Embed Size (px)
Citation preview
Australasian Emergency Nursing Journal (2014) 17, 135—137
Available online at www.sciencedirect.com
ScienceDirect
journa l h om epage: www.elsev ier .com/ l ocate /aenj
CASE STUDY
Sudden onset Oculo-cardiac Reflexpost-traumatic eye injury in PNG: A casestudy and discussion
Aaron D. Grogan, RN, MN (Nurse Practitioner) ∗
Oil Search PNG, Medical and Occupational Health Department, Level 7, Credit Haus, Cuthbertson Street,Port Moresby, Papua New Guinea
Received 17 October 2013; received in revised form 9 April 2014; accepted 9 April 2014
KEYWORDSOcular trauma;Nurse Practitioner;Autonomous practice;
Summary This case study examines the onset of traumatic OCR — Oculo-cardiac Reflex —in the remote southern highlands of PNG. The spontaneous occurrence of OCR post-traumain the clinical setting leads to sudden onset bradycardia, nausea and hypotension, resultingin cardiovascular compromise and deteriorating clinical conditions. Initial recognition of the
Trauma;Oculo-cardiac Reflex;Nursing
characteristics of OCR will prepare the clinician to deal with the sequence of events that arisepost the reflex initiation.© 2014 College of Emergency Nursing Australasia Ltd. Published by Elsevier Ltd. All rightsreserved.
hpifatoe
Introduction
Oculo-cardiac Reflex (OCR) refers to the sudden onset ofepisodes of bradycardia, arrhythmias, hypotension and asys-tole, resulting from pressure on the globe or tension on theinternal rectus muscle of the eye.6 OCR was first describedin 1908 through simultaneous reports from Bernard Aschnerand Guisppe Dagnini, and is commonly referred to as the
Aschner-Dagnini reflex.11 Extensive literature exists on theoccurrence of OCR interoperatively, where by enucleationand procedures involving extraocular muscles of the eye∗ Correspondence to: 6 McConnell Street, Bulimba, QLD 4171,Australia. Tel.: +61 0405047715.
E-mail address: [email protected]
al
C
Tiw
http://dx.doi.org/10.1016/j.aenj.2014.04.0021574-6267/© 2014 College of Emergency Nursing Australasia Ltd. Publish
ave resulted in unpredictable vasovagal responses in theatient.3,9 The manifestation of OCR post-traumatic eyenjuries results from the impact to the orbit from a bluntorce resulting in increased internal pressures of the globend possible rupture of the contents via scleral perfora-ion, and also penetration into and threw the lateral musclesf the eye.4,5 Atropine has been used successfully to treatpisodes of OCR intraoperatively, and is also currently useds premedication in children undergoing corrective manipu-ation of ocular muscles.8
ase study
he patient was a 35 year-old female with no known med-cal history, current medications or allergies to date. Sheas approximately 150 cm in height and 50 kg in weight. The
ed by Elsevier Ltd. All rights reserved.

136
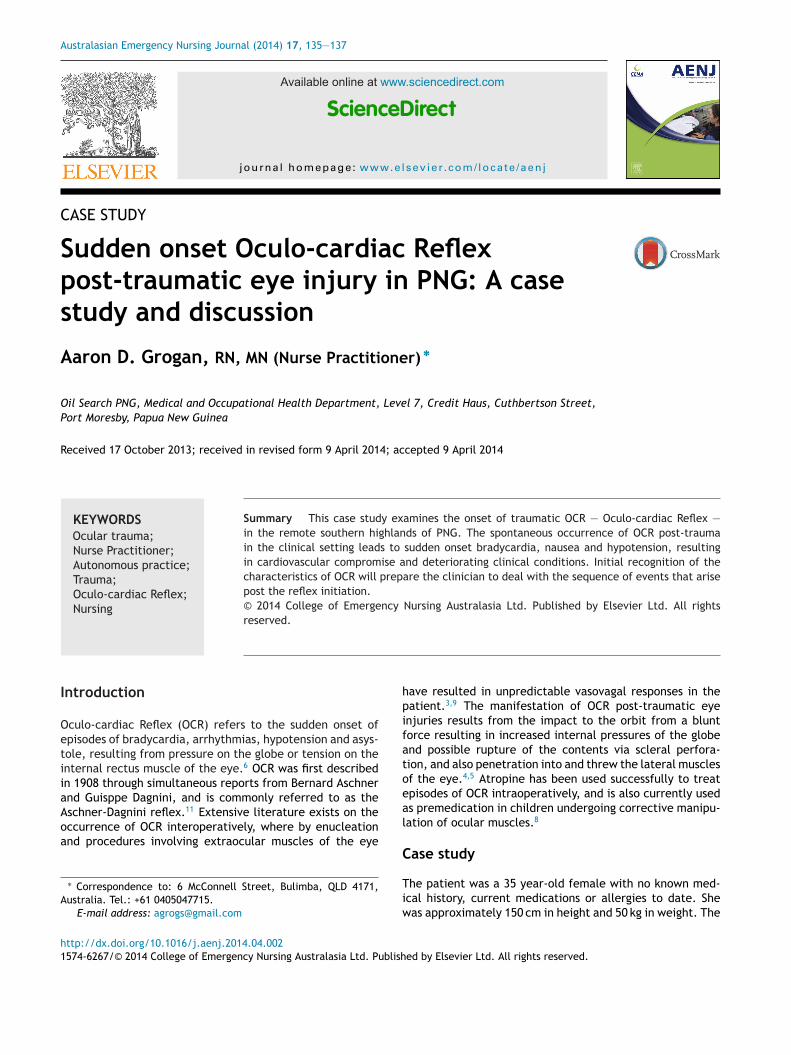
Figure 1 Penetration through the lateral canthus and lowerconjunctiva with rupture of the globe.
persawtn
frmSsctpoh(flba
anwapOcso
rtrtmtca
D
Ontstpiiatdebvi
rtptfriwts
rueaai
P
N
F
N
R
2009;25(6):496—8.5. Jurdy L, Malhotra R. White-eyed medial wall blowout fracture
mimicking head injury due to persistent oculocardiac reflex. J
resentation to an oil company medical clinic, in the south-rn highlands of PNG, occurred after an alleged assaultesulting in a traumatic penetrating right eye injury. It wastated that she was stabbed with a wooden implementfter an altercation with her partner, and the implementas removed at the scene of the injury some 3 hours prior
o presentation. Nil prior eye conditions or history wasoted.
Her initial physical examination was unremarkable apartrom the obvious right sided eye injury. Normal neurological,espiratory, abdominal and limb assessments were docu-ented along with initial observations of: HR 52, BP 103/53,
aO2 99% on room air, and a RR of 20 min. ECG displayedinus bradycardia. On examination the right eye was signifi-antly oedematose and showed a penetrating entry throughhe lateral canthus into and through the lower conjunctivaenetrating through the globe with associated herniationf the intraocular contents through the scleral laceration,aematoma and active bleeding over the anterior eye massFig. 1). Probable penetration of the ethmoid and orbitaloor zones. Sensation over the infra-orbital nerve distri-ution was intact. No obvious ocular movements, no visualcuity attended.
Intravenous morphine was given for pain, 1 g ceftriaxonend 180 mg gentamycin were given intravenously. The exter-al eye was cleaned with 0.9% normal saline and coveredith a light combine pad for comfort. Approximately 30 minfter arrival her heart rate dropped to 30 beats a minutereceded by an episode of associated nausea and vomiting.CR was thought to be the nature of the profound brady-ardia, and as such 600 mcg Atropine was administered. Aubsequent increase in heart rate to 70 beats a minute wasbserved with the ECG remaining in sinus rhythm.
During helicopter transfer of the patient to a regionaleferral hospital another episode of profound bradycardiao 35 beats a minute lasting approximately 20 s occurred,eturning to a rate of 65 beats a minute without interven-ion. This episode was thought to be as a result of turbulentovement in flight, and this occurred 1 h post the adminis-
ration of Atropine. The remaining flight was uneventful, noomplaints or findings of chest pain, shortness of breath or
ltered level of consciousness were noted.A.D. Grogan
iscussion
CR is characterised as the stimulation of the trigeminalerve or branches thereof, and the vagal nerve, referredhroughout literature as the trigeminovagal reflex.2,4 Thetimulation of any branch or nerve endings associated withhe trigeminal nerve is thought to activate the afferentathway sending signal to the sensory nucleus of the trigem-nal nerve via the Gasserian ganglion.7 Vagal stimulations via the efferent pathway whereby OCR is interposednd propitiated via the motor nucleus of the vagal nerve,hus providing negative chronotropic effects on the car-iovascular system.12 OCR therefore has been documentedxtensively post the manipulation of the trigeminal nerveoth traumatically and surgically as leading to cardio-ascular compromise requiring immediate and life-savingnterventions.7
Traumatic eye injuries associated with a vagal medicatedesponse such as nausea and vomiting should always behought of as a precursor or possible onset of OCR and theotential decline of cardiac output.1,10 It would be suggestedhat such patients receive appropriate cardiac monitoringor a designated period of time to detect possible dys-hythmic effects associated with the onset of OCR. Earlydentification of OCR will enable the clinician to interveneith an anticholinergic (Atropine) which has been shown
o prevent and inhibit the efferent effects of vagal nervetimulation.3,4
This case highlights the need for clinicians working inural and remote locations to develop a strong clinicalnderstanding of the physiological processes involved whenncountering traumatic eye injuries. The need for appropri-te clinical monitoring, reassessment and re-evaluation of
patient’s clinical condition is essential in the early timelydentification of OCR.
rovenance and conflicts of interest
one. This paper was not commissioned.
unding
one obtained.
eferences
1. Baek SH, Lee EY. Clinical analysis of internal orbital fractures inchildren. Korean J Ophthalmol 2003;17:44—9.
2. Hemmer LB, Afifi S, Koht A. Trigeminocardiac reflex inthe postanesthesia care unit. J Clin Anesth 2010;22(3):205—8.
3. Jackson BF. Orbital trauma, bradycardia and vomiting: trapdoorfracture and the oculocardiac reflex: a case report. PediatrEmerg Care 2010;26(2):143—5.
4. Joseph JM, Rosenberg C, Zoumalan CL, Zoumalan RA, WhiteWM, Lisman RD. Oculocardiac reflex associated with alarge orbital floor fracture. Ophthalmic Plast Reconstr Surg
Craniofac Surg 2011;22(5):1977—9.

y in P
1
1
Sudden onset Oculo-cardiac Reflex post-traumatic eye injur
6. Kim BB, Qaqish C, Frangos J, Caccamese Jr JF. Oculocar-diac reflex induced by an orbital floor fracture: report ofa case and review of the literature. J Oral Maxillofac Surg2012;70(11):2614—9.
7. Levine JM, Bisker E, Galetta SL, Kumar MA. The oculocardiacreflex may mimic signs of intracranial hypertension in patientswith combined cerebral and ocular trauma. Neurocrit Care2012;16(1):151—3.
8. Schaller B, Cornelius JF, Prabhakar H, Koerbel A, Gnanal-ingham K, Sandu N, et al. The trigemino-cardiac reflex: anupdate of the current knowledge. J Neurosurg Anesthesiol2009;21(3):187—95.
1
NG 137
9. Simon JW. Complications of strabismus surgery. Curr Opin Oncol2010;21:361—6.
0. Sires BS, Stanley RB, Levine LM. Oculocardiac reflex caused byorbital floor trapdoor fracture: an indication for urgent repair.Arch Ophthalmol 1998;116:955—6.
1. Tsai MD, James C, Heitz MD, James W, Bedrossian J. Ocu-locardiac reflex elicited during debridement of an emptyorbit. In: Wills Eye Institute Papers. Paper 2.; 2009
http://jdc.jefferson.edu/willsfp/2. Worthington JP. Isolated posterior orbital floor fractures,diplopia and oculocardiac reflexes: a 10-year review. Br J OralMaxillofac Surg 2010;48(2):127—30.