Embed Size (px)
Citation preview

957
Superselective Injection of Polyvinyl Alcohol Microemboli for the Treatment of Cerebral Arteriovenous Malformations Giuseppe Scialfa' and Giuseppe Scotti'
Treatment of cerebral arteriovenous malformations (AVMs) with isobutyl-2 cyanoacrylate (IBCA) injected through a calibrated-leak balloon is a well established procedure. Technical problems, selection of patients, indications, contraindications, and complications have been reported and discussed extensively [1-10]. This technique, though effective, has several risks such as injection of glue into the venous side of the AVM, proximal occlusion of the feeding artery, and gluing of the balloon catheter within the vessels.
Particulate embolic agents such as Silastic spheres have also been used, but the injection is not selective and the results are not as effective as with glue [11-13]. Polyvinyl alcohol (PV A) microemboli are usually used to treat dural malformations or malformations of the face and neck [14]. Recent experimental work in animals has shown the histopathologic changes of intraarterial injection of PV A microemboli in rat cerebral cortex [15]. The results of these experiments using particles of small size (50-150 fLm in diameter) indicate that the emboli adhered to the vessel walls and were covered by endothelium by 5-7 days after injection. Between 7 days and 9 months no further changes were seen either in the vessel walls or in the PVA fragments. There was no evidence of any inflammatory response to the PV A in the absence of occlusion . The arterial wall remained free of acute or chronic inflammatory cells for the entire period of the study, its only response being that of endothelial overgrowth. Instead of using IBCA in two recent patients with cerebral AVMs, we superselectively injected PV A microemboli directly into the feeding pedicles close to the nidus of the lesion using silastic microcatheters.
Technique
Silastic tubing 2.5 French in caliber, with an internal diameter of 0.5 mm and an outer diameter of 0.95 mm (Ingenor Medical Systems, Paris), and no. 17 latex balloons (Ingenor Medical Systems, PariS) were used. The latex balloon was glued to the tip of the catheter by using a drop of plasma and
IBCA. A hole in the balloon was made with a surgical blade, cutting a very limited part of the distal tip of the balloon. The resulting hole was larger than the one usually made when injection of isobutyl is planned.
The balloon was introduced with a coaxial technique within a 5.8 French Elecath catheter placed within a 6 French Cordis introducer in the femoral artery. The balloon was propelled into one of the feeding pedicles of the A VM using a pressure injection chamber (Becton-Dickinson, Rutherford, NJ). Even after rapid and strong injections the balloon never inflated, but its round and smooth form helped the Silastic tubing to pass the narrow curves of the siphon or branches of the middle cerebral artery, when pressure was exerted within the chamber.
PVA foam particles of 149-250 or 250-590 fLm (Unipoint Labs., High Point, NC) were prepared in a distilled water sterile solution after emulsifying the dry powder with distilled water in a blender for about 1 half hour [16] . The solution was then filtered and the wet powder was placed in a test tube with fresh distilled water, steam sterilized , and stored. When the sterile solution was to be used, the distilled water was decanted; about 1 g of the wet bloc of particles was suspended in 50 ml of non ionic contrast medium (iopamidol 300, Bracco Industria Chimica, Milan) and repeatedly aspirated and ejected from a 20 ml syringe through a one-way plastiC stopcock during progressive tightening of the stopcock. When a homogeneous suspension of particles was obtained, 50 ml of saline and 20 ml of albumin were added. The PV A particles usually precipitated but no agglutination occurred, and thus a homogeneous solution of suspended particles was obtained. This solution could be injected through the Silastic tubing provided the solution was dilute. The elasticity of the Silastic tubing allowed some dilatation, permitting the passage of particles up to 590 fLm .
To obtain a continuous delivery of separate particles, we used a 20 cm connecting tube between the syringe and the catheter. The catheter was connected to the tube by a 20 gauge plastic needle introduced into its proximal end for about 1 cm. Particles were injected using 1 ml insulin syringes; the
Received July 18, 1984; accepted after revision May 13, 1985. 1 Servizio di Neuroradiologia, Ospedale Niguarda Cil Granda, Piazza Ospedale Maggiore 3, 20162 Milan , Italy. Address reprint requests to G. Scialfa .
AJNR 6:957-960, November/December 1985 0195-6108/85/0606-0957 © American Roentgen Ray Society

958 SCIALFA AND SCOTTI AJNR:6, Nov/Dec 1985
A
c
E F
concentration depended on the volume of particles that was aspirated each time from the bottom of the solution into the syringe. We have used this technique in two patients , injecting a total of seven pedicles: three lenticulostriate and four cortical branches.
B
o
Case Reports
Case 1
G
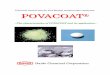
Fig. 1.-Case 1. Lateral (A) and anteroposterior (8) left internal carotid angiegrams. Large, deep AVM . Selective injection of middle cerebral artery pedicle supplying AVM before (C) and after (0) embolization. Venous drainage is no longer opacified, and normal, previously unopacified , cortical branches are seen. E-G, CT scans after different stages of embolization with PV A particles. Progressive increase in amount of opacified particles in different parts of AVM.
j
A 29-year-old man had a severe cerebral hemorrhage followed by
prolonged coma and right hemiparesis 10 years before. He recovered

AJNR:6, Nov/Dec 1985 PYA MICROEMBOLI FOR TREATING CEREBRAL AVMs 959
A
c
but remained hemiparetic. The hemiparesis worsened slightly in the last few years . The AVM (figs. 1 A and 1 B) was situated in the frontotemporoparietal region involving the basal ganglia and was fed by cortical and deep branches of the middle cerebral , anterior, and posterior cerebral arteries. The patient was treated in three stages, and six different pedicles were injected, always with PYA particles of 149-250 /lm. In the first stage two sylvian branches were injected; in the second stage three pedicles were injected: a frontal branch and two lenticulostriate arteries. The frontal branch was the same one injected in the first stage. The catheter became obstructed once and had to be replaced . Rupture of the proximal end close to the connecting needle occurred twice. The broken segments were cut with a blade and the needle reinserted allowing the continuation of the procedure. In the third stage five pedicles were injected, three lenticulostriate and two cortical branches. One of the lenticulostriate arteries and one of the cortical branches had been treated in the previous sessions. The catheter became obstructed once and had to be replaced. Rupture of the proximal end occurred twice.
Figures 1 C and 1 D show one of the pedicles before and after injection of particles . Before injection an early draining vein was seen, while after injection of PYA there was no more arteriovenous shunting, and many tiny branches became evident. This was never seen after embolization with IBCA, since the occlusion of vessels is more massive. The particles were usually injected in relatively large amounts, using the delivery technique described. Injection of a pedicle was terminated when it was believed, by fluoroscopic and angiographic control , that the part of the AVM supplied by it was occluded.
B
D
Fig. 2.-Case 2. Lateral (A) and anteroposterior (8) right internal carotid angiograms. Large, deep temporoparietooccipital AVM . C, Selective injection of cortical branch of sylvian artery before embolization with PVA particles. Contrast material is diluted because of high flow. 0 , After embolization . Many tiny cortical branches are opacified.
Figures 2E-2G are CT scans obtained after different stages of embolization. The amount of hyperdense PYA particles within the malformation is seen to increase progressively . No side effects occurred , and the patient tolerated the procedure well.
Case 2
A 14-year-old boy had an extensive deep right temporoparietooccipital AVM fed by branches of the middle and posterior cerebral arteries (figs. 2A and 2B). He had been having headaches and had a left homonymous hemianopia. He was treated in four stages, three times injecting IBCA and once injecting PYA particles of 149-250 /lm. Particles were injected in a sylvian branch. Figures 2C and 2D show the superselective injection of the pedicle before and after embolization with PYA particles. The high flow diluted the contrast material before embolization, while after injection of particles more branches were seen because of occlusion of the part of AVM fed by that pedicle. The patient tolerated the procedure well.
Discussion
Our experience demonstrates that selective injection of PV A particles through a calibrated-leak balloon directly into the feeding pedicles of cerebral AVMs very close to the nidus

960 SCIALFA AND SCOTII AJNR:6, Nov/Dec 1985
is technically possible and can be effective in occluding the compartment of the AVM fed by the embolized pedicle. On the basis of our experience, however, we believe this technique is not as effective in occluding the malformation as is IBCA. However, it is safer and can be applied to more pedicles in the same session. In fact, a catheter can be reused to embolize different pedicles in the same session since it does not remain occluded by glue. The angiographic result may be different from that obtained after embolization with IBCA. Using PVA particles, the nidus is occluded, but the embolized pedicle may remain patent over a longer segment, and tiny cortical branches not seen before embolization can become visible. More experience is needed to evaluate long-term clinical and angiographic results and to identify the ideal group of patients for this type of treatment.
REFERENCES
1. Kerber CW. Balloon catheter with a calibrated leak: a new system for superselective 'angiography and occlusive catheter therapy. Radiology 1976; 120 : 547 -550
2. Vifiuela FV, Debrun GM, Fox AJ , Girvin JP, Peerless SJ. Dominant hemisphere arteriovenous malformations: therapeutic embolization with isobutyl-2-cyanoacrylate. AJNR 1983;4 :959-966
3. Pevsner PH, Doppman JL. Therapeutic embolization with a microballoon catheter. AJNR 1980;1 :171-181 , AJR 1980;134: 949- 958
4. Bank WO, Kerber CW, Cromwell LD. Treatment of intracerebral arteriovenous malformations with isobutyl-2-cyanoacrylate. Initial clinical experience. Radiology 1981 ;139 :609-616
5. Cromwell LD, Harris AB. Treatment of cerebral arteriovenous
malformations. A combined neurological and neuroradiological approach. J Neurosurg 1980;52 :705-708
6. Debrun G, Vifiuela F, Fox A, Drake CG. Embolization of cerebral arteriovenous malformations with bucrylate. Experience in 46 cases. J Neurosurg 1982;56 : 615- 627
7. Kerber CW, Bank WO, Cromwell CD. Calibrated leak balloon catheter. A device for arterial exploration and occlusive therapy. AJR 1979;132 :207-212
8. Debrun G, Lacour P, Caron J, Hurth M, Comoy J, Keravel Y. Detachable balloon and calibrated-leak balloon techniques in the treatment of cerebral vascular lesions. J Neurosurg 1978; 49:635-649
9. Cromwell LD, Kerber CWo Modification of cyanoacrylate for therapeutic embolization: preliminary experiences. AJR 1979; 132 : 799-801
10. Pevsner PH. Microballoon catheter for superselective angiography and therapeutic occlusion. AJR 1977;128:225-230
11 . Patronas MJ , Marx WJ, Duda EE, Mullan JJ. Microvascular embolization of arteriovenous malformations: predicting success by cerebral angiography. AJNR 1980;1 :459-462
12. Wolpert SM, Stein BM. Catheter embolization of intracranial arteriovenous malformations as an aid to surgical excision. Neuroradiology 1975;10 :73-85
13. Wolpert SM, Stein BM. Factors governing the course of emboli in the therapeutic embolization of cerebral arteriovenous malformations. Radiology 1979;131 :125-131
14. Latchaw RE, Gold LHA, Polyvinyl foam embolization of vascular and neoplastic lesions of the head, neck and spine. Neuroradiology 1979;131 :669-679
15. Quisling RG, Mickle JP, Ballinger WB, Carver CC, Kaplan B. Histopathologic analysis of intraarterial polyvinyl alcohol microemboli in rat cerebral cortex. AJNR 1984;5 : 1 01-1 04
16. Berenstein A, Graeb DA. Convenient preparation of ready-to use particles in polyvinyl alcohol foam suspension for embolization. Radiology 1982;145 :846



















![Unplasticized polyvinyl chloride [uPVC] Facts](https://img.pdfslide.us/doc/110x75/56812ba2550346895d8fceab/unplasticized-polyvinyl-chloride-upvc-facts.jpg)







