Embed Size (px)
Citation preview

Surgery Journal Club
By : Ahmad Zahmatkesh
Mohammadreza Nazemian

As the number of women who are long term survivors of breast cancer increases , chronic toxicities such as breast cancer related lymphedema ( BCRL ) gain importance
Purpose of this Review : Summarize the latest studies addressing BCRL in order to provide patients and health care providers with optimal recommendations

Well documented in older randomized breast cancer treatment trials exemplified by NSABP B-04 Trial :
Rate of BCRL ( Measured using arm
circumference )
Type of Procedure
58.1% Radical Mastectomy
38.2% Total Mastectomy With Axillary Radiation
49.1% Total Mastectomy Arms
* NSABP : National Surgical Adjuvant Breast & Bowel Project

Recent data has emerged that rates of BCRL are predicated on the aggressiveness of treatment : Breast surgical procedure performed Method of axillary surgery ( Sentinel LN
Vs. Axillary LN Dissection ) Use and extent of adjuvant radiation
therapy Use of adjuvant chemotherapy

In a Series of over 3000 patients which evaluated for incidence of BCRL after breast conservation (BC) via survey were :
Rates of BCRL( without/with ) chemotherapy
Type of Treatment
13% / 23% BC + SLND
51% / 61% BC + ALND
53% / 65% BC + Regional Irradiation

NSABP B-32 Trial demonstrated that rates of BCRL significantly reduced with the use of SLND over ALND , 8% vs. 14%
Coen et al. examined 727 patients who were treated with BCS and WBI with or without regional irradiation and found that rates of BCRL were 2% for tangents alone vs. 9% with regional irradiation
Norman et al. found that patients receiving chemotherapy had an increased risk of developing BCRL with a HR of 1.46
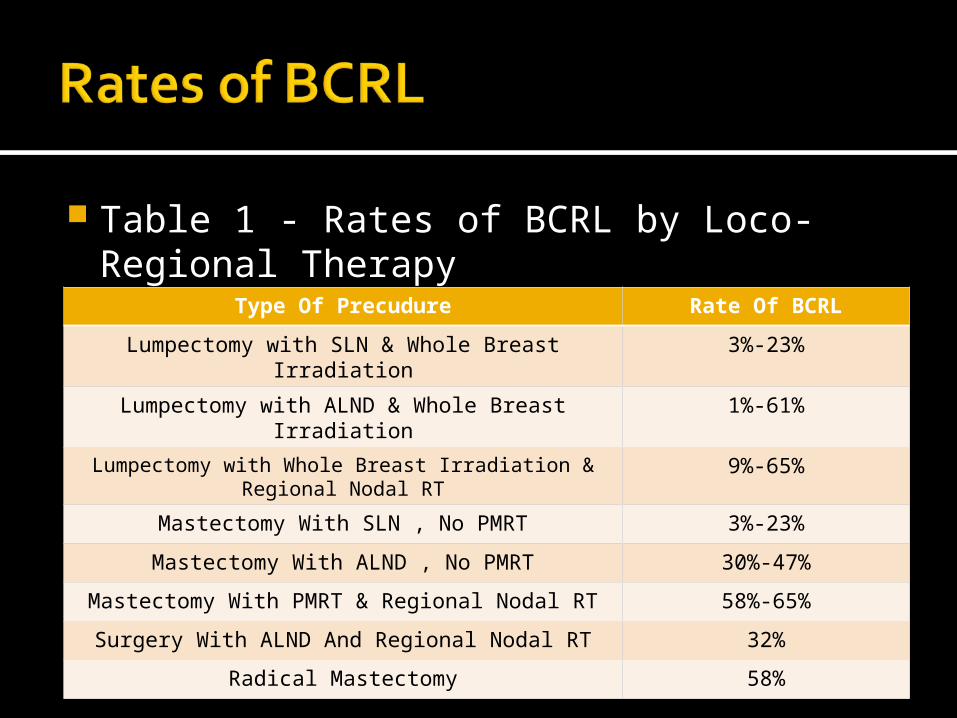
Table 1 - Rates of BCRL by Loco-Regional Therapy
Type Of Precudure Rate Of BCRL
Lumpectomy with SLN & Whole Breast Irradiation 3%-23%
Lumpectomy with ALND & Whole Breast Irradiation
1%-61%
Lumpectomy with Whole Breast Irradiation & Regional Nodal RT
9%-65%
Mastectomy With SLN , No PMRT 3%-23%
Mastectomy With ALND , No PMRT 30%-47%
Mastectomy With PMRT & Regional Nodal RT 58%-65%
Surgery With ALND And Regional Nodal RT 32%
Radical Mastectomy 58%

With Traditional studies the diagnosis of BCRL in the subclinical phase of disease remain limited and often diagnosed after development of significant BCRL
Improvements in BCRL diagnostic modalities decreased the number of women suffering with the long term complications

Traditional Studies : Arm circumference measurement : ▪ Simple ▪ Lack of standardized measuring points and definition of
BCRL , Intra and Inter-Observer variability
Water displacement :▪ Lacks Sensitivity
Self-assessment

New detection techniques : Bioimpedance Spectroscopy ( BIS )▪ Standardized cut-off point ▪ Increased sensitivity and detect BCRL 4
months earlier >> Potential for subclinical detection
Optoelectric Perometry ▪ Increased Sensitivity and Decreased
variability
BCRL management involves : Severity of volume accumulation Severity of Symptoms Acute vs. Chronic nature of disease

Treatments include : Compression therapy : ▪ The efficacy remains controversial▪ Techniques and Devices :▪ Compression bandages or garments▪ Gradient compression devices▪ Pneumatic compression devices
Multi-modality ( ie., Complex Decongestive physiotherapy )
Pharmacotherapy : ▪ Benzopyrones : ▪ Decrease fluid volume , Improvement of Subjective Pain , Tightness and Acute
inflammation
▪ Diuretics▪ Selenium

Complex Decongestive physiotherapy Utilized for more advanced BCRL Includes : Compression , MLD , Basic Skin care and Exercise Administered by well-trained therapists
Phase I : Outpatient / Multi-week program of MLD , Short-stretch compression bandaging , Exercise and Proper skin-nail care and preparing patient for phase II
Phase II : At Home / Entails Skin care , Exercise , Self-massage and Use of compression
The Efficacy of CDP has been verified in multiple studies and improved patient’s quality of life as well as decreasing excess arum volume accumulation

By Eliminating ALND and not adding regional irradiation , the rates of BCRL may be significantly reduced
By Limiting the number of patients receiving regional irradiation further reduction of BCRL would be seen
By Using new techniques that examine genetic markers in tumors and provide recurrence risk scores , the number of patients requiring chemotherapy will likely decrease so developing of BCRL will reduce
Early Diagnosis at the subclinical stages represent a novel and recently tested method to reduce the risk of BCRL

BCRL is more prevalent than generally appreciated even after less morbid axillary procedures ( including SLND ) are utilized
BCRL can be detected earlier when newer diagnostic interventions are applied to prevent the chronic phase of the disease as well as sequelae including infection , ulceration and disfigurement

Simple and reproducible assessment aids currently exist and should be used both prior and after local therapies in virtually all “at risk “ patients
Data regarding optimal treatment strategies is limited and controversies do exist but based on the currently available CDP represents a therapeutic modality with significant supporting evidence in patients with clinically detectable BCRL

Utilization of new diagnostic modalities may facilitate earlier clinician detection and management of BCRL and have the potential to significantly reduce costs associated with the management of BCRL

Thanks For Your Attention