Embed Size (px)
Citation preview

The Royal Marsden
1
Dr Claire Dearden
Consultant Haematologist
The Royal Marsden
Chronic Lymphocytic Leukaemia

The Royal Marsden
Chronic Lymphocytic Leukaemia
2
– Commonest leukaemia in western world
– Incidence of 4/100,000 pa
– Familial risk (7-8 fold)
– Median Age 72 years
– M:F = 2:1
– Diagnosis is usually made as an incidental
finding on a routine FBC
– Highly variable natural history
– Clinical and genetic heterogeneity
– Prognostic markers (IGVH, TP53)
The Royal Marsden
Case History
• A 78 year old man
• Fit and well
• Routine monitoring for PSA
• FBC also taken
• Noted to have a raised WBC 11 x 109/l
• Lymphocytes 6 x 109/l (normal range 1-3)
• Report states- “ smear cells seen on film ? CLL”
3

The Royal Marsden
What would you do?
4
A. Ignore the result
B. Repeat the FBC in a year when the PSA is next due
C. Repeat the FBC in 3 months
D. Refer for a standard haematology specialist appointment
E. Tell the patient they may have leukaemia and refer on an urgent two-week-wait rule with suspected malignancy
F. Phone/write to the Haematologist for advice
Ignore
the re
sult
Repeat the FB
C in a
year..
.
Repeat the FB
C in 3
month
s
Refer f
or a st
andard h
a...
Tell th
e patie
nt they m
a...
Phone/writ
e to th
e Hae...
0% 0%
39%
27%
21%
13%

The Royal Marsden
Chronic Lymphocytic Leukaemia
5
– Most patients are asymptomatic at
the time of diagnosis
– Clinical features
– Immune dysfunction
– Infection
– Autoimmunity (affecting components
of blood)
– Tissue infiltration
– Lymph nodes, spleen & other tissues
– Eventual BM failure (cytopenia)

The Royal Marsden
Case History
• A 52 year old woman
• Mild fatigue, no other B symptoms (fevers, sweats ,
weight loss)
• No recent infections or dental problems
• Cervical lymph nodes present for 2 months –about 1-
1.5 cm, painless, mobile
• No other palpable disease or signs of local infection
6

The Royal Marsden
What would you do?
7
A. Ask her to return in a
month if the nodes have
not gone
B. Check viral screen
C. Check a FBC
D. Send a TWW referral to
the head and neck team
E. All of B-D
F. None of the above
Ask h
er to re
turn
in a
m...
Check v
iral s
creen
Check a
FBC
Send a TW
W re
ferr
al to ..
.
All of B
-D
None of t
he above
4%0% 0%
27%
9%
60%

The Royal Marsden
Case History
• The patient was sent to the head and neck surgeons
• Lymph node biopsy reported as Small Lymphocytic
Lymphoma
• Referred for full TAP CT which showed generalised low-
volume lymphadenopathy (<1.5 cm)
• Referred to haematology
• Had a FBC – lymphocyte count of 35, otherwise normal
• Flow cytometry confirmed CLL !!
8

The Royal Marsden
• CLL and SLL are the same disease. About 10% patients may
present with lymphadenopathy alone with normal FBC (BM
usually involved)
• About 1/3rd patients with CLL may never require any treatment
• Infection is a risk even in patients with untreated CLL
• Progression is associated with increased tumour bulk and genetic
complexity
• Treatment requirement is based on a set of criteria confirming
disease activity/progression
• Natural History- remissions /relapses over years-decades
• Incurable (but often manageable) with current therapy
9
Chronic Lymphocytic Leukaemia

The Royal Marsden
A 52 year old man with untreated CLL presents
with a painful rash on his right chest wall
10

The Royal Marsden
What would you do?
11
A. Send him home
B. Send him to A&E
C. Phone his haematology
team
D. Prescribe topical aciclovir
cream
E. Prescribe oral aciclovir
F. Administer the zoster
vaccine Send h
im h
ome
Send him
to A
&E
Phone his
haemato
logy
...
Presc
ribe to
pical a
ciclo
vi...
Presc
ribe o
ral a
ciclo
vir
Admin
ister t
he zost
er v...
0% 0% 0%
68%
0%
32%

The Royal Marsden
• Common: 0.26- 0.47 per patient year
• Mainly bacterial respiratory tract (S pneumonia, S
aureus, H influenzae )
• Chronic sinusitis and bronchiectasis
• Herpes virus re-activation (shingles)
• Fungal and opportunistic infections rare in untreated
patients
• Infection is major cause of morbidity and mortality
(50%) in advanced CLL
Infectious complications in CLL
12

Early-Stage CLL:
Watch & Wait Remains the Standard Approach
Chlorambucil
No
Therapy
Low risk: W&W
High risk: FCR
High risk: W&W
French-German CLL7 Trial French Binet-A Trial
Dighiero et al. N Engl J Med 1998 Schweighofer et al. ASH 2013
Patients on W&W should be encouraged to follow a normal healthy lifestyle
13
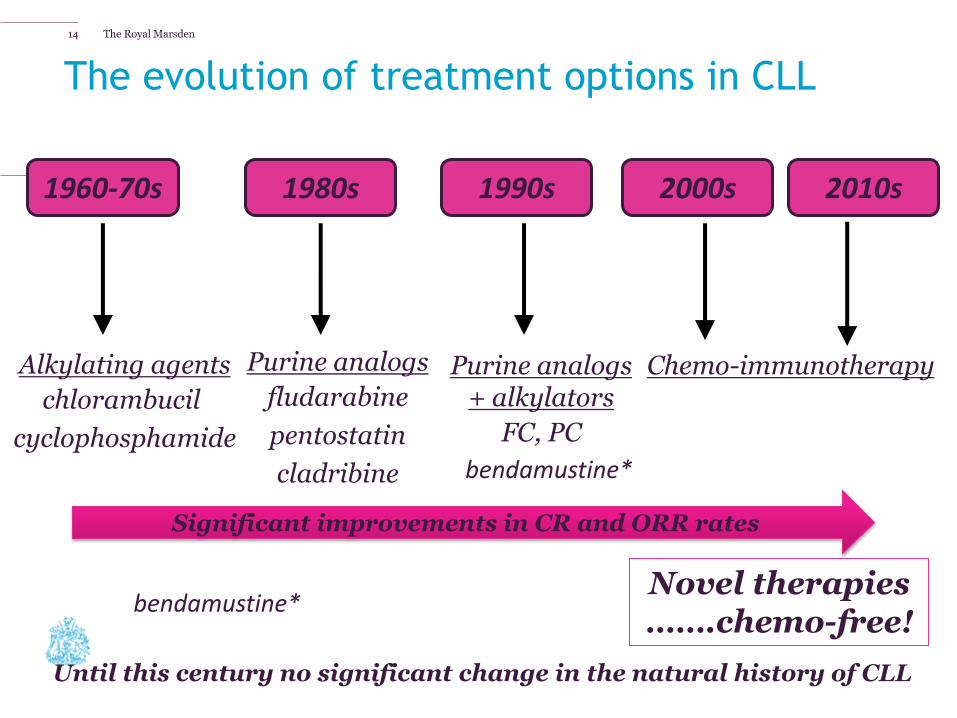
The Royal Marsden
2010s
Chemo-immunotherapy
1980s 1960-70s
Alkylating agents
chlorambucil
cyclophosphamide
1990s
Purine analogs
fludarabine
pentostatin
cladribine
2000s
Purine analogs + alkylators
FC, PC
The evolution of treatment options in CLL
bendamustine* Novel therapies …….chemo-free!
Until this century no significant change in the natural history of CLL
Significant improvements in CR and ORR rates
bendamustine*
14

Tailoring treatment for CLL patients
CIRS, Cumulative Illness Rating Scale Eichhorst et al. Leuk Lymphoma. 2009; 50:171–178.
Many factors must be considered in order to optimise management in patients with CLL
Comorbidities and vital organ
status
Quality of life Supportive
care
Life expectancy
Patient preference
(administration)
What is the personalised goal of treatment?
Toxicity
Medical fitness (CIRS)
Disease evaluation (Stage, prognostic/predictive
markers- TP53)
Age

The Royal Marsden
Tailoring First-line therapy for patients with CLL: what are the challenges ?
16
A. Patient assessment
B. Defining treatment goals
C. Selection of appropriate therapy
D. Improving remissions and survival
E. Improving quality of life
Patie
nt ass
essm
ent
Definin
g treatm
ent goals
Select
ion o
f appro
priate
...
Impro
ving re
miss
ions a
nd...
Impro
ving q
uality
of l
ife
0% 0% 0%
100%
0%

Challenge 1: Patient Assessment
Assessing co-morbidity
Single assessments Combined assessments
Comorbidity scores
Nutrition scores
Comprehensive global assessment
Locomotion scores
Ability scores
Frailty scores
Cognition scores Toxicity scores
17

CLL patients are older and most have some co-
morbidity
75 years
31%
42%
27%
65–74 years
0–64 years
Minor co-morbidity Major co-morbidity
No co-morbidity
46% 43%
11%
Median Age at diagnosis 72 years
18

• All cause mortality increased in co-morbid patients
• However, CLL related deaths major determinant of lower OS
• Maintenance of dose intensity is a problem
• Key issue is being able to deliver safe and effective therapy in this group of patients
Goede V et al. Haematologica. 2014; 99: 1095-1100.
Co-morbidity and outcome
19

The Royal Marsden
• Life expectancy in the UK has improved
• Patients with CLL still have reduced survival compared with the general population
• Good remissions can be achieved with therapy and result in longer survival
• Longer remission is associated with improved quality of life
• Simple palliation/symptom control is not appropriate for most patients with CLL
Lowest
Highest
20.9 years
Challenge 2: Defining Treatment Goals
20

The Royal Marsden
SLOW-GO GO-GO NOT–SO-GO-GO
Hypertension Creatinine
clearance < 50ml
Fitness is more important than age
Challenge 3: Selection of appropriate therapy 21

Median observation time 25.5 months
Med. PFS (6yr FU)* FCR: 57 months* FC: 33 months*
The Go-Go patient
FCR is the ‘gold standard’1
1. Hallek et al. Lancet. 2010; 376: 1164-1174; *Fischer et al. Blood. 2012; 120: 435.
FCR (n=408)
FC (n=409)
Overall survival
Main toxicities-: neutropenia and infection
22

The Royal Marsden
A 65 year old woman who has recently been treated for CLL presents with a dry cough and SOB, chest sounds clear. Do you:
23
A. Send her to A&E
B. Call her specialist team
C. Conclude that this is
likely viral and send her
home
D. Give a course of
antibiotics
Send her t
o A&E
Call her s
pecialis
t team
Conclude th
at this
is lik
el...
Give a co
urse o
f antib
iotic
s
17%
30%
5%
48%

Opportunistic Infections in CLL
• Particularly related to treatment (steroids, purine analogues, alemtuzumab, idelalisib)
• Increased risk in heavily pre-treated patients
• A good response to CLL therapy may reduce infection risk
• Listeria monocytogenes, pneumcystis jerovcii, nocardia, mycobacteria, fungal
• Viral reactivation (herpes, CMV, EBV, Hepatitis B&C)
• Respiratory viruses (Para Flu, RSV)
• PML (JC virus)
PJP Pneumonia
24

Mr AW 65 y man with heavily pretreated fludarabine-refractory CLL treated with CamPred and achieved a good PR. Presented 3 months after completing
treatment with blurred vision in one eye. Otherwise asymptomatic.
Ophthalmology review revealed mass.Biopsy showed aspergillus. MRI revealed small fungal lesion. Treated with voriconazole as OP
and all completely resolved.
25

CLL10 Study: FCR vs BR in front-line
The Not-So-Go-Go patient
Eichhorst et al Lancet Oncology 2016; 17:928-42.
Adverse event FCR (% of pt)
BR (% of pt)
p value
All 90.8 78.5 <0.001
Haematological AEs 90.0 66.9 <0.001
Neutropenia 81.7 56.8 <0.001
Leukocytopenia 79.6 47.8 <0.001
Anemia 12.9 9.7 0.28
Thrombocytopenia 21.5 14.4 0.036
Infection 39.0 25.4 0.001
• Improved PFS with FCR • Less toxicity with BR

The Slow-Go Patient: Adding Targeted treatment CLL11 and Complement 1
• Reflected this group of patients well: • Median age 72 y, • Median CIRS score 8 • 2/3 patients creatinine
clearance < 70 • Both studies confirm that addition
of a CD20 monoclonal antibody improves efficacy- PFS • Chlorambucil: 11-13 m • R-chlorambucil: 16.3m • G-chlorambucil: 31.1m • O-chlorambucil: 22.4m
• Comparable toxicity • MRD neg remissions achieved in a
proportion
R-Chl
G-Chl
O-Chl
Goede et al NEJM 2014, Hillmen Lancet 2015
27

CLL11: Chlorambucil vs G + Clb vs R + Clb Time to next treatment (TTNT)
Goede et al. Blood 2015; 126 (23): Abstr 1733.
Obinutuzumab + Clb prolonged median TTNT by more than one year compared to R-chlorambucil and
by 3 years compared to chlorambucil alone
28

The Royal Marsden
Mr M: DOB 1936
• Referred from prostate team, aged 74y in 2010 with mild lymphocytosis and thrombocytopenia
• Asymptomatic
• Prostate cancer diagnosed 2003, IMRT 2004 hormone treatment until 2006
• No other co-morbidities
• BBC TV documentary producer
29

The Royal Marsden
Mr M: DOB 1936
• No palpable disease • FBC: Hb 141, WBC 10.1 (L 6.7) platelets 131 • Diagnosed Stage A CLL • Watch and wait • 2013 developed DVT and PE following long haul flight,
anticoagulated • Slow steady disease progression- splenomegaly, LN,
falling Hb and platelets • 2014 Wife had acute diagnosis of DLBCL, successfully
treated • Developed mild intra-cerebral bleed following a fall
2015
30

The Royal Marsden
Mr M: DOB 1936
• By Sept 2015 Hb 95, WBC 80, Platelets 57
• Commenced Chlorambucil + obinutuzumab (NICE
approved)
• WBC fell from 80 to 45 after 1st dose and to 1.2
(neutrophils 1) at day 8
• Initial Infusion reaction but no other AEs
• Completed 6 cycles Feb 2016- No palpable disease; Hb
131, WBC 8.3 (N7), platelets 128
• Re-staging investigations (CT and BM) showed CR
31

Challenge 3:Selection of Appropriate Therapy
Patient group Treatment
Fit GO-GO FCR
Intermediate NOT-SO-GO-GO (older age, renal function)
BR
Older less fit SLOW-GO Chlorambucil+ Obinutuzumab Chlorambucil+ ofatumumab
TP53 del/mutation Alemtuzumab+ steroids Idelalisib+ Rituximab Ibrutinib
All patients Available Clinical Trial
32

Challenge 4: Improving Survival
FC vs FCR Chlorambucil alone vs + GA101 or R
Addition of an Anti-CD20 monoclonal antibody to conventional chemotherapy backbone improves survival for GO-GO and SLOW-GO patients
33

Challenge 5: Improving quality of life (QoL)
• Most patients requiring treatment report impaired QoL (fatigue, reduced physical, role and social function)
Else et al. Br J Haematol. 2008; 143: 690-7. Else et al. Leuk Lymphoma. 2012; 53: 1289-98.
34

The Royal Marsden
0%
10%
20%
30%
40%
Month 3 Month 6 Year 1 Year 2 Year 3 Year 4
Assessment period
Pe
rce
nta
ge
im
pro
ve
d
Responders
Non-responders
0%
10%
20%
30%
40%
Year 1 Year 2 Year 3 Year 4
Assessment period
Pe
rce
nta
ge
im
pro
ve
d
Remission
Progressed
• Patients who respond to therapy have improved QoL compared to baseline and compared to those who do not respond
• Patients who remain in remission have better QoL than those who have progressed
• Therefore achieving a remission and remaining in remission is associated with the greatest QoL improvement
Global OoL: Percentage improved by Quality and Duration of Response to Treatment
35

The Royal Marsden
• Most patients are diagnosed on a routine FBC when they are otherwise well
• Some patients will present with lymph node enlargement, but the diagnosis can often be made from PB without need for biopsy
• A significant proportion of patients will never require treatment and others not for years or even decades
• Treatment is carefully tailored and based on numerous personal (age and co-morbidity) and disease-related factors
• Treatment is very effective at achieving durable remissions in the majority of patients, even older less fit individuals, and delivering a good quality of life
• Many new therapies (“just need to stay one drug ahead of your disease” !)
• The major complication of the disease and the therapy is INFECTION
CLL: Conclusions
36



















![Ibrutinib for treating chronic lymphocytic leukaemia [ID749]](https://img.pdfslide.us/doc/110x75/61bd033261276e740b0e7527/ibrutinib-for-treating-chronic-lymphocytic-leukaemia-id749.jpg)