Embed Size (px)
Citation preview

Physical urticariasBoonthorn
30 December 2009

Mechanical◦ Symptomatic dermographism◦ Delayed pressure urticaria◦ Vibratory angio-oedema
Thermal◦ Cholinergic urticaria◦ Localized heat urticaria◦ Cold contact urticaria
Other◦ Exercise-induced anaphylaxis◦ Solar urticaria◦ Aquagenic urticaria
Outline Physical urticarias

Clinical appearance◦ rapid appearance of wheals and/or angioedema◦ wheal consists
Central swelling of variable size, almost invariably surrounded by reflex erythema
itching or sometimes burning sensations with skin return to normal appearance, usually
within 1–24 h
Urticaria ( Definition )
EAACI/GA 2LEN/EDF guideline. Allergy 2006: 61: 316–320

wheal demonstrates ◦ edema of upper and mid-dermis◦ dilatation of postcapillary venules and
lymphatic vessels of upper dermis◦ Upregulation of endothelial adhesion molecules◦ mixed inflammatory perivascular infiltrate of
neutrophils and/or eosinophils, macrophages and T-helper lymphocytes
◦ mild to moderate increase of mast cell numbers
Urticaria ( histology )
EAACI/GA 2LEN/EDF guideline. Allergy 2006: 61: 316–320

Group Subgroup Definition
Spontaneous urticaria Acute urticaria Spontaneous wheals <6 weeks
Chronic urticaria Spontaneous wheals >6 weeks
Physical urticaria Cold contact urticaria Eliciting factor: cold air/water/wind
Delayed pressure urticaria Eliciting factor: vertical pressure (wheals arising with a 3–8 h latency)
Heat contact urticaria Eliciting factor: localized heat
Solar urticaria Eliciting factor: UV and/or visible light
dermographic urticaria Eliciting factor: mechanical shearing forces (wheals arising after 1–5 min)
Vibratory urticaria/angioedema Eliciting factor: vibratory forces, e.g. pneumatic hammer
Other urticaria disorders
Aquagenic urticaria Eliciting factor: water
Cholinergic urticaria Elicitation by increase of body temperature
Contact urticaria Elicitation by contact with urticariogenic substance
Exercise-induced anaphylaxis/urticaria
Eliciting factor: physical exercise
Classification of urticaria
EAACI/GA 2LEN/EDF guideline. Allergy 2006: 61: 316–320

subset of chronic urticaria. approximately 20% - 30% of chronic
urticaria induced by variety of environmental stimuli
eg. exercise, temperature changes, cold, heat,pressure, sunlight, vibration, and water
physical stimuli are predominant cause of condition
incidental factor in case of chronic idiopathic urticaria
multiple physical urticarias ( small number )
Physical urticarias
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Dermographism ( urticaria factitia )

means to‘‘write on the skin’’ most common of physical urticarias incidental finding in evaluation of other skin
conditions ( AD, CIU, and other PU ) rapid onset of cutaneous wheal & flare after
experiencing skin pressure Epidemiology
◦ Simple dermographism ( most common ) approximately 2-5% of general population
◦ Symptomatic forms ( much less common ) no prevalence data
Dermographism ( urticaria factitia )
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Clinical features◦ simple dermographism
Wheal provoked by stroking skin with firm object typically appears within 6-7 minutes and begins to fade
15 to 30 minutes later◦ symptomatic dermographism
appearing in <5 minutes and lasting 30 minutes
◦ red dermographism ( variants of symptomatic ) Follicular or inflamed and swollen
◦ Purposeful stroking ( most common )◦ Unaware inciting event eg. Scratch (dry skin) ◦ Severe dermographism ass. With urticaria
pigmentosa or systemic mastocytosis
Dermographism ( urticaria factitia )
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Pathogenesis◦ remains uncertain◦ Elevated levels of serum histamine (whealing
episode)◦ successful passive transfer serum from
dermagraphic patient transferred dermographism to monkey
◦ Suggest IgE-mediated reaction, but no allergen has been identified
Dermographism ( urticaria factitia )
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Diagnostic testing◦ Stroking skin with firm object, eg. tongue blade◦ Provokes typical wheal&flare response (few mins.)◦ not taking antihistamines◦ Dermographometer ( research )
Apply well-defined,reproducible amount of pressure to subject’s skin
useful in documenting response to therapy Threshold in simple dermographism :4900 g/cm2
in symptomatic dermographism the threshold is 3200 -3600 g/cm2
Dermographism ( urticaria factitia )
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Dermographism ( urticaria factitia )
John Wiley & Sons A/S Allergy 2009: 64: 1715–1721
weal response without itch on provocation at 60 g/mm2 (589 kPa) or higher indicates simple dermographism

Treatment◦ Simple dermographism (asymptomatic) :
requires no therapy◦ symptomatic dermographism : ◦ avoidance of any inciting triggers◦ use of medications
skin hydration and emollients ( prevent scratch ) H1 antihistamines H2 antihistamine ( IF FAIL H1 alone )
◦ UVB light
Dermographism ( urticaria factitia )
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Dermographism ( urticaria factitia )
J Am Acad Dermatol 2008;59:752-7.
Narrowband ultraviolet B phototherapy is beneficial in antihistamine-resistant symptomatic dermographism: pilot study

Delayed pressure urticaria
F. Lawlor, A. Kobza Black / Immunol Allergy Clin N Am 24 (2004) 247–258
Pressure swelling provoked by a bra strap

marked subcutaneous swelling after application of sustained pressure stimulus to skin
Occur in 30 minutes,typically 4 to 6 hours may persist for up to 48 hours , distinguished
from other physical urticarias dependent on degree of pressure, duration of
stimulus, body site affected, activity of disease DPU are provoked (distinguished from CIU) Should be considered in all patients with CIU
whose disease is unresponsive to antihistamines
Delayed pressure urticaria
F. Lawlor, A. Kobza Black / Immunol Allergy Clin N Am 24 (2004) 247–258

Epidemiology Incidence
◦ 2% among 2310 urticaria1 ◦ 37% in 135 pts. In urticaria clinic2
Male:female =2:1 Onset
◦ 5-63 yrs. (peak onset 30-40) Duration
◦ 1-40 yrs. (mean 9yrs.) ,fluctuate condition
Delayed pressure urticaria
F. Lawlor, A. Kobza Black / Immunol Allergy Clin N Am 24 (2004) 247–2581. Champion RH. Br J Dermatol 1988;119:4272. Barlow RJ.et al. J Am Acad Dermatol 1993;29: 954– 8.

Clinical features◦ erythema and cutaneous and subcutaneous swelling◦ Edema of hands and feet (difficult to distinguish from
idiopathic angioedema)◦ Common triggers
Long walks, manual activities using heavy objects, overstaying in standing or sitting position, and wearing tight clothes
◦ Local symptoms Burning pain , warm sensation, dysesthesias, stinging, and
local tension,True itch is rare
◦ Localization of lesions Sites of sustained and constant pressure (e.g., palms, soles,
buttocks, and shoulders)
Delayed pressure urticaria
F. Lawlor, A. Kobza Black / Immunol Allergy Clin N Am 24 (2004) 247–2581. Lawlor F,et al. Br J Dermatol 1989;120:405.2. Czarnetzski BM,et al. Br J Dermatol 1984;111:315

Clinical features◦ Time of onset : 30 min.( early) , 4-6 hrs.(most)◦ Duration of lesions
mean, 22–38 hours; range, 8–72 hours◦ Systemic symptoms
up to 50% of patients, even if rarely relevant: shivering, hyperpyrexia,dizziness, arthralgia, nausea, headache, short breath, and asthenia
◦ Elevated ESR (17-71%) , α-1 and total antitrypsin (acute phase reactant)
◦ Neutrophilia without eosinophilia
Delayed pressure urticaria
Dermatologic Therapy, Vol. 22, 2009, S22–S26

Pathogeneis◦ Not known◦ Proposed mechanism
Late phase reaction ( timing ,cell infiltrate,histopathology)
Type III or other reaction to unknown allergy ( timing, histopathology , but no evidence of vascular damage DIF : negative & normal complement )
mast cell (histmine ,leukotriene not major part) IL-6 increase in lesion ( but nonspecific) Eosinophil ( found eosinophilic major basic protein) Upregulation of ELAM-1(6hrs.),VCAM-1(24hrs.)
Delayed pressure urticaria
F. Lawlor, A. Kobza Black / Immunol Allergy Clin N Am 24 (2004) 247–258

Diagnostic testing◦ Pressure testing ( no standard method)◦ Positive pressure challenge at least 30 min.◦ Usually read pressure test at 6 hrs.
Hanging 15-lb weight at end of crepe bandage over shoulder, thigh, or forearms at least 15 minutes ( usful in clinical setting , not for clinical trial )
apparatus in (known weight)metal rods are held vertically in place, resting on patient’s back
Calibrated dermographometer with spring loaded tip , press right angle to back lat. to spine (99.4g/mm2) 5,15,33,70(optimal),100 sec.
Delayed pressure urticaria
F. Lawlor, A. Kobza Black / Immunol Allergy Clin N Am 24 (2004) 247–258

Delayed pressure urticaria
John Wiley & Sons A/S Allergy 2009: 64: 1715–1721

Delayed pressure urticaria
Pressure instrument adapted from Illig and Kunick with weighted rods resting on apatients’ back.
Experimentally produced pressure swelling using pressure instrument
F. Lawlor, A. Kobza Black / Immunol Allergy Clin N Am 24 (2004) 247–258

Delayed pressure urticaria
calibrated dermographometer. The setting of 10 =pressure of application of 9.75 * 105 Pascals. The tip is pressed perpendicularly into the skin and held in place for 5, 15, 30, 70, or 100 seconds
Experimentally produced pressure papules using the dermographometer
F. Lawlor, A. Kobza Black / Immunol Allergy Clin N Am 24 (2004) 247–258

Treatment◦ Activities cause problem ,be modified or
stopped◦ No single effective drug treatment◦ adequate doses of antihistamine eg. Cetirizine 10
mg q 8hrs.1
◦ Prednisolone at least 30 mg/d may be used in short period for acute severe exacerbation
◦ Aspirin (3900mg/d) not suppress completely◦ colchicine , indomethacin (75mg/d) ineffective◦ Nimesulide+ketotifen improved compared with
steroid
Delayed pressure urticaria
F. Lawlor, A. Kobza Black / Immunol Allergy Clin N Am 24 (2004) 247–2581. Kontou-Fili K, et al. J Am Acad Dermatol 1991;24:1090.

Treatment◦ Dapsone 50mg/d ( clear,5pts.)1
◦ Sulphasalazine 4g/d ( 2pt.)2
◦ Montelukast 10 mg/d for 1 week( 1 pt.)3
◦ Montelukast +nonsedate antihistamine eg. Desloratadine > antihistamine alone
◦ Cyclosporin (3mg/kg/d)4
◦ IVIg ( 0.4g/kg/d for 5 d )4 =>5/8 response
Delayed pressure urticaria
F. Lawlor, A. Kobza Black / Immunol Allergy Clin N Am 24 (2004) 247–2581. Gould DJ et al. Br J Dermatol 1991;125:25.2. Engler RJM et al. Am Au Ast Immunol 1995;74:1553. Berkun Y et al. Allergy 2000;55:203.4. Kobza Black A . J Invest Dermatol 2001;6:148

development of pruritus and swelling after application of vibratory stimulus to the skin
Epidemiology◦ Reports are rare in literature◦ hereditary vibratory angioedema (AD) (4pt.)◦ sporadic and generally related to occupation
Vibratory angioedema
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Clinical features◦ After experiencing appropriate vibratory stimulus,
complain of local pruritus, erythema, and swelling arising within few minutes
◦ Symptoms peak in severity at 4-6 hours and typically resolve by 24 hours
◦ Riding motorcycle, horse, or mountain bike; handling jackhammer; mowing the lawn; toweling; massaging; clapping; and walking
◦ severity and duration to be proportional to : intensity and duration of applied vibratory stimulus area of exposed body surface
Vibratory angioedema
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Pathogenesis◦ not been satisfactorily elucidated◦ Elevated levels of serum histamine and mast
cell degranulation ◦ Passive transfer experiments : negative ◦ nonimmunologic immediate hypersensitivity
reaction◦ Direct mast cell stimulation from vibration may
lead to degranulation and local release of histamine
Vibratory angioedema
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Diagnostic testing◦subject’s arm is held on level plane, and a
vortex mixer is placed in contact with the skin
◦applied for 5 minutes◦observed for 5 to 6 hours◦If positive, develop pruritic erythema and
edema around full circumference of the arm◦Dermatographism and pressure urticaria
should be excluded using the appropriate tests
Vibratory angioedema
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Vibratory angioedema
-vibratory angioedema and weal can be reproduced using a laboratory vortex mixer-measurement of circumference of arm before and after challenge at 3 points (wrist, mid-forearm, elbow) can help define vibration induced swelling
John Wiley & Sons A/S Allergy 2009: 64: 1715–1721

Treatment◦avoidance of specific vibratory stimuli◦H1 antihistamine◦using a 5-minute desensitization protocol
every 5 to 7 days
Vibratory angioedema
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

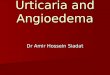
cholinergic urticariaHives induced in patient with cholinergic urticaria after running in place for 10 minutes

“generalized heat urticaria” precipitated by increase in core body temp. Common triggers : exercise, strong
emotions, bathing in hot water, ingestion of spicy or hot foods
Epidemiology◦ 5% of all cases of chronic urticaria ◦ 30% of all cases of physical urticaria◦ onset : during second or third decade of life◦ Male = female
Cholinergic urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Clinical features◦ Numerous punctate wheals (1–3 mm) surrounded
by large flares◦ tingling, itching, or burning sensation of skin
before appearance of hives◦ typically begin on trunk and neck and spread
distally to involve face and extremities◦ Systemic symptoms ( rare cases ) eg.
hypotension, angioedema, and bronchospasm◦ must be differentiated from exercise-induced
anaphylaxis (only appear with exercise)
Cholinergic urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Cholinergic urticaria
demonstrated Postulated
◦ increased number of muscarinic receptors in areas that demonstrate hives
◦ Elevated levels of histamine (during attack)
◦ neurogenic reflex◦ type I allergy to own
sweat
abnormal cutaneous response in presence of cholinergic agents
associated with hypohidrosis
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246
Pathogenesis not been fully elucidated

Diagnostic testing◦ intradermal injection of 0.01 mg of methacholine
in 0.1 mL saline produces local area of hives ( positive 1/3 , not used to rule out)
◦ Specific provocative challenges ( but not specific )◦ Best diagnostic tool : submerged partially in hot
water bath at 40ºC until core body temp. increased > 0.7ºC => genealized urticaria ( aquagenic can produce only submerge portion )
Cholinergic urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Cholinergic urticaria
John Wiley & Sons A/S Allergy 2009: 64: 1715–1721
test is positive if exercise challenge leads to typical rash over 10 min

Treatment◦ Identification and avoidance of known triggers◦ Medical therapy
Oral antihistamines Ketotifen anabolic steroid danazol (reserved only for severe
cases refractory to antihistamines) Beta-blocker ( use with extreme caution )
Prognosis◦ Favorable ( only 1/3 persist > 10yrs. )◦ Average duration 7.5 yrs. ( 3-16 yrs. )
Cholinergic urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

warm stimulus :direct contact with skin result in formation of wheal within minutes must be differentiated from cholinergic urticaria and
solar urticaria Pathogenesis :
◦ histamine release (mast cell cause of condition)◦ Passive transfer experiments : negative
Diagnostic testing◦ application of test tube containing water at 44ºC to arm for 4-5 mins.
=>localized hive develop within few mins.◦ Temp test
Treatment◦ antihistamines and oral cromolyn not been effective◦ Desensitization using hot baths successful in 1pt.
Local heat urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Local heat urticaria
John Wiley & Sons A/S Allergy 2009: 64: 1715–1721
Thresholds may allow for determination ofdisease activity and for assessing response to therapy

Acquired cold urticaria (cold contact urticaria)
Positive ice cube test in a patient with cold urticaria

development of weal-and-flare type skin reactions and ⁄ or angiooedema after exposure of the skin to cold
Fourth commonest type of longlasting urticaria occur minutes after the skin is exposed to cold air,
liquids or objects extensive cold contact may result in generalized
urticarial symptoms +/- systemic reactions endangered by drowning when swimming in cold
water suffocation due to pharyngeal angiooedema after
consuming cold foods and beverages
Acquired cold urticaria
F. Siebenhaar et al.Clinical and Experimental Dermatology, 32, 241–245

Epidemiology most frequently affects young adults Mean duration : 4–5 years remission or at least improvement of
symptoms in 50% of patients within 5 years Women > men (twice) Incidence
◦ 0.05% of urticaria◦ 5.2 - 33.8% of physical urticaria ◦ Varies depending on study and geographical
region, i.e. higher incidences with cold climate
Acquired cold urticaria
F. Siebenhaar et al.Clinical and Experimental Dermatology, 32, 241–245

Atypical cold urticaria Diagnostic distinction
Atypical acquired cold urticaria
Immediate CST-negative (subtypes have additional diagnostic distinctions, listed below)
Delayed cold urticaria Delayed development of urticarial lesions up to 24 h after testing
Cold-dependent dermographism Induction of urticarial lesions after stroking precooled skin
Cold-induced cholinergic urticaria Induction of urticarial symptoms by exercise in cold environments
Systemic atypical cold urticaria Induction of severe urticarial symptoms by exposure to unique environmental conditions;tendency to systemic symptoms
Acquired cold urticariaDDx of ACU
F. Siebenhaar et al.Clinical and Experimental Dermatology, 32, 241–245

Atypical cold urticaria Diagnostic distinction
Hereditary subtypes of cold urticaria
Delayed cold urticaria (AD) History of delayed urticarial lesions; negative immediate CST; delayed development of urticarial-like lesions after 9–18 h that typically resolve into hyperpigmentation
Familial cold auto-inflammatory syndrome (AD)
Episodic cold-induced urticarial-like lesions associated with conjunctival injection, fever, and other systemic inflammatory symptoms; often delayed development of lesions (1–2 h)
Acquired cold urticariaDDx of ACU
F. Siebenhaar et al.Clinical and Experimental Dermatology, 32, 241–245

Pathogenesis Still remain largely unclear Postulate autoimmune mechanism
◦ interaction of IgE autoAb with cold-dependent skin Ag
◦ Cold temperatures presumably encourage interaction of IgM or IgG anti-IgE Ab with IgE attached to mast cells, activate mast cells (primary target cell) and cause mediator release ( histamine,PGD2,PAF,neutrophil&eosinophil chemotactic factor
Acquired cold urticaria
A.A. Wanderer, H.M. Hoffman / Immunol Allergy Clin N Am 24 (2004) 259–286

etiology Secondary ACU
◦ Cryoglobulinemia : secondary to CLL, lymphosarcoma, LCV, HCV
infection, and angioimmunoblastic lymphadenopathy
◦ Infectious diseases ( virus&bact.) infectious mononucleosis ,Syphilis , rubeola, varicella
, hepatitis , and respiratory viral infections ◦ Leukocytoclastic vasculitis◦ Miscellaneous: insect stings, drugs(eg.
Penicillin ,oral contraceptive, ACEI), neoplasms
Acquired cold urticaria
A.A. Wanderer, H.M. Hoffman / Immunol Allergy Clin N Am 24 (2004) 259–286

Diagnostic testing first aim
◦ To confirm ACU by performing simple cold-provocation testing
◦ positive immediate cold-stimulation test (CST): development of urticarial skin lesions at sites of cold
challenge most common : application of ice cube to skin
Second◦ Determine disease activity and monitor response to
therapeutic interventions◦ threshold testing for critical cold-stimulation times and ⁄
or temperatures (Peltier effect based electronic device)
Acquired cold urticaria
Clinical and Experimental Dermatology, 32, 241–245

Acquired cold urticaria
John Wiley & Sons A/S Allergy 2009: 64: 1715–1721

Acquired cold urticaria
CSTT performed with beakers filled with ice slurry.
Confluent wheals appear after 2- and 4-minute applications of cold stimulus to separate skin sites. minimum time of cold stimulus (CSTT) was 2 minutes for this patient.
A.A. Wanderer, H.M. Hoffman / Immunol Allergy Clin N Am 24 (2004) 259–286

Acquired cold urticaria
Peltier effect-based electronic device (TempTest) fordiagnosing and monitoring ACU symptoms. (a,d) Control unitwith ⁄ without applicator; (b) applicator with 12 stimulators;(c) example of use
Clinical and Experimental Dermatology, 32, 241–245

Acquired cold urticaria
Critical temperature thresholds (CTTs) and their changes in ACU are correlated with disease severity and with changes in ACU activity, respectively. ACU severity (a, n = 16)
changes in disease activity (b, n = 19) were assessed in patients with ACU using a three-item and a five-item Likert scale, respectively
British Journal of Dermatology 2010 162, pp198–200

Treatment◦ Avoidance of cold
prevent ACU symptoms,serious events Threshold testing help to recognize and control
cold exposure in daily life◦ Symptomatic therapy
antihistamines : most effective symptomatic therapeutic option to prevent and reduce reactions
Required high dose antihistamine(4*) insufficiently treated patients with severe ACU are
at risk of developing life-threatening complications
Acquired cold urticaria
Clinical and Experimental Dermatology, 32, 241–245

◦ If insufficient response to antihistamines, consider concomitant use of leucotriene antagonists, ciclosporin,corticosteroids or anti-IgE
Curative therapy◦ antibiotic therapy (should be considered)
high doses of penicillin [e.g. oral phenoxymethylpenicillin 1 MU ⁄ day for 2–4 weeks or intramuscular benzylpenicillin 1 MU ⁄ day for 20 days and tetracyclines over 2–4 weeks (e.g.doxycycline 200 mg ⁄ day for 3 weeks)
Acquired cold urticaria
Clinical and Experimental Dermatology, 32, 241–245

Further treatment options◦ induction of cold tolerance (effective method),
needs to be done very cautiously under supervision because of risk of systemic reactions, required high patient compliance
◦ Treatment with topical capsaicin,reported to prevent ACU symptoms
◦ results in depletion of neuropeptides from sensory nerve fibres (pathogenetic role remains to be clarified in detail )
Acquired cold urticaria
Clinical and Experimental Dermatology, 32, 241–245

exercise is only trigger in exercise-induced anaphylaxis
isolated entity ,association with food ingestion, medication use, and menstruation
Epidemiology◦ Age of onset from 4-74 yrs. (mean,24.7 yrs.)◦ Female 71% of population◦ 50% had personal Hx of atopy
Exercise–induced anaphylaxis
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Clinical features◦ prodromal phase ( fatigue, warmth, pruritus, and
erythema ) ◦ progress to large hives that become confluent and
eventually appear as angioedema◦ develops into systemic anaphylaxis with
cardiovascular (hypotension, syncope), respiratory (wheezing, stridor), and gastrointestinal (colic, nausea, vomiting) symptoms. Once fully developed, attacks last 30 minutes to 4 hours
◦ late phase : manifests as headache, fatigue, and warmth and could last from 24 to 72 hours
Exercise–induced anaphylaxis
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Clinical feature◦ most commonly triggered by jogging, brisk
walking, dancing, and aerobic sports◦ Other factors : menstruation , use of aspirin and
NSAIDs, and exposure to cold weather◦ Reaction variable , not reproducible in same
activity◦ Variant type : punctate wheal , triggered only by
exercise and not by elevations in core body Temp.
◦ food-dependent, exercise-induced anaphylaxis
Exercise–induced anaphylaxis
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Pathogeneis◦ elevations in levels of serum histamine and
tryptase during attacks◦ cause of the mast cell degranulation remains
uncertain. Postulated reactions may be IgE mediated
◦ priming phenomenon may be at work , with food, medications, or other stimuli acting as necessary cofactors
Exercise–induced anaphylaxis
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Diagnostic testing◦ Exercise testing is method of choice◦ running on treadmill or using a stationary
bicycle with incremental increases in exertion◦ Passive warming tests to rule out cholinergic
urticaria with systemic symptoms ◦ difficult to reproduce◦ false-negative challenges are common◦ Testing may need to be repeated on multiple
occasions to prove the diagnosis
Exercise–induced anaphylaxis
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Treatment◦ identify and avoid any specific foods, medications, or
other associated factors◦ carry self-injectable epinephrine at all times◦ exercise with a partner who is trained to use
epinephrine◦ avoid exercising within 4 - 6 hours of eating◦ not exercising during extremely hot, humid, or cold
weather or during an allergy season ◦ Antihistamine therapy : only partial benefits in
preventing exercise-induced anaphylaxis and not prevent severe attack
◦ Long term F/U : stable (46%),decrease (47%)
Exercise–induced anaphylaxis
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

direct exposure of the skin to sunlight Epidemiology
◦ 0.4% of urticaria ◦ higher incidence in women ◦ mean age at initial presentation 35 years (range,
17–71 years)◦ risk factors for solar urticaria, such as patient age,
atopic history, and wavelength of light
Solar urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Clinical features◦ classic wheals◦ only erythema, itching, or a sensation of burning◦ DDx with sunburn ( more rapid,only minutes)◦ limitation of physical findings to areas of the body
exposed to direct sunlight◦ Severity increases with intensity of sun exposure◦ anaphylactic reactions are possible if exposed
body surface area is large enough◦ disappearance of urticaria within 24 hours
Solar urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Pathogenesis◦ hypothesized : presence in skin of precursor
molecule , activated by exposure to particular wavelength of light =>photoallergen
◦ Origin of precursor molecule not been determined ◦ Type I ( abn. Precursor molecule not found in
healthy )◦ Type II ( common precursor molecule ,found in
all )◦ passive transfer is not always successful◦ eliminated by removing horny layer of the skin
Solar urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Diagnostic testing◦ Phototesting◦ exposed to varying wavelengths using a
monochromatic light source, and threshold dose, which induces erythema or urticaria
◦ exposure to other light sources, eg. natural sunlight, high-intensity UV light, or slide-projector light, induced symptoms
Solar urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Solar urticaria
John Wiley & Sons A/S Allergy 2009: 64: 1715–1721

Treatment◦ Antihistamines : drug of choice◦ Topical & systemic steroids : used if
antihistamines are insufficient◦ Desensitization ( last only few days )◦ PUVA ( more long lasting protection , greater
long-term adverse effect )◦ Plasmapharesis +/- PUVA (may depend on
characteristics of specific photoallergen at work◦ Longterm F/U : 25% complete resolution , 32%
improved , 35% unchange , 8% worsened
Solar urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

direct skin contact with water Epidemiology
◦ rare disorder with < 50 cases ( case report )◦ Female > male◦ Age of onset : at or slightly after puberty◦ Familial occurrences have been reported ◦ personal or family Hx of atopy occasionally
reported
Aquagenic urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Clinical features◦ small, punctuate (1–3 mm), perifollicular wheals
may occur on all parts of body, although generally not on palms and soles ( Indistinguishable from cholinergic urticaria )
◦ Wheals appear rapidly after direct contact with any source of water (ie, distilled, tap, or saline) not influenced by temperature or pH
◦ fade within 30 - 60 minutes◦ Alcohol and other organic solvents applied to
skin do not lead to wheal formation
Aquagenic urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Clinical features◦ Systemic symptoms are rare◦ refractory period lasting several hours◦ primary differential diagnoses : ◦ cholinergic urticaria ( Exercise, sweating, heat,
and strong emotions )◦ aquagenic pruritus (occurs on skin contact with
water but lacks visible cutaneous manifestations)
Aquagenic urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Pathogenesis◦ still is poorly understood◦ postulated that water interacted with sebum to form
substance capable of acting as direct mast cell degranulation
◦ Enhancing ability of water to penetrate stratum corneum increases the wheal-provoking effects of water (complete removal of stratum corneum , rather than preventing urticaria, worsen reaction)
◦ Activation of cholinergic pathway (ability of the acetylcholine antagonist scopolamine to suppress wheal formation ( some study not suppress)
◦ Methacholine injection : negative
Aquagenic urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Diagnostic testing◦ standard test : application of water compress at
35ºC ( room temp.) to upper body for 30 minutes◦ extremities, are affected less commonly in
aquagenic urticaria◦ Certain areas of skin with thickened epidermal
layer may be less desirable for testing because of reduced penetration of water
◦ rule out other physical urticarias ( cholinergic and cold-induced urticaria )
Aquagenic urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

Treatment◦ Antihistamine therapy : variable response◦ Barrier method : application of petrolatum
ointment◦ UVB light treatment twice a week◦ PUVA therapy◦ Anabolic steroid stanozol
Aquagenic urticaria
J.P. Dice / Immunol Allergy Clin N Am 24 (2004) 225–246

conclusion Pathogenesis for these disorders remains
unclear sensitivity by the mast cell to environmental
stimuli future research is needed conditions share the features of rapid onset
and relatively short duration (except delayed pressure urticaria)
there is enough variability in presentation

Diagnostic testing should be completed for several of these conditions in each patient Because of occasional overlap of triggers and occasional coexistence of multiple physical urticarias,
Treatment ◦ generally avoidance of known triggers ◦ use of antihistamines for prophylaxis◦ Other modalities are occasionally effective◦ Life-threatening,systemic symptoms are rare (except in
exercise-induced anaphylaxis) but must be considered◦ Self-injectable epinephrine should be provided to any
patient at risk
conclusion