Embed Size (px)
Citation preview

Surgical Options for Venous Disease
Sandra C Carr MD Vascular Surgery
Meriter Wisconsin Heart

Chronic Venous Disease • Approximately 23% of adults in the US have varicose veins • Estimated 22 million women and 11 million men ages 40-80
years have varicose veins • Up to 0.5% of the population has had problems with venous
ulcers over the lower extremities

Socioeconomic Impact • Medical costs in the US approx. $1 billion annually,
mostly due to advanced cases with ulceration • Venous ulcers cause loss of 2 million work days per year
in the US • Multiple studies have shown decreased scores on health
related as well as venous disease related quality of life surveys

Clinical Classification
• C1 – spider veins or telangectasias • C2 – varicose veins • C3 – edema • C4 – skin changes (eczema, pigmentation) • C5 – healed ulcer • C6 – active ulcer

Telangectasias C1

Varicose Veins C2

Edema with Dermatitis

Venous Stasis Dermatitis

Hyperpigmentation

Lipodermatosclerosis

Atrophie Blanche

Healed Venous Ulcer

Venous Stasis Ulcer

Goals of Surgical Treatment • Attempt to address the underlying cause
of the ulcer • Speed ulcer healing rate • Prevent ulcer recurrence • Improve patient quality of life

Treat the Underlying Cause • Increased ambulatory venous pressures • Severity is related to magnitude of venous
hypertension • Reflux is the most important hemodynamic
feature

Pathophysiology
• Primary varicose veins – result from venous dilation and valve damage without previous DVT
• Secondary varicose veins – recanalization of thrombosed veins leads to reflux and residual obstruction

Normal Venous Valves

Venous Reflux

Postphlebitic Syndrome
• Chronic leg symptoms following old DVT • May be due to old occlusive disease • Valve damage and scarring leads to reflux

Venous Anatomy There are two venous systems in the lower
extremity • Deep venous system - veins that lie within the
muscular systems • Superficial veins – veins that lie outside the
muscular system.
These two systems are interconnected by many perforating veins

Venous Anatomy

Perforating Veins • Connectors between the
superficial and deep system.
• There are over 100 communicating veins in the leg.
• One way valves direct blood flow from the superficial system to the deep system.


Diagnostic Studies
• Physical Exam • Duplex Ultrasound • CT Venography • MR Venography • Venogram with IVUS

Duplex Ultrasound
• Unilateral / limited • Evaluate deep system
for reflux or obstruction • Locate sites of valvular
incompetence – GSV, SSV, perforators
• Develop a logical treatment plan

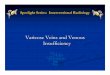
Venous Duplex Ultrasound
img 5
Image courtesy of Olivier Pichot, MD

Duplex for Venous Reflux
Normal GSV Reflux in the GSV

With extension into IVC
Large left iliofemoral thrombus Compression of left iliac vein by right iliac aretery
RCIA
LCIV
May Thurner Syndrome
CT Venogram

Venography with IVUS

Compression Therapy for Venous Ulcers

Compression Stockings
• Control edema • Decrease aching
and leg pain • Prevent recurrent
ulceration

Compression Stockings

Surgical Treatment
• Truncal superficial veins: GSV, SSV • Tributary veins • Perforating veins • Deep veins
–Deep vein occlusive disease –Deep vein reflux
It is not necessary to wait until the ulcer is healed to intervene

Treatment of GSV/SSV Reflux
• Saphenous stripping • Radiofrequency ablation • Endovenous laser ablation • Foam sclerotherapy

Open Surgical Techniques Ligation of the Saphenofemoral Junction
Stripping of the GSV

Radiofrequency Ablation

Radiofrequency Ablation – Venefit RFA Generator ClosureFast Catheter

Endovenous Laser Ablation (EVLT)

Endovenous Laser Ablation (EVLT)
• Diomed 810 nm • Dornier 940 nm • CoolTouch 1320 nm • Angiodynamics 1470 nm

VenaCure

Endovenous Ablation

Endovenous Ablation

Treatment of Tributary Varicosities
• Sclerotherapy • Phlebectomy

Sclerotherapy • Injection into the vein • Damages the endothelium • Most effective for spider veins, reticular
veins, and small varicosities • Larger veins more prone to phlebitis

Sclerotherapy Agents
• Hypertonic saline • Sodium tetradecyl sulfate • Sodium morrhuate • Polidocanol

Foam Sclerotherapy • Uses detergent sclerosing agent • Completely displaces blood from the vein • Allows better contact with the vein wall • Easily seen with ultrasound

Ultrasound Guided Sclerotherapy
• Method to increase the efficacy of sclerotherapy
• Provides precise visualization of the needle tip
• Used to treat saphenous veins or perforators

Duplex Guided Sclerotherapy

Ambulatory Phlebectomy

Perforating Veins

Venous Hypertension due to Incompetent Perforating Vein

Incompetent Perforating Veins

GSV plus Perforator Reflux

Subfascial Endoscopic Perforator Surgery
Perforating veins are clipped or divided with the harmonic scalpel

Foam Sclerotherapy of Perforating Veins

Endovascular Closure of Perforating Vein

Treatment of Deep Vein Disease
• Occlusive disease – postphlebitic syndrome
• Deep vein reflux – valve failure

Iliac Vein Occlusion
• Can present acutely with DVT
• May have underlying compression of the left common iliac vein (May-Thurner Syndrome)
• Some present with chronic swelling of the left lower extremity

Acute Iliac DVT
• Only 20% recannalize with anticoagulation alone
• 90% have chronic venous hypertension
• 40% develop venous claudication
• Up to 15% develop ulcers over 5 years

Mechanical Thrombolysis

Thrombolysis for Acute Iliofemoral DVT
Wire crossing CIV occlusion After tPA, compression seen

CIV after PTA / Stenting

Chronic iliac vein occlusion
• Venous claudication – bursting thigh and leg pain worse with exercise
• Swelling of the thigh and lower leg • Suprapubic collaterals

Endovascular Treatment for Chronic Occlusive Disease

Venous Bypass – Palma Procedure

Valvuloplasty

Valve Transplantation

Conclusions
• Surgical treatment for venous disease helps to address the underlying mechanism of the venous stasis ulcer
• Intervention may help speed ulcer healing and decrease recurrence rates
• Large prospective randomized studies showing clear benefit are lacking