8/18/2019 sudden deafness journal
1/2
Primary Care Update Brief Summaries for Clinical
Practice
www.Consultant360.com292 CONSULTANT APRIL 2012
Sudden Hearing Loss:
Guideline for Diagnosis and Management
Sudden hearing loss can befrightening for patients—and
challenging for clini-cians. One of the manycauses is
sensorineural
hearing loss (SNHL); early recogni-tion and treatment may
improve thelikelihood of hearing recovery.
Recently, the American Acade-
my of Otolaryngology–Head andNeck Surgery Foundation pub-lished
new guidelines on the diag-nosis and management of suddenhearing
loss in adults; the focus ofthe recommendations is on
suddenSNHL.1 Highlights of these guide-lines are presented
here.
BACKGROUND
Working definition. The guide-line panel defined
sudden SNHL as
a hearing loss of at least 30 dB thataffects at least 3
contiguous fre-quencies and occurs over a 72-hourperiod.1 An
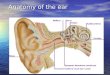
abnormality of the co-chlea, auditory nerve, or higher as-pects of
central auditory perceptionor processing is involved.
Causes. Up to 90% of cases ofsudden SNHL are idiopathic at
initialpresentation ( Table ); however, vas-cular,
viral, or multiple causes aretypically implicated.2 Among
thecauses of sudden SNHL that need tobe recognized and addressed
earlyare vestibular schwannoma (acousticneuroma), stroke, and
malignancy.3
Epidemiology. The incidenceof sudden SNHL is reported to
befrom 5 to 20 per 100,000 population;some estimates are as high as
160per 100,000.4,5 In the United States,about 4000 cases occur
each year.
EVALUATIONHistory. The first step is to dis-
tinguish SNHL from conductivehearing loss (CHL) in a patient
who
presents with sudden hearing loss. Ask the patient about
recent trau-ma, external ear and canal pain, eardrainage, fever,
and other systemicsymptoms.1 Patients with suddenSNHL often
report tinnitus, ear full-ness or pressure, and vertigo; how-ever,
these symptoms may also beassociated with CHL.
Physical examination. Inspectthe ear canals and visualize
the tym-panic membranes. Causes of CHL in-clude cerumen impaction,
middle earfluid, otitis media, foreign bodies, per-forated tympanic
membrane, canaledema from otitis externa, otosclero-sis, trauma,
and cholesteatoma.1 Theotoscopic examination typically
re- veals abnormalities in patients withCHL, while otoscopic
findings areusually normal in those with SNHL.
Traditionally, the Weber andRinne tuning fork tests have
beenused to distinguish SNHL from CHL. Although the results of
these testscan be misleading,6,7 the guidelinepanel recommends
that tuning forktests be used to confirm audiometricfindings.
A Weber test is per formed byplacing the fork on the
patient’sforehead; look for lateralization of
sound to one side. If the soundlateralizes to the affected side,
it islikely that the hearing loss is con-ductive. If the sound
lateralizes tothe opposite ear, the loss is proba-bly
sensorineural.
The Rinne test is done to com-pare bone conduction with
air con-duction for both ears. An abnormal
result of a Rinne test indicates a con-ductive hearing loss of
at least 20 dB.Patients with presumptive sud-
den SNHL should be assessed forbilateral hearing loss,
recurrentepisodes of sudden hearing loss,and focal neurologic
findings. These clinical features can point toan underlying
cause of the hearingloss, such as autoimmune condi-tions, metabolic
disorders, bilateralMeniere disease, and certain neu-
rological disorders.Diagnostic studies. A CT scan
of the head is not warranted duringthe initial evaluation of
patients withsudden SNHL. The scan providesno useful information
that would af-fect initial management, and it posessignificant
risks, including radiationexposure and adverse effects of
in-travenous contrast. Reserve CT forpatients with focal
neurological find-
Table – Causes of sensorineural hearing loss
Cause Examples
Infectious Viral and bacterial infections (including Lyme
disease)
Vascular Stroke, other thromboembolic phenomena,hypercoagulable
states
Neoplastic Vestibular schwannoma, malignancy
Inflammatory Immune-mediated or in conjunction with other
factors
Idiopathic –Data from Stachler RJ et al. Otolaryngol Head Neck
Surg. 2012.1
8/18/2019 sudden deafness journal
2/2
www.Consultant360.com296 CONSULTANT APRIL 2012
Primary Care Update Sudden Hearing Loss:
Guideline for Diagnosis and Management
ings, a history of trauma, or chronicear disease.
The guideline panel also advis-es against routine
laboratory testsin patients with idiopathic suddenSNHL. A specific
test may be con-sidered if the history indicates itmight be useful
in identifying a po-tential cause of the hearing loss,such as
drawing Lyme titers in en-demic regions.
Further workup. For patients with idiopathic sudden
SNHL, orderan MRI scan, auditory brainstem re-sponse (ABR), or
audiometric fol-
low-up to detect retrocochlear pa-thology. A small but
significant per-centage of these patients have anunderlying lesion,
most often a ves-tibular schwannoma.1 In addition,MRI can help
identify other causesof sudden SNHL, such as cochlearinflammation
or multiple sclerosis,or it may reveal evidence of an un-derlying
cause of the sudden SNHL,such as small vessel cerebral isch-emia.
The overall percentage of MRI
abnormalities directly related to sud-den SNHL ranges from 7% to
14%.8,9 Thus, MRI has the highest yield ofany diagnostic
test in the setting ofsudden SNHL.1 If MRI is contraindi-cated
(eg, in patients with pacemak-ers or other metallic implants), an
al-ternative is a fine-cut CT scan of thetemporal bones with
contrast.
The ABR test is highly sensitivefor vestibular schwannomas
that arelarger than 1 cm; however, its report-ed sensitivity for
smaller schwanno-mas varies from 8% to 42%.10-12 Con-sider the
ABR test for the initial eval-uation of older patients in whom
theconsequences of a missed diagnosisof a small tumor may be less
worri-some than in younger patients.
While the guideline panel gen-erally recommends MRI and
ABR todetect any underlying retrocochlearpathology in patients with
sudden
SNHL, serial audiometry is an optionin selected patients. For
those whohave some residual hearing after theinitial episode of
sudden SNHL, pro-
gression of hearing loss detected onrepeated hearing tests is
suggestiveof retrocochlear pathology.
MANAGEMENT
Spontaneous recovery. Somepatients recover completely
withoutmedical intervention, often within thefirst 3 days; others
regain their hear-ing slowly over a 1- to 2-week period. The
greatest spontaneous improve-ment in hearing occurs during thefirst
2 weeks; late recovery is rare.
Corticosteroids. For patients with idiopathic sudden
SNHL, corti-
costeroids may be offered as initialtherapy. These agents have
sites ofaction in the inner ear, and they areeffective in the
treatment of viral, vascular, syphilitic, autoimmune,
en-dolymphatic hydrops (Meniere dis-ease), and other causes of
hearingloss. The recommended regimenconsists of oral prednisone
given at1 mg/kg/d in a single (not divided)dose, with the usual
maximum doseof 60 mg/d, and treatment duration
of 10 to 14 days. Corticosteroidtherapy seems to be most
effectiveduring the first 2 weeks after the ep-isode of sudden
hearing loss; littlebenefit is seen after 4 to 6 weeks.
Consider intratympanic cortico-steroid perfusion for patients
in whom systemic corticosteroids areineffective. The
corticosteroid maybe delivered by a needle throughthe tympanic
membrane, or it maybe placed into the middle earthrough a
tympanostomy tube or amyringotomy. The intratympanicroute avoids
the significant adverseeffects of additional systemic
corti-costeroid therapy.
Other treatments. Hyperbaricoxygen therapy may be beneficial
asan adjuvant intervention if this treat-ment is started within 3
months ofthe onset of idiopathic suddenSNHL. The greatest benefit
has
been seen in patients with severe toprofound hearing loss.1
Antivirals, thrombolytics, vaso-dilators, vasoactive
substances, and
antioxidants have no role in the treat-ment of idiopathic sudden
SNHLbecause their effectiveness has notbeen demonstrated in this
setting.1
FOLLOW-UP
Within 6 months of the diagno-sis of idiopathic sudden
SNHL, orderfollow-up audiometric evaluation. Ifthe patient’s
hearing loss is perma-nent, auditory rehabilitation may berequired.
Counsel patients who haveresidual hearing loss about the po-tential
benefits of hearing aids andassistive listening devices.
A list of organizations thatprovide information and
supportfor patients with hearing loss canbe found on the web site
of theNIH National Institute on Deafnessand Other Communication
Disor-ders: http://www.nidcd.nih.gov/directory/. n
REFERENCES:1. Stachler RJ, Chandrasekhar SS, Archer SM,et
al. Clinical practice guideline: sudden hearingloss. Otolaryngol
Head Neck Surg. 2012;146:S1.
DOI: 10.1177/01945998124364492. Rauch SD. Clinical
practice: idiopathic suddensensorineural hearing loss. N Engl
J Med. 2008;359(8):833-840.3. Saunders JE, Luxford WM, Devgan
KK,Fetterman BL. Sudden hearing loss in acousticneuroma patients.
Otolaryngol Head Neck Surg.1995;113(1):23-31.4. Byl FM Jr.
Sudden hearing loss: eight years’experience and suggested
prognostic table.
Laryngoscope. 1984;94(5, pt 1):647-661.5. Klemm E,
Deutscher A, Mosges R. A presentinvestigation of the epidemiology
in idiopathicsudden sensorineural hearing loss [in German].
Laryngorhinootologie. 2009;88(8):524-527.6. Miltenburg
DM. The validity of tuning fork testsin diagnosing hearing
loss. J Otolaryngol. 1994;23
(4):254-259.7. Browning GG, Swan IR, Chew KK. Clinical
roleof informal tests of hearing. J Laryngol
Otol.1989;103(1):7-11.8. Schick B, Brors D, Koch O, Schafers
M, KahleG. Magnetic resonance imaging in patients withsudden
hearing loss, tinnitus and vertigo. Otol
Neurotol. 2001;22(6):808-812.9. Cadoni G,
Cianfoni A, Agostino S, et al. Magneticresonance imaging findings
in sudden sensorineu-ral hearing loss. J Otolaryngol.
2006;35(5):310-316.10. Chandrasekhar SS, Brackmann DE,
DevganKK. Utility of auditory brainstem response audiom-etry in
diagnosis of acoustic neuromas. Am J
Otol.1995;16(1):63-67.11. El-Kashlan HK, Eisenmann D, Kileny
PR. Auditory brain stem response in small acoustic
neu-romas. Ear Hear. 2000;21(3):257-262.12. Schmidt RJ,
Sataloff RT, Newman J, Spiegel JR,Myers DL. The sensitivity of
auditory brainstemresponse testing for the diagnosis of acoustic
neu-romas. Arch Otolaryngol Head Neck Surg.
2001;127(1):19-22.