40 In 23% of cas-es, we made use of FDG-PET to support the clinical and/orimaging hypothesis. In 10 of 12 cases, the FDG-PET datasupported the MR imaging and clinical findings, and in 2cases the results were discordant. Ictal SPECT was per-formed in 3 patients in our series, and in each case hyper-perfusion ipsilateral to the lesion was observed. When ictalinjection was not possible, however, interictal SPECT wasperformed in 9 patients, and only 67% resulted in lateral-izing findings. Kim et al.19 found ictal SPECT to be suffi-ciently lateralizing in 76%, but the correct localization waspossible in only 29%. In their study, FDG-PET was superi-or in localizing epileptogenic zones, showing 93% correctlateralization and 60% correct localization.19 Thus, FDG-PET and SPECT can be regarded as diagnostic adjuncts,but they must be interpreted carefully and further study isnecessary to determine the specific role of each modali-ty.22,23 In 1 case in our series, FDG-PET and SPECT re-vealed contradictory results.
Surgery and Complications
The majority of patients (43 [83%] of 52) underwent le-sionectomies tailored to include the lesion and the sur-rounding presumed epileptogenic zones as derived fromnoninvasive or invasive EEG monitoring. In a few cases,
D. K. Binder et al.
66 J. Neurosurg. / Volume 109 / July 2008

results from FDG-PET and SPECT were also consideredfor resection planning. In some cases, the resection waslimited when preservation of visual fields was intended, butrestricting the extent of resection may worsen outcome.8,33
Epileptogenic zones are known to be quite extensive in oc-cipital epilepsies,31 often involving posterior temporal andparietal regions, so that it is often difficult to achieve com-plete resection with an acceptable risk for permanent neu-rological deficits. Furthermore, it is possible that the epi-leptogenic focus may be distant from the morphologicallesion, due to either fast propagation and/or intense cou-pling of the structures involved.1,33 Proximity to eloquentareas is the main reason that most patients underwent ex-tended lesionectomies, and only 9 patients (17%) under-went lobectomies. In 9 patients, the planned lesionectomieswere not able to encompass the entire presumed epilep-togenic zone, as derived from invasive EEG monitoring;these patients underwent additional MST. Six of these 9patients became completely seizure free, and another 3had significant improvement in seizure frequency. Otherstudies have previously shown that MST may be a help-ful surgical adjunct in eloquent areas, because seizure out-come can be superior when combined with a resective ap-proach.32,38
Five patients had a history of previous intracranial sur-gery for different diseases, which resulted mostly in incom-plete resection. All 4 patients who underwent reoperationsin the same area as before became seizure free after occip-ital epilepsy surgery. Thus, reoperation should be con-sidered in those cases with residual MR imaging–visiblelesions, and resection of a glial scar alone may be quitebeneficial in individual cases.
A concern for occipital lobe surgery is aggravation ofexisting or creation of new visual field defects. Preopera-tively, visual field deficits were present in 36% of patients,and 42% had new or aggravated visual field deficits aftersurgery. These results compare well with those in publishedfindings.8,9,22 In addition, several authors have found thatvisual field deficits are rarer in lateral OLE compared withmesial OLE, which is understandable based on the locationof the calcarine cortex and is also supported by our data onextended OLE. Clearly, the informed consent process mustinvolve a frank discussion of the likelihood of visual fieldloss following OLE surgery.
Histopathological Findings
Histopathological diagnoses were obtained in all 52cases. The most common finding was glial scars/gliosis(29%), followed by vascular malformations (25%), gan-gliogliomas (17%), dysplasias (17%), and other tumors(12%). The spectrum of these occipital lesions is differentfrom other areas of the brain and has not previously beendescribed in detail. Other investigators have found a pre-dominance of malformations of cortical development ortumors.2,28 In our series, 2 of the astrocytomas were WHOGrade I, 2 were Grade II, and 1 was Grade III, which cor-responds to larger patient cohorts who underwent epilepsysurgery.26 The most notable result was that 15 cases of glialscar/gliosis were found, with variable evidence of otherpathological features such as cortical and subcortical astro-cytosis, hemosiderin deposition, microglial activation, andcyst formation. Some of these cases were related to clear
evidence of prior trauma. The predominance of this di-agnosis emphasizes the importance of glial scars not onlyin the classic location of mesial temporal sclerosis but al-so in contributing to occipital epileptogenesis.7 Gliotic le-sions can be associated with continuous epileptiform dis-charges.16
Outcome Predictors
Of 52 patients with a mean follow-up of 6.7 years, 36(69.2%) were classified as seizure free (Engel Class I), and4 (7.7%) had rare nondisabling seizures (Engel Class II).Thus, overall satisfactory seizure outcome was achieved in40 patients (76.9%). Eight patients (15.4%) were catego-rized in Engel Class III, and 4 patients (7.7%) experiencedno significant improvement (Engel Class IV); thus, unsat-isfactory seizure outcome was observed in 12 patients(23.1%). Our outcome results are better compared withthose in older patient series, although direct comparison isdifficult due to differences in patient selection and use ofdifferent classification schemes. As illustrated in Table 7,however, seizure-free outcomes were attained in 33–50% ofpatients in most of the larger studies, which were publishedin the 1990s. The results of the more recent studies on sur-gical treatment of OLE described seizure control rates sim-ilar to ours. It appears that the introduction of modern MRimaging, video-EEG monitoring, and individualized use ofinvasive monitoring improved the seizure-free outcome ofepilepsy surgery in the occipital lobe by ~ 20%. Similarimprovements over time have been noted for TLE sur-gery.12,34
In the subgroup of 29 patients with pure OLE, a total of21 patients (72.4%) were seizure free (Engel Class I) and 2patients (6.9%) had rare nondisabling seizures (Class II);thus, satisfactory seizure outcome was achieved in 79.3%of the pure OLE population. With more extended occipitalsurgery in 23 patients, similar results were obtained (65.2%Engel Class I and 8.7% Engel Class II), resulting in 74%satisfactory seizure relief in this subgroup. There was nosignificant difference in seizure outcome according to thelocation of the lesion (occipital, occipitoparietal, occipi-totemporal, or occipitotemporoparietal). Furthermore, nei-ther clinical, semiological, or EEG factors correlated withoutcome. With respect to histopathology, the best seizureoutcome was noted in the ganglioglioma group (89% EngelClass I and 11% Engel Class II), and the poorest outcomewas noted in the “other tumor” group (50% Engel Class Iand 0% Engel Class II). Similar findings have been de-scribed for TLE, and these results support the idea of thespecial behavior of the developmental tumors and their rolein long-term epilepsy.2,12,26,27,40
We found that young age at epilepsy manifestation wasa significant predictor of satisfactory seizure outcome insome analyses. Duration of epilepsy was associated withpoorer outcome in our study, whereas age at operation wasnot predictive. Other studies have reported that duration ofepilepsy may affect outcome, although this is not consis-tently reported to be significant.15,18 In a recent study of 44patients with posterior cortex epilepsies, Dalmagro et al.13
found that a favorable outcome was associated with short-er epilepsy duration. This finding, together with our data,suggests that an earlier operation is preferable. The epilep-sy duration of 17 years in our pure OLE subgroup should
J. Neurosurg. / Volume 109 / July 2008
Surgery for occipital lobe epilepsy
67

be regarded as a challenge to accelerate patient selectionand presurgical evaluation.
Conclusions
Occipital lobe epilepsy is a rare but significant causeof extratemporal epilepsy. Satisfactory results (Engel ClassI or II) were obtained in 77% of patients in our series witha mean follow-up of 6.7 years. Our study supports the im-provement of seizure outcomes in the modern era withhigh-resolution MR imaging and careful video-EEG mon-itoring and other appropriate tests. Postoperative visualfield deficits occur in a significant proportion of patients.Long epilepsy duration is a negative prognostic factor, sug-gesting that diagnosis and treatment of patients with lesion-al OLE should be performed early for better outcome.
Acknowledgments
We thank Dr. T. Pietsch and Dr. A. Becker for providing histolog-ical findings and diagnoses. We also thank Dr. C. E. Elger for con-tinuous support and helpful discussions.
References
1. Awad IA, Rosenfeld J, Ahl J, Hahn JF, Luders H: Intractable epi-lepsy and structural lesions of the brain: mapping, resection strate-gies, and seizure outcome. Epilepsia 32:179–186, 1991
2. Aykut-Bingol C, Bronen RA, Kim JH, Spencer DD, Spencer SS:Surgical outcome in occipital lobe epilepsy: implications forpathophysiology. Ann Neurol 44:60–69, 1998
3. Aykut-Bingol C, Spencer SS: Nontumoral occipitotemporal epi-
lepsy: localizing findings and surgical outcome. Ann Neurol 46:894–900, 1999
4. Bautista RE, Cobbs MA, Spencer DD, Spencer SS: Prediction ofsurgical outcome by interictal epileptiform abnormalities duringintracranial EEG monitoring in patients with extrahippocampalseizures. Epilepsia 40:880–890, 1999
5. Bidzinski J, Bacia T, Ruzikowski E: The results of the surgicaltreatment of occipital lobe epilepsy. Acta Neurochir (Wien) 114:128–130, 1992
6. Bien CG, Benninger FO, Urbach H, Schramm J, Kurthen M, ElgerCE: Localizing value of epileptic visual auras. Brain 123:244–253, 2000
7. Binder DK, Steinhäuser C: Functional changes in astroglial cellsin epilepsy. Glia 54:358–368, 2006
8. Blume WT, Whiting SE, Girvin JP: Epilepsy surgery in the poste-rior cortex. Ann Neurol 29:638–645, 1991
9. Blume WT, Wiebe S, Tapsell LM: Occipital epilepsy: lateral ver-sus mesial. Brain 128:1209–1225, 2005
10. Boesebeck F, Schulz R, May T, Ebner A: Lateralizing semiologypredicts the seizure outcome after epilepsy surgery in the posteri-or cortex. Brain 125:2320–2331, 2002
11. Clusmann H, Kral T, Schramm J: Present practice and perspectiveof evaluation and surgery for temporal lobe epilepsy. ZentralblNeurochir 67:165–182, 2006
12. Clusmann H, Schramm J, Kral T, Helmstaedter C, Ostertun B,Fimmers R, et al: Prognostic factors and outcome after differenttypes of resection for temporal lobe epilepsy. J Neurosurg 97:1131–1141, 2002
13. Dalmagro CL, Bianchin MM, Velasco TR, Alexandre V Jr, WalzR, Terra-Bustamante VC, et al: Clinical features of patients withposterior cortex epilepsies and predictors of surgical outcome.Epilepsia 46:1442–1449, 2005
14. Engel J Jr, Van Ness P, Rasmussen TB, Ojemann LM: Outcomewith respect to epileptic seizures, in Engel J Jr (ed): Surgical
D. K. Binder et al.
68 J. Neurosurg. / Volume 109 / July 2008
TABLE 7Summary of studies of surgery for OLE*
Authors & Year Patient Characteristics Outcome/Comments
Dalmagro et al., 2005 44 patients w/ pst cortex epilepsies (oc- 65% seizure free; favorable outcome associated w/ shorter epi- cipital, parietal, occipitotemporal) lepsy duration
Kun Lee et al., 2005 26 patients w/ OLE FU .2 yrs; 61.5% seizure freeBoesebeck et al., 2002 42 patients w/ lesional focal epilepsies of 2-yr FU; 45% seizure free; favorable outcome associated w/
occipitoparietal or occipitotemporal lateralizing semiology (auras or seizures), tumors, & absence lobes treated btwn 1990 & 1999 of postop IED
Olivier & Boling, 2000 39 occipital resections in 30 patients 71% seizure free; benign tumors most common group (33%)Bautista et al., 1999 8 patients w/ pst resections FU not mentioned; 25% seizure free, 38% marked seizure re-
duction; poor outcome associated w/ extralesional IEDAykut-Bingol et al., 35 patients w/ OLE FU .1 yr; 46% seizure free; 12% marked seizure reduction;
1998 developmental malformations worse outcome compared w/tumors
Kuzniecky et al., 1997 10 patients w/ occipital dysplasias FU 2–5 yrs; 30% seizure free, 70% marked seizure reductionZentner et al., 1996 13 occipital resections in 60 patients w/ 54% seizure free, 20% ,2 seizures/yr; favorable seizure out-
extratemporal epilepsy come associated w/ tumor pathologyBidzinski et al., 1992 12 patients (2%) w/ an occipital focus out 11/12 had satisfactory result; 9/12 had brain scarring on histol-
of 502 patients treated in Warsaw btwn ogy1957 & 1989
Salanova et al., 1992 42 occipital resections performed at the mean FU 17 yrs (range 1–46 yrs); 46% seizure free, 21% Montreal Neurological Institute btwn marked seizure reduction; poor outcome associated w/ postop1930 & 1991 IED
Williamson et al., 1992 16 patients w/ occipital resections FU not mentioned; 88% w/ “excellent” resultsBlume et al., 1991 19 patients w/ seizure foci in occipital or median FU 3.7 yrs (range 1–14 yrs); 32% seizure free, 68%
pst temporoparietal cortex marked seizure reduction; poor outcome associated w/ in-complete resection, age of epilepsy onset, & extralesional IED
Wyler & Hermann, 14 patients w/ OLE 50% seizure free1990
* FU = follow-up; pst = posterior.

Treatment of the Epilepsies, ed 2. New York: Raven Press,1993, pp 609–621
15. Grivas A, Schramm J, Kral T, von Lehe M, Helmstaedter C, ElgerCE, et al: Surgical treatment for refractory temporal lobe epilepsyin the elderly: seizure outcome and neuropsychological sequelscompared with a younger cohort. Epilepsia 47:1364–1372, 2006
16. Guerreiro MM, Quesney LF, Salanova V, Snipes GJ: Continuouselectrocorticogram epileptiform discharges due to brain gliosis. JClin Neurophysiol 20:239–242, 2003
17. Huott AD, Madison DS, Niedermeyer E: Occipital lobe epilepsy.A clinical and electroencephalographic study. Eur Neurol 11:325–339, 1974
18. Janszky J, Janszky I, Schulz R, Hoppe M, Behne F, Pannek HW,et al: Temporal lobe epilepsy with hippocampal sclerosis: predic-tors for long-term surgical outcome. Brain 128:395–404, 2005
19. Kim SK, Lee DS, Lee SK, Kim YK, Kang KW, Chung CK, et al:Diagnostic performance of [18F]FDG-PET and ictal [99mTc]-HMPAO SPECT in occipital lobe epilepsy. Epilepsia 42:1531–1540, 2001
20. Kleihues P, Sobin LH: World Health Organization classificationof tumors. Cancer 88:2887, 2000
21. Kral T, Clusmann H, Urbach H, Schramm J, Elger CE, KurthenM, et al: Preoperative Evaluation for Epilepsy Surgery (Bonn Al-gorithm). Zentralbl Neurochir 63:106–110, 2002
22. Kun Lee S, Young Lee S, Kim DW, Soo Lee D, Chung CK:Occipital lobe epilepsy: clinical characteristics, surgical outcome,and role of diagnostic modalities. Epilepsia 46:688–695, 2005
23. Kuzniecky R: Symptomatic occipital lobe epilepsy. Epilepsia 39(4 Suppl):S24–S31, 1998
24. Kuzniecky R, Gilliam F, Morawetz R, Faught E, Palmer C, BlackL: Occipital lobe developmental malformations and epilepsy:clinical spectrum, treatment, and outcome. Epilepsia 38:175–181, 1997
25. Lee SK, Lee SY, Kim KK, Hong KS, Lee DS, Chung CK: Sur-gical outcome and prognostic factors of cryptogenic neocorticalepilepsy. Ann Neurol 58:525–532, 2005
26. Luyken C, Blümcke I, Fimmers R, Urbach H, Elger CE, WiestlerOD, et al: The spectrum of long-term epilepsy-associated tumors:long-term seizure and tumor outcome and neurosurgical aspects.Epilepsia 44:822–830, 2003
27. Luyken C, Blümcke I, Fimmers R, Urbach H, Wiestler OD,Schramm J: Supratentorial gangliogliomas: histopathologic grad-ing and tumor recurrence in 184 patients with a median follow-upof 8 years. Cancer 101:146–155, 2004
28. Olivier A, Boling W Jr: Surgery of parietal and occipital lobe epi-lepsy. Adv Neurol 84:533–575, 2000
29. Palmini A, Andermann F, Dubeau F, Gloor P, Olivier A, QuesneyLF, et al: Occipitotemporal epilepsies: evaluation of selected pa-tients requiring depth electrodes studies and rationale for surgicalapproaches. Epilepsia 34:84–96, 1993
30. Rasmussen T: Surgery for epilepsy arising in regions other thanthe temporal and frontal lobes. Adv Neurol 8:207–226, 1975
31. Salanova V, Andermann F, Olivier A, Rasmussen T, Quesney LF:Occipital lobe epilepsy: electroclinical manifestations, electrocor-ticography, cortical stimulation and outcome in 42 patients treat-ed between 1930 and 1991. Surgery of occipital lobe epilepsy.Brain 115:1655–1680, 1992
32. Schramm J, Aliashkevich AF, Grunwald T: Multiple subpial tran-sections: outcome and complications in 20 patients who did notundergo resection. J Neurosurg 97:39–47, 2002
33. Sveinbjornsdottir S, Duncan JS: Parietal and occipital lobe epilep-sy: a review. Epilepsia 34:493–521, 1993
34. Tellez-Zenteno JF, Dhar R, Wiebe S: Long-term seizure outcomesfollowing epilepsy surgery: a systematic review and meta-analy-sis. Brain 128:1188–1198, 2005
35. Urbach H, Hattingen J, von Oertzen J, Luyken C, Clusmann H,Kral T, et al: MR imaging in the presurgical workup of patientswith drug-resistant epilepsy. AJNR Am J Neuroradiol 25:919–926, 2004
36. Williamson PD, Thadani VM, Darcey TM, Spencer DD, SpencerSS, Mattson RH: Occipital lobe epilepsy: clinical characteristics,seizure spread patterns, and results of surgery. Ann Neurol 31:3–13, 1992
37. Wolf HK, Zentner J, Hufnagel A, Campos MG, Schramm J, ElgerCE, et al: Surgical pathology of chronic epileptic seizure disor-ders: experience with 63 specimens from extratemporal cortic-ectomies, lobectomies and functional hemispherectomies. ActaNeuropathol 86:466–472, 1993
38. Wyler AR: Recent advances in epilepsy surgery: temporal lobec-tomy and multiple subpial transections. Neurosurgery 41:1294–1301, 1997
39. Wyler AR, Hermann BP: Surgical treatment of occipital lobe epi-leptogenic foci. Epilepsia 31:638, 1990
40. Yun CH, Lee SK, Lee SY, Kim KK, Jeong SW, Chung CK: Prog-nostic factors in neocortical epilepsy surgery: multivariate anal-ysis. Epilepsia 47:574–579, 2006
41. Zentner J, Hufnagel A, Ostertun B, Wolf HK, Behrens E, CamposMG, et al: Surgical treatment of extratemporal epilepsy: clinical,radiologic, and histopathologic findings in 60 patients. Epilepsia37:1072–1080, 1996
Manuscript submitted April 7, 2007.Accepted October 8, 2007.Sources of support: Devin K. Binder, M.D., Ph.D., was supported
by a van Wagenen Fellowship from the American Association ofNeurological Surgeons. Johannes Schramm, M.D., and ThomasKral, M.D., are supported by the Deutsche Forschungsgemeinschaft,Transregio Sonderforschungsbereich TR3.
Address correspondence to: Devin K. Binder, M.D., Ph.D., De-partment of Neurological Surgery, University of California, Irvine,101 The City Drive South, Building 56, Suite 400, ZOT 5397,Orange, California 92868-3298. email: [email protected].
J. Neurosurg. / Volume 109 / July 2008
Surgery for occipital lobe epilepsy
69