Embed Size (px)
Citation preview

Surfaced-Enhanced Laser Desorption/Ionization Time-of-Flight(SELDI-TOF) Differentiation of Serum Protein Profiles of
BRCA-1 and Sporadic Breast Cancer
Stephen Becker, MD, Lisa H. Cazares, Patrice Watson, PhD, Henry Lynch, MD,O. John Semmes, PhD, Richard R. Drake, PhD, and Christine Laronga, MD
Background: BRCA-1 mutations predispose women to early onset breast cancer, but �20%never develop cancer. Surface-enhanced laser desorption/ionization time-of-flight mass spectrom-etry (SELDI-TOF MS) profiling can differentiate protein signatures of cancer and normal subjects.Our objective was to distinguish women with BRCA-1 mutations who developed breast cancer(BRCA-1 Ca) from those who did not (Carrier), normal volunteers (NL), and women with sporadicbreast cancer (SBC), using SELDI-TOF.
Methods: Baseline serum specimens were obtained from women with BRCA-1 mutationswithout cancer, SBC, and NL. BRCA-1 women were later divided into two cohorts, pending cancerdevelopment. The sera were spotted onto protein chips for SELDI-TOF analysis and analyzed withclassification algorithm software.
Results: BRCA-1 Ca patients (n � 15) developed cancer within 3 years of baseline, whileBRCA-1 carriers (n � 15) were cancer-free in 7 years of follow-up. SELDI-TOF analysis revealeddifferentially expressed proteins (P � .05) between BRCA-1 Ca, Carrier, and SBC patients (n �16), such that 13/15 BRCA-1 Ca vs. Carrier women were correctly identified (sensitivity/specificityof 87%/87%) and 14/15 BRCA-1 Ca vs. SBC patients were correctly identified (sensitivity/specificity 94%/100%). Profiles of Carriers resembled NL profiles (n � 16).
Conclusions: SELDI-TOF protein profiles from this small pilot study distinguished betweenwomen with BRCA-1 Ca, Carriers, and women with SBC. Whether BRCA-1 Ca represents earlierdetection of occult cancer or other risk factors is unknown. Follow-up studies with larger numbersand longer follow-up are required to validate these findings but may allow more timely prophylacticor therapeutic strategies.
Key Words: BRCA-1—Breast cancer—Protein profiling—Serum.
Breast cancer is the most common malignancy thataffects women in the United States today. In fact, one innine women can expect to develop the disease withintheir lifetime. Although most causes of breast cancer are
sporadic, approximately 7% to 10% of them are attrib-uted to hereditary syndromes, with BRCA-1 mutationsaccounting for most.1 The BRCA-1 gene itself was onlyrecently discovered by Hall2 and is the focus of ongoingresearch to define its functional tumor suppressor role inthe DNA damage response pathways. However, twoclinical manifestations for carriers of this gene mutationare quite clear: early onset breast cancer and lack of100% penetrance of disease occurrence. Thus, forBRCA-1 mutation carriers, the challenge is to identifywhich women will develop breast cancer and to do so atan age at which our “gold standard” for cancer detection,mammography, is found to be least accurate. Conversely,the need exists to identify BRCA-1 mutation carriers atlow risk for cancer.
Received March 19, 2004; accepted July 5, 2004.From the Department of Surgery (SB, CL) and Departments of
Microbiology and Molecular Cell Biology (LHC, OJS, RRD), EasternVirginia Medical School, and Virginia Prostate Center (LHC, OJS,RRD), Norfolk, Virginia; and the Department of Preventative Medicine(PW, HL), Creighton University, Omaha, Nebraska.
Address correspondence and reprint requests to: Christine Laronga,MD, Department of Surgery, Eastern Virginia Medical School, 825Fairfax Avenue, Suite 610, Norfolk, Virginia 23507; Fax: 757-446-8951; e-mail: [email protected].
Published by Lippincott Williams & Wilkins © 2004 The Society of SurgicalOncology, Inc.
Annals of Surgical Oncology, 11(10):907–914
DOI: 10.1245/ASO.2004.03.557
907

Proteomic profiling of clinical body fluids to differen-tiate protein expression patterns characteristic of a can-cerous or noncancerous state is an evolving field of studythat may offer a solution. These differentially expressedproteins could be from the cancer itself, i.e., CA 27.29,CEA, or Her2/neu, or from the host response. With useof surface-enhanced laser desorption/ionization time-of-flight mass spectrometry (SELDI-TOF MS), protein pro-files have been generated that can accurately discrimi-nate between cancerous and noncancerous samples formany cancer types.3–7 To date, however, there have beenlimited studies of its utility in breast cancer, with the firstreport originating from Li et al.,8 who utilized SELDI-TOF to discriminate breast cancer from benign breastdisease with a sensitivity and specificity of 93% and91%, respectively. In a similarly small cohort, Vlahou etal.9 demonstrated the power of SELDI-TOF MS to dis-criminate breast cancer patients from normal healthyvolunteers. These studies illustrated the potential ofproteomic profiling to discriminate between cancerousand noncancerous states with reasonable sensitivity andspecificity.
Given the fact that up to 20% of women with BRCA-1mutations will not develop breast cancer10 and the recentsuccess of SELDI-TOF MS differentiation in breast can-cer, we hypothesized that a proteomic profile could begenerated that would allow for accurate discriminationbetween BRCA-1 mutation carriers at high risk for breastcancer and carriers at lower risk, as well as differentiateBRCA-1 breast cancers from sporadic breast cancers andnormal healthy volunteers.
METHODS
SpecimensFollowing institutional review board (IRB) approval,
age-matched baseline serum specimens were identifiedfrom a collection of sera obtained during genetic testingat the Hereditary Cancer Institute at Creighton Univer-sity from 1987 to 2001. All samples were retrospectivelylabeled from women found to have germ-line BRCA-1mutations who were without evidence of breast cancer atthe time of the baseline sample. The BRCA-1 womenwere followed until the development of breast cancer orfor at least 7 cancer-free years and subsequently dividedinto two cohorts according to the presence or absence ofbreast cancer development (BRCA-1 Cancer and Carriercohorts).
At Eastern Virginia Medical School, women requiringan operative biopsy for an abnormal mammogram orclinical breast examination and normal healthy volun-teers were eligible to participate in a study for breast
cancer protein profiling. They were enrolled through theDivision of Surgical Oncology after signing an IRB-approved consent form. For those women having a di-agnostic biopsy, the blood sample was retrospectivelylabeled as “benign” or “cancer” once the pathologicevaluation was complete. Serum samples were randomlycollected from healthy females during the same timeperiod in which the sporadic breast cancer specimenswere obtained. All samples were collected by venipunc-ture into a 10-cc SST Vacutainer tube (Becton Dickin-son) and allowed to clot at 4°C for 30 minutes. Coagu-lated blood was spun at 3000 rpm for 10 minutes, and theserum portion was immediately aliquoted and frozen forstorage at �80°C.
SELDI Processing Of Serum SamplesSerum samples were processed robotically on a Bi-
omek 2000 liquid handling system in a 96-well formatfor SELDI analysis (Biomek 2000; Beckman Coulter,Fullerton, CA) in the following manner. In brief, 20 �Lof serum was pretreated with 8 M urea and 1% CHAPSand was vortexed for 10 minutes at 4°C. A furtherdilution was made in 1 M urea, 0.125% CHAPS, andPBS. Each sample position was randomized and spottedin duplicate onto copper-coated immobilized metal af-finity (IMAC-Cu). ProteinChips were used for SELDI-TOF analysis with the aid of a bioprocessor. The proteinchips were then incubated at room temperature for 30minutes, followed by washes of PBS and water. TheIMAC-Cu chip arrays were allowed to air dry, and asaturated solution of sinapinic acid in 50% (v/v) aceto-nitrile and 0.5% (v/v) trifluoroacetic acid was added toeach spot. The protein chip arrays were analyzed with theSELDI ProteinChip System (PBS-II, Ciphergen Biosys-tems, Fremont, CA). The spectra were generated by theaccumulation of 192 shots at laser intensity 220 in apositive mode. The protein masses were calibrated ex-ternally with use of purified peptide standards.
Afterward, each protein peak was labeled and its in-tensity was normalized for total ion current to accountfor variation in ionization efficiencies. Peak clusteringwas performed with Biomarker Wizard Software (Ci-phergen Biosystems) at settings that provide a 5% min-imum peak threshold, 0.2% mass window, and 1 to 3signal/noise determination. The peak intensities fromduplicate samples were then averaged.
SELDI Data AnalysisPattern recognition and sample classification were
performed with the Biomarker Pattern Software (Cipher-gen Biosystems), in which multiple decision trees areinitially generated with use of all the peaks as variables.
908 S. BECKER ET AL.
Ann Surg Oncol, Vol. 11, No. 10, 2004

During the analysis, a pruning step occurs in whichbranches are removed and the cost of the removal deter-mined to establish a minimal tree size. This is referred toas a learning set. Second, the decision tree was subjectedto cross-validation. In this step the data were partitionedsuch that randomly selected samples were categorizedwith the decision tree being tested, to ensure that thedecision tree was valid. The number of samples used totest the tree during cross-validation was increased from10 to 20. While choosing a smaller number of samples(e.g., 5) to test the tree can result in overfitting the data,increasing the number of samples used to test the tree isan acceptable means of ensuring the validity of thesplitters in a small sample population.
The peaks that formed the main splitters of the tree(s)with the highest prediction rates in the cross-validationanalysis were then selected and used to make a finaldecision tree with the greatest possible predictive power.
RESULTS
Thirty age-matched baseline serum specimens (� 3years; except the oldest patient with cancer, who wasage-matched within 6 years) were collected from womendetermined to have a BRCA-1 mutation during genetictesting at the Hereditary Cancer Institute at CreightonUniversity from 1987 to 2001. No demographic infor-mation, in particular any relation to Ashkenazi Jewishdescent, is available on these samples. They were sub-sequently followed with 15 women developing breastcancer within 3 years and the other 15 women remainingcancer-free for the 7 years of follow-up. The mean timeto diagnosis of breast cancer from the baseline serumsample was 1.3 years (range � 1 to 36 months). The meanage of the women who developed cancer at the time ofbaseline serum sampling was 44.2 years, and the meanage was 44.6 years among those BRCA-1 Carriers whodid not develop breast cancer (age range for cancer �29–74 years; age range for noncancer � 29–68 years).All the cancers identified were found to be an invasiveductal histology with the following breakdown of stages:stage I (n � 8), stage II (n � 3), stage I or II (n � 3), andstage III (n � 1). The three patients who were classifiedas stage I or II had incomplete staging information: onewoman had a primary tumor �2 cm but the lymph nodestatus was unknown, and two women were node-nega-tive but the primary tumor size was �5 cm.
At Eastern Virginia Medical School, 16 sera sampleswere obtained from normal healthy volunteers and 16samples were obtained from patients with sporadic breastcancer diagnosed during the same time frame, from 2001to 2003. The mean age at sample procurement for the
healthy volunteers was 45 years (range � 18 to 81years), and for the women with sporadic breast cancer itwas 52.2 years (range: 31 to 67 years). No attempt wasmade to age-match-control the samples between the twoinstitutions. In the sporadic breast cancer group, all sam-ples were from women found to have invasive ductalcarcinoma of stage I or II at diagnosis. Thirteen of the 16were sentinel lymph node–negative, while three weresentinel lymph node–positive but had a small primarylesion.
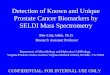
The first sera groups analyzed were from the 15BRCA-1 noncancer subjects versus the 15 individualswho developed BRCA-1 breast cancers during follow-up. Aliquots of diluted serum were applied to copper-coated affinity ProteinChips. The resulting SELDI-TOFMS data were analyzed with Biomarker Wizard andgenerated a total of 107 peaks, representing differentiallyexpressed proteins in the 1500-Da to 100,000-Da range.Of these, 23 protein peaks were significantly (P � .05)overexpressed in the BRCA-1 cancer cohort, 19 of whichwere in the 6500-Da to 9200-Da molecular weight range,as listed in Table 1. Differentially expressed lower-masspeptides (�6200 Da) tended to be present at higherlevels in the BRCA-1 noncancer samples (Table 1).Examples of the peak intensities in all samples for two ofthe most differentially expressed peaks are shown in thescatter plots in Figure 1. The protein peak at 8138-Dawas overexpressed in the BRCA-1 cancer cohort (Fig.1A), and a protein at 5909 was underexpressed relative tothe BRCA-1 noncancers (Fig. 1B).
The peak intensity values of the 107 differentiallyexpressed peaks were collectively applied to the Biomar-ker patterns algorithm program to generate a representa-tive decision classification tree. As shown in Figure 2,the resulting decision tree utilized the peak at 5909 Da asa primary splitter in the classification process. In thelearning data set, all 30 samples were correctly classifiedas either BRCA-1 with breast cancer or BCRA1 carrierwithout breast cancer, for a sensitivity and specificity of100%. Cross-validation analysis of this final decisiontree correctly identified 13 of the 15 BRCA-1 with breastcancer and 13 of the 15 BRCA-1 carriers. This resultedin a final sensitivity of 87% and a specificity of 87%(Table 2).
Next, the serum protein profiles from the BRCA-1carriers who developed cancer (n � 15) were comparedwith the serum profiles obtained from 16 women withsporadic breast cancers. With use of the copper-coatedaffinity ProteinChips, a total of 122 peaks were gener-ated with the SELDI-TOF mass spectrometer. Thirty-five of these proteins were overexpressed in the BRCA-1carrier-with-cancer group, in comparison with the spo-
909PROTEIN PROFILE OF BRCA-1 AND SPORADIC BREAST CANCER
Ann Surg Oncol, Vol. 11, No. 10, 2004

radic breast cancer cohort, all in the 6000-Da to15,000-Da mass range. Again, a protein peak of 8.1 kDawas identified that was highly overexpressed in theBRCA-1 cancer samples in comparison with the sporadicbreast cancer cohort. The decision tree generated fromthese protein peaks was able to correctly identify 14 ofthe 15 BRCA-1 breast cancer samples and all 16 spo-radic breast cancers, for a sensitivity of 94% and speci-ficity of 100% on cross-validation. For visual compari-son, the spectra ranging from 2000 to 10,000 Da fromrepresentative samples of each group are shown in Fig-ure 3.
Finally, a comparison of the normal healthy volunteersto the other three cohorts was performed, for severalreasons. A variety of factors, namely the number offreeze/thaws and sample storage, can affect the proteinprofile of a sample and thus create the illusion of differ-
ences in the spectra generated. Because the samples wereobtained from two geographically separate locations, itwas necessary to evaluate whether any apparent institu-tional differences were present. Thus, the serum from theBRCA-1 noncancer cohort was compared with serumobtained from 15 normal healthy volunteers. The proteinspectra were interchangeable to such a degree that accu-rate discrimination was not possible without overfittingthe data (Fig. 3). Additionally, the spectra appeared quitedifferent from both the BRCA-1 cancer and sporadiccancer cohorts (Fig. 3) and confirmed prior results ofdistinction of normal from sporadic breast cancer.9 Con-sistent with the previous study,9 the 15 women withBRCA-1 cancer were separated from the normal healthyvolunteers with a sensitivity and specificity of 87% and94%, respectively.
TABLE 1. SELDI protein peak intensities in serum withsignificant differences (P � 0.05) between BRCA-1 non-
cancer and BRCA-1 cancer samples
M/Z P-valueMean - BRCA1
no cancerMean - BRCA1
cancer
1588.673 0.020278 0.800588 0.6323152956.088 0.005445 0.277154 0.1184123278.707 1.05E-05 0.677433 0.1677953779.663 1.81E-05 0.192743 0.0549643959.636 0.000246 2.673944 0.9853363975.987 3.06E-05 1.226725 0.470134066.664 2.08E-06 0.180127 0.8025854285.457 8.4E-05 2.069959 0.639644306 0.034501 0.700822 0.3506744471.631 0.045945 0.161915 0.2108294493.134 0.029757 0.238686 0.147134648.0 0.004128 1.155082 0.7878255341.586 9.18E-07 1.724943 0.5289885550.199 6.28E-07 0.222015 0.0684045909.051 1.02E-07 6.204226 1.2819725974.019 4.62E-07 0.429481 0.0959756117.279 4.62E-07 0.741567 0.1625746539.982 0.007129 0.044529 0.0933136807.266 0.001905 0.020025 0.0607957057.232 0.002211 0.02504 0.0785167191.317 0.000145 0.022606 0.2414877347.652 0.008498 0.033724 0.129477480.653 0.015959 0.196596 0.4467437569.754 0.028663 0.092773 0.1424337633.829 0.000879 0.070543 0.2005227705.621 4.22E-05 0.087181 0.2561817838.505 0.007451 0.311728 0.4007877929.163 2.78E-06 0.296329 0.612957984.951 0.007786 0.381652 0.499398138.558 7.89E-07 1.187543 5.7395938344.606 4.99E-07 0.168643 0.7857768444.507 1.33E-06 0.097324 0.3992278607.898 1.93E-06 0.517182 1.3269278814.697 3.96E-07 0.078132 0.2313298938.414 0.001905 0.684039 1.0626829071.567 0.000388 0.174937 0.264987
16265.25 0.000791 0.006598 0.02488
FIG. 1. Expression level of the (A) 8138-Da and (B) 5909-Da pro-teins in all of the BRCA-1 noncancer and BRCA-1 cancer serumprofiles (—-, mean normalized intensity; O, values of individualpatients).
910 S. BECKER ET AL.
Ann Surg Oncol, Vol. 11, No. 10, 2004

DISCUSSION
Over 211,000 new cases of breast cancer are expectedin the United States this year, making breast cancer thesecond leading cause of cancer death. Genetic mutationsare known to increase a woman’s risk for cancer devel-opment by 10-fold and account for 7% to 10% of allbreast cancer cases, with the BRCA-1 gene mutationsbeing the most common (52%).1
The BRCA-1 gene was first identified by Hall in 1990and subsequently was found to be a tumor suppressor.2
This gene, located on the long arm of chromosome 17,encodes a 190-kDa protein that functions as part of alarge enzymatic complex. Although all the functions ofBRCA-1 are not known, it has been demonstrated to playa role in DNA repair, cell cycle regulation, and transcrip-tion regulation. There are over 250 known mutations inthe BRCA-1 gene. Although the gene is inherited in anautosomal dominant fashion, a second mutation in thewild-type gene is required for carcinogenesis. Clinically,King et al. showed that BRCA-1 mutations are morecommon in Ashkenazi Jewish women and overall muta-tion carriers have a 82% lifetime risk of developing
breast cancer, compared with 13% in the general popu-lation.1,11 Furthermore, the BRCA-1 mutation confersonset of disease at an earlier age (37% of cases occur byage 50 years), with a higher incidence of recurrent,multifocal, bilateral, and atypical breast carcinomas, i.e.,medullary.10 Screening for BRCA-1 mutation is cur-rently recommended for women with a family history of(1) early onset breast cancer (i.e., before age 50 years);(2) breast and ovarian cancer, especially if in the sameperson; (3) bilateral breast cancer; and (4) male breastcancer. Once a BRCA-1 mutation is identified, determin-ing which carriers are at the highest risk for breast canceris not currently possible.
SELDI-TOF MS may offer a solution to this problem,as it has several potential advantages as a clinical assay.Using readily accessible serum samples, this technologyhas proven to be reproducible, has adequate throughput,poses minimal risk to patients, and is relatively inexpen-sive.3–7 To date, serum protein profiling with SELDI-TOF MS has been applied to early detection of cancerstudies, with minimal application to prognostic assayevaluation. In particular, in prostate cancer, our labora-tory was able to distinguish invasive prostate cancerfrom benign prostatic hypertrophy and normal healthyvolunteers, using sera that were stratified for PSA lev-els.5–6,12 These results indicated a role for SELDI-TOFMS in the early detection of malignancy with use ofminimally invasive techniques (phlebotomy). However,these highly successful results have not been replicatedin breast cancer, probably reflecting the vast heteroge-
TABLE 2. Results from cross-validation analysis of thedecision classification trees for each sample set
Condition Sensitivity Specificity
BRCA-1 carrier vs. BRCA-1 Ca 87% (13/15) 87% (13/15)Sporadic vs. BRCA-1 Ca 94% (14/15) 100% (16/16)Normal vs. BRCA-1 Ca 87% (13/15) 94% (14/15)
FIG. 2. Diagram of a classification treefor BRCA-1 patients with cancer (Ca)and without cancer (No CA). Thesquares are the primary nodes andthe diamonds indicate terminal nodes.The mass value in the root nodes is fol-lowed by � the intensity value. Thequestion forming the first splitting rule isthe following: Is the intensity levels ofthe peak at 5909 Da lower or equal to1.871? Samples that follow the rule go tothe left “yes” terminal node, and samplesthat do not follow the rule go to a “no”daughter node to the right. The numbersof BRCA-1 (Ca) and (No Ca) samples ineach node are shown.
911PROTEIN PROFILE OF BRCA-1 AND SPORADIC BREAST CANCER
Ann Surg Oncol, Vol. 11, No. 10, 2004

neity of breast cancer, including inherited subtypes.8,9 Infact, the striking differences in the clinical manifestationsof BRCA-1 mutated breast cancer versus sporadic breastcancer speak to different disease entities that are notbeing adequately reflected under the pathologist’s micro-scope. Our ability to demonstrate these differences in theprotein profiling using SELDI-TOF MS lends credenceto the fact that sporadic breast cancer and hereditarybreast cancer are not one and the same.
Investigation into identifying these differentiating pro-teins may allow further elucidation of the roles of theBRCA-1 gene and lead to better-targeted therapy. Forexample, a primary target is the protein peak at 8.1-kDathat was overexpressed in the BRCA-1 cancer cohort,compared with both the BRCA-1 noncancer and sporadicbreast cancer samples. A peak of 8.1 kDa was alsoidentified in a separate serum profiling study as beingupregulated in breast cancer subjects.8 Purification andsequencing determinations of the differentially expressedpeaks detected in our study are ongoing.
Our ability to differentiate the BRCA-1 mutation car-riers who developed breast cancer from those who didnot holds much promise. Currently, once a woman isfound to have a BRCA-1 mutation, she is offered threepaths: (1) high-risk surveillance, (2) chemoprevention, or(3) prophylactic surgery. High-risk surveillance involvesmonthly breast self-examinations, clinical breast exami-nations every 6 months, and annual mammograms start-ing at age 25 years. For a BRCA1 carrier, by the age of40 years, the chance of developing carcinoma of thebreast is 20% (vs. 0.5% in the general population), andby age 50 years the risk increases to 50% (vs. 2% in thegeneral population). Close surveillance has the advan-tages of being noninvasive and minimally intrusive but isnot a preventative strategy; rather, it is an earlier detec-tion modality.
Additionally, mammography, the “gold standard” forcancer detection, has the shortcoming of an inability todetect masses in younger patients with dense breasts.Ironically, for BRCA-1 carriers, this is the very agegroup for which cancer detection is most needed. Che-moprevention, aside from its plethora of side effects,offers a 50% reduction in cancer development. In high-risk women, this occurs by reducing estrogen receptor–positive sporadic breast cancer, but its role in BRCA-1mutation carriers who traditionally generate estrogen re-ceptor–negative breast cancer is unclear. Prophylacticsurgery comprises bilateral oophorectomy (50% risk re-duction) and bilateral mastectomy (90% risk reduction).In a 2001 study, Meijers-Heijboer prospectively random-ized 76 BRCA-1 carriers to prophylactic bilateral mas-tectomies versus observation.13 There were no reportedcases of breast cancer among the patients who underwentsurgery, at a mean follow-up of 2.9 � 1.4 years. In thesurveillance cohort (N � 63), there were eight cases ofbreast cancer after a mean follow-up of 3.0 � 1.5 years.Despite the advantages of prophylactic mastectomies andoophorectomy, the effect these procedures may have onyoung women’s body image, quality of life, and long-term health sequela of premature menopause may makeprophylactic surgery a nonviable option.14 Obviously,the path chosen by a BRCA-1 carrier comes only withmuch contemplation and counseling regarding the riskand benefits of each treatment strategy, thus emphasizingthe need for better predictive diagnostic tests in order tohave a more complete clinical picture.
Our encouraging results would allow for the smallsubset of women with a BRCA-1 mutation who will notdevelop the disease in the near future to avoid unneces-sary chemoprevention and/or prophylactic surgery. Forthose women who will develop breast cancer, proteinprofiling offers reassurance that the preventative actions
FIG. 3. Representative SELDI spectracomparison of serum from normal healthyvolunteers (NHV), BRCA-1 noncancers(BRCA-1 No-Ca), BRCA-1 cancers(BRCA-1 Ca), and sporadic breast can-cers (Sporadic) in the 2,000 to 10,000m/z are shown. Each “boxed” regionidentifies a differentially expressedprotein within one of the samplegroups.
912 S. BECKER ET AL.
Ann Surg Oncol, Vol. 11, No. 10, 2004

were necessary. Since the time frame from baselineserum sample to cancer development was relatively short(within 3 years), one could envision following a wom-an’s protein profile annually and, when the profile beginsto change toward the BRCA-1 cancer profile, performingthe prophylactic mastectomies. Performing prophylacticsurgery when the woman is older may have less impacton body image and quality of life.
Although the results of our study are very provocative,several limitations must be addressed. First and fore-most, the sample size is too small to draw any definitiveconclusions. Second, regarding the sporadic breast can-cer vs. BRCA-1 cancer, the samples were from twodifferent institutions, and differences may have resultedin a geographic and specimen acquisition bias in theprotein profile comparison. Although this bias was pre-liminarily addressed by comparing the normal healthvolunteers (from Virginia) and the BRCA-1 carriers(from Nebraska), clarification with use of samples fromBRCA-1 carriers with and without cancer from Virginiafor comparison with the sporadic cases is currently underway. Last, both of these potential biases (small samplesize and different collection techniques) could be ad-dressed by enrolling multiple institutions with a standardcollection protocol.
The last limitation involves the BRCA-1 cohorts withrespect to timing. Since most breast cancers take years ofgrowth to become clinically apparent, one could postu-late that the protein profile of the BRCA-1 cancer groupreflected occult disease rather than prediction of pendingcancer development. Because they all developed cancerwithin 3 years of the baseline specimen, perhaps thecancer was there all along and escaped our detection byclinical examination and mammography. It is not uncom-mon for a woman with a BRCA-1 mutation to have anegative clinical breast examination and imaging studies,including a breast MRI, and then have breast cancerdiagnosed within a few short months. To address thisconcern, a longer window of time—say, 10 years—would be needed between baseline specimen and cancerdiscovery. Even if SELDI-TOF is only detecting occultcancer and not predicting for development of cancer, thiswould still be a powerful tool. Earlier detection of anycancer is known to increase survival. Our prophylacticsurgery would thus become “therapeutic” in cases foundto have occult disease but would still be prophylactic forthe contralateral side.
Conversely, the BRCA-1 carriers who did not developcancer were followed for 7 years. Ideally, a much longerfollow-up would be necessary to truly identify the car-riers who will never develop cancer. Unfortunately, theincidence of breast cancer continues to increase with age,
and thus a “long enough” follow-up may never beachieved. Perhaps it would be better to say that for thosewomen with a BRCA-1 carrier profile, we predict theywill not develop breast cancer within the next few years(in our study that would be up to 7 years). As ourfollow-up increases and the woman remains cancer-free,the prediction of disease-free interval would lengthen.
In summary, this exploratory small pilot study dem-onstrated that the serum protein profiles generated bySELDI-TOF MS differentiated BRCA-1 mutation carri-ers who developed breast cancer from those carriers whodid not with reasonable sensitivity and specificity. Inaddition, our results showed that the protein profiles ofsporadic breast cancer differ significantly from heredi-tary breast cancer attributed to BRCA-1 mutations andgives credence to the molecular heterogeneity of breastcancer. Perhaps a more feasible approach toward devel-oping a serum test for early detection of breast cancershould involve the analysis of more homogeneous co-horts such as BRCA-1 mutations and then progressiontoward the common thread that represents “breast can-cer” as a whole. Furthermore, determining the identitiesof the differentially expressed protein peaks could pro-vide new biomarkers for disease or a potential target fortherapy.
ACKNOWLEDGMENTS
The acknowledgments are available online in the full-text version at www.annalssurgicaloncology.org. They
are not available in the PDF version.
REFERENCES
1. Reynolds T. Study clarifies risk of breast, ovarian cancer amongmutation carriers. JNCI 2003;95:1816–18.
2. Hall JM, Lee MK, Newman B, et al. Linkage of early-onsetfamilial breast cancer to chromosome 17q21. Science 1990;250:1684–9.
3. Xiao Z, Adam BL, Cazares LH, et al. Quantitation of serumprostate-specific membrane antigen by a novel protein biochipimmunoassay discriminates benign from malignant prostate dis-ease. Cancer Res 2001;61:6029–33.
4. Wright Jr GL, Cazares LH, Leung SM, et al. ProteinChip surfaceenhanced laser desorption/ionization mass spectrometry: a novelprotein biochip technology for detection of prostate cancer biomar-kers in complex protein mixtures. Prostate Cancer and ProstateDiseases 1999;2:264–76.
5. Cazares LH, Adam, B-L, Ward MD, et al. Normal, benign, pre-neoplastic, and malignant prostate cells have distinct protein ex-pression profiles resolved by SELDI mass spectrometry. ClinCancer Res 2002;8:2541–52.
6. Adam BL, Qu Y, Davis JW, et al. Serum protein fingerprintingcoupled with a pattern-matching algorithm distinguishes prostatecancer from benign prostate hyperplasia and healthy men. CancerRes 2002;62:3609–14.
7. Petricoin EF, Ardekani A, Hitt B, et al. Use of proteomic patternsin serum to identify ovarian cancer. Lancet 2002;359:572–7.
913PROTEIN PROFILE OF BRCA-1 AND SPORADIC BREAST CANCER
Ann Surg Oncol, Vol. 11, No. 10, 2004

8. Li J, Zhang Z, Rosenzweig J, Wang Y, Chan D. Proteomics andbioinformatics approaches for identification of serum biomarkersto detect breast cancer. Clinical Chemistry 2002;48:1296–303.
9. Vlahou A, Laronga C, Wilson L, et al. A novel approach towardsdevelopment of a rapid blood test for breast cancer. Clin BreastCancer 2003;4:203–9.
10. Breast Cancer Linkage Consortium. Pathology of familial breastcancer: Differences in breast cancers in carriers of BRCA1 orBRCA2 mutations and sporadic breast cases. Lancet 1997;349:1505–10.
11. King MC, Marks JH, Mandell JB, and the New York BreastCancer Study Group. Breast and ovarian cancer risks due to
inherited mutations in BRCA1 and BRCA2. Science 2003;302:643–6.
12. Wright Jr GL. SELDI proteinchip MS: a platform for biomarkerdiscovery and cancer diagnosis. Expert Rev Mol Diagn 2002;2:549–63.
13. Meijers-Heijboer H, van Geel B, van Putten WL, et al. Breastcancer after prophylactic bilateral mastectomy in women with aBRCA-1 or BRCA-2 mutation. N Engl J Med 2001;345:159–64.
14. van Oostrom I, Meijers-Heijboer H, Ladder LN, et al. Long-termpsychological impact of carrying a BRCA1/2 mutation and pro-phylactic surgery: a 5-year follow- up study. J Clin Oncol 2003;21:3867–74.
914 S. BECKER ET AL.
Ann Surg Oncol, Vol. 11, No. 10, 2004