Embed Size (px)
Citation preview
SUPERFICIAL BLADDER CANCER THERAPY
MOSHE SHALEV MDDEPARTMENT OF UROLOGY
MEIR MEDICAL CENTER KFAR-SABA
INTRODUCTION
Fourth most common cancer in men, eighth in women.
Superficial at time of diagnosis - 74% Stage Ta -70%, T1-30%. Despite complete tumor resection, 66%
will develop tumor recurrence in 5 years. By 15 years 88% will develop
recurrence.
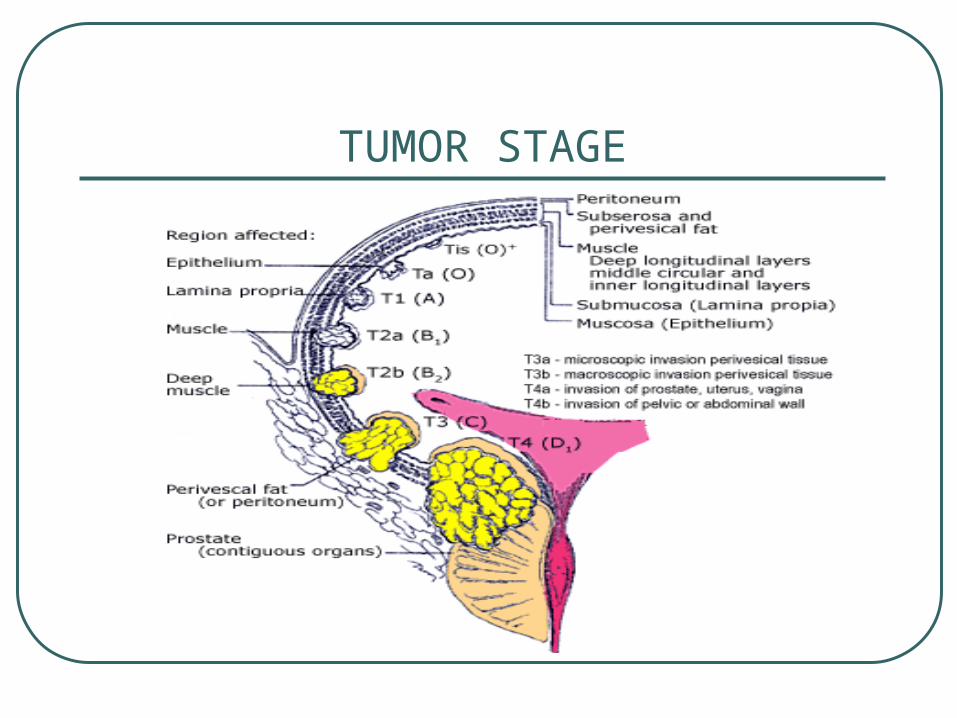
TUMOR STAGE
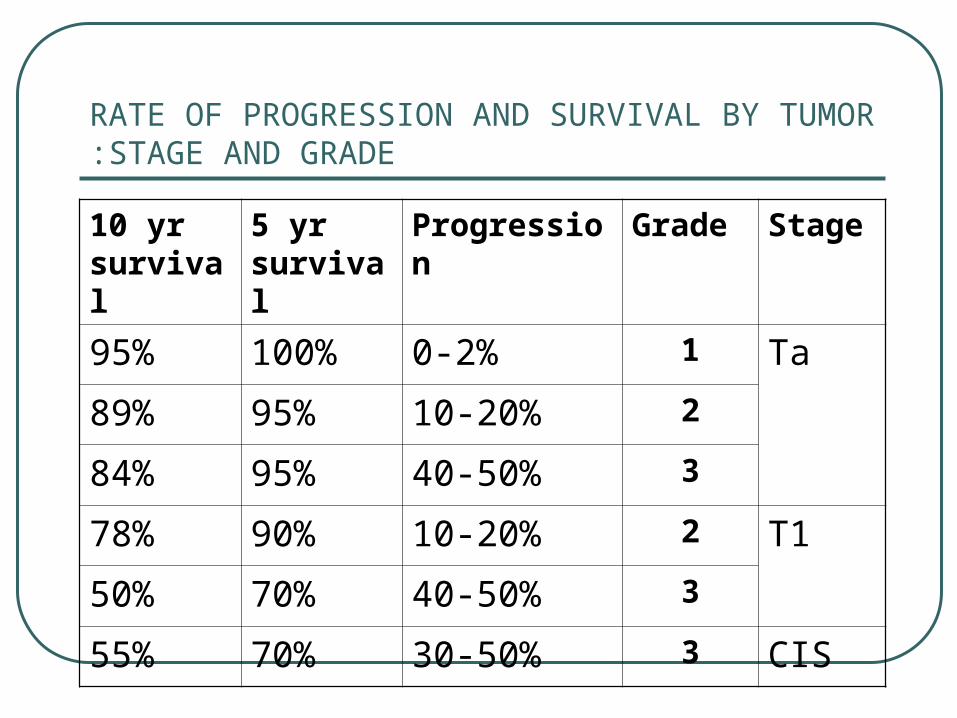
RATE OF PROGRESSION AND SURVIVAL BY TUMOR STAGE AND GRADE:
StageGradeProgression5 yr survival
10 yr survival
Ta10-2%100%95%
210-20%95%89%
340-50%95%84%
T1210-20%90%78%
340-50%70%50%
CIS330-50%70%55%
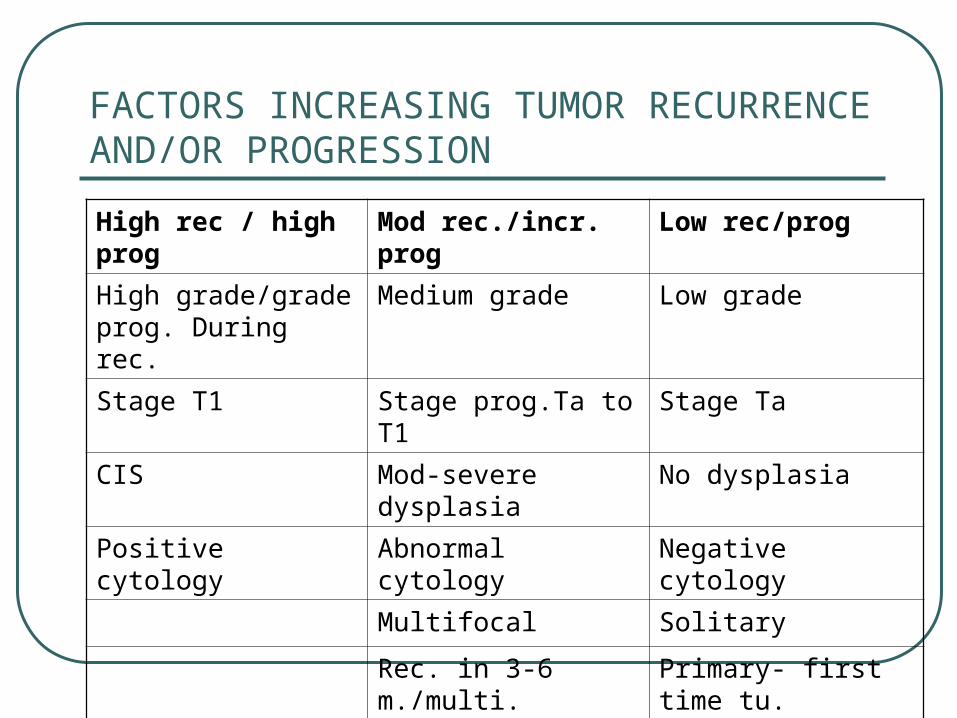
FACTORS INCREASING TUMOR RECURRENCE AND/OR PROGRESSION
Low rec/progMod rec./incr. progHigh rec / high prog
Low gradeMedium gradeHigh grade/grade prog. During rec.
Stage TaStage prog.Ta to T1Stage T1
No dysplasiaMod-severe dysplasiaCIS
Negative cytologyAbnormal cytologyPositive cytology
SolitaryMultifocal
Primary- first time tu.Rec. in 3-6 m./multi.
PapillarySessile/nodular

FACTORS INCREASING TUMOR RECURRENCE AND/OR PROGRESSION
Low rec/progMod rec./incr. progHigh rec / high prog
Size < 5 cmSize > 5 cm
Short dis.durationLong duration > 4 yr
Complete resectionIncomplete resection
No prior intraves. TxFailed intraves. Tx
Low prolif. Markers eg. Ki-67
High prolif. markers
Normal DNA ploidyAbnormal ploidyFrank DNA aneuploidy
E-cadherin positiveE- cadherin negative
P53 negativeP53 positive
RB positiveRB negative
P21 positiveP21 negative

TCC PROGRESSION
GOALS OF INTRAVESICAL THERAPY IN THE MANAGEMENT OF SUPERFICIAL TCC
ERADICATING EXISTING/RESIDUAL TUMOR
PREVENTING RECURRENCE AFTER COMPLETE BLADDER TUMOR RESECTION
PREVENTING PROGRESSION OF DISEASE
INDICATIONS FOR INTRAVESICAL THERAPY
Most effective when tumor burden is minimized by TURT or fulguration of visible areas of CIS
In the absence of other risk factors for progression – not required for grade 1 Ta lesions.
Multifocal Ta disease is a relative indication for intravesical therapy
INDICATIONS FOR INTRAVESICAL THERAPY
Stage T1 irrespective of grade The presence of even small foci of CIS Low grade Ta disease recurring within 2
years Persistent positive urine cytology
localized to bladder

INDICATIONS FOR INTRAVESICAL THERAPY Prostatic urethral involvement with CIS
carries a high risk of progression and poor prognosis
The use of BCG immunotherapy has effectively spared cystectomy
Intravesical chemotherapy appears to be ineffective in the treatment of the prostatic urethra
TURP is recommended for staging and to open the bladder neck to allow BCG to bathe the prostatic urethra.
CHEMOTHERAPY

INTRAVESICAL CHEMOTHERAPY IN SUPERFICIAL BLADDER CANCER
Responses to topical chemotherapy are proportional to drug concentration rather than drug dose.
Responses are dependent on duration of exposure which is short and limited by bladder capacity.
CYTOTOXIC DRUGS ARE ACTIVE AGAINST DNA IN RAPIDLY DIVIDING CELLS.
INTRAVESICAL CHEMOTHERAPY IN SUPERFICIAL BLADDER CANCER
Review of over 4000 pts. In controlled intravesical trials concerning recurrence rates:
1. Average net benefit of IVC over TUR
alone is 14% at 1 to 3 years.
2. Of the 23 reported clinical trials, 13
demonstrated significant reduction of
tumor recurrence.
INTRAVESICAL CHEMOTHERAPY IN SUPERFICIAL BLADDER CANCER
3. Most studies show an advantage of chemotherapy in reduction of tumor recurrence for the first 2 or 3 years.
Traynelis CL and Lamm DL: Current status of intravesical therapy for
bladder cancer, In: Urology Annual Vol 8 pp. 113-143, 1994.
INTRAVESICAL CHEMOTHERAPY IN SUPERFICIAL BLADDER CANCER
Drugs tested in comparative, prospective randomized trials were the antitumor antibiotics Epirubicin, and Doxorubicin, the alkylating agents Thiotepa and Mitomycin C and the heavy metal Cisplatin.
INTRAVESICAL CHEMOTHERAPY IN SUPERFICIAL BLADDER CANCER
Superiority of any of the commonly used intravesical drugs has never been demonstrated
The time to initiate therapy is important for treatment outcome

INTRAVESICAL CHEMOTHERAPY IN SUPERFICIAL BLADDER CANCER
EORTC trials with Mitomycin C(30mg) and Doxorubicin (50mg) :
* Given early on the day of TUR or delayed between 7-15 days
* After 4 weekly and 5 monthly pts. were randomized again for maintenance (6 monthly) or no therapy.
INTRAVESICAL CHEMOTHERAPY IN SUPERFICIAL BLADDER CANCER
EORTC results:1. Time to first recurrence – pts. in the
delayed +no maintenance group tended to do worse.
2. Recurrence rate per year – pts. treated early did better.
3. Tumor free survival (10y f/u) – small but significant difference in favor of adjuvantly treated pts.
INTRAVESICAL CHEMOTHERAPY IN SUPERFICIAL BLADDER CANCER
With 2535 patients enrolled in controlled studies, evidence fails to support the conclusion that intravesical chemotherapy reduces the rate of tumor progression.
On the other hand, overall only 14% of all patients followed up to 10 years progressed.

INTRAVESICAL CHEMOTHERAPY IN SUPERFICIAL BLADDER CANCER
Single early instillation of Mitomycin C after TURT vs. no adjuvant therapy in low risk superficial TCC.
Results: significantly increased recurrence free
interval and decrease number of
recurrences/year
but – benefit is not maintained with long
term follow up after 2 years.

WHAT DO YOU NEED FOR AN EFFECTIVE CHEMO-THERMOTHERAPY?
LOCAL CHEMO-THERMOTHERAPY TREATMENT IN INTERMEDIATE/HIGH RISK SUPERFICIAL TCC
Treatment regimen included 6-8 weekly sessions of MMC+hyperthermia ( 42-43ºc) followed by 4-6 monthly sessions with follow up of 2 years.
Eur Urol Vol. 46 2004

TREATMENT RESULTS
LOCAL CHEMO-THERMOTHERAPY TREATMENT IN INTERMEDIATE/HIGH RISK
SUPERFICIAL TCC
Risk of recurrence after 2 years was 24.6% as compared to 56-66% for similar patients treated with MMC alone.

IMMUNOTHERAPY
PRINCIPLES OF BCG IMMUNOTHERAPY
Maybe either nonspecific or specific Often optimal responses are seen at less
than the maximum tolerated dose. The typical dose response curve is therefore bell shaped with optimal response at intermediate doses.
The optimal dose of BCG remains to be defined and may vary from patient to patient.
PRINCIPLES OF BCG IMMUNOTHERAPY
Current data suggest that intravesical doses between 100 million and 1 billion CFU are effective (1X108 – 1X1010 ), but responses have been reported with doses as low as 10 million CFU OR 1 MG.
It depends on the concentration of organisms that attach to the bladder wall
Agents that inhibit clot formation reduce fibronectin expression – may reduce BCG attachment

PRINCIPLES OF BCG IMMUNOTHERAPY
There are reports that antitubercular AB (INH, Resprim, and Quinolons) do not impair local immunological stimulation but they should be used with caution if no side effects are present.

EFFICACY OG BCG IMMUNOTHERAPY
Long-term follow-up studies consistently demonstrated prolonged protection from tumor recurrence by BCG as well as increasing evidence to suggest that optimal BCG intravesical immunotherapy also reduces tumor progression and mortality.
Randomized comparisons of BCG with intravesical chemotherapy have also demonstrated a statistically significant decrease in tumor recurrence rate with BCG compared with Thiotepa, Doxorubicin and MMC.
SWOG STUDY Urol Oncol 1995
Compared 469 randomized high risk pts. Stage Ta or T1 receiving BCG or MMC.
In the MMC arm – tumor recc. 33% in median time of 18.4 months.
In the BCG arm with a median time of 30 months, 60% were without recc. As opposed to 46% in the MMC arm.
No toxicity – 18% in BCG, 30% in MMC

MELEKOS et al. CANCER 1993
Three arm study of Ives. prophylaxis comparing Epirubicin, BCG and TUR alone.
60%, 68% and 41% respectively remained free from recurrence at a median follow up of 33 months.
BCG was significantly better in preventing recurrence of T1 high grade tumors.

HERR et al. J Clin Oncol 1988
Within 8 months mortality reduced from 32% in TUR alone to 14% in BCG treated patients.
Five-year survival improved to 87% versus 63% for TUR.
Cancer deaths reduced from 37% to 12% and cystectomy rate reduced from 42%to 26%.
LAMM D.L. Urol Clin North Amer 1992
With over 1000 patients from several series the average complete response rate of CIS to BCG is in excess of 70%.
Response rate for chemotherapy – 50% and fewer than 20% remain disease free long term .
EFFICACY OF BCG IMMUNOTHERAPY
Maintenance therapy improves long term results
SWOG- CR=87%. Long term disease free status was maintained in 83%of patients.
In CIS patients treated with BCG the complete response at 6 months is increased from 73% to 87% with 3 additional instillations given at 6 monthly intervals.
EFFICACY OF BCG IMMUNOTHERAPY
Maintenance therapy has improved survival
86% Survival at 4 years with induction therapy improved to 92% in patients receiving maintenance.
THE “OPTIMAL” BCG PROTOCOL
At least 1 week after complete TUR or biopsy of CIS, 6 week induction course of Ives. BCG. 3 months following induction start maintenance.
Maintenance – 3 weekly instillations given 3,6,12,18,24,30,36 months from initiation of induction therapy.
CONCLUSIONS Intravesical BCG remains the most effective
therapy in the management and prophylaxis of superficial TCC of the bladder.
BCG immunotherapy has improved tumor recurrence rates, disease progression rates and has prolonged survival of patients with TCC.
Intravesical chemotherapy has reduced tumor recurrence rates but has had no positive impact on disease progression or survival.
The long term impact of chemo-thermotherapy on recurrence rates, and progression is not yet known.



![Guy Kleinmann , Roy Alon2,Ehud I. Assia · Guy Kleinmann1, Roy Alon2,Ehud I. Assia2 [1] Kaplan Medical Center, Rehovot, Israel [2] Meir Medical Center, Kfar-Saba, Israel](https://img.pdfslide.us/doc/110x75/5f7c90db067d4c24af7cdc67/guy-kleinmann-roy-alon2ehud-i-guy-kleinmann1-roy-alon2ehud-i-assia2-1-kaplan.jpg)