Embed Size (px)
Citation preview
ARTICLE IN PRESS
0277-9536/$ - se
doi:10.1016/j.so
�Correspondfax: +44 (0)121
E-mail addr
Social Science & Medicine 63 (2006) 851–857
www.elsevier.com/locate/socscimed
Discussion
Subjective and objective status and health: A response to Adler’s‘‘When one’s main effect is another’s error: Material vs.
psychosocial explanations of health disparities. A commentaryon Macleod et al., ‘‘Is subjective social status a more importantdeterminant of health than objective social status? Evidence
from a prospective observational study of Scottish men’’ (61(9),2005, 1916–1929) (doi:10.1016/j.socscimed.2006.03.018)
John Macleoda,�, George Davey Smithb, Chris Metcalfeb, Carole Hartc
aDepartment of Primary Care and General Practice, Primary Care Clinical Sciences and Learning Centre Building,
University of Birmingham, Edgbaston, Birmingham B15 2TT, UKbDepartment of Social Medicine, Canynge Hall, University of Bristol, Whiteladies Road, Bristol BS8 2PR, UK
cPublic Health and Health Policy, Division of Community Based Sciences, University of Glasgow, 1 Lilybank Gardens,
Glasgow G12 8RZ, Scotland
Available online 17 April 2006
We share the aim outlined in Nancy Adler’scommentary (Adler, 2006) of clarifying the causes ofhealth inequalities (or disparities as she prefers) sothat such inequalities can be effectively reduced.Surely this clarification must involve a careful andcritical appraisal of the evidence, including anattempt to make a distinction between causal andnon-causal associations and an assessment of therelative importance of factors acting throughdifferent mechanisms?
In a large cohort of working men, we relatedvarious measures of social position to subsequenthealth. We found that both objective and subjectivesocial advantage showed an association with betterhealth that was partly explained by a social gradient
e front matter r 2006 Elsevier Ltd. All rights reserved
cscimed.2006.03.020
ing author. Tel.: +44 (0)121 414 3351;
414 3759.
ess: [email protected] (J. Macleod).
in established risk factors. Adverse psychologicalstate, despite an association with unhealthy beha-viour, did not appear to be an important determi-nant of health in this population. Interestingly,adverse psychological state in this population wasconsistently associated with advantageous socialposition. Social position indexed by perceptions ofworkplace status also showed the typical gradient inhealth though differences between the health offoremen and employees were slight. Sociologicaltheory holds that the principal difference betweenforemen and employees is one of social status ratherthan material rewards. (Wright, 1987, 2000) Thestrongest associations between social position andhealth were those between indices of materialenvironment in early life and mortality. From thesepatterns of association we concluded that to reducehealth inequalities, in this population, it would bemore rational to target established risk factors and
.
ARTICLE IN PRESSJ. Macleod et al. / Social Science & Medicine 63 (2006) 851–857852
to reduce material disadvantage, particularly thatexperienced by young children, than to try andimprove psychological state or increase perceptionsof status. We also discussed the problems ofinterpretation that bedevil this type of observationalepidemiology.
Adler suggests that methodological shortcomingsof our study limit the validity of our conclusions; wedisagree. She disputes, for example, the validity ofour measure of workplace status (the distinctionbetween foreman, employee and manager). Thisclassification is theoretically based and has beenused by others. (Muntaner, Eaton, Diala, Kessler, &Sorlie, 1998) It is useful because it allows someinsight into the question of whether objective orsubjective social position is a more importantdeterminant of health since foremen are in acontradictory location where their subjective statusis higher than their objective status. There are otherways to address the question of the relativeimportance of objective and subjective status. Weused the data available to us and were notdismissive of different approaches to the question.Nor was our study, which started in the early 1970s,‘‘designed to show weaknesses’’ in the psychosocialapproach, as Adler claims on two occasions. Ratherwe considered the results of studies that haveadopted various approaches and discussed ourown findings in this context. Adler seems incon-sistent. She chastises us for being supposedlydismissive of others whilst appearing to dismissour own efforts. Further, she proposes a ‘‘different’’approach that seems to be different only in itsconclusions and its apparent readiness to subjectthe hypotheses it advances to rigorous empiricaltesting.
She suggests that our results may have beenbiased by the fact that a blue-collar foreman mayoccupy a lower social position than a white-collaremployee. This seems possible, since some whitecollar employees may be better paid than some blue-collar foremen. In other words this would beprimarily a material difference rather than a statusdifference. If it is a potential source of bias this mustbe because material differences (remuneration) aremore important than status differences (position inthe workplace hierarchy). So we agree that if blue-collar foremen were materially disadvantaged inrelation to white-collar employees and if partici-pants in our study were predominantly from white-collar workplaces then ‘‘confounding by organisa-tional status’’ could have influenced our results.
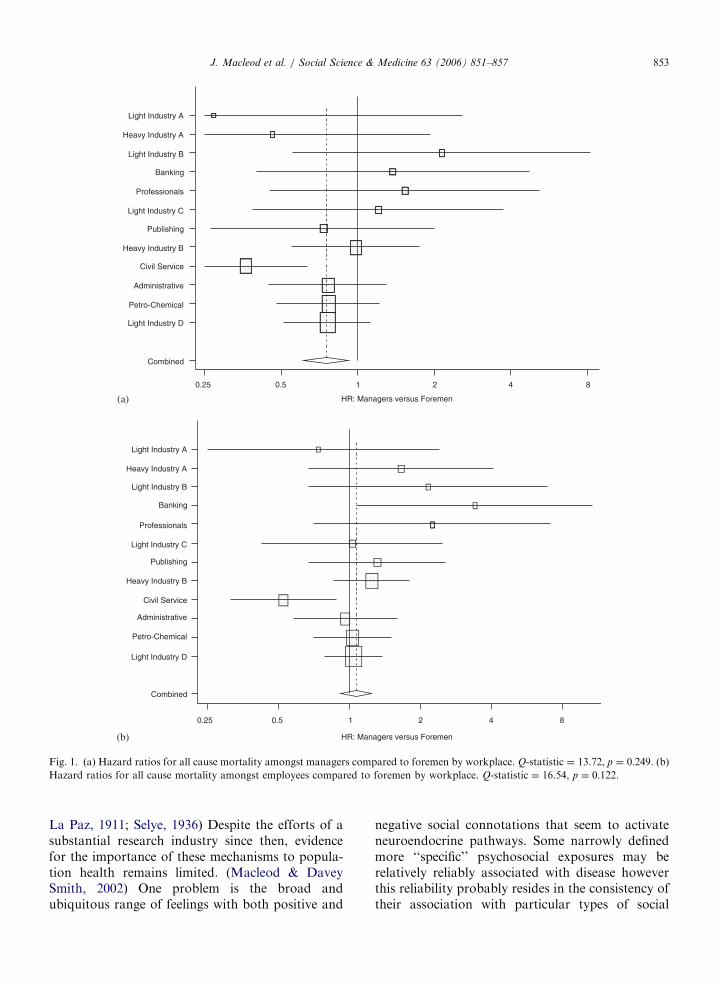
The analyses below address this point. In Table 3of the paper, which illustrates the ‘‘relative risks ofall cause mortality (2158 deaths) over 25 years offollow-up according to different measures of socialposition’’, the age-adjusted estimate for all causemortality of managers compared to foremen is 0.75(0.62,0.90); for employees compared to foremen it is1.11 (0.96,1.30). With further adjustment for work-place the corresponding estimates are 0.78 (0.65,0.95) and 1.12 (0.96, 1.31). This seems to beevidence against confounding by organisationalstatus. A meta-analysis of estimates by workplace(pooled according to inverse of their variance) ispresented below. The 27 work-sites have beencollapsed to 12 (full details available on request)to accommodate small numbers. The pooled esti-mate for managers compared to foremen is 0.75(0.61, 0.92); for employees compared to foremen itis 1.07 (0.92, 1.25). In both instances the Q-statisticsuggests a degree of heterogeneity in estimatesacross workplaces compatible with that expectedby chance. Again this argues against confounding ofthe type suggested. Inspection of the plots shows anobvious outlier. Amongst civil servants (n ¼ 447)mortality risk for managers compared to foremenwas 0.36 (0.20, 0.63) whereas for employeescompared to foremen it was 0.52 (0.31, 0.88). Thesepost hoc analyses should not be over-interpreted,however they do suggest that workplace statusmay have idiosyncratic effects amongst civil ser-vants that do not generalise to other groups ofworkers. (Fig. 1)
Adler also criticises the validity of our stressmeasure. Both the four-item Reeder Stress Inven-tory, and Cohen’s more elaborate instrument (aspreferred by Adler) are subject to very similaramounts of evidence with regard to validity.(Metcalfe et al., 2003) Men reporting higher stressin our study showed the typical profile of unhealthybehaviour associated with psychosocial adversity;they were also more likely to be admitted to apsychiatric hospital (Heslop et al., 2001). Thus ourassessments seem valid.
The question of validity of psychosocial exposuremeasures raises an important general point. Otherthan where it is reasonable to believe a priori that anexposure relates to a particular pathway the searchfor ‘‘specific’’ psychosocial exposures with specificeffects may be misleading. There are, broadly, twopossible pathways from feelings to physical disease.Direct neuroendocrine pathways were first proposedin the early part of the 20th century. (Cannon & De
ARTICLE IN PRESS
HR: Managers versus Foremen
HR: Managers versus Foremen
0.25 0.5 1 2 4 8
0.25 0.5 1 2 4 8
Combined
Light Industry D
Petro-Chemical
Administrative
Civil Service
Heavy Industry B
Publishing
Light Industry C
Professionals
Banking
Light Industry B
Heavy Industry A
Light Industry A
Combined
Light Industry D
Petro-Chemical
Administrative
Civil Service
Heavy Industry B
Publishing
Light Industry C
Professionals
Banking
Light Industry B
Heavy Industry A
Light Industry A
(a)
(b)
Fig. 1. (a) Hazard ratios for all cause mortality amongst managers compared to foremen by workplace. Q-statistic ¼ 13.72, p ¼ 0:249. (b)Hazard ratios for all cause mortality amongst employees compared to foremen by workplace. Q-statistic ¼ 16.54, p ¼ 0:122.
J. Macleod et al. / Social Science & Medicine 63 (2006) 851–857 853
La Paz, 1911; Selye, 1936) Despite the efforts of asubstantial research industry since then, evidencefor the importance of these mechanisms to popula-tion health remains limited. (Macleod & DaveySmith, 2002) One problem is the broad andubiquitous range of feelings with both positive and
negative social connotations that seem to activateneuroendocrine pathways. Some narrowly definedmore ‘‘specific’’ psychosocial exposures may berelatively reliably associated with disease howeverthis reliability probably resides in the consistency oftheir association with particular types of social

ARTICLE IN PRESSJ. Macleod et al. / Social Science & Medicine 63 (2006) 851–857854
disadvantage. (Macleod & Davey Smith, 2002) Thisdoes not take us much further in our search forcauses—we already know that social disadvantage isreliably associated with many diseases. For thisreason it is potentially instructive to look atinstances where a psychosocial exposure is notassociated with social disadvantage or to considerdisease outcomes that are not disproportionatelyexperienced by the deprived. If the associationsbetween heightened psychological ‘‘stress’’ anddisease predicted by the neuroendocrine hypothesiswere apparent in these circumstances (which bytheir nature are unusual) we would have moreconfidence in the importance of neuroendocrinemechanisms to health inequalities. In the exampleswe are aware of, however, they are not apparent(Macleod & Davey Smith, 2005; Nielsen et al.,2005).
Behavioural pathways seem more likely. It hasnever been our intention to deny the importance ofhow people feel to their health, particularly wherenegative emotions are the quite understandable andreasonable response to injustice, disempowermentand marginalisation. Misery (we use this term toencompass the many dimensions of psychosocialadversity invoked in this debate) is important ofitself as it erodes the quality of peoples’ lives. It mayalso make it harder for them to behave in healthyways as immediate solace or avoidance of discom-fort may take precedence over hard to imaginefuture benefit. Perceptions of relative social failuremay well make some people particularly miserableand particularly likely to behave in ways thatdamage their health. But in our study, men whowere materially advantaged experienced psycholo-gical disadvantage (and such disadvantage wasassociated with an adverse health related behaviourprofile). Overall higher stress was associated withslightly better health (Macleod et al., 2001; Macleodet al., 2002). Surely this is clear evidence, in thispopulation, of a primacy of material circumstancesas determinants of health?
We also note that some psychosocial theorists’opinion on the validity of psychosocial measuresseems substantially dependent on whether the studyusing those measures produces results compatiblewith their world-view. Our work casting doubt onthe causal role of stress in heart disease used theReeder Stress Inventory to measure stress (Macleodet al., 2002). This led to strong criticism by somepsychosocial theorists, mirroring that advanced byAdler, and including suggestions that the Reeder
scale failed a ‘‘quality control filter’’ as a measure ofstress. (Marmot, 2005a). This viewpoint is interest-ing in the context of the same theorists’ apparentview of the component of the INTERHEART studythat considered effects of stress on heart disease(Rosengren et al., 2004). This study incorporated apsychological stress measure essentially equivalentto just a single item of the Reeder inventory. Stresswas positively associated with heart disease inINTERHEART, possibly because it was measuredretrospectively in people who had recently experi-enced a heart attack (Macleod, Davey Smith,Metcalfe, & Hart, 2005). However, rather thansuggest that these findings should be discounted, oreven viewed cautiously, INTERHEART has beenapprovingly cited by psychosocial theorists asadding to the weight of evidence supporting apsychological causation of heart disease (Chandola,Brunner, & Marmot, 2006).
We continue to believe that careful considerationof possible non-causal mechanisms is neitherpedantry nor nihilism but is an essential part ofcritical appraisal. For example, Adler suggests that,‘‘Psychosocial and material factors are not mutuallyexclusive but, rather, are complementary. Unex-plained variation in health when material factors areaccounted for may be explained in part bypsychosocial factors and vice versa’’. This may betrue; however, identifying independent effects in thesituation where psychosocial and material disad-vantage are highly correlated and imperfectlymeasured is fraught with difficulty (Christenfeld,Sloan, Carroll, & Greenland, 2004; Macleod &Davey Smith, 2003). Again, this illustrates theadvantages of examining these questions in apopulation where confounding is broken by a lackof the conventional association between materialand reported psychosocial adversity.
Considering the role of reporting bias is alsocrucial in any situation where subjective psychoso-cial exposure is related to subjective symptoms ofdisease. For example, in both the Whitehall II study(cited by Adler as providing some of the strongestevidence for a psychosocial cause of health inequal-ities) and the West of Scotland Collaborative Studyperceived psychosocial adversity is strongly asso-ciated with symptoms of angina yet shows acompletely different relation to objective signs ofheart disease. (Bosma et al., 1997; Macleod et al.,2002; Stansfeld, Fuhrer, Shipley, & Marmot, 2002)(Table 1) We interpret our findings of a link withreported morbidity but not objective indicators such

ARTICLE IN PRESS
Table 1
Associations between perceived stress and job control and subjective and objective outcomes in the West of Scotland Collaborative Study
and the Whitehall II Study
Outcome type Effects in collaborative study Effects in Whitehall II study
Fully subjectivea High exposure 2.66 (1.61–4.41) High exposure 2.02 (1.22–2.34)
Medium exposure 1.37 (0.91–2.08) Medium exposure 1.44 (0.86–2.39)
Low exposure 1.00 Low exposure 1.00
Fully objectiveb High exposure 0.67 (0.36–1.26) High exposure 1.17 (0.8–1.8)
Medium exposure 1.03 (0.71–1.49) Medium exposure 1.16 (0.8–1.7)
Low exposure 1.00 Low Exposure 1.00c
All estimates adjusted for age, social position and cardiovascular risk factors other than c (only unadjusted estimates were reported in the
paper).aRose angina in both studies.bECG abnormalities (Minnesota coding system) in both studies.
J. Macleod et al. / Social Science & Medicine 63 (2006) 851–857 855
as mortality to reflect that a common reportingtendency influences both the manner in whichadverse psychological state and adverse healthstatus are reported (Macleod et al., 2002).
Similar considerations should apply to attemptsto interpret other evidence cited by Adler, such asthe further report from the Whitehall studyshowing that low self-esteem predicts poorer self-perceived health–particularly poorer mental health(Singh-Manoux, Marmot, & Adler, 2005). Thisassociation could be causal but drawing thisconclusion with any security is very difficult. Firstlow self-esteem is a symptom of poorer mentalhealth. Second people who report low perceptionsof their social status (i.e. low self esteem) may alsoreport more symptoms of illness not because,objectively, they are sicker but because, subjectively,they have a generally negative view of theirexperience. (Macleod et al., 2002; Watson &Pennebaker, 1989) With regard to the importanceof status perceptions to health it is interesting thathigh self-esteem is, objectively, often unhealthy.People with high self-esteem tend to report betterhealth (along with greater attractiveness and socialsuccess) but are also more likely to engage in riskybehaviour and less likely to learn from theirmistakes. Despite apparent benefits of high selfesteem for many outcomes inferred from observa-tional studies, interventions to improve self-esteemdo not seem to lead to objective improvements inthese outcomes. (Baumeister, Campbell, Krueger, &Vohs, 2003) As Baumeister and colleagues pointout, many of the links seen in the observationalstudies could be due to reporting tendency, as webelieve may be the case with respect to psychosocialpredictors of health.
Helping people who feel bad to feel better isobviously important. It does not follow, however,that the best way to reduce health inequalities is toimprove the psychological state of the disadvan-taged. Adler suggests that we should not ignore thepotential of interventions at the psychosocial levelto reduce health inequalities. We are not ignoringthis theoretical potential, we are simply noting thecurrent lack of evidence that it can be realised(Macleod & Davey Smith, 2003). Behaviouralinterventions generally show modest effects. Forexample, Adler mentions mood management as anadjunct to smoking cessation. Effective adjuncts tosmoking cessation are obviously a good thing inabsolute public health terms. However, a review ofthe many trials in this area suggests that interven-tion effects are not necessarily mediated through aninfluence on mood (Hughes, Stead, & Lancaster,2004). Further, smoking cessation interventionstend to be less successful amongst the disadvantaged(Honjo, Tsutsumi, Kawachi, & Kawakimi, 2006).Like many effective health technologies they maytend to increase, rather than decrease, healthinequalities (Susser, 2000; Watt, 2002). Behavioursare complex and are not simply influenced by theway people feel but by the structures, contingenciesand choices that shape their lives. However, we didnot mean to suggest that psychosocial theorists (asopposed to conservative politicians) attribute un-healthy behaviour to individual fecklessness and weapologise for this misunderstanding.
Adler states that differences between material andpsychosocial explanations may be more politicalthan intellectual and seems to suggest that we havean ideologically driven intention to denigratepsychosocial research. We are happy to reassure

ARTICLE IN PRESSJ. Macleod et al. / Social Science & Medicine 63 (2006) 851–857856
her that this is not the case. We should rememberthat the debate between the psychosocialist and neo-materialist camps arose following suggestions by theformer that, in societies where the basic materialneeds of every citizen were apparently met, psycho-social factors were the predominant cause of healthinequalities (Marmot, Bosma, Hemingway, Brun-ner, & Stansfeld, 1997). Health inequalities, thisthesis continued, would most effectively be reducedthrough psychosocial interventions rather thanthrough attempts to reduce inequalities in materialcircumstances (Marmot, 1998). Far from embracingthe integrated psychosocial/material model appar-ently advocated by Adler some psychosocial theor-ists consider that:
Material deprivation is no longer a major causeof illness. It’s finished. It’s done with (Marmot,2005b).
On the subject of ideology, we do not think it willbe difficult for readers to see how this particularhypothesis might appeal to those with an ideologicalantipathy to concepts such as wealth redistribution.We have never suggested, nor do we believe, thatsuch a personal ideology motivates psychosocialtheorists, however it seems naı̈ve to ignore theinfluence this may have on the readiness of somepoliticians to embrace the psychosocial hypothesis.
The point is that we simply do not see thisessentially mono-causal psychosocial theory of thecauses of health inequalities as being congruent withthe evidence. The most heartening aspect of Adler’sresponse is her apparent acknowledgement that,even in developed societies, material conditions stillinfluence health, irrespective of the (quite under-standable) negative feelings that may be associatedwith material disadvantage. We agree, moreover wedo not think that psychosocial factors are irrelevant,though we remain sceptical (as discussed above)about their direct contribution to health inequalitiesthrough neuroendocrine mechanisms. Finally, itseems unfair that Adler takes us to task forsupposedly trying to ‘‘disprove the value of adifferent approach’’. We did not do this, we simplyassessed whether our evidence suggested a primacyof material or psychosocial determinants of healthin a particular population. This is precisely thestrategy that proponents of the psychosocial hy-pothesis have adopted for at least the past decade.(Adler, Epel, Castellazo, & Ickovics, 2000; Marmotet al., 1997; Singh-Manoux et al., 2005). In thislight, Adler’s apparent attempts to claim both the
moral and methodological high ground seemunjustified.
Acknowledgements
The work of Victor Hawthorne, Charles Gillis,David Hole and Pauline MacKinnon has providedus with the data required for this analysis. A grantwithin phase two of the Economic and SocialResearch Council’s, Health Variations researchprogramme allowed linkage to hospital admissiondata. JM is supported by a Career Scientist fellow-ship from the Department of Health. All viewsexpressed are those of the authors and notnecessarily of the Department of Health.
References
Adler, N.E. (2006). ‘‘When one’s main effect is another’s error:
Material vs. psychosocial explanations of health disparities. A
commentary on Macleod et al., ‘‘Is subjective social status a
more important determinant of health than objective social
status? Evidence from a prospective observational study of
Scottish men’’ (61: 9, 2005, 1916–1929)’’, in press.
Adler, N. E., Epel, E. S., Castellazo, G., & Ickovics, J. R. (2000).
Relationship of subjective and objective social status with
psychological and physiological functioning: Preliminary data
in healthy white women. Health Psychology, 19(6), 586–592.
Baumeister, R. F., Campbell, J. D., Krueger, J. I., & Vohs, K. D.
(2003). Does high self-esteem cause better performance,
interpersonal success, happiness or healthier lifestyles? Psy-
chological Science in the Public Interest, 4(1), 1–44.
Bosma, H., Marmot, M. G., Hemingway, H., Nicholson, A. C.,
Brunner, E., & Stansfeld, S. A. (1997). Low job control and
risk of coronary heart disease in Whitehall II (prospective
cohort) study. BMJ, 314(7080), 558–565.
Cannon, W. B., & De La Paz, D. (1911). The stimulation of the
adrenal gland by emotional excitement. JAMA, 56, 742.
Chandola, T., Brunner, E., & Marmot, M. (2006). Chronic stress
at work and the metabolic syndrome: Prospective study.
BMJ, 332(7540), 521–525.
Christenfeld, N. J., Sloan, R. P., Carroll, D., & Greenland, S.
(2004). Risk factors, confounding, and the illusion of
statistical control. Psychosomatic Medicine, 66(6), 868–875.
Heslop, P., Davey Smith, G., Carroll, D., Macleod, J., Hyland,
F., & Hart, C. (2001). Perceived stress and coronary heart
disease risk-factors: The contribution of socio-economic
position. British Journal of Health Psychology, 6, 167–178.
Honjo, K., Tsutsumi, A., Kawachi, I., & Kawakimi, N. (2006).
What accounts for the relationship between social class and
smoking cessation? Results of a path analysis. Social Science
& Medicine, 62(2), 317–328.
Hughes, J. R., Stead, L. F., & Lancaster, T. (2004). Antidepres-
sants for smoking cessation. Cochrane Database Systems
Review(4), CD000031.
Macleod, J., & Davey Smith, G. (2002). Stress and the heart: 50
years of progress? International Journal of Epidemiology, 31,
1111–1113.

ARTICLE IN PRESSJ. Macleod et al. / Social Science & Medicine 63 (2006) 851–857 857
Macleod, J., & Davey Smith, G. (2003). Psychosocial factors and
public health: A suitable case for treatment? Journal of
Epidemiology and Community Health, 57(8), 565–570.
Macleod, J., & Davey Smith, G. (2005). Job stress and breast
cancer risk: The nurses’ health study. American Journal of
Epidemiology, 162, 1–2.
Macleod, J., Davey Smith, G., Heslop, P., Metcalfe, C., Carroll,
D., & Hart, C. (2001). Are the effects of psychosocial
exposures attributable to confounding? Evidence from a
prospective observational study on psychological stress and
mortality. Journal of Epidemiology and Community Health,
55(12), 878–884.
Macleod, J., Davey Smith, G., Heslop, P., Metcalfe, C., Carroll,
D., & Hart, C. (2002). Psychological stress and cardiovascular
disease: Empirical demonstration of bias in a prospective
observational study of Scottish men. BMJ, 324(7348),
1247–1251.
Macleod, J., Davey Smith, G., Metcalfe, C., & Hart, C. (2005).
Effects of psychosocial factors in INTERHEART. Lancet,
365(9454), 118–119.
Marmot, M. G. (1998). Improvement of social environment to
improve health. Lancet, 351(9095), 57–60.
Marmot, M. G. (2005a). Discussion. In P. White (Ed.),
Biopsychosocial medicine: An integrated approach to under-
standing illness (p. 100). Oxford: OUP.
Marmot, M. G. (2005b). Social determinants of longevity and
mortality. Sage Crossroads, Rio, 28th June 2005 (http://
www.sagecrossroads.net).
Marmot, M. G., Bosma, H., Hemingway, H., Brunner, E., &
Stansfeld, S. (1997). Contribution of job control and other
risk factors to social variations in coronary heart disease
incidence. Lancet, 350(9073), 235–239.
Metcalfe, C., Davey Smith, G., Wadsworth, E., Sterne, J. A. C.,
Heslop, P., Macleod, J., et al. (2003). A contemporary
validation of the reeder stress inventory. British Journal of
Health Psychology, 8(pt 1), 83–94.
Muntaner, C., Eaton, W. W., Diala, C., Kessler, R. C., & Sorlie,
P. D. (1998). Social class, assets, organizational control and
the prevalence of common groups of psychiatric disorders.
Social Science and Medicine, 47(12), 2043–2053.
Nielsen, N. R., Zhang, Z. F., Kristensen, T. S., Netterstrom, B.,
Schnohr, P., & Gronbaek, M. (2005). Self reported stress and
risk of breast cancer: Prospective cohort study. BMJ,
331(7516), 548.
Rosengren, A., Hawken, S., Ounpuu, S., Sliwa, K., Zubaid, M.,
Almahmeed, W. A., et al. (2004). Association of psychosocial
risk factors with risk of acute myocardial infarction in 11119
cases and 13648 controls from 52 countries (the INTERHEART
study): Case-control study. Lancet, 364(9438), 953–962.
Selye, H. (1936). A syndrome produced by diverse nocuous
agents. Nature, 936, 138 32.
Singh-Manoux, A., Marmot, M. G., & Adler, N. E. (2005). Does
subjective social status predict health and change in health
status better than objective status? Psychosomatic Medicine,
67(6), 855–861.
Stansfeld, S. A., Fuhrer, R., Shipley, M. J., & Marmot, M. G.
(2002). Psychological distress as a risk factor for coronary
heart disease in the Whitehall II study. International Journal
of Epidemiology, 31(1), 48–255.
Susser, M. (2000). The technological paradox of health inequal-
ity, and a probe with a practical tool. Journal of Epidemiology
and Community Health, 54(12), 882–883.
Watson, D., & Pennebaker, J. W. (1989). Health complaints,
stress and distress: Exploring the central role of negative
affectivity. Psychological Review, 96(2), 234–254.
Watt, G. (2002). The inverse care law today. Lancet, 360(9328),
252–254.
Wright, E. O. (1987). Class boundaries and contradictory class
locations. In A. Giddens, & D. Held (Eds.), Classes power and
conflict (pp. 112–129). London: Macmillan.
Wright, E. O. (2000). Class counts. Cambridge: Cambridge
University Press.