Embed Size (px)
Citation preview

1860 CASE REPORT ELLIS ET AL Ann Thorac SurgCOLD-INDUCED URTICARIA DURING HCA 2013;96:1860–2
FEATUREARTIC
LES
hospital day 24, a second ventilator was used to providecontinuous positive airway pressure of 5 cm water togently reexpand the atelectatic left lung. Over the nextseveral days, PEEP was slowly increased to the left lung,with gradual improvement in lung compliance andconcomitant improvement in chest roentgenograms. Thesmall residual pneumothoraces continued to remain sta-ble in size, with increasing left lung aeration, and onhospital day 31, the double-lumen endotracheal tube wasexchanged for a conventional endotracheal tube andconventional ventilation was well tolerated.
The patient was successfully weaned from ECMO anddecannulatedonhospital day 32 after 19 days of support.Onhospital day 41, after several days of improvementin respiratory status andweaning fromPEEP, tracheostomyand gastrostomy tubes were placed. He was dischargedfrom the pediatric intensive care unit on hospital day 55,remained in the rehabilitation service for the next fewweeks, and wasdischarged uneventfully on hospital day 73.
Accepted for publication March 1, 2013.
Address correspondence to Dr Payne, Kingston General Hospital, 76Stuart St, Kingston, ON K7L 2V7; e-mail: [email protected].
Comment
Our experience is the first reported pediatric case whereindifferential lung ventilation strategy and ECMO supportwere used for managing persistent BP fistula. Previousreports indicated successful differential lung ventilation inadults with BP fistula either intraoperatively [3, 4] orpostoperatively [4]. Differential lung ventilation has alsobeen used successfully in patients with unilateral lungdisease wherein lung compliance in the two lungsnecessitates vastly different ventilation strategies for thetwo lungs. Among children, differential lung ventilationhas predominantly been used in smaller patients in theoperating room for video-assisted thoracoscopic surgerywhere lung deflation optimizes the surgical field reducingretractor-induced injury of lung tissue [5]. The use ofdifferential lung ventilation is limited in children becauseit requires at least a 26F double-lumen tube (Rusch,Kemen,Germany) thatmay only be used for children olderthan 8 years. Alternatively, a Univent tube (Fuji, Tokyo,Japan) is available with a 3.5-mm internal diameter thatmay be used in children older than 6 years [6]. Pawar andMarraro [6] have related some experience with a newdevice, the Marrow double-lumen tube with the poten-tial for perioperative use in the infant age range. In ourcase, although single-lung occlusion and ventilation sta-bilized an air leak, improving oxygenation and ventilation,it ultimately failed because ventilation from a single, alsoinjured, lung could not sustain our patient long enough forcomplete resolution of the contralateral injury.
In adults, some case reports indicate successful uses ofECMO, extracorporeal lung assist devices, or both for thetreatment of persistent BP fistulas, mostly in the post-operative period after surgical resection [2, 7, 8], but toour knowledge no reported pediatric cases have includedthe simultaneous use of differential lung ventilation andECMO for managing BP fistula. In clinical scenarioswhere survival rates are extremely low [1], we show thatECMO can successfully be used in children whenconventional strategies used to treat BP fistula fail.
� 2013 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
Differential lung ventilation while a patient is receivingECMO also allows the healthy lung to be ventilatedwhile concomitantly allowing the diseased lung tocollapse completely and heal the BP fistula. This strategyprevents or mitigates atelectasis while also graduallyreinflating the diseased or injured lung, thus protectingagainst extreme and rapid pressures, with the potentialto rupture a healing fistula.
We demonstrate that a combination of differential lungventilation and judicious use of ECMO has an importantrole for rescue therapy when conventional treatment ofBP fistula has failed. Further, this strategy can be used inthe pediatric age range, subject to size limitation.
References
1. Pierson DJ, Horton CA, Bates PW. Persistent bronchopleuralair leak during mechanical ventilation: a review of 39 cases.Chest 1986;90:321–3.
2. Daoud O, Augustine P, Mordant P, et al. Extracorporeal mem-brane oxygenation in 5 patients with bronchial fisutla with se-vere acute lung injury. Ann Thorac Surg 2011;92:327–30.
3. Knoll H, Ziegeler S, Schreiber JU, et al. Airway injuries afterone-lung ventilation: a comparison between double-lumentube and endobronchial blocker: a randomized, prospective,controlled trial. Anesthesiology 2006;105:471–7.
4. Cheatham ML, Promes JT. Independent lung ventilation inthe management of traumatic bronchopleural fistula. Am Surg2006;72:530–3.
5. Hammer GB, Harrison TK, Vricella LA, Black MD, Krane EJ.Single lung ventilation in children using a new pediatricbronchial blocker. Paediatr Anaesth 2002;12:69–72.
6. Pawar DK, Marraro GA. One lung ventilation in infantsand children: experience with Marraro double lumen tube.Paediatr Anaesth 2005;15:204–8.
7. Khan NU, Al-Aloul M, Khasati N, Machaal A, Leonard CT,Yonan N. Extracorporeal membrane oxygenator as a bridge tosuccessful surgical repair of bronchopleural fistula followingbilateral sequential lung transplantation: a case report andreview of literature. J Cardiothorac Surg 2007;2:28.
8. Korvenoja P, Pitkanen O, Berg E, Berg L. Veno-venousextracorporeal membrane oxygenation in surgery for bron-chial repair. Ann Thorac Surg 2008;86:1348–9.
Successful Management ofCold-Induced Urticaria DuringHypothermic Circulatory ArrestAnne K. Ellis, MD, Tarit Saha, MD,Ramiro Arellano, MD, Andrew Zajac, CPC, andDarrin M. Payne, MD
Departments of Medicine, Biomedical and Molecular Sciences,Anesthesiology and Perioperative Medicine, Perfusion, andSurgery, Queen’s University, Kingston General Hospital,Kingston, Ontario, Canada
Cold-induced urticaria (CIU) is a potentially life-threatening immunologic disorder characterized byswelling and edema of exposed tissue in response to
0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2013.03.030
1861Ann Thorac Surg CASE REPORT ELLIS ET AL2013;96:1860–2 COLD-INDUCED URTICARIA DURING HCA
a cold stimulus. We describe the successful man-agement of a patient with a history of severe CIUwho required coronary bypass and repair of anascending aortic aneurysm using hypothermic circu-latory arrest.
(Ann Thorac Surg 2013;96:1860–2)� 2013 by The Society of Thoracic Surgeons
old-induced urticaria (CIU) is a potentially life-
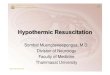
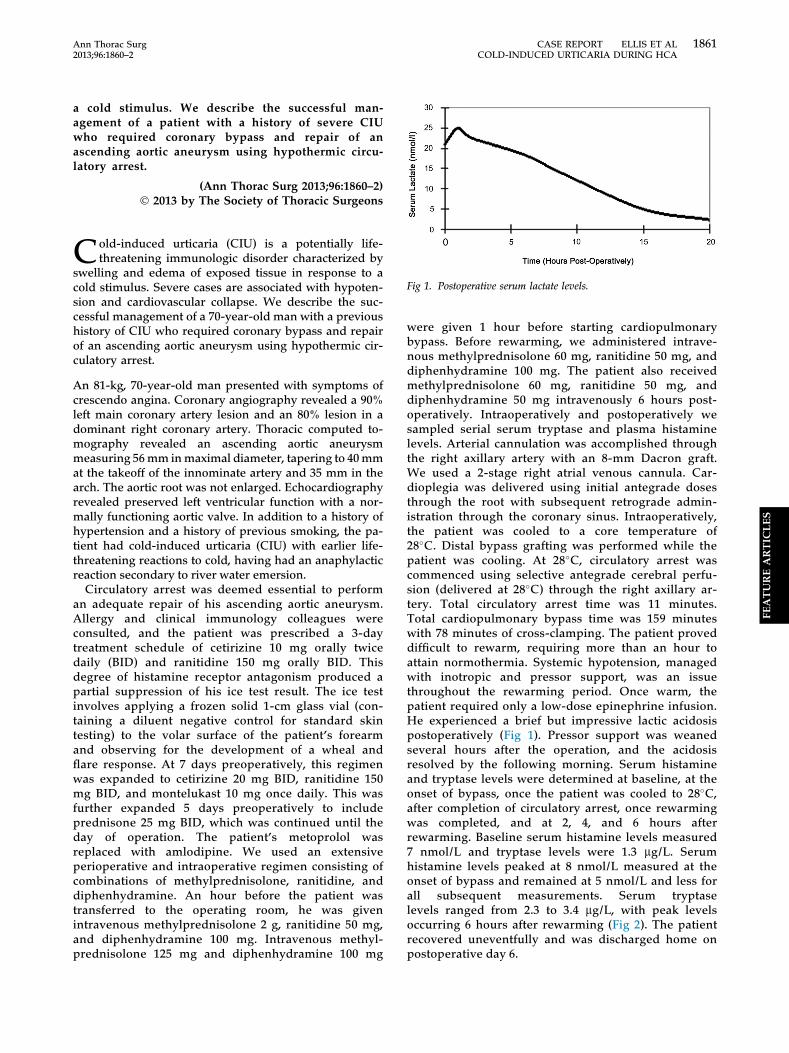
Fig 1. Postoperative serum lactate levels.
FEATUREARTIC
LES
Cthreatening immunologic disorder characterized byswelling and edema of exposed tissue in response to acold stimulus. Severe cases are associated with hypoten-sion and cardiovascular collapse. We describe the suc-cessful management of a 70-year-old man with a previoushistory of CIU who required coronary bypass and repairof an ascending aortic aneurysm using hypothermic cir-culatory arrest.
An 81-kg, 70-year-old man presented with symptoms ofcrescendo angina. Coronary angiography revealed a 90%left main coronary artery lesion and an 80% lesion in adominant right coronary artery. Thoracic computed to-mography revealed an ascending aortic aneurysmmeasuring 56mm inmaximal diameter, tapering to 40mmat the takeoff of the innominate artery and 35 mm in thearch. The aortic root was not enlarged. Echocardiographyrevealed preserved left ventricular function with a nor-mally functioning aortic valve. In addition to a history ofhypertension and a history of previous smoking, the pa-tient had cold-induced urticaria (CIU) with earlier life-threatening reactions to cold, having had an anaphylacticreaction secondary to river water emersion.
Circulatory arrest was deemed essential to performan adequate repair of his ascending aortic aneurysm.Allergy and clinical immunology colleagues wereconsulted, and the patient was prescribed a 3-daytreatment schedule of cetirizine 10 mg orally twicedaily (BID) and ranitidine 150 mg orally BID. Thisdegree of histamine receptor antagonism produced apartial suppression of his ice test result. The ice testinvolves applying a frozen solid 1-cm glass vial (con-taining a diluent negative control for standard skintesting) to the volar surface of the patient’s forearmand observing for the development of a wheal andflare response. At 7 days preoperatively, this regimenwas expanded to cetirizine 20 mg BID, ranitidine 150mg BID, and montelukast 10 mg once daily. This wasfurther expanded 5 days preoperatively to includeprednisone 25 mg BID, which was continued until theday of operation. The patient’s metoprolol wasreplaced with amlodipine. We used an extensiveperioperative and intraoperative regimen consisting ofcombinations of methylprednisolone, ranitidine, anddiphenhydramine. An hour before the patient wastransferred to the operating room, he was givenintravenous methylprednisolone 2 g, ranitidine 50 mg,and diphenhydramine 100 mg. Intravenous methyl-prednisolone 125 mg and diphenhydramine 100 mg
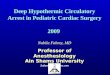
were given 1 hour before starting cardiopulmonarybypass. Before rewarming, we administered intrave-nous methylprednisolone 60 mg, ranitidine 50 mg, anddiphenhydramine 100 mg. The patient also receivedmethylprednisolone 60 mg, ranitidine 50 mg, anddiphenhydramine 50 mg intravenously 6 hours post-operatively. Intraoperatively and postoperatively wesampled serial serum tryptase and plasma histaminelevels. Arterial cannulation was accomplished throughthe right axillary artery with an 8-mm Dacron graft.We used a 2-stage right atrial venous cannula. Car-dioplegia was delivered using initial antegrade dosesthrough the root with subsequent retrograde admin-istration through the coronary sinus. Intraoperatively,the patient was cooled to a core temperature of28�C. Distal bypass grafting was performed while thepatient was cooling. At 28�C, circulatory arrest wascommenced using selective antegrade cerebral perfu-sion (delivered at 28�C) through the right axillary ar-tery. Total circulatory arrest time was 11 minutes.Total cardiopulmonary bypass time was 159 minuteswith 78 minutes of cross-clamping. The patient proveddifficult to rewarm, requiring more than an hour toattain normothermia. Systemic hypotension, managedwith inotropic and pressor support, was an issuethroughout the rewarming period. Once warm, thepatient required only a low-dose epinephrine infusion.He experienced a brief but impressive lactic acidosispostoperatively (Fig 1). Pressor support was weanedseveral hours after the operation, and the acidosisresolved by the following morning. Serum histamineand tryptase levels were determined at baseline, at theonset of bypass, once the patient was cooled to 28�C,after completion of circulatory arrest, once rewarmingwas completed, and at 2, 4, and 6 hours afterrewarming. Baseline serum histamine levels measured7 nmol/L and tryptase levels were 1.3 mg/L. Serumhistamine levels peaked at 8 nmol/L measured at theonset of bypass and remained at 5 nmol/L and less forall subsequent measurements. Serum tryptaselevels ranged from 2.3 to 3.4 mg/L, with peak levelsoccurring 6 hours after rewarming (Fig 2). The patientrecovered uneventfully and was discharged home onpostoperative day 6.

Fig 2. Preoperative, intraoperative, andpostoperative serum histamine and tryptaselevels. (DHCA ¼ deep hypothermic circula-tory arrest; X-clamp ¼ cross-clamp.)
1862 CASE REPORT ELLIS ET AL Ann Thorac SurgDABIGATRAN FOR PROSTHETIC VALVES 2013;96:1860–2
FEATUREARTIC
LES
Comment
CIU is an uncommon albeit well-described phenomenonresulting from mast cell degranulation with subsequentrelease of inflammatory mediators after cold exposure.Histamine appears to mediate most of the clinical mani-festations. Its release is greatest on withdrawal of thecold stimulus. Avoidance of short-term and prolongedexposures to cold stimuli is central to the management ofthese individuals.
Although patients with CIU requiring cardiac operationshave been reported [1–4], this remains an unusual clinicalentity for cardiac surgeons. Booth and Parissis [1] reportedon a patient with known CIU requiring coronary arterybypass grafting (CABG). They administered a combinationof hydrocortisone, ranitidine, and chlorphenamineimmediately before induction of anesthesia. This patientwas kept normothermic throughout the case. Bakay andOnan [2] reported a similar patient with CIU whounderwent CABG; they maintained the patient at or near37�C. They administered 1 mg/kg methylprednisolone12 hours preoperatively, with another 1 mg/kg methyl-prednisolone and a single dose of an antihistamine(pheniramine maleate, 45 mg) given intravenously beforeinduction. Postoperatively the patient was given a 3-daytapering regimen of intravenous methylprednisolone.Johnston and colleagues [3] reported a patient withknown CIU who required a coronary operation. He wasadministered diazepam, scopolamine, morphine, andhydrocortisone before entering the operating room; healso received intravenous administration of cimetidine(300 mg), diphenhydramine (90 mg), and hydrocortisone(100 mg) before induction of anesthesia. This patient wascooled to 31�C. Before rewarming, he was given 300 mgcimetidine and 90 mg diphenhydramine. Intraoperativelythey observed a significant rise in serum histamine levels;however, the patient remained clinically stable. Lanceyand associates [4] reported a case of combined aortic valvereplacement and CABG in a patient with CIU. This patientwas cooled to 32�C for the procedure. An extensiveregimen of fexofenadine, ranitidine, methylprednisolone,and diphenhydramine was used beginning 5 dayspreoperatively and continuing into the postoperativecourse.
To our knowledge, this is the first reported case of apatient with CIU undergoing hypothermic circulatoryarrest. Similar to Lancey and colleagues, we used an
extensive preoperative, intraoperative, and post-operative regimen to blunt the CIU response. Ante-grade cerebral perfusion throughout the period ofcirculatory arrest allowed us to cool the patient to nolower than 28�C.
Others have shown an increase in plasma histaminelevels with rewarming during cardiopulmonary bypass[3]. To blunt this response we used an extensivepharmacologic regimen initiated well in advance of theoperative date. The lack of an observed rise in tryptaselevels suggests that we successfully achieved mast cellstabilization. Our patient required transient low-levelinotropic support for a few hours postoperatively. Healso experienced significant lactic acidosis, with serumlactate levels peaking at 25 mmol/L 2 hours post-operatively. There was no clinical evidence of organmalperfusion or ischemia, and he remained clinicallystable. Although the cause of the lactic acidosis remainsunclear, we believe it to be due to “washout” from pe-ripheral tissue beds. Although not known to be charac-teristic of CIU, perhaps this patient had a pronouncedperipheral arterial vasoconstriction in response to coldstimuli. If this patient had effectively reduced flow toperipheral tissue beds during cooling, this would explainthe accumulation of lactic acid and the subsequent spikewe observed after reperfusion. This could also helpexplain the time it took and the difficulty we hadrewarming the patient.In conclusion, this case suggests that patients with CIU
complicated by anaphylaxis can successfully undergocardiac bypass operations using deep hypothermic circu-latory arrest. We would recommend using an aggressivepreoperative, intraoperative, and postoperative pharma-cologic strategy.
References
1. Booth K, Parissis H. Management of cold-induced urticariaduring cardiac surgery. J Card Surg 2011;26:158–9.
2. Bakay C, Onan B, Onan IS, Ozkara A. Coronary artery bypassgrafting in cold- induced urticaria. Ann Thorac Surg 2010;89:949–51.
3. Johnston WE, Moss J, Philbin DM, et al. Management of coldurticaria during hypothermic cardiopulmonary bypass.N Engl J Med 1986;306:219–20.
4. Lancey RA, Schaefer OP, McCormick MJ. Coronary arterybypass grafting and aortic valve replacement with cold car-dioplegia in a patient with cold-induced urticaria. Ann AllergyAsthma Immunol 2004;92:273–5.