Embed Size (px)
Citation preview

Surface CD14 positivity in B-cell chronic
lymphocytic leukaemia is related to clinical outcome
VINCENZO CALL EA, FORTUNATO MORABITO, BIANCA MARIA OLIVA, CATERINA STELITANO, DOME NICO LE VATO,*
ANGELA DATT ILO,* FRANCESCA GANGEMI, ANTONEL LA IORFI DA,* PASQUALE IACOPINO, FRANCESCO NO BILE,
ST EFAN O MOLICA* A ND MAURA BRUGIATE LLI Dipartimento Emato-Oncologia, Azienda Ospedaliera `Bianchi-Melacrino-
Morelli', Reggio Calabria, and *Divisione Ematologia, Azienda Ospedaliera `Ciaccio-Pugliese', Catanzaro, Italy
Received 20 April 1999; accepted for publication 23 July 1999
Summary. The aberrant expression of the myelomonocyticantigen CD14 was investigated in 128 untreated patientsdiagnosed with B-cell chronic lymphocytic leukaemia(B-CLL). A cut-off value of 5 ´ 109/l CD14-positive cells waschosen for statistical analysis because it showed the bestdiscriminating power among patients with different clinicalfeatures. 56 cases had a CD14� cell count >5 ´ 109/l. Asigni®cant correlation was found between Rai and Binetstages and total tumour mass (TTM) score on one hand, andthe absolute CD14� cell cut-off, on the other. This relation-ship was more evident in Rai 0±II and Binet A±B stages,where a CD14� cell count >5 ´ 109/l was preferentiallydistributed among patients with a higher tumoral mass. Inunivariate analysis the survival probability at 5 and 10 yearsshowed a signi®cant correlation with Rai and Binet stages,TTM score, CD14� absolute cell count and median age. The
median overall survival (OS) was 63 months for patientswith a CD14� cell count >5 ´ 109/l and 136 months forthose with a CD14� cell count <5 ´ 109/l. In the multi-variate Cox regression model, Rai stage, age and CD14�
cell count were independent signi®cant factors for theprediction of OS. Finally, when the same analysis wasrestricted to Rai stages 0±II, CD14� cell count was the onlysigni®cant independent parameter in¯uencing OS, with arelative death risk of 3´8. In conclusion, these data revealthat CD14� represents an important marker for predictingOS in B-CLL patients and, therefore, we suggest that itshould be included in the immunological characterization ofB-CLL.
Keywords: CD14, B-CLL, Rai stage, TTM score, overallsurvival.
The aberrant expression of myelomonocytic (MyMo) anti-gens on acute lymphoblastic leukaemia and multiplemyeloma neoplastic cells has been reported and associatedwith a poor prognosis (Sobol et al, 1987; Wiersma et al,1991; Grogan et al, 1989). The presence of MyMo antigenshas also been described in B-cell chronic lymphocyticleukaemia (B-CLL), but the de®nition of their real frequencyand clinical signi®cance is still debated (Woessner et al,1992; Nakase et al, 1996; Polliack et al, 1993; Tassies et al,1995). MyMo antigens on B-CLL cells have been related tothe oncogene c-fos expression and IL-1 production (Pintoet al, 1987; Morabito et al, 1987). Moreover, a directcorrelation with advanced disease stages and diffuse bonemarrow histology has been found in some studies (Molicaet al, 1991; Pinto et al, 1992). Among the MyMo antigens,
CD14 is a glycosyl-phosphatidylinositol cell surface mole-cule, which is involved in endotoxin-induced monocyteactivation by acting as a receptor for lipopolysaccharides(LPS) or complexes of LPS/LPS binding proteins (Goyertet al, 1988; Wright et al, 1990). Some authors reported ahigh CD14 antigen frequency in their B-CLL series(Morabito et al, 1987; Molica et al, 1991; Pinto et al,1992) and a direct correlation between CD14 expressionand advanced clinical stages (Molica et al, 1991; Pinto et al,1992). These results were not con®rmed by other studies(Polliack et al, 1993; Tassies et al, 1995). In addition thesoluble form of CD14 (sCD14), released from CD14expressing cells, was reported to be signi®cantly elevatedin B-CLL patients as compared to normal controls (Calleaet al, 1996).
In the present study we con®rmed the high frequency ofCD14 expression on B-CLL cells. In addition we demon-strated that surface CD14 positivity was associated withmore advanced disease and a shorter overall survival.
British Journal of Haematology, 1999, 107, 347±352
347q 1999 Blackwell Science Ltd
Correspondence: Dr Vincenzo Callea, Dipartimento Emato-Oncolo-gia, Azienda Ospedaliera `Bianchi-Melacrino-Morelli', 89100 Reggio
Calabria, Italy. e-mail: [email protected].

MATERIALS AND METHODS
Patients. 128 untreated patients with B-CLL, from twohaematological institutions in Southern Italy, entered thisstudy.
All cases ful®lled the recommended diagnostic criteria(International Workshop on CLL, 1989), presenting thetypical morphology of the classic B-CLL and showing theSIgdim, CD5�, CD19�, CD23� immunological pattern(Bennett et al, 1989).
The main clinical characteristics are summarized in TableI. Patients were prognostically strati®ed according to the Rai(Rai et al, 1975) and Binet stages (Binet et al, 1981) and totaltumour mass (TTM) score (Jaksic & Vitale, 1981). Rai stageswere grouped according to B-CLL guidelines (Cheson et al,1996). Bone marrow biopsy was performed in 89 cases andevaluated according to criteria published by Rozman et al(1984). Doubling time (DT) could be calculated in 38patients only; chemotherapy was started in the remainderbefore a suf®cient period of observation had elapsed; thus theinadequate number of patients with available DT preventedthe prognostic evaluation of this parameter.
Twenty-eight patients did not receive any treatment at thetime of study, and the others were treated with chlorambucil(CLB), either at high continuous dose or at intermittentstandard dose (Jaksic & Brugatelli, 1988), Binet's modi®edCHOP (Travade, 1990) and ¯udarabine (Keating et al, 1991).
Response to therapy was evaluated according to thefollowing de®nitions: (1) complete response (CR): achieve-ment of TTM score <2´3, which is the CLL diagnostic
threshold, in absence of bone marrow failure; (2) partialresponse (PR): reduction of the TTM score <50% of the initialvalue, which is a de®nition similar to that suggested by theNCI guidelines (Cheson et al, 1996); (3) no response (NR):absence of CR or PR.
Phenotype studies. Peripheral blood mononuclear cells(PBMC) were separated by Ficoll-Hypaque density gradient.PBMC were labelled with the following monoclonal anti-bodies: CD19 and CD23 (Becton Dickinson), CD5 (Dako), SIgFITC (Dako), CD14 (Ortho), CD21 (Ortho). Two-colourimmuno¯uorescence was performed using a phycoerythrin(PE) conjugated CD21 and FITC conjugated CD14, CD5 (PE)and CD19 (FITC).
Subsequently cells were stained with a FITC-labelledsecondary reagent F(ab)2 fragment of a rabbit anti-mouseimmunoglobulin (Ortho). From 5000 to 10 000 cells wereexamined for ¯uorescence, using an EPICS Prophyle II ¯owcytometer (Coulter). The lymphocyte population was gated ona two-parameter forward angle versus 908 light scatterhistogram. The percentage of cells expressing the surfaceantigen of interest was determined by establishing a cursorposition channel, using an irrelevant FITC-conjugated mouseIgG and a FITC secondary reagent as a negative control.
Statistical analysis. All calculations were performed usingthe SAS/STAT software package, release 6.06 of SASInstitute Inc., 1993.
The chi-square test was used for overall comparisons of thedistribution of CD14� absolute cell count for the cut-offvalue of 5 ´ 109/l among Rai and Binet stage, TTM scorevalue, bone marrow biopsy pattern, type of treatment andresponse to therapy. Actuarial survival was calculated by themethod of Kaplan and Meier. Difference in survival betweenprognostic groups was evaluated by univariate analysisusing the log-rank test, and the respective in¯uence of thedifferent variables on survival was calculated according toCox regression method.
RESULTS
CD14 antigen frequency in our series is depicted in Table I.To differentiate our patients, the level of 5 ´ 109/l CD14�
cells was chosen as a cut-off value because, according to ourstatistical analysis, this level showed the best discriminatingpower among patients with different clinical features.Overall, 43´7% of cases showed a CD14� cell count>5 ´ 109/l (Table I).
A signi®cant correlation was found between Rai and Binetstages and TTM value, on one hand, and the absolute CD14�
cell cut-off, on the other (Table II). This relationship wasparticularly evident when Rai 0±II and Binet A±B stageswere considered (Table II). In fact, patients showing a CD14�
cell count >5 ´ 109/l were preferentially distributed amongcases with a higher tumoural mass (Rai I±II, Binet B andTTM score >9 stages) as compared to the majority of patientsin Rai 0 and Binet A stages and TTM score <9, who had aCD14� cell count <5 ´ 109/l. No signi®cant difference wasfound in CD14 expression after strati®cation of patientsaccording to bone-marrow biopsy pattern (Table II), type oftreatment, and response to therapy (data not shown).
q 1999 Blackwell Science Ltd, British Journal of Haematology 107: 347±352
348 Vincenzo Callea et al
Table I. Main clinical and laboratory characteristics of B-CLL
patients.
Sex, male/female 76/52
Age, mean 6 SD 64´3 6 15´2
Rai stage
0 53I 11
II 36
III 9IV 19
Binet stage
A 85B 15
C 28
Total tumour mass score<9 65
>9 54
Bone marrow pattern
Non-diffuse 54
Diffuse 35
Lymphocyte count ´109/l (mean 6 SD) 58´1 6 63´9
CD14 cells (%) (mean 6 SD) 25´1 6 29´9
Absolute CD14� cell count ´ 109/l (mean 6 SD) 16´2 6 37´2
Cases with CD14� cell count ´109/l
<5 72
>5 56

349CD14 Expression and Survival in B-CLL
q 1999 Blackwell Science Ltd, British Journal of Haematology 107: 347±352
Table II. Absolute CD14� cell distribution in Rai, Binet, TTM score and bone
marrow biopsy pattern, according to a cut-off value of 5 ´ 109/l positive cells.
<5 ´ 109/l >5 ´ 109/l
No. of No. of
patients % patients % P*
Rai stage
0 40 31´2 13 10´1 0´001I±II 12 9´3 35 27´3
III±IV 20 15´6 8 6´2
Binet stageA 48 37´5 37 28´9 0´019
B 4 3´1 11 11´7
C 20 15´6 8 6´2
TTM score
<9 41 34´4 24 20´1 0´026
>9 23 19´3 31 26´0
BM pattern
Non-diffuse 34 38´2 20 54 n.s
Diffuse 18 20´2 17 19
* Chi-square test.
Table III. Survival probability according to age, Rai, Binet, TTM score, bone marrow biopsy pattern andabsolute CD14� cells.
At 5 years At 10 years(% of predicted (% of predicted Univariate analysis*
survivors 6 SEM) survivors 6 SEM) (P)
Age (years)
<66 78´8 6 5´4 51´6 6 9´3 0´01>66 51´7 6 7´2 36´6 6 8´6
Rai stage
0 80´6 6 5´9 77´5 6 6´4 0´0001I±II 61´1 6 8´6 14´3 6 12´2
III±IV 46´9 6 9´8 20´5 6 8´4
Binet stage
A 76´0 6 5´1 46´0 6 14´4 0´0003
B 48´0 6 16´0 0
C 42´6 6 9´8 0
TTM score
<9 76´5 6 5´7 60´2 6 8´2 0´003
>9 52´6 6 7´9 29´6 6 10´9
BM pattern
Non-diffuse 68´0 6 7´2 46´4 6 10´0 0´06Diffuse 56´1 6 10´0 31´6 6 12´5
Absolute CD14� cell count
<5 ´ 109/l 72´2 6 5´8 41´1 6 13´3 0´02>5 ´ 109/l 54´6 6 7´6 0
* Chi-square test.

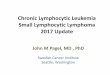
After a median follow-up of 56´4 months, 52 patients haddied and 11 were lost to follow-up. Table III shows thesurvival probability at 5 and 10 years, in univariate analysis,of patients strati®ed according to the main clinical char-acteristics and to the absolute CD14� cell count. Asigni®cant correlation was found between survival and Raiand Binet stages, TTM score values, CD14� cell absolutecount and median age. In particular, the median overallsurvival (OS) was 63 months for patients with CD14� cellcount >5 ´ 109/l and 136 months for those showing CD14�
cell count <5 ´ 109/l (Fig 1). All of the factors which were
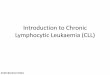
signi®cant in univariate analysis entered the multivariateCox regression method. As reported in Table IV, Rai stage,age and CD14� cell count were found to be independentsigni®cant prognostic factors for OS. The absolute CD14� cellcount was associated with the highest relative risk ofdeath compared to the remaining factors. Furthermore, thesame analysis was performed with the subset of patientsin Rai stages 0±II: absolute CD14 cell count was theonly signi®cant independent parameter in¯uencing theoverall survival, with a relative death risk of 3´8 (Table V,Fig 2).
q 1999 Blackwell Science Ltd, British Journal of Haematology 107: 347±352
350 Vincenzo Callea et al
Fig 1. Overall survival of B-CLL patients according to a cut-off value of CD14� absolute cell count of 5 ´ 109/l.
Fig 2. Overall survival of Rai 0±II stage B-CLL patients according to CD14� absolute cell count cut-off of 5 ´ 109/l.

351CD14 Expression and Survival in B-CLL
q 1999 Blackwell Science Ltd, British Journal of Haematology 107: 347±352
DISCUSSION
A high frequency of CD14 antigen expression was observedin our series, con®rming the results of some studies(Woessner et al, 1992; Nakase et al, 1996; Morabito et al,1987; Molica et al, 1991; Pinto et al, 1992) and contrastingwith other reports (Polliack et al, 1993; Tassies et al, 1995).
These differences cannot be due to methodologicalreasons: ¯ow cytometry was employed to perform all testsand controls with irrelevant FITC-conjugated antibodies andFITC-labelled secondary reagent were constantly used.Furthermore, in the present study positive and negativecells were found in individual patients with the same mouseisotype MoAbs. Possibly, the contrasting results obtained inother studies could be attributed to the different types ofMoAbs employed, as they could recognize different CD14epitopes. In this respect, Wormsley et al (1990) reportedcon¯icting results on CD14 expression in B-CLL. In thisreport, differences were documented not only using distinctanti-CD14 MoAbs, but also different lots of the same product.
When the analysis was limited to Rai 0±II and Binet A andB stages, a lower CD14 expression was found in patients at amore initial phase of the disease. Likewise, CD14 expressionwas directly correlated with TTM score values, which betterexpresses the tumoural burden. In contrast, this correlationwas not observed in Rai III±IV and Binet C cases, whereanaemia and/or thrombocytopenia are not necessarily dueto the neoplastic mass; in fact, in 11/28 cases autoimmunephenomena could be postulated.
To our knowledge, previous studies dealing with CD14
expression did not correlate this parameter with overallsurvival. Our results indicated that patients who express>5000 CD14� cells have a shorter probability of survivalwith a median OS of 63 months as compared with amedian OS of 136 months in those who express <5000CD14 cells. Multivariate analysis con®rmed this ®nding:CD14 absolute count, together with Rai stage and age, wasan independent signi®cant variable. Finally, when thisanalysis was limited to Rai 0±II stages, the absoluteCD14� cell count was the only signi®cant variablein¯uencing overall survival.
From a biological point of view, it is dif®cult to explain theassociation of CD14 expression with clinical outcome. Thefunction of the CD14 antigen in B-CLL is unknown. Thisantigen is normally expressed on the monocyte-macrophagesurface (Goyert et al, 1988) and works as a receptor forlipopolysaccharide (LPS) and LPS binding proteins (Wrightet al, 1990) which stimulate these cells to synthesize andsecrete immunoregulatory and in¯ammatory moleculessuch as IL-1, IL6 and TNFa (Morrison & Ryan, 1987). Weknow that B-CLL cells can secrete all these pro-in¯ammatorycytokines (Morabito et al, 1987; Uggle et al, 1987; Callea et al,1996; Foa et al, 1990). Furthermore, we found that thesoluble form of CD14 (sCD14), which enhances themonocyte-macrophage activity (Frey et al, 1992), is over-expressed in B-CLL sera (Callea et al, 1996). Taking all these®ndings together, it could be hypothesized that CD14,whether as a surface antigen or in the soluble form, exertsan important role in B-CLL infections. Further studies arenecessary to explore this hypothesis, considering thatinfections represent frequent relevant complications andcause of death in B-CLL patients.
In conclusion, although the biological role of CD14 in B-CLL should be further investigated, we suggest the inclusionof this marker in the panel of B-CLL immunologicalcharacterization because of its ability to discriminatebetween groups with different prognoses which may needmore appropriate treatments (Molica, 1999).
REFERENCES
Bennett, J.M., Catovsky, D., Daniel, M.T., Flandrin, G., Galton, D.A.G.,
Gralnick, H.R., Sultan, C., the French±American±British (FAB)
Cooperative Group (1989) Proposal for the classi®cation of
chronic (mature) B and T lymphoid leukaemias. Journal of ClinicalPathology, 42, 567±584.
Binet, J.L., Auquier, A., Dighiero, G., Chastang, C., Piguet, H.,
Goasguen, J., Vaugier, C., Potron, G., Colona, P., Oberling, E.,Thomas, M., Tchernia, G., Jaquillat, C., Boivin, P., Lesty, C., Duault,
M.T. & Gremy, F. (1981) A new prognostic classi®cation of chronic
lymphocytic leukemia derived from a multivariate survival
analysis. Cancer, 48, 198±206.Callea, V., Morabito, F., Luise, F., Piromalli, A., Filangeri, M.,
Stelitano, C., Iacopino, P., Nobile, F. & Brugiatelli, M. (1996)
Clinical signi®cance of sIL2R, sCD23, sICAM1, IL6 and sCD14
serum levels in B-cell chronic lymphocytic leukemia. Haematolo-gica, 81, 310±315.
Cheson, B.D., Bennett, J.M., Grever, M., Kay, N., Keating, M.J.,
O'Brien, S. & Rai, K.R. (1996). National Cancer Institute sponsoredworking group guidelines for chronic lymphocytic leukemia: revised
guidelines for diagnosis and treatment. Blood, 87, 4990±4997.
Table IV. Multivariate analysis of prognostic vari-
ables for survival.
Variable P* Risk
Age 0´012 1´041
Sex n.s. ±
Rai stage 0´0009 1´45Binet stage n.s. ±
TTM score n.s. ±
CD14 (absolute count) 0´0027 2´69
* Cox regression analysis.
Table V. Multivariate analysis of prognostic vari-
ables for survival for Rai stage 0±II patients.
Variable P* Risk
Age n.s. ±
Sex n.s. ±
Rai stage n.s. ±Binet stage n.s. ±
TTM score n.s. ±
CD14 (absolute count) 0´0017 3´38
* Cox regression analysis.

Foa, R., Massaia, M., Cardona, S., Tos, A.G., Bianchi, A., Attisano, C.,
Guarini, A., Francia di Celle, P. & Fierro, M.T. (1990) Production of
tumor necrosis factor-alpha by B-cell chronic lymphocytic
leukemia cells: a possible role of TNF in the progression of thedisease. Blood, 76, 393±400.
Frey, E.A., Miller, D.S., Jahr, T.G., Sundan, A., Bazil, V., Espevik, K.T.,
Finlay, B.B. & Wright, S.D. (1992) Soluble CD14 participates in the
response of cells to lipopolysaccharides. Journal of ExperimentalMedicine, 176, 1665±1671.
Goyert, S.M.E., Ferrero, W.J., Rettig, A.K., Yenamandra, F., Obata, F.
& Le Beau, M.M. (1988) The CD14 monocyte differentiationantigen maps to a region encoding growth factors and receptors.
Science, 239, 497±500.
Grogan, T.M., Durie, B.G.M., Spier, C.M., Richter, L. & Vela, E. (1989)
Myelomonocytic antigen positive multiple myeloma. Blood, 73,763±769.
International Workshop on Chronic Lymphocytic Leukemia (1989)
Recomendations for diagnosis, staging and response criteria.
Annals of Internal Medicine, 110, 236±238.Jaksic, B. & Brugiatelli, M. (1988) High dose continuous chloram-
bucil vs intermittent chlorambucil plus prednisone for treatment
of B-CLL. Nouvelle Revue FrancËaise d'HeÂmatologie, 30, 437±442.Jaksic, B. & Vitale, B. (1981) Total tumor mass score (TTM): a new
parameter in chronic lymphocytic leukaemia. British Journal of
Haematology, 49, 405±413.
Keating, M.J., Kantarajian, H., O'Brien, S., Koller, C., Talpaz, M.,Schachner, J., Chilps, C.C., Freireich, E.J. & McCredie, K.B. (1991)
Fludarabine: a new agent with marked cytoreduction activity in
untreated chronic lymphocytic leukemia. Journal of Clinical
Oncology, 9, 44±49.Molica, S. (1999) Is it time for a reassessment of prognostic features
in B-cell chronic lymphocytic leukemia? Hematology and Cell
Therapy, 41, 87±93.
Molica, S., Dattilo, A. & Alberti, A. (1991) Myelomonocyticassociated antigens in B-chronic lymphocytic leukemia:
analysis of clinical signi®cance. Leukemia and Lymphoma, 5,
139±144.Morabito, F., Prasthofer, E.F., Dunlap, N.E., Grossi, C.E. & Tilden, A.B.
(1987) Expression of myelomonocytic antigens on chronic
lymphocytic leukemia B cells correlates with their ability to
produce interleukin 1. Blood, 70, 1750±1757.Morrison, D.C. & Ryan, J.L. (1987) Endotoxin and disease mechan-
ism. Annual Review of Medicine, 38, 417±422.
Nakase, K., Kita, K., Shiku, H., Tanaka, I., Nasu, K., Dohy, H., Kyo, T.,
Tsutani, H. & Kamada, N. (1996) Myeloid antigen, CD13, CD14and/or CD33 expression is restricted to certain lymphoid
neoplasms. American Journal of Clinical Pathology, 105, 761±768.
Pinto, A., Colletta, G., Del Vecchio, L., Rosati, R., Attadia, V., Cimino,R. & Colombatti, A. (1987) c-fos expression in human hemopoietic
malignancies is restricted to acute leukemias with monocytic
phenotype and to subset of B cell leukemias. Blood, 70, 1450±1457.
Pinto, A., Zagonel, V., Carbone, A., Serraino, D., Marotta, G.,
Volpe, R., Colombatti, A. & Del Vecchio, L. (1992) CD13expression in B-cell chronic lymphocytic leukemia is associated
with the pattern of bone marrow in®ltration. Leukemia and
Lymphoma, 6, 209±218.
Polliack, A., Rabinowitz, R., Leizerowitz, R., Keren-Zur, Y. &Schlesinger, M. (1993) Myelomonocytic antigens are rarely
expressed on B-lymphocytic leukemia cells. Leukemia and Lym-
phoma, 9, 125±131.Rai. K.R., Sawitsky, A., Cronkite, E.P., Chanana, A.D., Levy, R.N. &
Pasternak, B.S. (1975) Clinical staging of chronic lymphocytic
leukemia. Blood, 46, 219±234.
Rozman, C., Montserrat, E., Rodriguez-Fernandez, J.M., Ayats, R.,VallespiÁ, T., Parody, R., Rios, A., Prados, D., Gomis, F., AlcalaÁ, A.,
Gutierrez, M., Maldonado, J., Gonzales, C., Giralt, M., Hernandez-
Nieto, L., Cabrera, A. & Fernandez-Ranada, J.M. (1984) Bone
marrow histologic pattern, the best single prognostic parameter inchronic lymphocytic leukemia: a multivariate survival analysis of
329 cases. Blood, 64, 642±648.
Sobol, R.E., Mick, R., Royston, I., Davey, F.R., Ellison, R.R., Newman,R., Cuttner, J., Grif®n, J.D., Collins, H., Nelson, D.A. & Bloom®eld,
C.D. (1987) Clinical importance of myeloid antigen expression in
adult lymphoblastic leukemia. New England Journal of Medicine,
316, 1111±1117.Tassies, D., Montserrat, E., Reverter, J.C., Villamor, N., Rovira, M. &
Rozman, C. (1995) Myelomonocytic antigens in B-cell chronic
lymphocytic leukemia. Leukemia Research, 19, 841±848.
Travade, P., for the French Cooperative Group on CLL (1990) Theexperience of the French Cooperative Group in the treatment of
CLL. Nouvelle Revue FrancËaise d'HeÂmatologie, 32, 313±317.
Uggle, C., Aguilar-Santelises, M., Rosen, A., Mellstedt, H. & Jondel,
M. (1987) Spontaneous production of interleukin 1 activity bychronic lymphocytic leukemia cells. Blood, 70, 1851±1857.
Wiersma, S.R., Ortega, J., Sobel, E. & Weinberg, K.I. (1991) Clinical
importance of myeloid antigen expression in acute lymphoblasticleukemia of childhood. New England Journal of Medicine, 324, 800±
825.
Woessner, S., Florensa, L., Besses, C., Vila, R.M., Galles, C., Palou, L.
& Sabrafen J.S. (1992) Immunocytochemical investigation ofnormal and chronic lymphocytic leukemia lymphocytes reveals
frequent reactivity with some myelomonocytic associated anti-
bodies. Leukemia Research, 16, 505±510.
Wormsley, S.B., Saiget, S.L., Gadol, N. & Rai K.R. (1990) Will the realCD14 please stand up? Blood, 76, 393a (abstract 1563).
Wright, S.D., Ramos, R.A., Tobias, P.S., Ulevitch, R.J. & Mathison, J.C.
(1990) CD14, a receptor for complexes of lipopolysaccharides(LPS) and LPS binding protein. Science, 249, 1431±1433.
q 1999 Blackwell Science Ltd, British Journal of Haematology 107: 347±352
352 Vincenzo Callea et al