Embed Size (px)
Citation preview

Bscidt
a
t
e
U
B
U
S
H
J Oral Maxillofac Surg69:11-18, 2011
Surface Characteristics of BiomaterialsUsed for Space Maintenance in a
Mandibular Defect: A Pilot Animal StudyCharles Nguyen, MD, DDS,* Simon Young, DDS, PhD,†
James D. Kretlow, BS, BA,‡ Antonios G. Mikos, PhD,§ and
Mark Wong, DDS�
Purpose: The purpose of the present study was to evaluate the effect of implant porosity on wound healingbetween solid and porous implants placed within a bony mandibular defect with intraoral exposure.
Materials and Methods: Solid poly(methyl methacrylate) (PMMA) implants similar to those usedcurrently in clinical space maintenance applications in maxillofacial surgery were compared withpoly(propylene fumarate) implants that contained a porous outer surface surrounding a solid core. A10-mm diameter nonhealing bicortical defect with open communication into the oral cavity was createdin the molar mandibular region of 12 adult male New Zealand white rabbits. Of the 12 rabbits, 6 receivedthe hybrid poly(propylene fumarate) implants and 6 received the solid PMMA implants. At 12 weeks, therabbit mandibles were harvested and sent for histologic staining and sectioning.
Results: Gross inspection and histologic examination showed all 6 poly(propylene fumarate) implants to beintact within the defect site at the termination of the study period, with 3 of the 6 specimens exhibiting acontinuous circumferential soft tissue margin. In contrast, 5 of the 6 PMMA-implanted specimens wereexposed intraorally with an incomplete cuff of soft tissue around the implant. One of the PMMA-implantedspecimens exhibited complete extrusion and subsequent loss of the implant. Fisher’s exact test was used tocompare the occurrence of oral cavity wound healing between the 2 groups (P � .09).
Conclusions: Although statistically significant differences between the 2 groups were not seen, ourresults have indicated that advantages might exist to using porous implants for space maintenance.Additional study is needed to evaluate these findings.© 2011 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg 69:11-18, 2011fctacc
M
o
B
t
t
C
D
p
H
t
©
0
iomaterials can be used in oral and maxillofacialurgery for space maintenance before definitive re-onstruction of bony defects. A number of materials,ncluding poly(methyl methacrylate) (PMMA)1 andegradable calcium phosphates,2 have been used forhis purpose. These materials are used to facilitate
*Resident in Oral and Maxillofacial Surgery, Department of Oral
nd Maxillofacial Surgery, University of Texas Health Science Cen-
er at Houston, Houston, TX.
†Resident in Oral and Maxillofacial Surgery, Department of Bio-
ngineering, Rice University, Houston, TX.
‡MD/PhD Graduate Student, Department of Bioengineering, Rice
niversity, Houston, TX.
§Louis Calder Professor of Bioengineering and Chemical and
iomolecular Engineering, Department of Bioengineering, Rice
niversity, Houston, TX.
�Professor and Chairman, Department of Oral and Maxillofacial
urgery, University of Texas Health Science Center at Houston,
ouston, TX.
Dr Kretlow received support from the Baylor College of d
11
uture reconstruction in cases in which delayed re-onstruction is judged to be the most appropriatereatment option. Distortion of the surgical landmarksnd a decreased volume of the defect space afterollapse, contracture, and fibrosis of the tissue bedomplicate secondary surgical procedures. Deliberate
edicine Medical Scientist Training Program (National Institutes
f Health T32GM07330), Rice Institute of Biosciences and
ioengineering’s Biotechnology Training Grant (National Insti-
utes of Health T32GM008362), and a training fellowship from
he Keck Center Nanobiology Training Program of the Gulf
oast Consortia (National Institutes of Health grant 5 T90
K070121-04).
Address correspondence and reprint requests to Dr Wong: De-
artment of Oral and Maxillofacial Surgery, University of Texas
ealth Science Center at Houston, 6516 MD Anderson Blvd, Hous-
on, TX 77030; e-mail: [email protected]
2011 American Association of Oral and Maxillofacial Surgeons
278-2391/11/6901-0003$36.00/0
oi:10.1016/j.joms.2010.02.026

mtwsttoaBsdm
rospibiitogctthesisspbsabict
ibtbamtmvftfl
M
NaMupts1b
l2fiapp
fmctttpc
(TpN6wsh
tltp�mlootm
12 SURFACE CHARACTERISTICS OF BIOMATERIALS USED FOR SPACE MAINTENANCE
aintenance of the space within a bony defect allowshe surgeon to readily access the original defect sitehose dimensions have been preserved. Successful
pace maintenance involves the prevention of softissue collapse, combined with mechanical support ofhe defect as the incision heals. This does not alwaysccur, and wound dehiscence after the placement ofn implant is a problem encountered by surgeons.3
reakdown of the wound usually occurs late anduggests a failure of wound strength, rather than aefect in the initial healing of the soft tissue incisionargins.The problem of late wound dehiscence and mate-
ial exposure has been hypothesized to be the resultf failure of the connective tissue to mechanicallyupport the overlying epithelium during healing. Thisroblem has been encountered with a number of
mplant materials in various sites throughout theody, including the craniofacial complex.4-8 Improv-
ng the interface between the healing tissue and anmplant might reduce the incidence of this complica-ion. Previous studies have demonstrated the effectsf porosity and pore morphology on neotissue in-rowth into polymer constructs.9,10 This technologyan be adopted to create highly porous space main-ainers that facilitate tissue in-growth to promote re-ention of the implant.11,12 A porous–solid–porousybrid composite implant has been studied by Deant al13 for its potential to provide both mechanicalupport and local retention through tissue integrationn the healing defect site while preserving the defectpace. The present study compared the potentialpace maintenance capabilities of a porous–solid–orous hybrid polymer with PMMA, a commonly usediomaterial for space maintenance with a nonporousurface. Poly(propylene fumarate) (PPF) was selecteds the test material, because it is a well-characterizediopolymer with mechanical and handling character-
stics comparable to PMMA. PPF has also been directlyompared with PMMA14 in other biomedical applica-ions.
In the present study, we chose a nonhealing defectn the mandibular molar region of the rabbit on theasis of a model previously developed in our labora-ory.15 The defect was located entirely within theody of the mandible16 and had the advantage ofllowing the creation of an oral communication toore realistically simulate clinical conditions (ie,
rauma, widespread tumor resection) requiring spaceaintainer technology. This model allowed the obser-
ation of soft tissue regeneration within the oral de-ect and around the implanted biomaterials, despitehe potential contamination from oral secretions and
ora. oaterials and Methods
A total of 12 healthy, skeletally mature adult maleew Zealand white rabbits, at least 6 months old and
ll approximately the same age were purchased fromyrtle’s Rabbitry (Thompson Station, TN) and weresed as the model in the present study. All surgicalrocedures followed protocols approved by the insti-utional animal care and use committee of the Univer-ity of Texas Health Science Center at Houston. Of the2 rabbits, 6 received PPF porous–solid–porous hy-rid implants and 6 received solid PMMA implants.
PPF SYNTHESIS
PPF was synthesized according to previously estab-ished protocols developed in our laboratory as a-reaction process.17 The PPF structure was con-rmed by 1H nuclear magnetic resonance, and theverage molecular weight number was 1282, with aolydispersity index of 1.9, as determined by gelermeation chromatography.
PPF POROUS–SOLID–POROUS HYBRIDIMPLANT FABRICATION
The porous–solid–porous hybrid PPF implants wereabricated using 2 types of custom Teflon molds. Aold with 4-mm-thick � 8-mm-diameter cylindrical
utouts was first used to form the solid PPF core ofhe hybrid construct. A larger mold, with 6-mm-hick � 10-mm-diameter cylindrical cutouts was usedo form the final hybrid PPF implant by cross-linkingorous PPF around a the centrally located solid PPFore.For implant fabrication, PPF/N-vinyl pyrrolidone
NVP) (1:1 wt/wt ratio) implants were formed ineflon molds by cross-linking with 0.5 wt% benzoyleroxide (0.1 mg/mL in acetone). In brief, PPF andVP were manually mixed together after warming at0°C. After mixing, the benzoyl peroxide solutionas added before the mixture was placed into the
maller core molds. The samples were cured for 3ours at 60°C to ensure cross-linking.The remaining mixed PPF/NVP was used to make
he porous component of the hybrid implants. A salt-eaching technique was used, as previously described,o create the porous outer shell of the hybrid im-lants.18 In brief, 80 wt% NaCl crystals (500 to 700m) were added to the remaining PPF/NVP andixed thoroughly. This mixture was loaded into the
arge Teflon mold to form a 1-mm layer at the bottomf the well. The partially cured solid core disk previ-usly formed in the small Teflon mold was placed inhe center of the packed bottom layer in the largerold, and the remaining void (approximately 1 mm
n all sides of the core disk and above) was filled with

tp
rspNPcts
src1estePpwt
Swtc(u
aTasTe
imehaplKxwpummmnsrurdaN
S
NS
NYUGEN ET AL 13
he PPF/NVP-NaCl mixture. The mold was thenlaced in an oven at 60°C to fully cure for 24 hours.At the end of the 24 hours, the constructs were
emoved from their molds, placed in individual cas-ettes, and submerged in a sealed container of Milli-ore water on an agitator table for leaching of theaCl to form the outer porous layers of the hybridPF implant. Once the leaching was completed, theassettes were frozen and lyophilized under vacuumo sublimate any water remaining within the poroustructure of the hybrid implant (Fig 1).
Six porous–solid–porous hybrid PPF implants wereelected for implantation in vivo. The selection crite-ia included matching dimensions of the final implantonstruct with the size of the mandibular defect (ie,0 mm diameter � 6 mm height/thickness) and anven thickness of the 2 layers of porous PPF polymer,uch that the solid PPF core disk was centered withinhe entire construct. The selected implants were alsoxamined for a consistent outer covering of porousPF material, without large defects within the outerorous layer. The 6 selected implants were sterilizedith ethylene oxide and allowed to de-gas for more
han 24 hours in preparation for implantation.
PMMA IMPLANT FABRICATION
PMMA (cranioplastic type I, Slowset, Codman &hurtleff, DuPuy; Johnson & Johnson, Raynham, MA)as mixed according to the manufacturer’s instruc-
ions. When the mixture had reached a “dough-like”onsistency, it was packed into the large Teflon mold10-mm diameter � 6-mm-thick wells) previouslysed to form the PPF hybrid implants. The PMMA was
FIGURE 1. Porous–solid–porous hybrid PPF scaffold.
tyugen et al. Surface Characteristics of Biomaterials Used forpace Maintenance. J Oral Maxillofac Surg 2011.
llowed to set fully until completely hardened (Fig 2).he PMMA implants were selected for implantationccording to the presence of a completely solid outerurface with no visible pockets, pores, or bubbles.he PMMA implants were then sterilized with ethyl-ne oxide in the same manner as the PPF implants.
CREATION OF A NONHEALING MANDIBULARDEFECT AND CONSTRUCT IMPLANTATION
A previously established, 10-mm-diameter, nonheal-ng rabbit mandibular defect was used with a slight
odification in the present study.15 Before surgery,ach rabbit was given intramuscular buprenorphineydrochloride (0.1 mg/kg body weight) for postoper-tive analgesia and 0.5 mL Durapen (150,000 U/mLenicillin-G benzathine and 150,000 U/mL penicil-
in-G procaine) for perioperative antibiotic coverage.etamine hydrochloride (40 mg/kg body weight) andylazine hydrochloride (7.5 mg/kg body weight)ere given before induction. Next, the rabbits werelaced in the supine position, intubated, and placednder general anesthesia using an isoflurane/oxygenixture (2.5% to 3% isoflurance for induction, 2% foraintenance), with constant cardiac and respiratoryonitoring. The rabbit was draped in a sterile man-er, and a 7-cm midline incision through the skin anduperficial fascia was made, beginning 0.5 cm poste-ior to the mentum. Monopolar electrocautery wassed for dissection through the fascia, after which theight masseter muscle belly was exposed with bluntissection, taking care to identify and avoid the facialrtery and its major branches. Once visible, the soft
FIGURE 2. Solid PMMA scaffold.
yugen et al. Surface Characteristics of Biomaterials Used forpace Maintenance. J Oral Maxillofac Surg 2011.
issue along the inferior border of the body of the

motwah1Bitpf
sphprdwrrtutndotb1twftr
wmiAw
knmfdsTamtp
ecn5a
R
tidasd
Fmd
NS
14 SURFACE CHARACTERISTICS OF BIOMATERIALS USED FOR SPACE MAINTENANCE
andible was incised with electrocautery. The peri-steum was then elevated and the dissection ex-ended superiorly to expose a 4-cm-long � 1.5-cm-ide area on the lateral surface of the mandible. Next,10-mm trephine attached to a Stryker TPS surgicalandpiece (Stryker, Kalamazoo, MI) operating at5,000 rpm was used to create a bicortical defect.efore completion of the defect, a titanium-support-
ng plate (1.5-mm, 6-hole heavy gauge titanium; Syn-hes, West Chester, PA) was secured in place to laterrevent iatrogenic fracture and then rotated away
rom the defect site.Care was taken to cut through the mandible in 3
tages. First, the lateral cortical plate was completelyenetrated with the trephine and removed usingand instruments. Once the tooth roots were ex-osed and sectioned, a root elevator was used toemove the roots of the teeth, which traversed theefect. A 701 bur mounted on the Stryker handpieceas used to cut a 2- to 3-mm window on the alveolar
idge in the middle of the defect to provide access foremoval of the crowns of the associated teeth. Oncehe teeth had been removed, the trephine was againsed to complete the defect through the lingual cor-ical plate, with care taken not to damage the lingualerve on the medial aspect of the plate. After theefect was completed (Fig 3A), the site was thor-ughly irrigated with normal saline. The implant washen placed (Fig 3B), and the bone plate was rotatedack in place and secured with three additional.5-mm screws (Synthes). The communication intohe oral cavity was not closed. The surgical incisionas closed in 4 layers, securing the muscle, deep
ascia, superficial fascia, and skin using 4-0 Vicryl. Athe conclusion of the procedure, the anesthesia waseversed, and the rabbit was extubated.
For the postoperative 12-week period, all rabbitsere given a soft diet to avoid undue stress on theirandibles and were monitored closely for signs of
nfection, failure to thrive, and other complications.ll rabbits survived the 12-week postoperative periodithout complications.
MANDIBLE-IMPLANT HARVEST
At the end of the 12-week period, each rabbit wasilled by intravenous administration of 1 mL Beutha-asia-D (390 mg/mL pentobarbital sodium and 50g/mL phenytoin sodium). The mandibles were care-
ully dissected from the cranium with conservativeissection of the soft tissue and muscle of the rightide of the mandible around the area of the implant.he mandible was sectioned to obtain a specimenpproximately 6 � 4 cm, with the portions of theasseter and medial pterygoid muscles intact around
he area of the defect. The specimens were then
laced in 10% neutral buffered formalin for 48 hours, tmbedded in Exakt Technovit 7200 VLC, and thenut. Ground sections were prepared using the Do-ath/Exakt technique.17 The sections were ground to0 �m in thickness and stained with a methylene bluend basic fuchsin stain.
esults
GROSS SPECIMEN EXAMINATION
All 12 rabbits survived the surgery and postopera-ive period without significant adverse effects. Grossnspection of the defect area on harvesting the man-ibular specimens was performed. Superficially, thereas in and around the sutures placed to secure thekin and soft tissue layers did not exhibit woundehiscence in any of the 12 rabbits, and it appeared
IGURE 3. A, Ten-millimeter diameter defect in right mandibularolar area of rabbit. B, PPF hybrid implant placed in 10-mmiameter mandibular defect.
yugen et al. Surface Characteristics of Biomaterials Used forpace Maintenance. J Oral Maxillofac Surg 2011.
hat all the extraoral soft tissue incisions had healed
wsdcs
3sspia(esi
mfrd
gsPmpsimeoio
hppg
Fs
NS
Fb
NS
Fod(
NS
NYUGEN ET AL 15
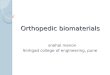
ell. Of the 6 rabbits receiving the PMMA implant, 5pecimens exhibited failed wound healing at the oralefect site (Fig 4). The sixth PMMA implant wasompletely extruded, and the surrounding teeth andoft tissue had collapsed into the defect.
Of the 6 rabbits receiving the hybrid PPF implants,specimens exhibited intact implants located in the
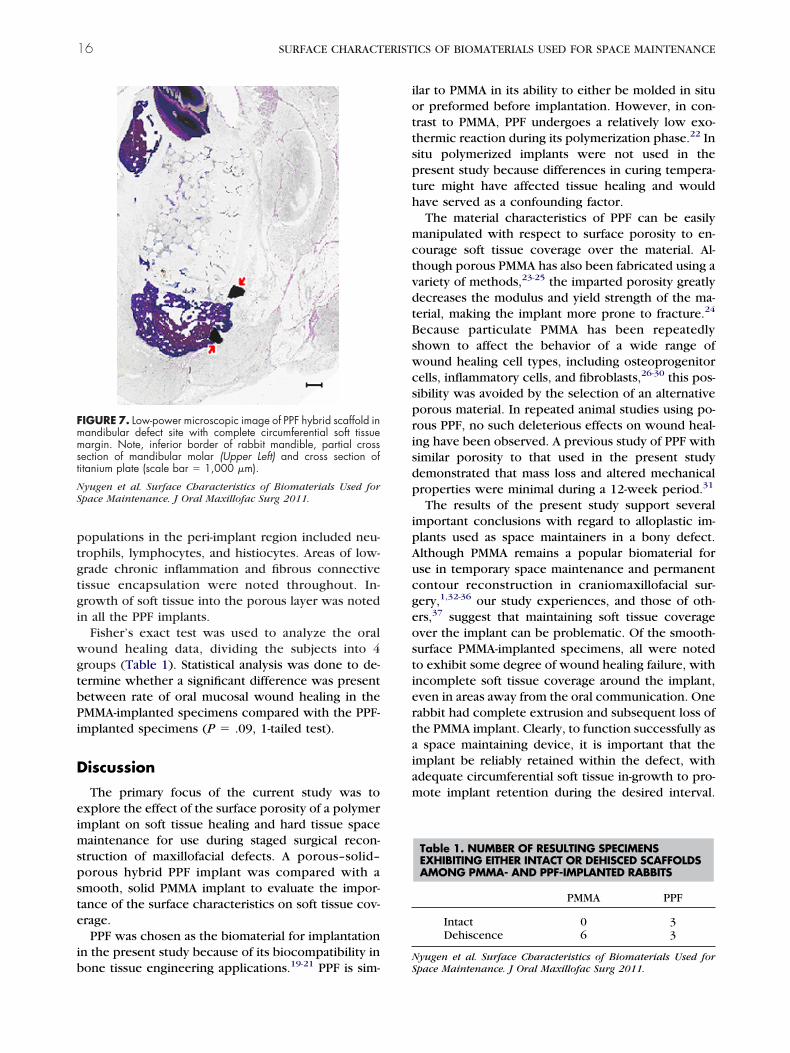
ame initial position, with the titanium plate andcrews still secured, and intact soft tissue growthresent around the wound site. No gross signs of
nflammation, suppuration, or necrosis were presentt the site of the defect or in the surrounding tissueFig 5). The other 3 rabbits had a similar result; how-ver, a hardened, dark green substance was noted,imilar to degrading rabbit feed, that had covered themplants at the superior aspect within the oral com-
IGURE 5. Gross examination of PPF-implanted rabbit mandiblehowing intact soft tissue healing around defect site.
IGURE 4. Gross examination of PMMA-implanted rabbit mandi-le, showing wound dehiscence in region of defect site.
yugen et al. Surface Characteristics of Biomaterials Used forpace Maintenance. J Oral Maxillofac Surg 2011.
syugen et al. Surface Characteristics of Biomaterials Used forpace Maintenance. J Oral Maxillofac Surg 2011.
unication. Veterinary personnel in charge of caringor the rabbits in the postoperative period did noteport any unusual long-term problems regarding theiet or health of any of the rabbits.
HISTOLOGIC EXAMINATION
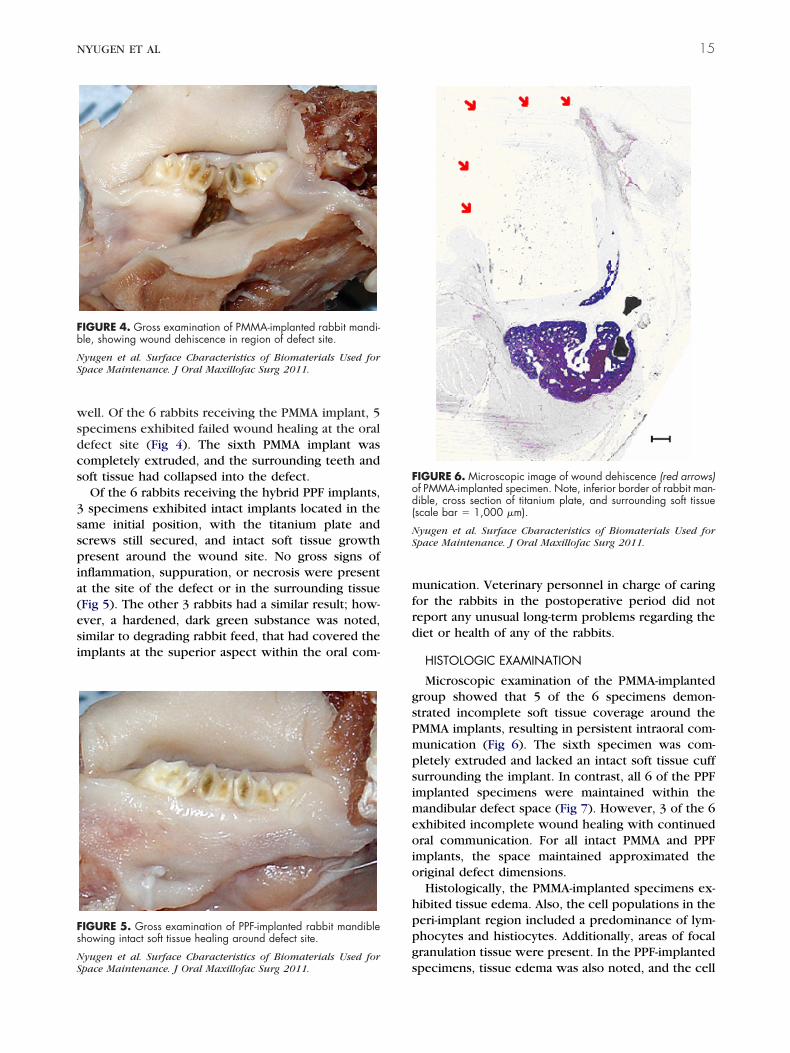
Microscopic examination of the PMMA-implantedroup showed that 5 of the 6 specimens demon-trated incomplete soft tissue coverage around theMMA implants, resulting in persistent intraoral com-unication (Fig 6). The sixth specimen was com-letely extruded and lacked an intact soft tissue cuffurrounding the implant. In contrast, all 6 of the PPFmplanted specimens were maintained within the
andibular defect space (Fig 7). However, 3 of the 6xhibited incomplete wound healing with continuedral communication. For all intact PMMA and PPF
mplants, the space maintained approximated theriginal defect dimensions.Histologically, the PMMA-implanted specimens ex-
ibited tissue edema. Also, the cell populations in theeri-implant region included a predominance of lym-hocytes and histiocytes. Additionally, areas of focalranulation tissue were present. In the PPF-implanted
IGURE 6. Microscopic image of wound dehiscence (red arrows)f PMMA-implanted specimen. Note, inferior border of rabbit man-ible, cross section of titanium plate, and surrounding soft tissuescale bar � 1,000 �m).
yugen et al. Surface Characteristics of Biomaterials Used forpace Maintenance. J Oral Maxillofac Surg 2011.
pecimens, tissue edema was also noted, and the cell
ptgtgi
wgtbPi
D
eimspste
ib
iottspth
mctvdtBswcsprisdp
ipAucgeostiertaiam
Fmmst
NS
16 SURFACE CHARACTERISTICS OF BIOMATERIALS USED FOR SPACE MAINTENANCE
opulations in the peri-implant region included neu-rophils, lymphocytes, and histiocytes. Areas of low-rade chronic inflammation and fibrous connectiveissue encapsulation were noted throughout. In-rowth of soft tissue into the porous layer was notedn all the PPF implants.
Fisher’s exact test was used to analyze the oralound healing data, dividing the subjects into 4
roups (Table 1). Statistical analysis was done to de-ermine whether a significant difference was presentetween rate of oral mucosal wound healing in theMMA-implanted specimens compared with the PPF-
mplanted specimens (P � .09, 1-tailed test).
iscussion
The primary focus of the current study was toxplore the effect of the surface porosity of a polymermplant on soft tissue healing and hard tissue space
aintenance for use during staged surgical recon-truction of maxillofacial defects. A porous–solid–orous hybrid PPF implant was compared with amooth, solid PMMA implant to evaluate the impor-ance of the surface characteristics on soft tissue cov-rage.PPF was chosen as the biomaterial for implantation
n the present study because of its biocompatibility in
IGURE 7. Low-power microscopic image of PPF hybrid scaffold inandibular defect site with complete circumferential soft tissueargin. Note, inferior border of rabbit mandible, partial cross
ection of mandibular molar (Upper Left) and cross section ofitanium plate (scale bar � 1,000 �m).
yugen et al. Surface Characteristics of Biomaterials Used forpace Maintenance. J Oral Maxillofac Surg 2011.
one tissue engineering applications.19-21 PPF is sim-NS
lar to PMMA in its ability to either be molded in situr preformed before implantation. However, in con-rast to PMMA, PPF undergoes a relatively low exo-hermic reaction during its polymerization phase.22 Initu polymerized implants were not used in theresent study because differences in curing tempera-ure might have affected tissue healing and wouldave served as a confounding factor.The material characteristics of PPF can be easilyanipulated with respect to surface porosity to en-
ourage soft tissue coverage over the material. Al-hough porous PMMA has also been fabricated using aariety of methods,23-25 the imparted porosity greatlyecreases the modulus and yield strength of the ma-erial, making the implant more prone to fracture.24
ecause particulate PMMA has been repeatedlyhown to affect the behavior of a wide range ofound healing cell types, including osteoprogenitor
ells, inflammatory cells, and fibroblasts,26-30 this pos-ibility was avoided by the selection of an alternativeorous material. In repeated animal studies using po-ous PPF, no such deleterious effects on wound heal-ng have been observed. A previous study of PPF withimilar porosity to that used in the present studyemonstrated that mass loss and altered mechanicalroperties were minimal during a 12-week period.31
The results of the present study support severalmportant conclusions with regard to alloplastic im-lants used as space maintainers in a bony defect.lthough PMMA remains a popular biomaterial forse in temporary space maintenance and permanentontour reconstruction in craniomaxillofacial sur-ery,1,32-36 our study experiences, and those of oth-rs,37 suggest that maintaining soft tissue coveragever the implant can be problematic. Of the smooth-urface PMMA-implanted specimens, all were notedo exhibit some degree of wound healing failure, withncomplete soft tissue coverage around the implant,ven in areas away from the oral communication. Oneabbit had complete extrusion and subsequent loss ofhe PMMA implant. Clearly, to function successfully as
space maintaining device, it is important that themplant be reliably retained within the defect, withdequate circumferential soft tissue in-growth to pro-ote implant retention during the desired interval.
Table 1. NUMBER OF RESULTING SPECIMENSEXHIBITING EITHER INTACT OR DEHISCED SCAFFOLDSAMONG PMMA- AND PPF-IMPLANTED RABBITS
PMMA PPF
Intact 0 3Dehiscence 6 3
yugen et al. Surface Characteristics of Biomaterials Used forpace Maintenance. J Oral Maxillofac Surg 2011.

Fnci
taTtosfgtmwdwpncodgcrigaatapd
motosttinacpttta
crpt
ctilhrospaiihmfip
rtgtmectctfiwwrm
A
MwSfJMp
R
NYUGEN ET AL 17
rom this perspective, PMMA-based solid implants doot appear to fulfill the criteria of reliable soft tissueoverage, particularly when intraoral exposure of themplant is present.
In contrast to the solid PMMA-implanted specimens,he rabbits receiving a porous implant fared better,lthough the difference was not statistically significant.hree rabbits had complete soft tissue coverage over
he implanted defect sites and regeneration of theverlying oral epithelium at the termination of thetudy at 12 weeks postoperatively. Complete circum-erential soft tissue growth was also noted, and in-rowth of soft tissue into the porous outer surface ofhe hybrid implants was present. However, the re-aining 3 specimens did not achieve oral closure andere found to have food impacted into the oral
efects. It is not known whether these specimensould have achieved complete coverage had the foodellets not become lodged into the defect sites. Alter-atively, food impaction might have occurred be-ause of failure of the wound to heal. However, thether areas surrounding the exposed PPF implants,istant from the oral communication, demonstratedood soft tissue in-growth. Regardless of the reason, aomparative analysis of the PPF and PMMA specimensevealed no statistically significant difference in thencidence of dehiscence (P � .09) between these 2roups. In the future, it would be desirable to conductsimilar study with a larger sample size and with the
nimals given a liquid diet. This would help establishhe effect of food impaction on oral soft tissue healinground porous PPF implants, because this unantici-ated outcome complicated the interpretation of ourata.By using a mandibular defect with an open com-unication with the oral cavity, it was possible to
bserve how soft tissue heals in close approximationo a polymer implant, despite bacterial seeding andral fluid contamination.38-45 In those cases in whichuccessful oral closure was observed, the porous na-ure of the hybrid implant provided the initial reten-ive features for connective tissue in-growth, which,n turn, supported epithelial migration across the con-ective tissue surface. The soft-tissue in-growth mightlso have helped reduce implant micromotion, an-horing the implant in place. This appears to haveromoted coverage over the implant and retention ofhe alloplast. This observation supports our conten-ion that mechanical support of the overlying softissue promotes wound healing and soft tissue cover-ge.
Although previous research has established the bio-ompatibility of both PMMA and PPF,20,46,47 all theabbits in the present study exhibited some degree oferi-implant inflammation, regardless of the polymer
ype. On microscopic examination, the predominantells noted were lymphocytes and histiocytes, consis-ent with a chronic inflammatory response. Grossnspection of the specimens did not reveal any puru-ence or other signs of active infection; thus, theistologic inflammation might have been a subclinicaleaction to the polymers or to contamination from theral communication. Similar chronic inflammatory re-ponses have been described in previous studies oforous acrylic-based cements, suggesting that this re-ction might be a normal response to an alloplasticmplant.48 Although intuitively the presence of peri-mplant inflammation might adversely affect woundealing, the stimulation of an inflammatory responseight actually be beneficial, preventing infection
rom pathogens seeded onto and within the differentmplants. Overt infection associated with either im-lant was not observed in our study.From this pilot project, much information was de-
ived concerning the ability of an oral communicationo heal over an alloplastic implant, if soft tissue in-rowth is promoted around the implant surface. Fu-ure investigations will focus on the role of specificaterials on soft tissue healing and explore differ-
nces between a porous–solid–porous PMMA implantomparable to the porous hybrid PPF implant used inhe present study. Similarly, solid PPF implants can beompared with solid PMMA devices. Although statis-ically significant conclusions could not be reachedrom the present findings, that complete wound heal-ng and soft tissue coverage was observed after 12
eeks in the specimens receiving porous implantsarrants continued investigation into the role of po-
ous space maintainers for temporary use in oral andaxillofacial surgery.
cknowledgment
The authors gratefully acknowledge support from the Oral andaxillofacial Surgery Foundation for this project. Additionally, weish to thank Dr Catherine Ambrose, Department of Orthopedic
urgery, University of Texas Health Science Center (Houston, TX)or her assistance in the preparation of the histologic slides, Drerry Bouquot, for analyzing the histologic specimens, and Synthesaxillofacial (Paoli, PA) for their generous donation of the surgicallates and screws used in our study.
eferences1. Goodger NM, Wang J, Smagalski GW, et al: Methylmethacrylate
as a space maintainer in mandibular reconstruction. J OralMaxillofac Surg 63:1048, 2005
2. Kihara H, Shiota M, Yamashita Y, et al: Biodegradation processof alpha-TCP particles and new bone formation in a rabbitcranial defect model. J Biomed Mater Res B Appl Biomater79:284, 2006
3. Mellonig JT, Nevins M: Guided bone regeneration of bonedefects associated with implants: An evidence-based outcomeassessment. Int J Periodontics Restorative Dent 15:168, 1995
4. Benoist M: Experience with 220 cases of mandibular recon-struction. J Oral Maxillofac Surg 6:40, 1978
5. Abramo AC, Casas SG, Dorta AA, et al: Late spontaneous extru-
sion of a texturized silicone gel mammary implant. AesthetPlast Surg 23:433, 1999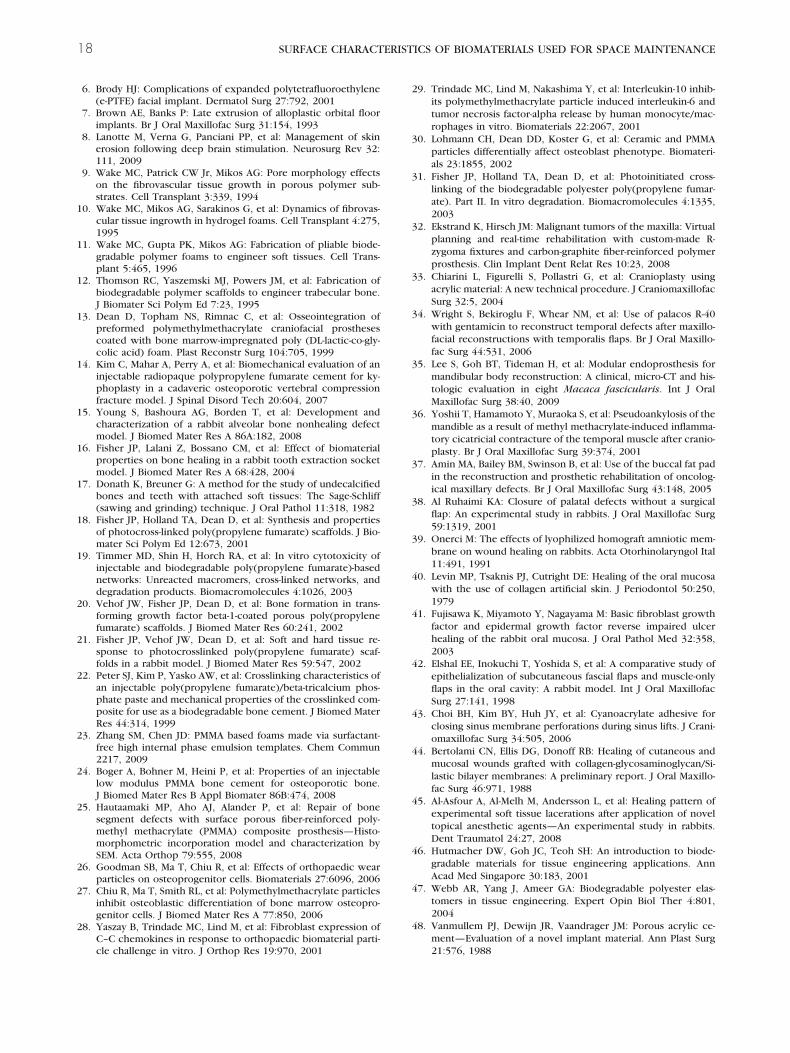
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
18 SURFACE CHARACTERISTICS OF BIOMATERIALS USED FOR SPACE MAINTENANCE
6. Brody HJ: Complications of expanded polytetrafluoroethylene(e-PTFE) facial implant. Dermatol Surg 27:792, 2001
7. Brown AE, Banks P: Late extrusion of alloplastic orbital floorimplants. Br J Oral Maxillofac Surg 31:154, 1993
8. Lanotte M, Verna G, Panciani PP, et al: Management of skinerosion following deep brain stimulation. Neurosurg Rev 32:111, 2009
9. Wake MC, Patrick CW Jr, Mikos AG: Pore morphology effectson the fibrovascular tissue growth in porous polymer sub-strates. Cell Transplant 3:339, 1994
0. Wake MC, Mikos AG, Sarakinos G, et al: Dynamics of fibrovas-cular tissue ingrowth in hydrogel foams. Cell Transplant 4:275,1995
1. Wake MC, Gupta PK, Mikos AG: Fabrication of pliable biode-gradable polymer foams to engineer soft tissues. Cell Trans-plant 5:465, 1996
2. Thomson RC, Yaszemski MJ, Powers JM, et al: Fabrication ofbiodegradable polymer scaffolds to engineer trabecular bone.J Biomater Sci Polym Ed 7:23, 1995
3. Dean D, Topham NS, Rimnac C, et al: Osseointegration ofpreformed polymethylmethacrylate craniofacial prosthesescoated with bone marrow-impregnated poly (DL-lactic-co-gly-colic acid) foam. Plast Reconstr Surg 104:705, 1999
4. Kim C, Mahar A, Perry A, et al: Biomechanical evaluation of aninjectable radiopaque polypropylene fumarate cement for ky-phoplasty in a cadaveric osteoporotic vertebral compressionfracture model. J Spinal Disord Tech 20:604, 2007
5. Young S, Bashoura AG, Borden T, et al: Development andcharacterization of a rabbit alveolar bone nonhealing defectmodel. J Biomed Mater Res A 86A:182, 2008
6. Fisher JP, Lalani Z, Bossano CM, et al: Effect of biomaterialproperties on bone healing in a rabbit tooth extraction socketmodel. J Biomed Mater Res A 68:428, 2004
7. Donath K, Breuner G: A method for the study of undecalcifiedbones and teeth with attached soft tissues: The Sage-Schliff(sawing and grinding) technique. J Oral Pathol 11:318, 1982
8. Fisher JP, Holland TA, Dean D, et al: Synthesis and propertiesof photocross-linked poly(propylene fumarate) scaffolds. J Bio-mater Sci Polym Ed 12:673, 2001
9. Timmer MD, Shin H, Horch RA, et al: In vitro cytotoxicity ofinjectable and biodegradable poly(propylene fumarate)-basednetworks: Unreacted macromers, cross-linked networks, anddegradation products. Biomacromolecules 4:1026, 2003
0. Vehof JW, Fisher JP, Dean D, et al: Bone formation in trans-forming growth factor beta-1-coated porous poly(propylenefumarate) scaffolds. J Biomed Mater Res 60:241, 2002
1. Fisher JP, Vehof JW, Dean D, et al: Soft and hard tissue re-sponse to photocrosslinked poly(propylene fumarate) scaf-folds in a rabbit model. J Biomed Mater Res 59:547, 2002
2. Peter SJ, Kim P, Yasko AW, et al: Crosslinking characteristics ofan injectable poly(propylene fumarate)/beta-tricalcium phos-phate paste and mechanical properties of the crosslinked com-posite for use as a biodegradable bone cement. J Biomed MaterRes 44:314, 1999
3. Zhang SM, Chen JD: PMMA based foams made via surfactant-free high internal phase emulsion templates. Chem Commun2217, 2009
4. Boger A, Bohner M, Heini P, et al: Properties of an injectablelow modulus PMMA bone cement for osteoporotic bone.J Biomed Mater Res B Appl Biomater 86B:474, 2008
5. Hautaamaki MP, Aho AJ, Alander P, et al: Repair of bonesegment defects with surface porous fiber-reinforced poly-methyl methacrylate (PMMA) composite prosthesis—Histo-morphometric incorporation model and characterization bySEM. Acta Orthop 79:555, 2008
6. Goodman SB, Ma T, Chiu R, et al: Effects of orthopaedic wearparticles on osteoprogenitor cells. Biomaterials 27:6096, 2006
7. Chiu R, Ma T, Smith RL, et al: Polymethylmethacrylate particlesinhibit osteoblastic differentiation of bone marrow osteopro-genitor cells. J Biomed Mater Res A 77:850, 2006
8. Yaszay B, Trindade MC, Lind M, et al: Fibroblast expression ofC–C chemokines in response to orthopaedic biomaterial parti-
cle challenge in vitro. J Orthop Res 19:970, 20019. Trindade MC, Lind M, Nakashima Y, et al: Interleukin-10 inhib-its polymethylmethacrylate particle induced interleukin-6 andtumor necrosis factor-alpha release by human monocyte/mac-rophages in vitro. Biomaterials 22:2067, 2001
0. Lohmann CH, Dean DD, Koster G, et al: Ceramic and PMMAparticles differentially affect osteoblast phenotype. Biomateri-als 23:1855, 2002
1. Fisher JP, Holland TA, Dean D, et al: Photoinitiated cross-linking of the biodegradable polyester poly(propylene fumar-ate). Part II. In vitro degradation. Biomacromolecules 4:1335,2003
2. Ekstrand K, Hirsch JM: Malignant tumors of the maxilla: Virtualplanning and real-time rehabilitation with custom-made R-zygoma fixtures and carbon-graphite fiber-reinforced polymerprosthesis. Clin Implant Dent Relat Res 10:23, 2008
3. Chiarini L, Figurelli S, Pollastri G, et al: Cranioplasty usingacrylic material: A new technical procedure. J CraniomaxillofacSurg 32:5, 2004
4. Wright S, Bekiroglu F, Whear NM, et al: Use of palacos R-40with gentamicin to reconstruct temporal defects after maxillo-facial reconstructions with temporalis flaps. Br J Oral Maxillo-fac Surg 44:531, 2006
5. Lee S, Goh BT, Tideman H, et al: Modular endoprosthesis formandibular body reconstruction: A clinical, micro-CT and his-tologic evaluation in eight Macaca fascicularis. Int J OralMaxillofac Surg 38:40, 2009
6. Yoshii T, Hamamoto Y, Muraoka S, et al: Pseudoankylosis of themandible as a result of methyl methacrylate-induced inflamma-tory cicatricial contracture of the temporal muscle after cranio-plasty. Br J Oral Maxillofac Surg 39:374, 2001
7. Amin MA, Bailey BM, Swinson B, et al: Use of the buccal fat padin the reconstruction and prosthetic rehabilitation of oncolog-ical maxillary defects. Br J Oral Maxillofac Surg 43:148, 2005
8. Al Ruhaimi KA: Closure of palatal defects without a surgicalflap: An experimental study in rabbits. J Oral Maxillofac Surg59:1319, 2001
9. Onerci M: The effects of lyophilized homograft amniotic mem-brane on wound healing on rabbits. Acta Otorhinolaryngol Ital11:491, 1991
0. Levin MP, Tsaknis PJ, Cutright DE: Healing of the oral mucosawith the use of collagen artificial skin. J Periodontol 50:250,1979
1. Fujisawa K, Miyamoto Y, Nagayama M: Basic fibroblast growthfactor and epidermal growth factor reverse impaired ulcerhealing of the rabbit oral mucosa. J Oral Pathol Med 32:358,2003
2. Elshal EE, Inokuchi T, Yoshida S, et al: A comparative study ofepithelialization of subcutaneous fascial flaps and muscle-onlyflaps in the oral cavity: A rabbit model. Int J Oral MaxillofacSurg 27:141, 1998
3. Choi BH, Kim BY, Huh JY, et al: Cyanoacrylate adhesive forclosing sinus membrane perforations during sinus lifts. J Crani-omaxillofac Surg 34:505, 2006
4. Bertolami CN, Ellis DG, Donoff RB: Healing of cutaneous andmucosal wounds grafted with collagen-glycosaminoglycan/Si-lastic bilayer membranes: A preliminary report. J Oral Maxillo-fac Surg 46:971, 1988
5. Al-Asfour A, Al-Melh M, Andersson L, et al: Healing pattern ofexperimental soft tissue lacerations after application of noveltopical anesthetic agents—An experimental study in rabbits.Dent Traumatol 24:27, 2008
6. Hutmacher DW, Goh JC, Teoh SH: An introduction to biode-gradable materials for tissue engineering applications. AnnAcad Med Singapore 30:183, 2001
7. Webb AR, Yang J, Ameer GA: Biodegradable polyester elas-tomers in tissue engineering. Expert Opin Biol Ther 4:801,2004
8. Vanmullem PJ, Dewijn JR, Vaandrager JM: Porous acrylic ce-ment—Evaluation of a novel implant material. Ann Plast Surg
21:576, 1988