Embed Size (px)
Citation preview
Surgical Grand Rounds
Cytoreductive Surgery andIntraperitoneal Chemotherapy
Phillip D. Smith, MD4.28.8
HistoryHistory
Cytoreductive surgery alone does not increase survival Adjuvant therapy needed to
decrease microscopic tumor burden peri-operatively Paul Sugarbaker, MD at
Washington Cancer Center 25 years ago

TheoryTheory
Peritoneal seeding occurs via lymphatics and intra-operatively during resectionBlood clots containing viable cancer cells Spread during blunt dissection Fibrin entrapment of cancer cells on
traumatized peritoneal surfacesTumor progression due to biochemical
environment of wound healing
TheoryTheory
Theory Large molecular weight molecules are
sequestered at the site when instilled into the peritoneal cavity Chemotherapeutics will be
bioavailable for both surgically seeded tumor deposits and raw surfaces of incomplete surgical resection
Cytoreductive Surgery for Peritoneal CarcinomatosisCytoreductive Surgery for
Peritoneal Carcinomatosis Excision of all macroscopic tumor
within the abdomen Peritonectomy Often includes splenectomy,
cholecystectomy, partial/total gastrectomy, greater omentectomy, hysterectomy, multiple small bowel resections, and sigmoid colectomy Alimentary tract reconstruction
CytoreductionCytoreduction
Chemotherapy is infused after cytoreduction and before alimentary tract reconstruction Prevents tumor cells from being
trapped in suture lines and decreases local recurrence
Hyperthermic Intraperitoneal Chemotherapy
Hyperthermic Intraperitoneal Chemotherapy
With excision of macroscopic tumor, microscopic remnants can be treated
Up to 20 times the bioavailability of systemic chemotherapy
Hyperthermia Cytotoxic Increases tissue penetration of chemotherapy Synergistic effect on cytotoxicity of
chemotherapy
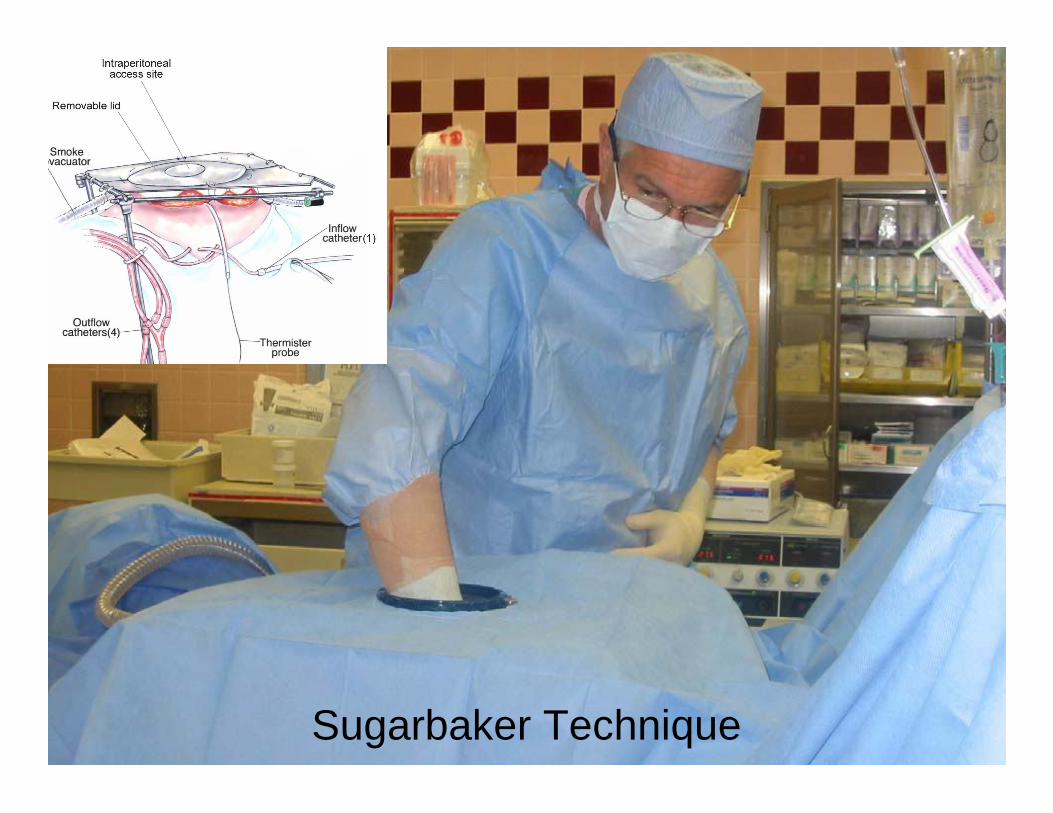
Sugarbaker Technique

Pearlman Technique
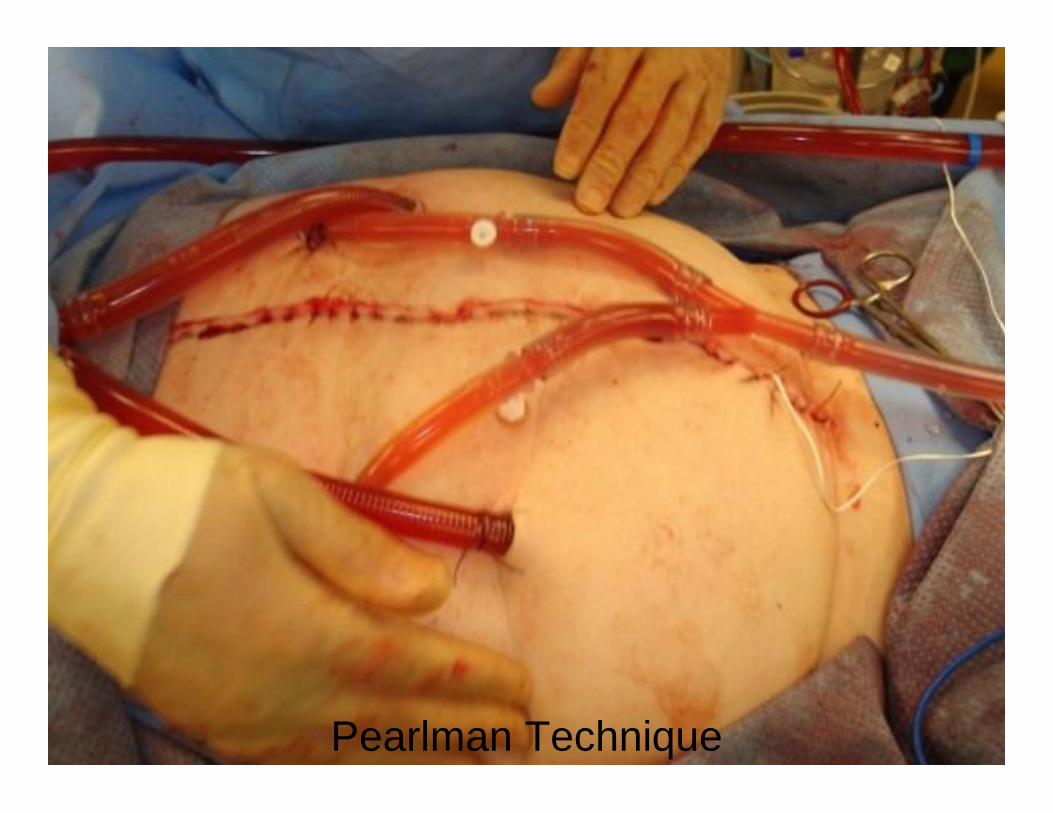
Pearlman Technique
The EvidenceThe Evidence
Verwaal, et. al. J Clinical Onc. 2003 Phase III RCT of 109 patients HIPEC vs standard chemo for carcinomatosis
secondary to colorectal cancer
HIPEC using Sugarbaker technique and mitomycin C Began standard chemotherapy at 6-12 weeks post-
op
Standard therapy was Fluorouracil and leucovorin
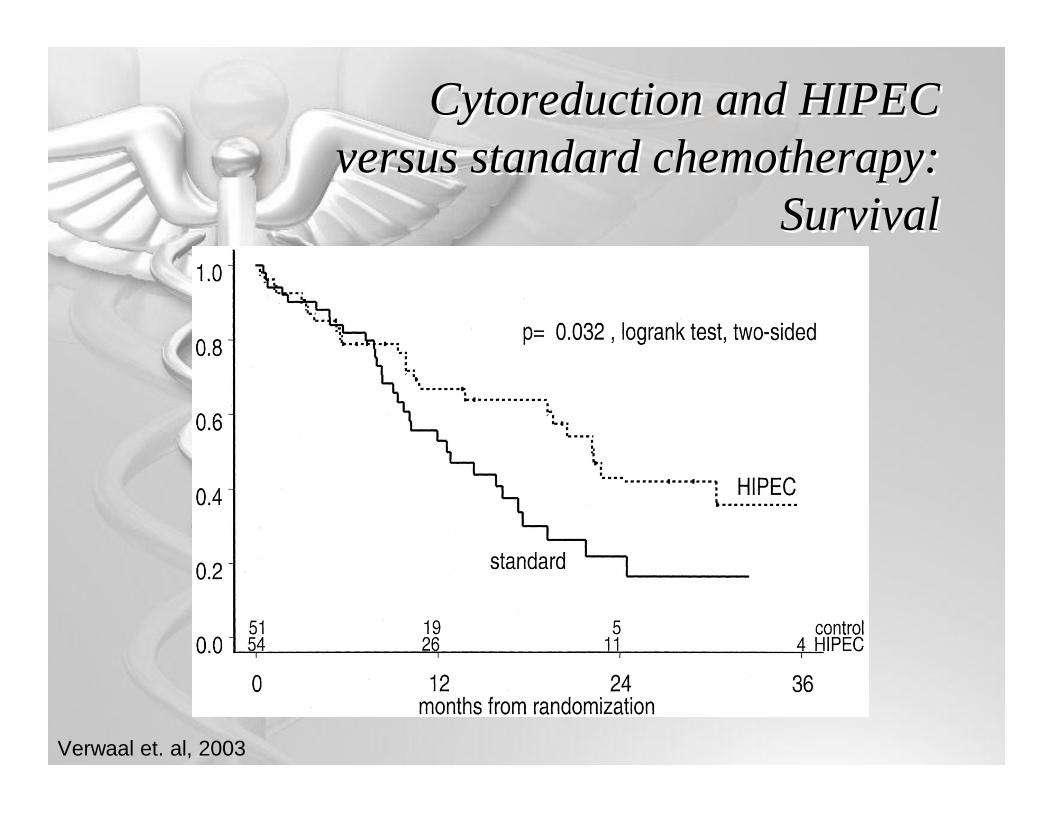
Cytoreduction and HIPEC versus standard chemotherapy:
Survival
Cytoreduction and HIPEC versus standard chemotherapy:
Survival
Verwaal et. al, 2003
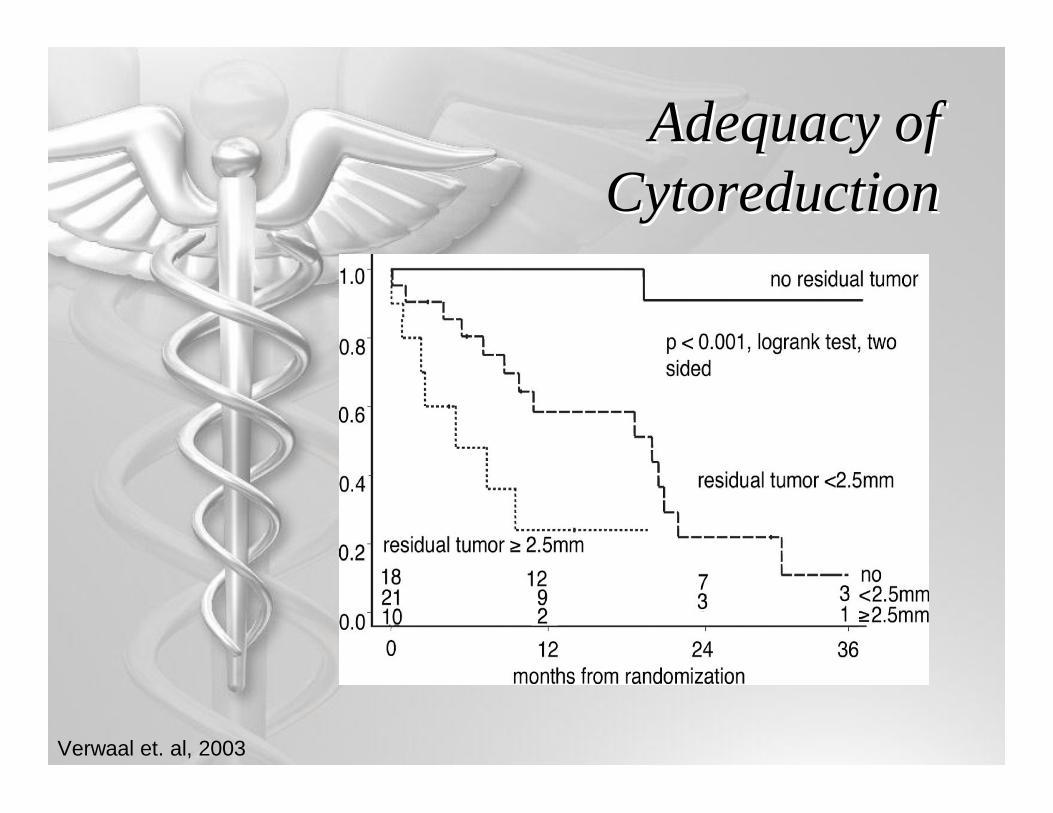
Adequacy of Cytoreduction
Adequacy of Cytoreduction
Verwaal et. al, 2003
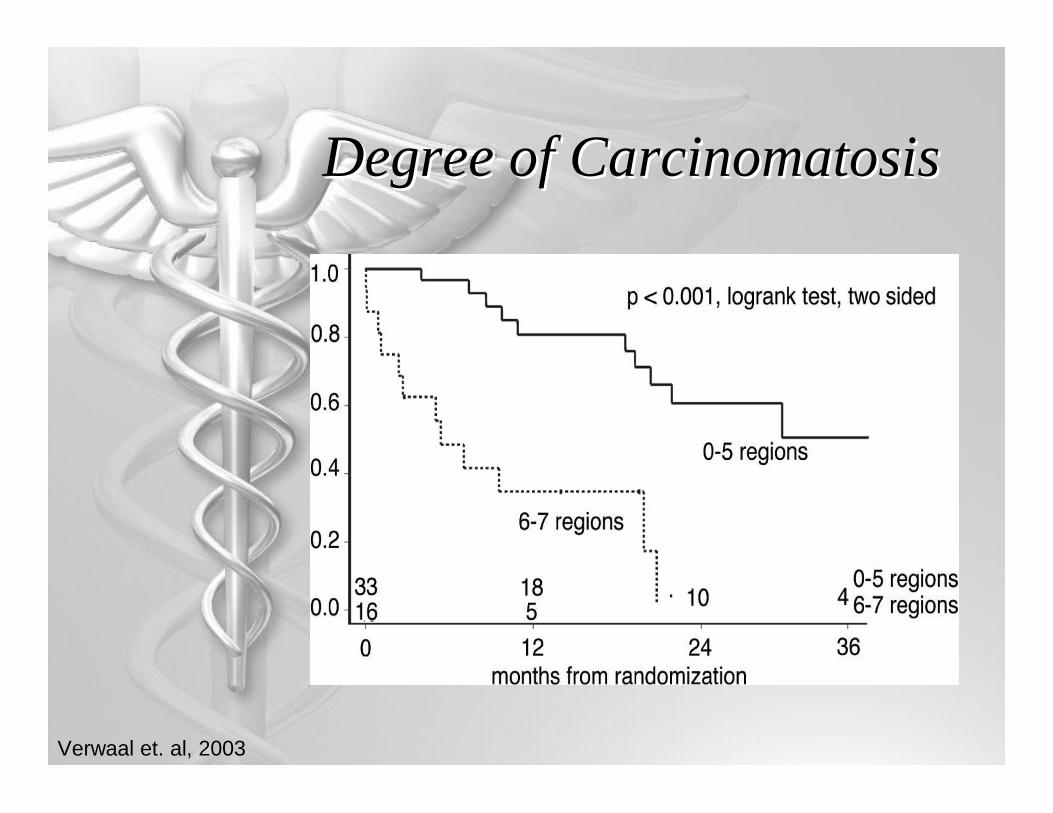
Degree of CarcinomatosisDegree of Carcinomatosis
Verwaal et. al, 2003
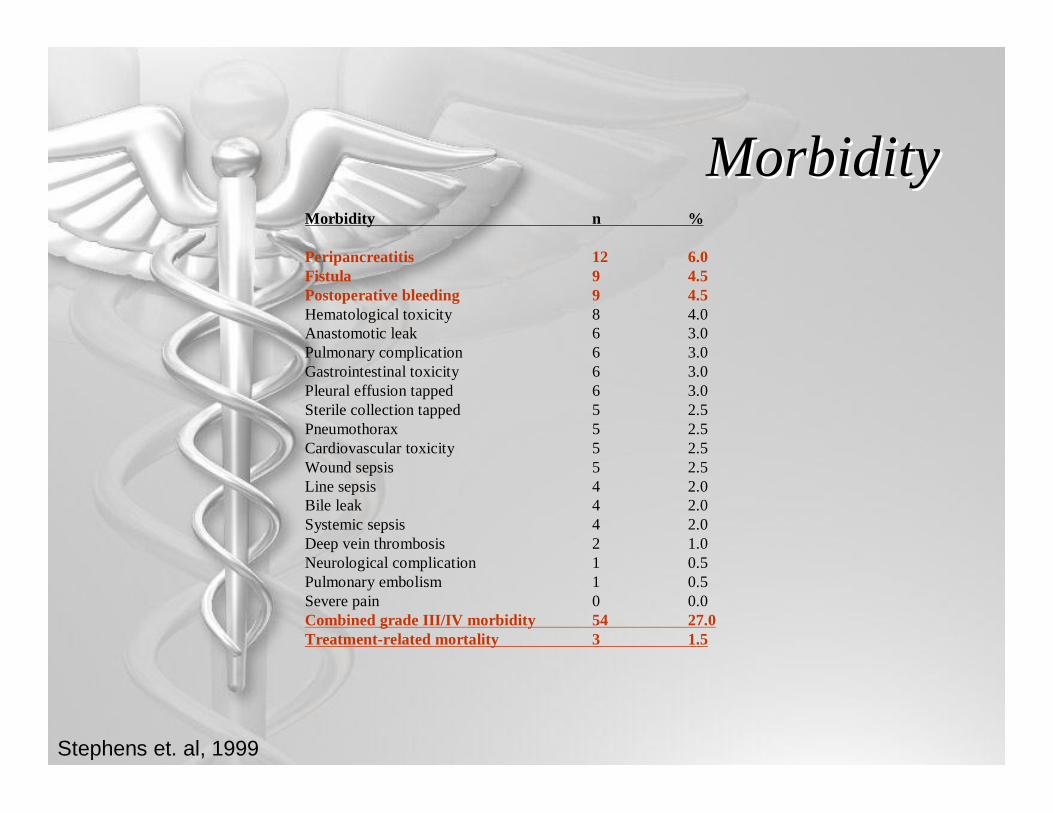
MorbidityMorbidity
Stephens et. al, 1999
Morbidity n %
Peripancreatitis 12 6.0Fistula 9 4.5Postoperative bleeding 9 4.5Hematological toxicity 8 4.0Anastomotic leak 6 3.0Pulmonary complication 6 3.0Gastrointestinal toxicity 6 3.0Pleural effusion tapped 6 3.0Sterile collection tapped 5 2.5Pneumothorax 5 2.5Cardiovascular toxicity 5 2.5Wound sepsis 5 2.5Line sepsis 4 2.0Bile leak 4 2.0Systemic sepsis 4 2.0Deep vein thrombosis 2 1.0Neurological complication 1 0.5Pulmonary embolism 1 0.5Severe pain 0 0.0Combined grade III/IV morbidity 54 27.0Treatment-related mortality 3 1.5

MorbidityMorbidity
Statistically significant variables affecting morbidity
0.066Dose of Mitomycin
0.0083Intraoperative Blood Loss
0.0078Number of Suture lines
>0.0001# of peritonectomy procedures and resections
>0.0001Duration of Operation
P
Stephens et. al, 1999
ConclusionsConclusions
Definite survival benefit Median survival
22.4 months with HIPEC 12.6 months with standard chemo
Degree of carcinomatosis predicts survival
Historical median survival with systemic FU and leucovorin Median survival ~ 5 months

Follow UpFollow Up
Verwaal, et. al. Ann Surg Onc. 2005. Included previous study participants
plus additional participants If complete macroscopic
cytoreduction successfulMedian Survival- 42.9 months 5-year survival rate- 43%
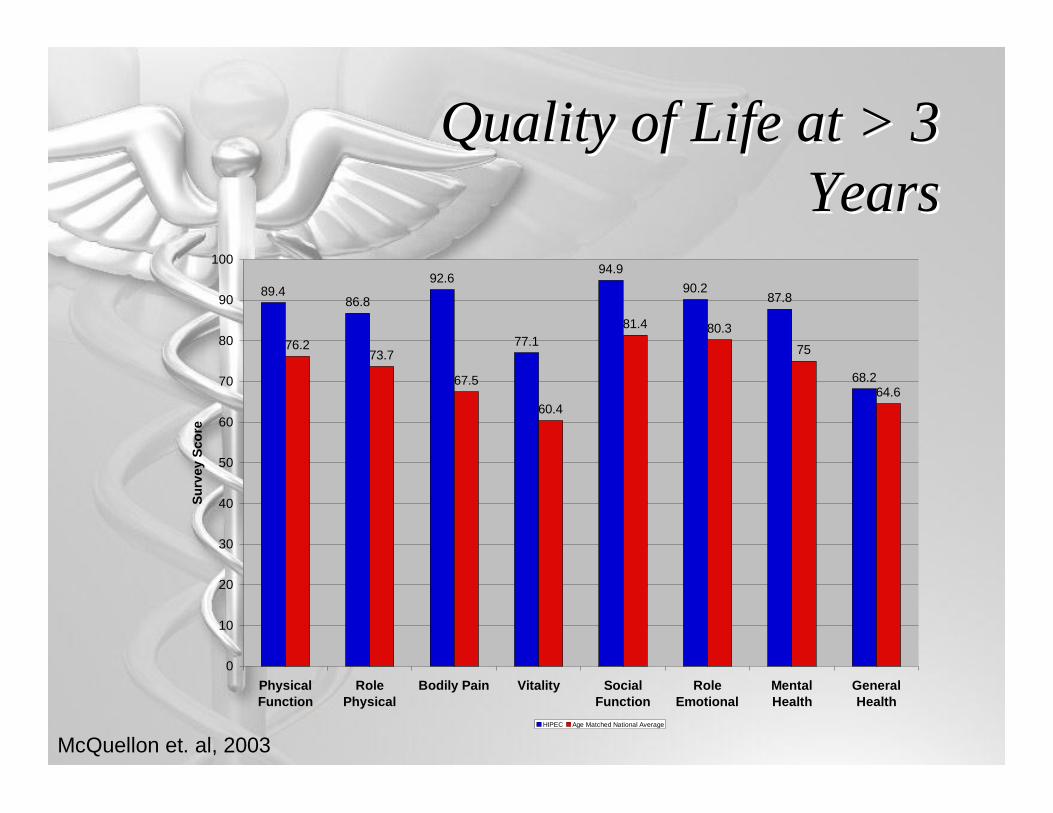
Quality of Life at > 3 Years
Quality of Life at > 3 Years
89.486.8
92.6
77.1
94.990.2
87.8
68.2
76.273.7
67.5
60.4
81.4 80.3
75
64.6
0
10
20
30
40
50
60
70
80
90
100
PhysicalFunction
RolePhysical
Bodily Pain Vitality SocialFunction
RoleEmotional
MentalHealth
GeneralHealth
Surv
ey S
core
HIPEC Age Matched National Average
McQuellon et. al, 2003

Application to Other Cancers
Application to Other Cancers
Diffuse Malignant Peritoneal Mesothelioma Yan, et. al, 2006 Median Survival 59 months, 5-year survival
49% Appendiceal Mucinous Tumors Yan, et. al, 2007
Repeated cytoreductions with HIPEC improve survival
5- and 10- year disease free survival, 70% and 67%
Gastric Cancer, Pseudomyxoma Peritonei, Ovarian Cancer, etc.
Shortcomings…Shortcomings…
Limited data No standard procedure No standard chemotherapy Morbidity Selection of patients Severe carcinomatosis may make
complete cytoreduction impossible
Standardized TherapyStandardized Therapy
Esquivel, et. al. Annals Surg Onc. 2007 Consensus Statement
Pearlman (Closed) or Sugarbaker (Open) technique -> Surgeon’s choice
5 days of immediate post op intraperitoneal chemotherapy with 5-FU -> Surgeon’s choice
HIPEC only for patients in which complete cytoreduction is deemed possible Can perform palliative HIPEC if malignant ascites
Perform HIPEC with mitomycin C, oxaliplatin promising

Selection CriteriaSelection Criteria
FutureFuture
Proven benefit in colorectal carcinomatosis
Need Phase III studies to extend to other cancers
Bottom LineBottom Line
Cytoreduction with HIPEC improves survival
Therapy associated deaths do not exceed deaths of those receiving standard chemo
QOL not diminished by therapy
Cytoreductive Surgery with HIPEC Works
ReferencesReferences Cameron, JL. Current Surgical Therapy. 9th ed. 2008. Verwaal, VJ, et. al, Randomized Trial of Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy
versus Systemic Chemotherapy and Palliative Surgery in Patients with Peritoneal Carcinomatosis ofColorectal Cancer. J Clinical Onc. 2003; 21(20): 3737-3743.
Yan, TD, et. al, A Systemic Review and Meta-analysis of the Randomized Controlled Trials on Adjuvant Intra-peritoneal Chemotherapy for Resectable Gastric Cancer. Annals Surg Onc. 2007; 14(10): 2703-2713.
Smeenk, RM, et. al, Survival Analysis of Pseudomyxoma Perotinei Patients Treated by Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. Annals Surg. 2007; 245(1): 104-109.
Yan, TD, et. al, Critical Analysis of Treatment Failure After Complete Cytoreductive Surgery and Perioperative Intraperitoneal Chemotherapy for Peritoneal Dissemination from Appendiceal Mucinous Neoplasms. Annals Surg Onc. 2007; 14(8): 2289-2299.
Yan, TD, et. al, Morbidity and Mortality Assessment of Cytoreductive Surgery and Perioperative Intraperitoneal Chemotherapy for Diffuse Malignant Peritoneal Mesothelioma. Annals Surg Onc. 2007; 14(2): 515-525.
Esquivel, J, et. al. Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy in the Management of Peritoneal Surface Malignancies of Colonic Origin. Annals Surg Onc. 2007; 14(1): 138-133.
Verwaal, VJ, et. al. Long-Term Survival of Peritoneal Carcinomatosis of Colorectal Origin. Annals Surg Onc. 2005; 12(1): 65-71.
Al-Shammaa, HAH, et. al. Current status and future strategies of cytoreductive surgery plus interperitoneal hyperthermic chemotherapy for peritoneal carcinomatosis. World J Gastroenterol. 2008; 14(8): 1159-1166.
Stephens, AD, et. al. Morbidity and Mortality Analysis of 200 Treatments with Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy using the Coliseum Technique. Annals Surg Onc. 1999; 6(8): 790-796.
Sugarbaker, P. www.surgicaloncology.com