Embed Size (px)
Citation preview

The Case for Child Development as a Determinant of HealthAuthor(s): Clyde HertzmanSource: Canadian Journal of Public Health / Revue Canadienne de Sante'e Publique, Vol. 89,SUPPLEMENT 1: SELECTED PAPERS FROM What on Earth? A National Symposium onEnvironmental Contaminants and the Implications for Child Health (MAY / JUNE 1998), pp.S14-S19Published by: Canadian Public Health AssociationStable URL: http://www.jstor.org/stable/41992862 .
Accessed: 17/06/2014 00:17
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
Canadian Public Health Association is collaborating with JSTOR to digitize, preserve and extend access toCanadian Journal of Public Health / Revue Canadienne de Sante'e Publique.
http://www.jstor.org
This content downloaded from 195.34.79.79 on Tue, 17 Jun 2014 00:17:33 AMAll use subject to JSTOR Terms and Conditions
The Case for Child Development
as a Determinant of Health
Clyde Hertzman, MD, MSc, FRCPC
ABSTRACT
The complex relationship between life course and social/economic-psychosocial conditions in a given society has a powerful determining effect on human health. The socioeconomic gradient emerges from a com- plex mixture of psychosocial and material influences operating at various levels of social aggregation and, also, a series of biological responses whose character and significance vary over the life course. Biological embed- ding and the "latency" and "pathways" model incorporate the notion of a critical period in development; the pathways model emphasizes the cumulative effect of life events and the ongoing importance of social/ economic-psychosocial conditions throughout the life cycle. The models, although conceptually complementary, result in ideological conflict and lend themselves to different policy directions.
Health status differs markedly among individuals within a given population. Yet, it does not necessarily follow that the fac- tors which determine the health status of large populations are the same as the fac- tors which operate at the individual level. In recent years we have come to under- stand how the health of the population as a whole is influenced by social/economic conditions and the "psychosocial" environ- ment on the one hand (termed SEP condi- tions here), and by experiences during sen- sitive periods early in human development, on the other. The complex relationship between the unfolding life course and SEP conditions in a given society turns out to have a powerful determining effect on human health.
Emergence of the "flat of the health- wealth curve"
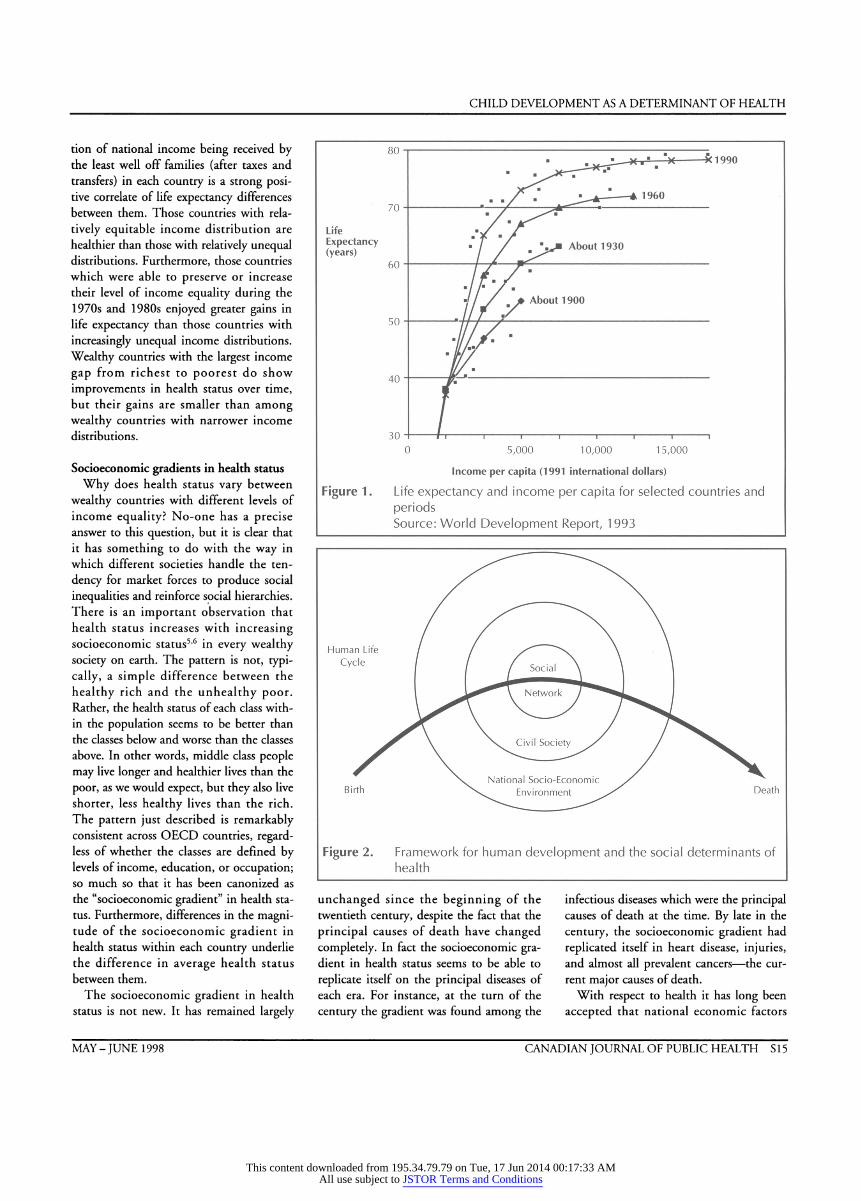
The role of SEP conditions is highlight- ed by the relationship between health and wealth in different countries over time. In general terms, international differences in per capita income (a measure of wealth) appear to be closely and positively related to the length and the healthfiilness of life. Early in this century the relationship was simple: life expectancy was greater in coun- tries with higher per capita incomes. Figure 1 shows that the longest lived and richest country had a life expectancy of approxi- mately 54 years.1 However, in recent decades the relationship between health and wealth has become more complex as rich nations have grown increasingly rich.
The health-wealth curves for 1930 and I960 are similar to 1900, but, as average
Professor, Department of Health Care and Epidemiology, Faculty of Medicine, James Mather Building, 5804 Fairview Avenue, Vancouver, BC, V6T 1Z3, Tel: 604-822-3002, Fax: 604-822-4994, E-mail: [email protected]
life expectancies and national incomes increased over the century, the simple rela- tionship between health and wealth broke down among the high income countries. By 1990, the world's richest nations had achieved levels of national wealth unprece- dented in history. At the same time, a dis- tinct 'flat of the health-wealth curve' had emerged, such that increasing income among those countries with per capita incomes greater than $10,000 US was no longer associated with further increases in life expectancy.1 Yet, the traditional monotonie relationship between health and wealth persisted among the world's poorer countries.
Why does the health-wealth curve flat- ten at the wealthy end? A closer look at the trends helps to answer this question. Among the Organization for Economic Co-operation and Development (OECD) countries, which make up virtually all of the countries on the flat of the curve, increases in per capita income from 1970 to 1990 did not correlate with increases in life expectancy. In other words, not only has the "one point in time" relationship between health and wealth broken down among wealthy countries, but the time sequence of increasing health accompany- ing increasing wealth over time has broken down, too. This does not mean, however, that all the world's wealthy countries have similar health status to one another. In fact, there are large variations in health sta- tus among them and, also, there are large differences in the rate of increase in health status over time.
Why does health status differ among wealthy countries? Useful insights into this question come from investigators who have scrutinized health and income distribution in wealthy societies2'3 and between U.S. states.4 They have shown that the propor-
S 14 CANADIAN JOURNAL OF PUBLIC HEALTH VOLUME 89, SUPPLEMENT 1
This content downloaded from 195.34.79.79 on Tue, 17 Jun 2014 00:17:33 AMAll use subject to JSTOR Terms and Conditions
CHILD DEVELOPMENT AS A DETERMINANT OF HEALTH
tion of national income being received by the least well off families (after taxes and transfers) in each country is a strong posi- tive correlate of life expectancy differences between them. Those countries with rela- tively equitable income distribution are healthier than those with relatively unequal distributions. Furthermore, those countries which were able to preserve or increase their level of income equality during the 1970s and 1980s enjoyed greater gains in life expectancy than those countries with increasingly unequal income distributions. Wealthy countries with the largest income gap from richest to poorest do show improvements in health status over time, but their gains are smaller than among wealthy countries with narrower income distributions.
Socioeconomic gradients in health status Why does health status vary between
wealthy countries with different levels of income equality? No-one has a precise answer to this question, but it is clear that it has something to do with the way in which different societies handle the ten- dency for market forces to produce social inequalities and reinforce social hierarchies. There is an important observation that health status increases with increasing socioeconomic status5'6 in every wealthy society on earth. The pattern is not, typi- cally, a simple difference between the healthy rich and the unhealthy poor. Rather, the health status of each class with- in the population seems to be better than the classes below and worse than the classes above. In other words, middle class people may live longer and healthier lives than the poor, as we would expect, but they also live shorter, less healthy lives than the rich. The pattern just described is remarkably consistent across OECD countries, regard- less of whether the classes are defined by levels of income, education, or occupation; so much so that it has been canonized as the "socioeconomic gradient" in health sta- tus. Furthermore, differences in the magni- tude of the socioeconomic gradient in health status within each country underlie the difference in average health status between them.
The socioeconomic gradient in health status is not new. It has remained largely
Figure 1. Life expectancy and income per capita for selected countries and periods Source: World Development Report, 1993
Figure 2. Framework for human development and the social determinants of health
unchanged since the beginning of the twentieth century, despite the fact that the principal causes of death have changed completely. In fact the socioeconomic gra- dient in health status seems to be able to replicate itself on the principal diseases of each era. For instance, at the turn of the century the gradient was found among the
infectious diseases which were the principal causes of death at the time. By late in the century, the socioeconomic gradient had replicated itself in heart disease, injuries, and almost all prevalent cancers - the cur- rent major causes of death.
With respect to health it has long been accepted that national economic factors
MAY - JUNE 1 998 CANADIAN JOURNAL OF PUBLIC HEALTH S 1 5
This content downloaded from 195.34.79.79 on Tue, 17 Jun 2014 00:17:33 AMAll use subject to JSTOR Terms and Conditions

CHILD DEVELOPMENT AS A DETERMINANT OF HEALTH
mattered, and the question has always been, how much? But the belief was that eco- nomic factors operated through the con- sumption of items affecting health, such as food, housing, and medical care. The debate seemed to end with the notion that, beyond a certain level of individual income necessary to buy healthful goods and ser- vices, no more health gains could be expected from increasing prosperity. It is now clear that there is much more at stake, and that the socioeconomic effect is not confined to those too poor to buy health- enhancing goods. Rather, the socioeconom- ic gradient emerges from a complex mix- ture of psychosocial and material influences operating at various levels of social aggrega- tion and, also, a series of biological respons- es whose character and significance varies from stage to stage over the life course.
A model of these relationships is present- ed in Figure 2, which represents the indi- vidual life course as an arrow piercing a bull's eye, which represents society. Society is shown to have three classes of factors (the three concentric circles) which repre- sent determinants of health and well-being at three levels of social aggregation. At the most intimate level are the factors associat- ed with social support. At the next level out are the factors at the level of the civil society which can buffer or exacerbate the stresses of daily living. Finally, at the broadest level of aggregation are state fac- tors: in particular, national wealth, income distribution, and the structure of opportu- nity created by history, geography, and for- tune, which support or undermine health and well-being.
The picture which emerges is of a life- long interaction between the coping skills and capabilities of the developing individual and SEP conditions as they present them- selves at the intimate, civic, and state level. The dimension of human development emerges as one of the principal compo- nents of the SEP conditions which deter- mine health throughout the life cycle.
Biologic embedding, latency and pathways Spending one's early years in an unstim-
ulating, emotionally and physically unsup- portive environment will affect brain development in adverse ways, and lead to cognitive and socioemotional delays. The
problems that children so affected will dis- play early in school will lead them to expe- rience much more acute and chronic stress than others, which will have both physio- logic and life course consequences. Because the central nervous system, which is the centre of human consciousness, "talks to" the immune, hormone, and clotting sys- tems, systematic differences in the experi- ence of life will increase or decrease levels of resistance to disease. This will change the long-term function of vital organs of the body and lead to socioeconomic differ- entials in morbidity and mortality. This process, whereby human experience affects the healthfulness of life across the life cycle, is called "biological embedding."7
Insights into biological embedding come from a variety of sources, including pri- mate studies, studies of critical periods in brain development, and the emergent fields of psychoneuroimmunology and psy- choneuroendocrinology. For instance, the observation that the neurological system can talk to the immune and endocrine sys- tems supports the notion that the condi- tions of life, filtered through a perceptual screen, could affect the length and health- fulness of life through a wide variety of biological pathways. From the perspective of modern medicine this is more than just a little bit counterintuitive, because it chal- lenges the importance of tackling health problems on a disease-by-disease basis.
Consider dementia of the Alzheimer's type (DAT) as an example of how the pop- ulation health perspective can transform our view of an "organic" condition. The example relates to the role of education in early life and the development of DAT in late life. When it first emerged that better- educated people scored better on the screening mental status exam for DAT, the response of biomedical traditionalists was to presume that people who are better edu- cated are better test- takers, and can 'fool' screening tests.8 If one did a full Alzheimer's diagnosis, they argued, this pattern of lower risk among the better edu- cated would disappear. This objection has since been put to rest. The Canadian Study of Health and Aging showed that there was a fourfold increase of risk for "fully diagnosed" DAT from most to least educated.9 Other studies have produced
consistent results.10"12 In addition, several longitudinal studies have shown that late in life mental status declines faster among those with lower levels of education than among those with higher levels of educa- tion.13
Learning and memory depend upon connections between nerve cells in various parts of the brain. Dementia involves the loss and disorganization of these connec- tions. Education likely enriches the net- work of interconnections, creating reserve capacity which can compensate for the inevitable losses which occur with aging, and postpone the onset of dementia. What is begged by observations like this is an understanding of how differing SEP condi- tions, unfolding over time, initiate and sus- tain processes which lead to differing levels of health, well-being, and competence across the life cycle. A developmental per- spective which begins at the very beginning of life would seem indispensible here. In practise, this means paying particularly close attention to insights gleaned from longitudinal studies, especially those which begin at birth and follow large population samples for decades into the future.
Two different, and sometimes conflict- ing, explanatory models emerge of the impact of childhood experiences in later life. The first, called the "latency" model, emphasizes the prospect that SEP condi- tions very early in life will have a strong effect later in life, independent of interven- ing experience. The second, called the "pathways" model, emphasizes the cumula- tive effect of life events and the ongoing importance of SEP conditions throughout the life cycle. The empirical relationship between latent effects, pathway effects, cumulating risk, and a putative "outcome" (arbitrarily ocurring at age 35) are present- ed graphically in Figure 3.
Latency Model The essence of the latency model can be
illustrated with an example from animal research. A series of studies has been car- ried out which examined the lifelong impact of "handling" newborn rats.14 Handling involves removing the mother from the litter, placing individual pups into a new cage for 15 minutes, then returning both mother and pups to their
S 16 CANADIAN JOURNAL OF PUBLIC HEALTH VOLUME 89, SUPPLEMENT 1
This content downloaded from 195.34.79.79 on Tue, 17 Jun 2014 00:17:33 AMAll use subject to JSTOR Terms and Conditions
CHILD DEVELOPMENT AS A DETERMINANT OF HEALTH
cage. This is done once per day for the first three weeks of life. When compared to nonhandled pups, this simple intervention improved the function of the "stress sys- tem" throughout the life course. The total lifetime exposure to "corticosterone" is lowered, which is toxic to nerve cells in a brain structure known as the "hippocam- pus." Cognitive functions are sensitive to relatively small degrees of hippocampal damage, so that by 24 months of age (elderly by rat standards), the handled rats had been spared some of the cognitive deterioration typical of aging. The signifi- cance of this was demonstrated by experi- ments which showed that nonhandled rats' ability to learn declined with age, whereas no deterioration occurred in aged handled rats. Most relevant in this context is the final observation: the protective effect on learning could not be induced by carrying out the handling manoevre at a later age.14
This example clearly illustrates the notion of a critical period in development. Its essence is an opportunity to develop a competence which occurs at a discrete and unique time in (early) life and has a life- long impact on well-being, independent of intervening experience. For instance, the risk of death from heart disease in the fifth decade of life is strongly associated with the size of an individual's placenta at birth and weight gain during the first year of life.15"23 Certain early childhood stimula- tion programs have been effective in improving the life trajectories of disadvan- taged children,24,25 even without any attempt to provide them with ongoing support. The common theme here is the notion of a discrete time, early in life, when the right things must happen, or else it is 'all over.'
Pathways Model The hypothesis underlying the pathways
model is that, over time, less than optimal development, chronic stress and its physio- logic impacts, a sense of powerlessn ess and alienation, and a dysfunctional social sup- port network will create a vicious cycle with short-term implications for educa- tional attainment, criminality, drug use, and teen pregnancy; and long-term impli- cations for the quality of working life, social support, chronic disease in mid life,
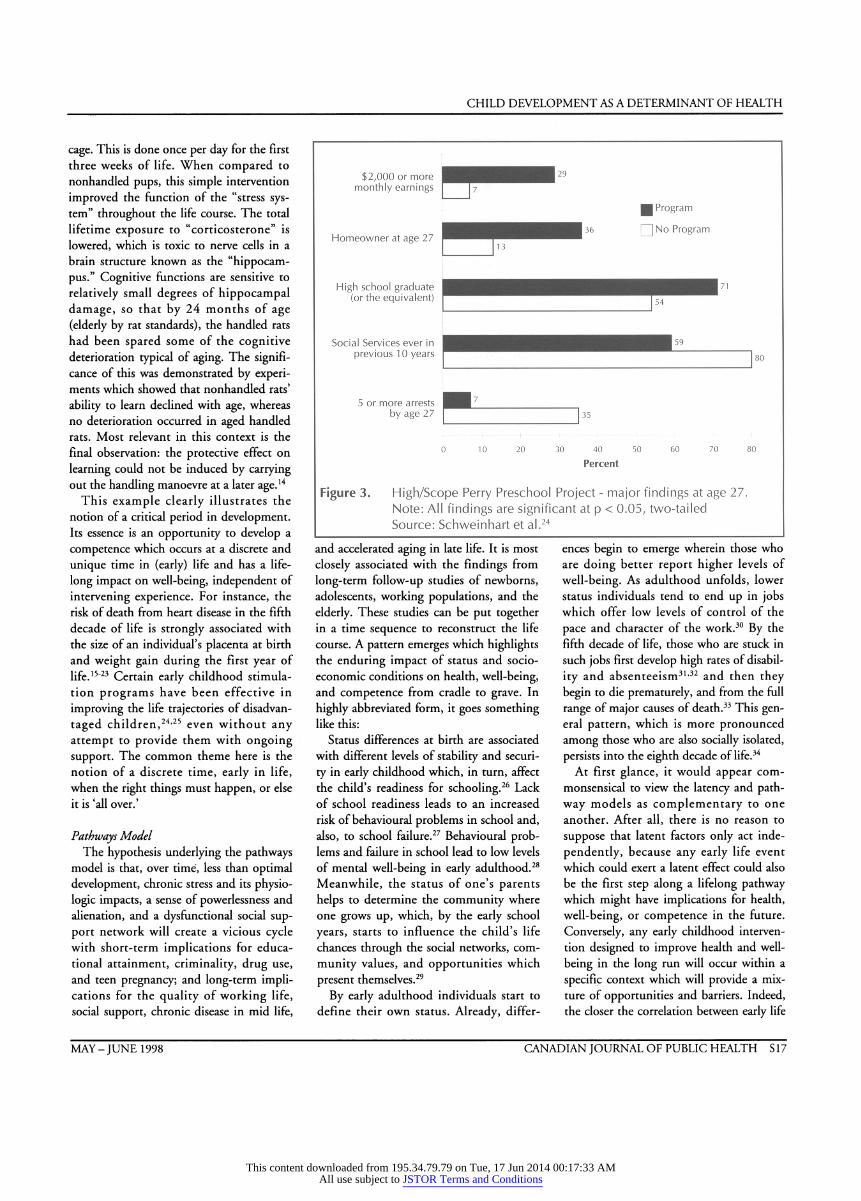
Figure 3. High/Scope Perry Preschool Project - major findings at age 27. Note: All findings are significant at p < 0.05, two-tailed Source: Schweinhart et al.24
and accelerated aging in late lite. It is most closely associated with the findings from long-term follow-up studies of newborns, adolescents, working populations, and the elderly. These studies can be put together in a time sequence to reconstruct the life course. A pattern emerges which highlights the enduring impact of status and socio- economic conditions on health, well-being, and competence from cradle to grave. In highly abbreviated form, it goes something like this:
Status differences at birth are associated with different levels of stability and securi- ty in early childhood which, in turn, affect the child's readiness for schooling.26 Lack of school readiness leads to an increased risk of behavioural problems in school and, also, to school failure.27 Behavioural prob- lems and failure in school lead to low levels of mental well-being in early adulthood.28 Meanwhile, the status of one's parents helps to determine the community where one grows up, which, by the early school years, starts to influence the child's life chances through the social networks, com- munity values, and opportunities which present themselves.29
By early adulthood individuals start to define their own status. Already, differ-
ences begin to emerge wherein those who are doing better report higher levels of well-being. As adulthood unfolds, lower status individuals tend to end up in jobs which offer low levels of control of the pace and character of the work.30 By the fifth decade of life, those who are stuck in such jobs first develop high rates of disabil- ity and absenteeism31,32 and then they begin to die prematurely, and from the full range of major causes of death.33 This gen- eral pattern, which is more pronounced among those who are also socially isolated, persists into the eighth decade of life.34
At first glance, it would appear com- monsensical to view the latency and path- way models as complementary to one another. After all, there is no reason to suppose that latent factors only act inde- pendently, because any early life event which could exert a latent effect could also be the first step along a lifelong pathway which might have implications for health, well-being, or competence in the future. Conversely, any early childhood interven- tion designed to improve health and well- being in the long run will occur within a specific context which will provide a mix- ture of opportunities and barriers. Indeed, the closer the correlation between early life
MAY- JUNE 1998 CANADIAN JOURNAL OF PUBLIC HEALTH S 17
This content downloaded from 195.34.79.79 on Tue, 17 Jun 2014 00:17:33 AMAll use subject to JSTOR Terms and Conditions
CHILD DEVELOPMENT AS A DETERMINANT OF HEALTH
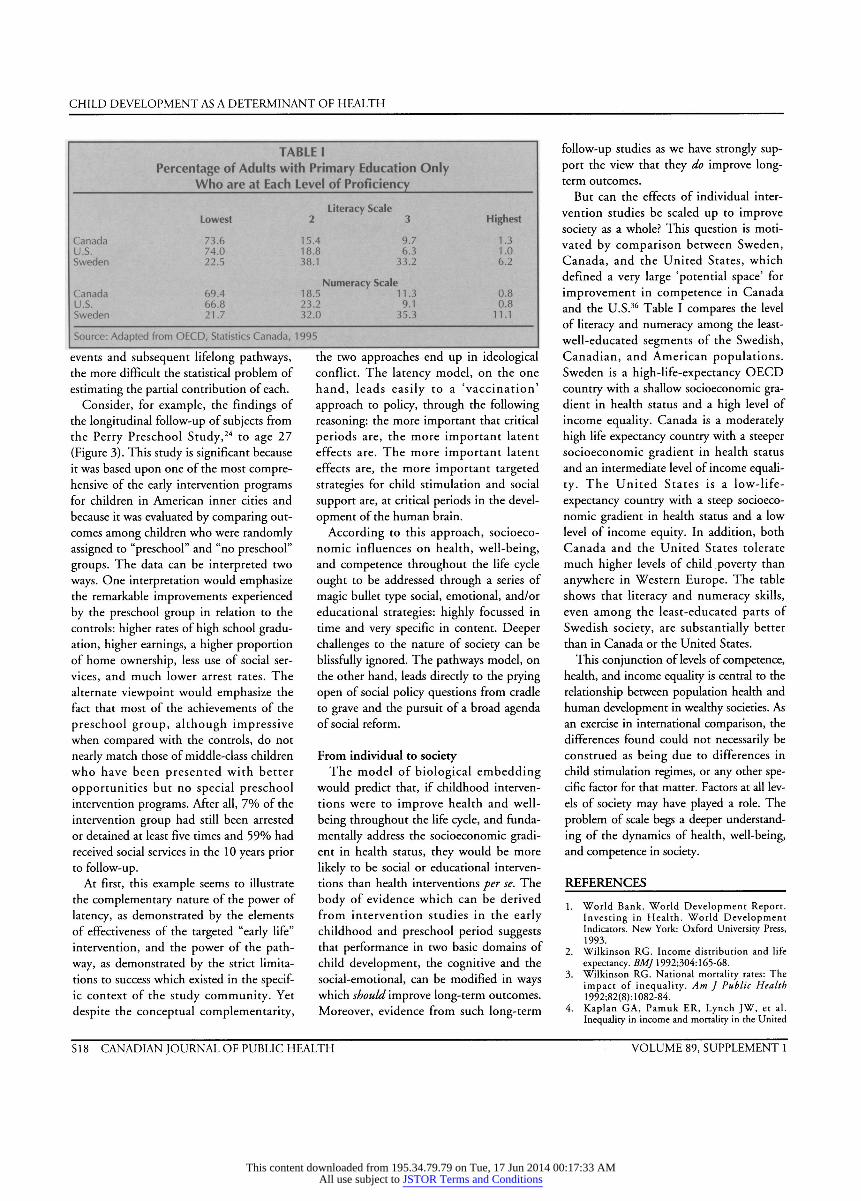
TABLE I Percentage of Adults with Primary Education Only
Who are at Each Level of Proficiency
Literacy Scale Lowest 2 3 Highest
Canada 73.6 15.4 9.7 1.3 U.S. 74.0 18.8 6.3 1.0 Sweden 22.5 38.1 33.2 6.2
Numeracy Scale Canada 69.4 18.5 11.3 0.8 U.S. 66.8 23.2 9.1 0.8 Sweden 21.7 32.0 35.3 11.1
Source: Adapted from OECD, Statistics Canada, 1995
events and subsequent lifelong pathways, the more difficult the statistical problem of estimating the partial contribution of each.
Consider, for example, the findings of the longitudinal follow-up of subjects from the Perry Preschool Study,24 to age 27 (Figure 3). This study is significant because it was based upon one of the most compre- hensive of the early intervention programs for children in American inner cities and because it was evaluated by comparing out- comes among children who were randomly assigned to "preschool" and "no preschool" groups. The data can be interpreted two ways. One interpretation would emphasize the remarkable improvements experienced by the preschool group in relation to the controls: higher rates of high school gradu- ation, higher earnings, a higher proportion of home ownership, less use of social ser- vices, and much lower arrest rates. The alternate viewpoint would emphasize the fact that most of the achievements of the preschool group, although impressive when compared with the controls, do not nearly match those of middle-class children who have been presented with better opportunities but no special preschool intervention programs. After all, 7% of the intervention group had still been arrested or detained at least five times and 59% had received social services in the 1 0 years prior to follow-up.
At first, this example seems to illustrate the complementary nature of the power of latency, as demonstrated by the elements of effectiveness of the targeted "early life" intervention, and the power of the path- way, as demonstrated by the strict limita- tions to success which existed in the specif- ic context of the study community. Yet despite the conceptual complementarity,
the two approaches end up in ideological conflict. The latency model, on the one hand, leads easily to a 'vaccination' approach to policy, through the following reasoning: the more important that critical periods are, the more important latent effects are. The more important latent effects are, the more important targeted strategies for child stimulation and social support are, at critical periods in the devel- opment of the human brain.
According to this approach, socioeco- nomic influences on health, well-being, and competence throughout the life cycle ought to be addressed through a series of magic bullet type social, emotional, and/or educational strategies: highly focussed in time and very specific in content. Deeper challenges to the nature of society can be blissfully ignored. The pathways model, on the other hand, leads directly to the prying open of social policy questions from cradle to grave and the pursuit of a broad agenda of social reform.
From individual to society The model of biological embedding
would predict that, if childhood interven- tions were to improve health and well- being throughout the life cycle, and funda- mentally address the socioeconomic gradi- ent in health status, they would be more likely to be social or educational interven- tions than health interventions per se. The body of evidence which can be derived from intervention studies in the early childhood and preschool period suggests that performance in two basic domains of child development, the cognitive and the social-emotional, can be modified in ways which should improve long-term outcomes. Moreover, evidence from such long-term
follow-up studies as we have strongly sup- port the view that they do improve long- term outcomes.
But can the effects of individual inter- vention studies be scaled up to improve society as a whole? This question is moti- vated by comparison between Sweden, Canada, and the United States, which defined a very large 'potential space' for improvement in competence in Canada and the U.S.36 Table I compares the level of literacy and numeracy among the least- well-educated segments of the Swedish, Canadian, and American populations. Sweden is a high-life-expectancy OECD country with a shallow socioeconomic gra- dient in health status and a high level of income equality. Canada is a moderately high life expectancy country with a steeper socioeconomic gradient in health status and an intermediate level of income equali- ty. The United States is a low-life- expectancy country with a steep socioeco- nomic gradient in health status and a low level of income equity. In addition, both Canada and the United States tolerate much higher levels of child poverty than anywhere in Western Europe. The table shows that literacy and numeracy skills, even among the least-educated parts of Swedish society, are substantially better than in Canada or the United States.
This conjunction of levels of competence, health, and income equality is central to the relationship between population health and human development in wealthy societies. As an exercise in international comparison, the differences found could not necessarily be construed as being due to differences in child stimulation regimes, or any other spe- cific factor for that matter. Factors at all lev- els of society may have played a role. The problem of scale begs a deeper understand- ing of the dynamics of health, well-being, and competence in society.
REFERENCES 1. World Bank. World Development Report.
Investing in Health. World Development Indicators. New York: Oxford University Press, 1993.
2. Wilkinson RG. Income distribution and life expectancy. BMJ 1992;304:165-68.
3. Wilkinson RG. National mortality rates: The impact of inequality. Am J Public Health 1992;82(8): 1082-84.
4. Kaplan GA, Pamuk ER, Lynch JW, et al. Inequality in income and mortality in the United
S 1 8 CANADIAN JOURNAL OF PUBLIC HEALTH VOLUME 89, SUPPLEMENT 1
This content downloaded from 195.34.79.79 on Tue, 17 Jun 2014 00:17:33 AMAll use subject to JSTOR Terms and Conditions
CHILD DEVELOPMENT AS A DETERMINANT OF HEALTH
States: Analysis of mortality and potential path- ways. BMJ 1996;312:999-1003.
5. Kunst AE, Mackenbach JP. An International Comparison of Socio-economic Inequalities in Mortality. Rotterdam: Erasmus University, 1992.
6. Kunst AE, Guerts JJM, Berg J. Internation Variation in Socio-economic Inequalities in Self- reported Health. The Hague: Netherlands Central Bureau of Statistics, 1992.
7. Hertzman C, Wiens M. Child development and long-term outcomes: A population health per- spective and summary of successful interventions. Soc Sei Med 1996;43(7): 1083-95.
8. Kittner SJ, White LR, Farmer ME, et al. Methodological issues in screening for dementia: The problem of education adjustment. J Chron Dis 1986;39(3): 163-70.
9. D'Arcy C. Education and socio-economic status as risk factors for dementia: Data from the Canadian Study of Health and Aging. Neurobiology of Aging 1994; 14: S40.
10. Fratiglioni L, Jorm AF, Grut M, et al. Predicting dementia from the mini-mental state examina- tion in an elderly population: The role of educa- tion. J Clin Epidemiol 1993;46(3):28 1-87.
11. Stern Y, Gurland B, Tatemichi TK, et al. Influence of education and occupation on the incidence of Alzheimer's disease. JAMA 1994;271:1004-10.
12. Mortimer JA, Graves AB. Education and other socioeconomic determinants of dementia and Alzheimer's disease. Neurology 1993;43:S39-S44.
13. Evans DA, Beckett LA, Albert MS, et al. Level of education and change in cognitive function in a community population of older persons. Ann Epidemiol 1993;3(l):71-77.
14. Meaney M, Aitken D, Bhatnager S, et al. Effect of neonatal handling on age-related impairments associated with the hippocampus. Science 1988;239:766.
15. Barker D, Osmond C. Infant mortality, child- hood nutrition, and ischaemic heart disease in England and Wales. Lancet 1986;May 10:1077- 81.
16. Barker D, Osmond C, Golding J, et al. Growth in utero, blood pressure in childhood and adult life, and mortality from cardiovascular disease. BMJ 1989;298:564-67.
17. Barker D, Osmond C, Winter P, et al. Weight in infancy and death from ischaemic heart disease. Lancet 1989;September 9:577-80.
18. Barker D, Bull A, Osmond C, Simmonds S. Fetal and placental size and risk of hypertension in adult life. BMJ 1990;301:259-62.
19. Barker D. The intrauterine environment and adult cardiovascular disease. In: The Childhood Environment and Adult Disease. Wiley, Chichester: Ciba Foundation Symposium 1991;156:3-16.
20. Barker D, Martyn C. The maternal and fetal ori- gins of cardiovascular disease. J Epidemiol Commun Health 1992;46:8-1 1.
21. Barker D, Godfrey K, Osmond C, Bull A. The relation of fetal length, ponderal index and head circumference to blood pressure and the risk of hypertension in adult life. Pediatric and Perinatal Epidemiology 1992;6:35-44.
22. Barker D, Meade T, Fall C, et al. Relation of fetal and infant growth to plasma fibrinogen and factor VII concentrations in adult life. BMJ 1992;304:148-52.
23. Barker D, Osmond C, Simmonds S, Wield G. The relation of small head circumference and thinness at birth to death from cardiovascular dis- ease in adult life. BMJ 1993;306:422-26.
24. Schweinhart LJ, Barnes HV, Weikart DP. Significant benefits: The High/Scope Perry preschool study through age 27. Monographs of the High/Scope Educational Research Foundation 1 993; 10.
25. Palmer FH. Long-term gains from early intervention: Findings from longitudinal studies. In: Zigler E, Valentine J (Eds.), Project Head Start: A Legacy of the War on Poverty. New York: The Free Press, 1979.
26. Case R, Griffin S. Rightstart: An early interven- tion program for insuring that children's first for- mal learning of arithmetic is grounded in their intuitive knowledge of numbers. Report to the James S. McDonnell Foundation, 1991.
27. Pulkkinen L, Tremblay RE. Patterns of boys' social adjustment in two cultures and at different ages: A longitudinal perspective. Int J Behav De v 1992;15:527-53.
28. Power C, Manor O, Fox J. Health and Class: The Early Years. London: Chapman & Hall, 1991.
29. Haan M, Kaplan GA, Camacho T. Poverty and health: Prospective evidence from the Alameda County Study. Am J Epidemiol 1987;125:989-97.
30. Karasek R, Theoreil T. Healthy Work: Stress, Productivity, and the Reconstruction of Working Life. New York: Basic Books, 1990.
31. Marmot M. Explaining Socioeconomic Differences in Sickness Absence: The Whitehall II Study. Toronto: Canadian Institute for Advanced Research, 1993.
32. Marmot M, Smith G, Stansfeld S, et al. Health inequalities among British Civil Servants: The Whitehall II Study. Lancet 1991;337:1387-93.
33. Marmot M, Kogevinas M, Elston M. Social/eco- nomic status and disease. Annu Rev Public Health 1987;8:111-35.
34. Wolfson M, Rowe G, Gentleman J, Tomiak M. Career earnings and death: A longitudinal analy- sis of older Canadian men. Canadian Institute for Advanced Research, Population Health Working Paper, 12, Toronto, 1991.
35. OECD and Statistics Canada. Literacy, Economy, and Society: Results of the First International Adult Literacy Survey. OECD/Ministry of Industry Canada, 1995.
MAY- JUNE 1998 CANADIAN JOURNAL OF PUBLIC HEALTH S 19
This content downloaded from 195.34.79.79 on Tue, 17 Jun 2014 00:17:33 AMAll use subject to JSTOR Terms and Conditions