Embed Size (px)
Citation preview

1
Suicide Prevention: A Public Health Approach
David A. Litts, O.D., F.A.A.O.Suicide Prevention Resource Center
December 13, 2005
“Problems are complex and go beyond the
capacity, resources, or jurisdiction for any single
person, program, organization, or sector to
change or control.”Lasker R., Weiss E., Broadening Participation in Community Problem Solving: A Multidisciplinary Model to SupportCollaborative Practice and Research. Journal of Urban Health: Bulletin of the New York Academy of Medicine. Vol 80,No 1. March 2003. p.5.

2
Suicide and Mental Illness
• 90% have diagnosable mental or substance abuse disorders or both
• 60% have unipolar depression– + Aggressiveness, anxiety, agitation
• Other associated mental health problems:– Schizophrenia– Bipolar disorder– Personality disorders, e.g., borderline– Anxiety disorders
Ecological Model
IndividualIndividualPeer/FamilySocietySociety
CommunityCommunity

3
Individual FactorsRisk Protective
• Age/Sex• Mental illness• Substance abuse• Loss• Previous suicide attempt• Personality traits or disorders• Incarceration• Access to means (e.g.,
firearms)• Failure/academic problems• Unemployment• Disability or illness
• Cultural and religious beliefs that discourage suicide and support self-preservation
• Support through ongoing health and mental health care relationships
• Coping/problem solving skills• Resiliency, self esteem, direction,
mission, determination, perseverance, optimism, empathy
• Intellectual competence (youth)• Reasons for living
Peer/Family FactorsRisk Protective
• History of interpersonal violence/conflict/abuse/bullying
• Exposure to suicide• No-longer married• Barriers to health
care/mental health care
• Access to means (e.g., firearms)
• Family cohesion (youth)• Sense of social support• Interconnectedness• Married/parent• Access to
comprehensive health care

4
Community FactorsRisk Protective
• Isolation/social w/drawal
• Barriers to health care and mental health care
• Stigma• Exposure to suicide• Unemployment
• Access to healthcare and mental health care
• Social support, close relationships, caring adults, participation and bond with school
• Respect for help-seeking behavior
• Skills to recognize and respond to signs of risk
Societal FactorsRisk Protective
• Western• Rural/Remote • Cultural values and
attitudes• Media influence• Alcohol misuse and
abuse• Social disintegration• Economic instability
• Urban/Suburban• Access to health care
& mental health care• Cultural values
affirming life• Media influence

5
Family cohesion
Resiliency
Self esteem
Problem solving skills
Social support
Academic problems
Mental health disorder
Bullying victim
Recent significant loss
Parental Psychopathology
4.1
3.1
11.7
17.5
7.5
21 39
6.4
19
12
11
22
2
10.7
293015
8
28
5
3.57
Source: World Health Organization

6
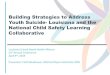
Age-adjusted suicide rates among all persons by state -- United States, 1999-2002
Rates per 100,000 population
0.0 to 9.1
9.2 to 11
11.1 to 13.4
13.5 to 21.1
Source: CDC vital statistics
6.2
20
19
6.3
19
6.6
13
11
11
16
19
12
1212
Suicide Rates by Age, Race, and Gender United States -- 2002
Source: National Center for Health Statistics
Note: non-Hispanic ethnicity
0
10
20
30
40
50
60
5-9
15-19
25-29
35-39
45-49
55-59
65-69
75-79 85
+
Age Group (Years)
Rat
e/10
0,00
0
White Male Black Male White Female Black Female

7
Suicide Rates by Age, Race, and Gender United States - 1999-2002
Source: National Center for Health Statistics
Note: non-Hispanic ethnicity
0
10
20
30
40
50
60
5-910
-1415
-1920
-2425
-2930
-3435
-3940
-4445
-4950
-5455
-5960
-6465
-6970
-7475
-7980
-84 85+
Age Group (Years)
Rat
e/10
0,00
0White Male AI/AN Male Black Male AI/AN Female
Suicide by MethodUnited States, 2002
Source: Natl. Center for Health Statistics
Cut/Pierce2%
Firearm55%
Suffocation20%
Poisoning17%
Fall 2%
Other4%
N= 31,655

8
Suicide Rates by Method
0 2 4 6 8 10 12 14 16 18
Suicide Deaths/100,000
Denmark
Australia
New Zealand
Canada
Scotland
Norw ay
US
The Netherlands
Eng & Wales
Israel
Firearm Poisoning Suffocation All Other
Source: Lois A. Fingerhut, MA, Centers for Disease Control and Prevention, 2000, Unpublished
Suicide RatesUnited States, 1933-2002
Source: Natl. Center for Health Statistics; Rates prior to 1999 Age-adjusted to 1940 U.S. population;1999 and after adjusted to 2000.
5
7
9
11
13
15
17
19
1930 1935 1940 1945 1950 1955 1960 1965 1970 1975 1980 1985 1990 1995 2000
Year
Rat
e/10
0,00
0

9
Necessary Conditions for Prevention
• Knowledge base• Political will• Social strategy
Essential Ingredients for Success
• Leadership• Coalition• Vision• Organization• Planning/Process • A Plan• Resources• Implementation/Evaluation

10
Coalition: Not Just Good Hearted People
Public Health Mental Health
Education Faith-based/community groups
Alcohol and Other Drug Abuse
Domestic violence/Child protective services
Child Welfare Juvenile Justice
Adult Corrections Law Enforcement/First Responders
Crisis Intervention Aging
Medical Examiner/Coroner Survivors/citizen advocates
Coalition
Effective coalitions with highly satisfied members can produce plans of poor quality if they are not trained and equipped to do otherwise.
Butterfoss F, Goodman R, Wandersman A. Community Coalitions for Prevention and Health Promotions: Factors PredictingSatisfaction, Participation, and Planning. Health Education Quarterly, Vol 23(1): 65-79, Feb 1996.

11
Data-Driven Prevention Planning Model
EstablishEstablishClear Vision Clear Vision
and and Framework Framework
for Preventionfor Prevention
Assess Incidence/Assess Incidence/Prevalence, Risk/Prevalence, Risk/
Protection & Protection & DemographicsDemographics
PrioritizePrioritizePopulationsPopulations
&&Risk/Risk/
ProtectiveProtectiveFactorsFactors
Assess Assess Community and Community and Local ReadinessLocal Readiness
forforPreventionPrevention
Assess Community Assess Community and Local and Local ResourcesResources
CompareComparePopulations,Populations,
Risk/Risk/Protection, &Protection, &
ResourcesResources
PromotePromoteReadinessReadiness
forforPreventionPrevention
ImplementImplementProgramsPrograms
totoAddressAddressRisks,Risks,
EnhanceEnhanceProtection,Protection,
and Filland FillGapsGaps
Monitor Data Monitor Data toto
EvaluateEvaluatePolicy, Policy,
Funding,Funding,&&
ProgramProgramDecisionsDecisions
Adapted from Richard Catalano and David Hawkins, U of Washington.
SPRC Goals
• Increase capacity• Enhance partnerships• Train clinicians and community
members • Disseminate evidence-based
practices and other science-based information

12
SPRC Services• Expert Consultation and Technical Assistance• Training support
– On-line training—youth suicide prevention • Workshop 1: Data
Workshop 2: Planning and Evaluation Workshop 3: An Introduction to Gatekeeping
– Face-to-face curricula• Community core competencies +• Clinical core competencies• First Responder Course
www.sprc.org [email protected] 1-877-GET-SPRC
Prevention goes beyond changing individuals--it changes cultural norms
--Murray Levine (1998)
The National Strategy for Suicide Prevention is designed to be a catalyst for social change with the power to transform attitudes, policies and services.
-- The National Strategy (2001)