Embed Size (px)
Citation preview

Thorax (1955), 10, 321.
SURGICAL TREATMENT OF ACQUIRED TRICUSPIDSTENOSIS
BY
JUDSON T. CHESTERMAN AND WILLIAM WHITAKERFromti the Department of Thoracic Surgery and the Regional Cardiovascular Centre, the Citi' General
Hospital, Sheffield, and the University Department of Medicine, the Royal Hospital, Sheffield
(RECEIVED FOR PUBLICATION AUGUST 29, 1955)
Tricuspid stenosis has now come within theambit of surgery, and, as always, the possibility ofsurgical intervention demands an accuracy ofdiagnosis which was previously unnecessary andusually unattained.
Acquired tricuspid stenosis was known toMorgagni in 1761, and, in spite of its rarity whencompared with mitral and aortic disease, Rolleston(1941) reported that Leudet was able to collect114 cases in 1888. The incidence of the involve-ment of the individual valves in chronic rheumaticcarditis is given by Wood (1954) as mitral 80%,aortic 48%, tricuspid 12%, and pulmonary 5%.Wood (1954) further states that at a " conservativeestimate" 3,000 mitral valvotomies should becarried out annually in Great Britain, and ittherefore seems probable that about 50 tricuspidvalvotomies a year is an appropriate figure on thebasis that about 15% of cases of tricuspid diseasehave predominantly stenotic lesions.
DIAGNOSISThere are certain features in the history of a
patient who is suffering from a chronic cardiaclesion which suggest the possibility of tricuspiddisease. First, Thompson and Levine (1937)point out that any adult patient who has repeatedattacks of oedema and ascites, and yet is able tolead a sedentary life with the aid of diuretics andcarry on with symptoms that ordinarily wouldcause his early demise, probably has tricuspidstenosis. Second, Cooke and White (1941) stressthat a patient with rheumatic carditis and asciteswho is able to sleep without extra pillows prob-ably has tricuspid stenosis, which accounts for theabsence of pulmonary congestion. Finally ortho-pnoea, usually a terminal symptom, may, accord-ing to Altschule and Blumgart (1937), be earlyand incapacitating if the systemic venous conges-tion is so marked that it rises to a level corre-sponding approximately to that of the respiratorycentres in the brain. In less marked cases com-
plaint may be made of fullness and congestion ofthe face and head.The first glance at the patient is often suggestive
of tricuspid disease on account of the bronzecoloration of the face, which is best seen on thetemporal region of the forehead and by the sidesof the nose. This coloration, known as Shattuck'ssign, has been attributed by Altschule and Blum-gart (1937) and Altschule and Budnitz (1940) to acombination of cyanosis and jaundice, the formeroccurring in dilated cutaneous veins and venulesand the latter being due to liver insufficiency.However, the pigmentation may be present inpatients without elevation of the serum bilirubinlevel, suggesting that jaundice is not an importantfactor in its production. Skin biopsies frompigmented areas of the forehead show no abnormalpigment such as haemosiderin, and the colorationis probably due to an increased melanin contentalthough such an increase cannot be detected byordinary histological examination. It has beenobserved to disappear some months after a suc-cessful tricuspid valvotomy (Case 2).
Closer observation shows abnormal distensionand pulsat on of the veins of the neck. In patientswith sinus rhythm giant " a" waves, with theircharacteristic sudden rise in presystole and rapidfall, are visible in the jugular venous pulse whenthere is tricuspid stenosis. These giant " a " wavesare associated with increased right atrial pulsepressure. In chronic rheumatic heart disease theyare usually related to pulmonary hypertension ortricuspid stenosis, and the latter is recognized asthe probable cause by the exclusion of the former.Whitaker (1954) has pointed out that the clinicalrecognition of pulmonary hypertension in patientswith mitral stenosis is made by noting a systoliclift over the right ventricular outflow tract, apalpable second heart sound, auscultating a splitsecond heart sound with a loud second component,combined with radiological evidence of prominentpulmonary arteries and electrocardiographic signsof right ventricular hypertrophy.
on June 3, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.10.4.321 on 1 Decem
ber 1955. Dow
nloaded from

JUDSON T. CHESTERMAN and WILLIAM WHITAKER
Ij
le ..
ji~ ~ ~ ~ i~
f v 8wAf
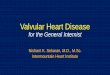
FIG. 1.-Synchronous records of the electrocardiogrami and thejugular plhlebogram showing giant " a" waves in a patient withtricuspid stenosis (Case 2).
FIG. 2.-Postero-anterior teleradiographs showing right atrialenlargement, all cases; normal pulmonary arteries, Cases 2(tricuspid stenosis) and 1 (tricuspid and mitral stenosis); enlargedpulmonary arteries, Case 4 (advanced tricuspid and mitralstenosis with mean pulmonary arterial blood pressure of55 mm. Hg); and pericardial effusion and pericardial adhesionsCase 3 (advanced tricuspid and mitral stenosis).
FIG. 2
322
...
'97-Opp"I"
....
on June 3, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.10.4.321 on 1 Decem
ber 1955. Dow
nloaded from

._ _ ~~~~~~~~~. ___......
V3R VI \\ 2 /3 V4 VS YE6
:~~~~~~~~~~.... :.._-...
The phlebogram in tricuspidstenosis when auricular fibrilla-tion is present is of doubtfulsignificance.The increased right atrial pulse
pressure produces not only giant" a " waves in the venous pulse,but is also transmitted to theliver to give a presystolic pulsa-tion of the liver which must bedifferentiated from the systolicpulsation characteristically asso-ciated with tricuspid incom-petence.
Auscultation may show adiastolic murmur localized tothe lower left border of thesternum, but sometimes it maybe either central in position oreven to the right of the midlinein the region of the fourth andfifth costal cartilages. Difficultyis experienced owing to the tri-valvular nature of many of thesecases and by the all but invari-able involvement of the mitralvalve.
Careful auscultation may sug-gest tricuspid stenosis by thelocalization of the murmurs andtheir lessening intensity in pass-ing between their maximum sitesat the lower end of the sternumand the mitral area. The tricuspiddiastolic murmur may be furtheraccentuated by listening during
.'
V3R VI
C-,-- .._ .
.......-.iF
V2 V3 V4 Vs V6~~V.WA,MP,loon
H..aVR
aVF IlI
aVL
_%gAe
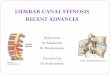
FIG. 3.-Electrocardiograms recorded before operation. The tallpointed P waves in lead II are evidence of tricuspid stenosisin Case 2, tricuspid stenosis in Case 1, tricuspid and mitralstenosis without pulmonary arterial hypertension in Case 4,tricuspid and mitral stenosis with mean pulmonary arterialhypertension of 55 mm. Hg.
VI V2 V3 V4 V5
.! v I,.........
-N.
aVF
C - S .... __avR I at
I
"'i
".014
on June 3, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.10.4.321 on 1 Decem
ber 1955. Dow
nloaded from

JUDSON T. CHESTERMAN and WILLIAM WHITAKER
inspiration and with the patient lying on theright side, in contradistinction to the mitraldiastolic murmur, which is best heard with thepatient lying on the left side and in expiration.In some cases the tricuspid murmurs are of ahigher frequency and resemble the cry of a sea-
gull. This " sea-gull " murmur may be diastolic or
systolic, presumably depending on the main lesionin the valve.The tricuspid diastolic murmur is of significance
when present, but its absence does not excludetricuspid stenosis, as murmurs originating frommitral valvular disease may render inaudible anysounds produced at the tricuspid valve. Kossmann(1955) has recorded an " opening snap" in tricuspidstenosis, and Wood (1950) states that there maybe a localized thrill at the lower end of thesternum. Phonocardiography has not proved a
diagnostic aid in our experience.Radiological examination shows definite right
atrial enlargement. Normal pulmonary arteriesare seen except in the more uncommon case whenpulmonary hypertension due to mitral stenosis ispresent. The oesophagus is displaced posteriorly.Grossly increased pericardial fluid may be foundin advanced cases and is attributed by Altschuleand Budnitz (1940) to the high venous pressure inthe coronary sinus.
Electrocardiography may be suggestive if show-ing in lead lI the increased and pointed P waveof right atrial hypertrophy rather than the flatteror even bifid P wave of left atrial hypertrophytogether with the absence of ventricular hyper-trophy. However, as Smith and Levine (1942)found auricular fibrillation in 55% of their casesof tricuspid stenosis and as other valvular lesionsare almost invariably present, the electrocardio-gram may not be of much diagnostic value.The clinical diagnosis of tricuspid stenosis may
be made by noting the giant "a" waves, theabsence of pulmonary hypertension, the presenceof the typical tricuspid diastolic murmurs, and theelectrocardiographic evidence of an increased andpointed P wave in lead II. However, some ofthese diagnostic points may be absent or equivocalin patients with tricuspid stenosis. In that case
the pathognomonic sign is the altered pressuregradient found on cardiac catheterization of theright side of the heart. Normally the diastolicblood pressures in the right atrium and the rightventricle are equal. When tricuspid stenosis ispresent the atrial diastolic blood pressure is raisedabove that of the ventricle, and in patients withsinus rhythm the atrial pulse pressure is abnorm-ally high and the pulse pressure is not transmitted
to the ventricle. The same type of pressuregradient is found when auricular fibrillation ispresent, and is diagnostic of tricuspid stenosis.If marked tricuspid incompetence is also presentthere is a definite atrial rise in pressure duringventricular systole (Chesterman and Whitaker,1954; Whitaker, 1955).
TREATMENTA major problem in treatment is to decide
which valve should be operated upon first, as bothtricuspid and mitral valves are usually involvedtogether. Neptune and Bailey (1954), who didthe first tricuspid valvotomy in 1952, have solvedthis difficulty by operating upon both valves atthe same operation through a right-sided approach.Brock has operated upon the mitral, aortic, andtricuspid valves at one time by using a transversesternal splitting incision. We have used this trans-verse sternal incision continued on both sides intothe fourth intercostal spaces in Case 5, but pre-viously we had endeavoured to decide which valvewas responsible for the greater degree of incapacityand to operate upon that one first. If in doubtwe prefer to operate upon the mitral valve firstso that excessive pulmonary congestion will nottake place. However, if the main disability is dueto the raised systemic venous pressure as evidencedby the marked congestion of the face and head,we prefer to operate upon the tricuspid valve first.We reassess the patients at short intervals afteroperation and proceed to the second valvotomyif necessary when we feel maximum relief hasbeen obtained from the first operation.
RESULTSWe have had five cases of proved tricuspid
stenosis which we deemed needed tricuspid valvo-tomy. Three of these were submitted to mitralvalvotomy first and one to tricuspid valvotomy asthe initial operation. In the last case first mitralthen tricuspid valvotomy were performed at thesame operation.CASE 1 (53/20397).-A married woman, aged 22,
sought advice in May, 1953, as her disability wasincreasing and she was now breathless after climbingsix steps. She had never suffered from nocturnaldyspnoea, haemoptysis, emboli, or congestive heartfailure (Chesterman and Whitaker, 1954). She pre-sented the typical features of both mitral and tricuspidstenosis. On June 16 a diaphragmatic mitral stenosisof I cm. long was split. She obtained some relief, buther exertional dyspnoea was but little changed. InOctober, 1953, she developed paroxysmal tachycardiaand was readmitted as an emergency with loss ofconsciousness during an attack. This was attributedto the lessened output.
324
on June 3, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.10.4.321 on 1 Decem
ber 1955. Dow
nloaded from

On November 17. 1953, tricuspidvalvotomy was done and the valvesplit from 3 cm. to about 3 cm.Slight regurgitation was present butwas unaffected by the operation.Now (May 18, 1955) the patient is
able to do all her housework and walkup hills.CASE 2 (54/31 536).-A married
woman, aged 40, suffered fromexertional dyspnoea which limitedher walking to short distances on thelevel ; she complained particularly ofcongestion of the face. She was aclassical case of tricuspid stenosis.On April 13, 1954, tricuspid valv-
otomy was performed and the valvewas split from+ cm. to 3 cm. Slightregurgitation, unaltered by the opera-tion, was present.When seen on May 17, 1955, her
condition had greatly improved. Shecan do all her own housework and alsogoes out part time to a factory. Shecan walk normally on the level.Mitral valvotomy has not yet beenconsidered necessary.
.20
FI 4a,
-50
Fla. 4c
353025J 20
Eio. 4d
30
~-20
-As1~~~~~~~~~I0
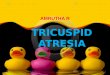
FIG. 4.-Blood pressure records (mm. Hg) from theright ventricle and right atrium of patients withtricuspid stenosis. Case 2, tricuspid stenosis.Case 1, tricuspid and mitral stenosis. Case 4,tricuspid and mitral stenosis with pulmonaryarterial hypertension. Case 3, tricuspid andmitral stenosis with auricular fibrillation. Case 5,tricuspid and mitral stenosis with auricularfibrillation.
FiGo 4e
on June 3, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.10.4.321 on 1 Decem
ber 1955. Dow
nloaded from

JUDSON T. CHESTERMAN and WILLIAM WHITAKER
CASE 3 (54/34821).-A married woman, aged 39,had typical advanced mitral and tricuspid stenosis withauricular fibrillation and ascites for which she requiredfrequent tapping. She had been refused operation inLondon one year previously.On July 6, 1954, mitral valvotomy, and on Sep-
tember 21 tricuspid valvotomy, were performed; bothshowed an orifice of 1{ cm. long and both split to3 cm. without any increase of the mild regurgitationalready present. She made slow but steady progressuntil she developed bronchopneumonia (proved atnecropsy) and died on December 12.CASE 4 (53/27631).-A married woman of 25 had
suffered from congestive heart failure and subacutebacterial endocarditis early in 1954 after seven yearsof increasing breathlessness.Her maximum cardiac output was 1.7 litres a minute
and her mean pulmonary arterial pressure was55 mm. Hg.
Mitral valvotomy was done on September 9, 1954,and the cusps were cut from 3 cm. to 2{ cm. Un-fortunately spontaneous respiration was never regainedand she died in a respirator several hours later.Necropsy confirmed the tricuspid stenosis of 3 cm.orifice in length.CASE 5 (54/41254).-A married woman of 33 had
been in congestive heart failure in October, 1954, whenshe refused operation but finally consented after acerebral embolus in May, 1955.She was a classical case of tricuspid and mitral
stenosis with auricular fibrillation.On July 27, 1955, mitral and tricuspid valvotomies
were performed, each orifice being split from 1 cm. to3 cm. in length. The immediate result showed markedimprovement.
OPERATION
There are three points in regard to the actualoperation which are worth mentioning.
First, the approach to the right atrium is madethrough a postero-lateral incision with resection ofpart of the fifth or sixth right rib, as this givesgood access, less post-operative pain, and betterreconstruction of the chest wall than a moreanterior incision and also avoids the risk of oozingand sepsis in the breast. If, however, other valvesbesides the tricuspid may have to be dealt withat the same operation, then adequate exposurecan be obtained by a bilateral intercostal incisionin the fourth spaces joined by a V osteotomy ofthe sternum. This V-shaped osteotomy of thesternum, described by Brock, aids in accurate andeasy closure.
Second, the approach to the valve often has tobe made through the atrial wall rather than viathe appendage. As in the left side of the heartwhen this is so, I have found that two purse-string sutures inserted to enclose an oblique fieldgive the most satisfactory access available. The
FIG. Sb.-Method ofinsertion of twot o u r n i q u e tsutures.
\I/\.
\'II
aFIG. 5a.-Shows all valves on one plane and
illustrates the analogy of the aortic mitralcusp to the infundibular and septal tri-cuspid cusps and points the suggested lineof valvotomy.
b
Rumel tourniquets should lie towards the radialborder of the finger which is used.The last point is that the infundibular and
septal cusps together correspond in function tothe aortic cusp of the mitral valve, as they areadjacent to the outflow tract of the ventricle.Therefore, the split is better made between thesetwo cusps on the one side and the marginal cuspon the other side. The primary site of regurgita-tion is at the junction of the cusps, and this maywell be increased by an additional split betweenthe infundibular and septal cusps. It follows thatthe safest place to start the split between the cuspsis not where the three meet but between the septaland marginal cusps which are found to lie directlyunder the finger.
CONCLUSIONThe diagnosis of tricuspid stenosis can now be
made with accuracy, and surgical interventiongives encouraging results.
We acknowledge with gratitude the help of theRegional Cardiological Centre under Dr. J. W. Brown,the Professorial Medical Unit under Professor Stuart-Harris, Dr. E. K. Abbott, radiologist, and Dr. J.Johnston, anaesthetist.
REFERENCESAltschule, M. D., and Blumgart, H. L. (1937). Amer. Heart J., 13,
589.- and Budnitz, E. (1940). Arch. Path., Chicago, 30, 7.Chesterman, J. T., and Whitaker, W. (1954). Amer. Heart J., 48
631.Cooke, W. T., and White, P. D. (1941). Brit. Heart J., 3, 147.Kossmann, C. E. (1955). Circulation, N.Y., 11, 378.Neptune, W. B., and Bailey, C. P. (1954). J. thorac. Surg., 28, 15.Rolleston, H. (1941). Brit. Heart J., 3, 1.Smith, J. A., and Levine, S. A. (1942). Amer. Heart J., 23, 739.Thompson. W. P., and Levine, S. A. (1937). Amer. J. med. lSci.,
193, 4.Whitaker, W. (1954). Quart. J. Med., 23, 105.- (1955). Amer. Heart J., 50, 237.Wood, P. (1950). Diseases of the Heart and Circulation. Eyre and
Spottiswoode, London.(1954). Brit. med. J., 1, 1051 and 1113.
326
on June 3, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.10.4.321 on 1 Decem
ber 1955. Dow
nloaded from