3. INTRODUCTION Lacrimas in latin : a tear Lacrimal gland is
exocrine gland Secretes aqueous component of tear It is located
under the superotemporal orbital rim in a shallow fossa of the
frontal bone. 3/77
4. EMBROYOLOGY Lacrimal gland Starts to develop from multiple
solid ectodermal buds arising from the basal cells of conjunctiva
in the superotemporal region of fornix at 6th-7th weeks Mesenchyme
surrounds these buds and proliferates to form the parenchyma of the
lacrimal gland Buds branch and canalize to form ducts and alveoli
4/77
5. At 5th month of gestation lateral horn of levator
aponeurosis divides it into palpebral and orbital part Lacrimal
glands do not function fully until approximately 6th week of life
Accessory lacrimal glands are formed from ectodermal invagination
of conjunctiva which detected at 6 to 7 months 5/77
6. Lacrimal passages Developed along the line of cleft between
lateral nasal & maxillary process at 32 days 6/77
7. Nasolacrimal duct Maxillary process grows medially to
override paraxial mesoderm of the nasolacrimal process Nasooptic
fissure is thus formed Surface ectoderm within the fissure thickens
in a cord-like fashion 7/77
8. cords of epithelium invaginate at the upper and lower lid
margins, eventually forming the canaliculi. These epithelial cords
fuse to form the nasolacrimal drainage system. 8/77
9. CONGENITAL ABNORMALITIES Dacryostenosis Absence of valves
Congenital fistula of lacrimal sac Punctal agenesis Double puncta
Atresia of canaliculi 9/77
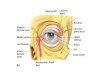
10. Anatomy of lacrimal apparatus Secretory lacrimal apparatus:
Main lacrimal gland Accessory lacrimal gland: glands of Krause
& glands of wolfring. Excretory lacrimal apparatus: Lacrimal
punctum Lacrimal canaliculus Lacrimal sac Nasolacrimal duct
10/77
11. Anatomy of lacrimal apparatus 11/77
12. Main lacrimal gland (Tear gland) SITE- in lacrimal fossa
formed by orbital plate of frontal bone in the anterolateral roof
of orbit SHAPE-almond shaped TYPE-exocrine PART-superior orbital
and inferior palpebral part Separated by lateral horn of
aponeurosis of levator muscle. 12/77
13. Structure of lacrimal gland Branched tubulo-alveolar gland
Similar to salivary gland Microscopically, it has glandular tissue,
stroma & septa. 1)Glandular tissue: consists of acini and ducts
arranged in lobes and lobules. This lobules joins to form
intralobular ducts which finally joins to form extralobular ducts.
13/77
14. 2)Stroma: connective tissue, elastic tissue, lymphoid
tissue, plasma cell, nerve terminals and blood vessels 3)Septa:
fibrovascular in nature and separates lobes and lobules from each
other 14/77
15. Acinar unit (secretory unit) Columnar or pyramidal shaped
secretory cells (luminal surface of the secretory cell has
microvilli) Central lumen Surrounding basal layer of myoepithelial
cells (aid in expulsion of secretion ) 15/77
16. Clinical significance 1. Acute dacryoadenitis Inflammation
of lacrimal gland. Develop as primary inflammation of the gland or
secondary to some local infection as in trauma,
conjuctivitis(especially gonococcal and staphylococcal) and orbital
cellulitis or systemic infection like mumps, infleunza, measles.
Clinical feature: inflammation of palpebral part, painful swelling
in lateral part of upper lid, typical S- shaped curve of lid.
16/77
17. 2. Chronic dacryoadenitis (mikuliczs syndrome) A chronic
enlargement of lacrimal gland secondary to systemic disease and
associated with salivary gland enlargment 17/77
19. Accessory Lacrimal gland Glands of Krause: In the subconj.
tissue near fornices. About 40-42 in upper lid, 6-8 in lower lids.
More numerous laterally. Supply aqueous phase of basal tear film.
Glands of wolfring: Situated near upper border of superior tarsus
plate, 2-5 in upper lid. lower border of inferior tarsus, 2-3 in
lower lid Supply aqueous phase of the basal tear film. 19/77
20. LACRIMAL DUCTS 10-12 lacrimal ducts 2-5from orbital portion
6-8 from palpebral portion The ducts from the orbital portion joins
with the palpebral portion & finally open into the superior
fornix approx.5mm above the lateral tarsus border Clinical
importance: Removal or damage even only to the palpebral portion of
the gland amounts to the excision of the entire gland as far as
secretory function is concerned 20/77
21. Clinical importance Lacrimal ductal cyst(dacryops) Cystic
swelling , which occur due to retention of lacrimal secretion
following blockage of the lacrimal ducts 21/77
22. Blood supply: Supplied by lacrimal artery - ophthalmic
artery internal carotid artery. Sometimes transverse facial artery
& infraorbital artery supplies The lacrimal vein joins to the
superior ophthalmic vein 22/77
23. Lymphatic drainage Lymphatics from the gland passes to the
conjunctival channels hence to the preauricular lymph nodes.
23/77
24. Nerve supply Sensory: from lacrimal nerve ophthalmic branch
of trigeminal nerve(fifth cranial nerve) Symphathetic: from carotid
plexus of cervical symphathetics. Secretomotor: from superior
salivary nucleus. 24/77
26. Lacrimal punctum Small rounded or oval opening. In upper
and lower eyelid at junction of ciliary and lacrimal portion of lid
margin Upper-6mm and lower 6.5mm later to inner canthus On closure
of eyelid punctum do not overlap 26/77
27. Contd Each punctum sits on top of an elevated mound known
as the papilla lacrimalis. They are relatively avascular in
comparison to the surrounding tissue, giving them a pale
appearance, which is accentuated with lateral traction of the lid.
This pallor can be helpful in localizing a stenosed punctum.
27/77
28. Lacrimal canaliculi LENGTH-Each are 8-12mm long
LENGTHCOURSE-2mm vertical&8-10mm horizontal. UNION-90% they
unite as a common canaliculus and in about 10% opens separately in
lateral wall of the orbital sac. VALVE-Valve of Rosenmuller,a
mucosal fold overhangs the junction between common canaliculi and
prevents reflux. 28/77
29. ANGLE- between the vertical and horizontal segments is
approximately 90 degrees, and the canaliculi dilate at the junction
to form the ampulla.. LININGS-by nonkeratinized stratified squamous
epithelium and are surrounded by elastic tissue, which permits
dilation to 2 or 3 times the normal diameter. CLINICAL SIGNIFICANCE
An incompetent valve of rosenmullar is observe clinically as air
escaping From the lacrimal puncta when the indivisual blows his or
her nose 29/77
30. Canaliculitis Inflammation of canalaiculi. Casuative agent:
actinomyces israelii. Presentation: unilateral epiphora with
chronic mocopurulent conjuctivitis. Signs: pouting punctum,
pericanalicular inflammation, mucopurulent discharge on pressure
over the canaliculus. Concretions consisting of sulphur granules
can be expressed. 30/77
31. Oedema and pouting of punctum Expressed concretions with
sulphur granules 31/77
32. LACRIMAL SAC Site lacrimal fossa: (anterior part of medial
orbital part) where sac is encovered by lacrimal fasica (periorbita
i.e periosteum lining of orbit) Length: 15mm Volume : 20cc Parts
:fundus (3-5mm) , body (10-12mm) & neck Lining of double layer
epithelium (upper is columnar and deeper is falter) 32/77
33. Relations Medial to sac separated by periorbita and bone
lie anterior ethmoidal sinuses Below it lies: nasal middle meatus
Lateral to it lies skin ,part of orbicularis oculi, lacrimal fascia
Anteriorly lies the medial palpebral ligament & angular vein
Posterior to sac lies lacrimal fasica & septum orbitale
33/77
34. CLINICAL SIGNIFICANCE Dacryocystitis Inflammation of
lacrimal sac. Acute and chronic form. Usually is secondary to NLD
obstruction. Also congenital which is secondary to NLD blockage.
34/77
35. Acute dacryocystitis Chronic dacryocystitis presentation:
subacute pain, redness and swelling at medial canthus. Sign: very
tender, red, tense swelling,can be associated with mild preseptal
cellulitis, abscess formation , fistula formation. Causative agent:
streptococcus, pneomococcus and staphylococcus.
Presentation:epiphora with mucocele Signs: painless swelling at
inner canthus, mucoid fluid regurgitate on pressing the swelling
area. Causative agent: satphylococci, streptococci, pneumococci
35/77
39. Contd Lower end- opens into the nose through an ostium
under the inferior turbinate, covered by valve of Hasner.
39/77
40. Blood supply and nerve supply to lacrimal passage Superior
and inferior palpebral arteries (ophthalmic artery) and also by
infraorbital artery , angular artery &branch of sphenopalatine
artery Infratrochlear nerve ophthalmic division of trigeminal nerve
and also by anterior superior alvolar nerve 40/77
41. CLINICAL IMPORTANCE CNLDO (Congenital nasolacrimal duct
obstruction)-failure of the canalization of the NLD after birth In
fetus, the NLD is a solid cord of cells, which gets canalized at
birth. In 30% of new borns canalization is delayed. This congenital
NLD blockage causes epiphora predisposing to congenital
dacryocystitis. PANDO (primary acquired nasolacrimal duct
obstruction)-an entity of nasolacrimal duct obstruction caused by
inflammation or fibrosis without any precipitating cause.. studies
have revealed inflammation, vascular congestion, and edema of the
nasolacrimal duct in the early phases and, ultimately, fibrosis
with complete occlusion of the nasolacrimal duct's lumen in the
late phases. 41/77
42. SALDO(secondary acquired lacrimal drainage obstruction) has
some etiology : infectious Bacteria such as Actinomyces
Fusobacterium Bacteroides Mycobacterium Chlamydia 42/77
43. Congenital nasolacrimal duct obstruction Epiphora and
matting Infrequently acute dacryocystitis Massage of nasolacrimal
duct and antibiotic drops 4 times daily Improvement by age 12
months in 95% of cases If no improvement - probe at 12-18 months
Results - 90% cure by first probing and 6% by second Treatment
43/77
44. Remnants of epithelium within the cords form inconsistent
valve like folds which are diagrammatically represented . 1, valve
of RosenMuller 2, valve of Krause 3, spiral valve of Hyrtl 4, valve
of Taillefer 5, valve of Hasner or plica lacrimalis. 44/77
45. Physiology of lacrimal appartus 45/77
46. Secretion of tears Continously secreted through out the day
by main &accessory lacrimal gland Rate of tear production
-1.2microl/min tear vol.-7 micro lit 2 Components: Basic Secretors
Reflex Secretors 46/77
47. Basic Secretors mucin secreting goblet cell of conjunctiva
Accessory lacrimal gland of krause & Wolfring tarsal gland
Gland of Zeiss & Moll 47/77
48. Reflex secretion due to irritation of 5th cranial nerve in
response to sensation from cornea and conjunctiva.(mainly by
lacrimal gland) 48/77
49. Tears Lost Absorbtion from conjunctiva Evaporation Size of
palpebral aperture Blink rate Ambient temperature and humidity
Nasolacrimal drainage Any obstruction on pathway 49/77
50. Lacrimal pump mechanism The secreted tear flows over the
ocular surface and reaches marginal tear strip running along the
ciliary margin of each eyelids and collects as lacrimal lacus in
inner canthus. From there it is drained to nasal cavity via
lacrimal excretory system by active lacrimal pump mechanism.
50/77
51. Working of lacrimal pump mechanism Operates with the
blinking movements. Performed by orbicularis muscle of eyelid. Two
major events Eyelid closure eyelid open 51/77
52. On eyelid closure following events occur concomitantly
Contraction of pretarsal fibres of orbicularis compress the ampulla
and shortens the canaliculi. This movement propels the tear fluid
present in the ampulla and horizontal part of canaliculi toward the
lacrimal sac Contraction of preseptal fibres pulls the lacrimal
fascia and lateral wall of the sac laterally thus opening the
normally closed lacrimal sac. This produces negative pressure and
draws the tear from canaliculi to lacrimal sac. At the same time
inferior portion closes more tightly thus preventing aspiration of
air from nose. 52/77
53. On eyelid opening following events occur concomitantly
Relaxation of pretarsal fibres allows canaliculi to expand and
reopen. This draws the tearfluid through the punctum from the
lacrimal lake. Relaxation of preseptal fibres allows the lacrimal
sac to collapse which inturn expels the fluid downard into open
NLD. At the same time puncta moves laterally, canaliculi lengthens
and is filled with tears. 53/77
54. 54/77
55. Drainage into the nasal cavity Gravity Air current movement
within the nose Final entry of tears into the nose :facilitated by
opening of Valve of Hasner which widens synchronously with opening
of lids 55/77
56. Tear film It consist of three layars 1. Mucous layer:
subconjunctival goblet cells 2. Aqueous layer: main and accessory
lacrimal glands 3. Lipid layer :Meibomian gland Gland of Zeis and
Moll 56/77
57. Lipid layer Outermost layer Secreted by meibomian gland,
zeiss and moll gland Thickness-0.1micrometre Consist of polar and
nonpolar lipid This layer prevents the overflow of tear and also
evaporation of tear 57/77
58. Aqueous layer Middle layer. Secreted by lacrimal gland and
accessory gland of krause. Thickness: 6.5-7.5 micrometre.
Constitute main bulk of tear. Consist of inorganic salts, glucose,
urea, and various biopolymers like proteins(Ig A), antibacterial
agent( lysozyme, lactoferrin). This layer serves to provide
atmospheric oxygen to epithelium,washes away debris and noxious
agent, maintain the normal level of electrolyte over occular
surface epithelium. 58/77
59. Mucin layer Innermost layer Secreted by conjuctival goblet
cells This layer makes the hydrophobic corneal surface hydrophilic
overwhich the aqueous and lipid layer get adheres. Thus plays a
vital role in stability of tear film Act as lubricant during eye
movement 59/77
60. Tear film abnormalities Dry Eye It is the state of abnormal
tear film that can be caused by number conditions which alter its
composition and affect stability. Normal tear Tear in dry eye
60/77
61. Tear film abnormalities classification on the basis of
physiological consideration: (holly and lemp ) Aqueous deficiency
Mucin deficiency Lipid abnormality Impaired lid function
epitheliopathy 61/77
62. Tests for tear film adequacy Schirmer test: assess aqueous
tear production. Performed with whatmann 41 filter paper. Two type:
Schirmer I: without anesthesia Normal lower limit is 10mm of
wetting after 5min Schirmer II: use of anesthesia Normal lower
limit is 6mm after 5min 62/77
63. Tear film break-up time Indicate adequacy of mucin
component of tear It is the time interval between complete blink
and appearance of first randomly distributed dry spot on cornea.
Done by instillation of fluorescein drop 2% or impregnated
fluoresceinstrip. Examined under cobalt blue light of slit lamp.
TBUT value less than 10 sec is said to be dry eye. 63/77
64. Clinical correlation of lacrimal apparatus Watering eye
Implies overflow of the tears from conjuctival sac Occur due to :
Excessive secretion of tears(hyperlacrimation) Obstruction of
lacrimal passage 64/77
65. Clinical evaluation of watering eye 1. External Ocular
examination with slit lamp: Ectropion entropion Punctal obstruction
by an eyelash Large carauncle displacing punctum away from globe
Pouting punctum Any occular FB 65/77
66. 2.Regurgitation test A steady pressure with index finger
over lacrimal sac area is applied. Punctal reflux of mucopurulent
material on compression indicates patent canalicular system with
obstruction at lacrimal sac or NLD 66/77
67. 3. Fluorescein dye disappearance test(FDDT) Performed with
instillation of 2% fluorescein dye in both conjuctival fornices.
Observations made after 2 min. No dye is seen in conjuctival
sac-patent passage Retention of dye inadequate drainage due to
atonia of sac or mechanical obstruction. 67/77
68. 4. Lacrimal syringing test Local anesthetic(4% xylocaine)
is instilled Punctum is dilated if narrow Gently curved, blunt
tipped lacrimal cannula on a 2mm saline filled syringe is inserted
into lower puncta and advanced few mm following the contour of the
cannulus prior to irrigation 68/77
69. Then after, normal saline is pushed into lacrimal sac . The
following conditions are obtained: 1. Free passage of saline
indicate patency of lacrimal passage. 2. Clear fluid from same
puncta indicate same pucta block. 3. Clear fluid from opposite
puncta indicate common camnalicular block. 4. Mucoid fluid from
opposite puncta indicate NLD block. 69/77
70. Probe test The hard stop and soft stop is encountered Hard
stop indicates the patency of lacrimal canaliculi Occurs when
cannula enters the lacrimal sac but comes to stop at the medial
wall of sac Soft stop indicates the non-patency of canaliculi
Occurs when cannula donot enter lacrimal sac and presses the soft
tissue of common canaliculus 70/77
71. 71/77
72. 5. Jones dye testing Performed in patients with suspected
partial obstruction of the drainage system. Type: John testI:
differentiate between watering due to partial obstruction and
hypersecretion of tear. John test II: identifies probable site of
partial obstruction. Done after John I. Two drops of 2% fluorescein
dye is instilled in conjuctival sac and a cotton bud dipped in 1%
xylocaine is placed in inferior meatus after 5 min. John test I:
Positive: fluorescien is recovered from the nose indicating patency
of drainage system. Watering is due to primary hypersecretion.
Negative: no dye is recovered indicating a partial obstruction. In
this case John II is recommended. 72/77
73. John test II: Cotton bud is placed in inferior meatus and
syringing is performed after application of anesthetic. Positive:
fluorescein stained saline is recovered from nose. Here fluorescein
has entered in sac thus conforming patency of upper lacrimal
passage. Negative: unstained saline is recovered from the nose. It
indicates no entry of dye in lacrimal sac and implies partial
obstruction of puncta, canaliculi or common canaliculus. 73/77
74. Introduction to obstruction of lacrimal passage Punctal
obstruction: Primary punctal stenosis: caused in absence of punctal
eversion e.g due to chronic blepharitis, herpes simplex, herpes
zooster, cicatrizing conjuctivitis, trachoma etc Secondary punctal
obstruction: caused by punctal eversion. 74/77
75. Canalicular obstruction: Occurs due to congenital trauma,
herpes simplex infection, drugs and chronic dacryocystitis.
Nasolacrimal duct obstruction: Congenital,idioapthic, naso- orbital
trauma,granulomatous disease like sarcoidosis,infiltration by
nasophyrangeal tumors. Dacryoliathiasis: lacrimal stone in any part
of lacrimal system. 75/77