Embed Size (px)
Citation preview

Br Heart J 1989;62:185-94
Subclinical cardiac dysfunction in acromegaly:evidence for a specific disease of heart muscle
ERWIN A RODRIGUES, MICHAEL P CARUANA, AVIJIT LAHIRI,J D N NABARRO,* HOWARD S JACOBS,* EDWARD B RAFTERY
From the Department of Cardiology and Division of Clinical Sciences, Northwick Park Hospital and Clinical
Research Centre, Harrow, and the *Middlesex Hospital, London
SUMMARY Acromegaly is associated with an increased cardiac morbidity and mortality, but it isnot clear whether this is the result of increased incidence of hypertension and coronary heartdisease or of a specific disease of heart muscle. Thirty four acromegalic patients were studied bynon-invasive techniques. Seven of these patients had raised plasma concentrations of growthhormone at the time of study; three were newly diagnosed and had not received any treatment.
Hypertension was present in nine (26%) but only three (9%) had electrocardiographic leftventricular hypertrophy. Echocardiography showed ventricular hypertrophy in 12 (48%) andincreased left ventricular mass in 17 (68%) patients. Holter monitoring detected importantventricular arrhythmias in 14 patients. Thallium-201 scanning showed evidence for coronary heartdisease in eight patients. Systolic time intervals were normal except when there was coexistentischaemic heart disease. A comparison between 19 acromegalic patients with no other detectablecause of heart disease and 22 age matched controls showed appreciably abnormal left ventriculardiastolic function in the group with acromegaly. The abnormalities shown did not correlate withleft ventricular mass or wall thickness. There was no difference in diastolic function betweenpatients with active acromegaly and those with treated acromegaly. Hypertensive acromegalicpatients had worse diastolic function than hypertensive controls, suggesting that hypertension mayfurther impair the left ventricular diastolic abnormality in acromegaly.This is the first study to find evidence of subclinical cardiac diastolic dysfunction in acromegaly
and it supports the suggestion that there is a specific disease of heart muscle in acromegaly.
While systemic hypertension, atherosclerosis, anddiabetes mellitus may contribute- to cardiovascularcomplications in acromegaly, cardiac failure hasoccurred in patients with acromegaly in the absenceof these and other established causes ofheart muscledisease.'" Such cases suggest the existence of aspecific disease of heart muscle in acromegaly. Post-mortem studies showed an "abnormal myocardium"in 59% of cases ofacromegaly and "definite myocar-ditis" in 26%,' suggesting that cardiac dysfunctionmay be more common than clinical examinationalone suggests. Although Jonas et al found abnormalsystolic time intervals in six of 10 patients with
Requests for reprints to Dr Edward B Raftery, Cardiology Depart-ment, Northwick Park Hospital, Watford Road, Harrow, MiddlesexHAI 3UJ.
Accepted for publication 7 March 1989
acromegaly,7 more recent studies with radionuclideangiography showed no abnormality of left ven-tricular systolic function unless other cardiac diseasewas present.89There is mounting evidence that radionuclide
measurements of diastolic function are more sen-sitive than measurements of ejection fraction, notonly in the detection and therapeutic assessment ofcoronary heart disease""2 but also in patients withleft ventricular hypertrophy, which produces ab-normal relaxation of the ventricle.""15 These non-invasive measurements ofdiastolic finction correlatewell with measurements obtained invasively at car-diac catheterisation."We used non-invasive methods to look for
evidence of a specific disease of cardiac muscle inpatients with acromegaly in whom other recognisedcauses had been excluded.
185
on July 19, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.3.185 on 1 S
eptember 1989. D
ownloaded from

186
Patients and methods
PATIENTSWe studied 34 consecutive patients with a firmdiagnosis of acromegaly. The diagnosis was based onclinical features and a resting, fasting serum concen-
tration of growth hormone of > 10 mU/l which was
not suppressed by a 50 g oral glucose load. Table 1summarises the clinical characteristics of thepatients. None of the patients had symptomaticischaemic heart disease or evidence of heart failure atthe time of study.
CONTROLSControl data were obtained from 22 healthy volun-teers with no history of cardiorespiratory disease.They were normotensive and had a normal physicalexamination, a normal resting electrocardiogram,and a negative maximal graded treadmill exercisetest. We compared radionuclide angiographic datafrom the age matched controls at rest and duringexercise with the data from the patients withacromegaly.
Rodrigues, Caruana, Lahiri, Nabarro, Jacobs, Raftery
ESSENTIAL HYPERTENSIONWe compared 14 age matched patients with essentialhypertension with the hypertensive acromegalicpatients. These 14 patients were symptom free, hadnormal electrocardiograms at rest and on exercise,normal wall motion on radionuclide angiography,and were on no medication at the time of the study.
CLINICAL ASSESSMENTWe took a detailed history from each patient beforephysical examination for clinical evidence ofischaemic heart disease, thyroid disease, excess
alcohol consumption, and concomitant illness. Drugmedication and the duration of acromegaly were
recorded. Blood pressure was measured twice withthe patients lying and standing and after five minutesof supine rest. Patients whose blood pressure was
> 160/95 mm Hg when they were lying down were
considered to have hypertension. Patients with a
history of hypertension who were on antihyperten-sive treatment were regarded as having hypertension,even if blood pressure readings at the time of theclinical assessment were < 160/95 mm Hg.
Table 1 Clinical details ofpatients with acromegaly
GrowthTime since Type of hormone
Patient No Age/sex Hypertension ECG treatment (yr) treatment concentration (mU/I)
1 56 F - N 6 HYP 1-72 48M + N 4 HYP,DXT 10-63 51 M - N 9 HYP 1-94 62M - N 12 HYP <1-95 63F + N 4 B 6-46 59M - RBBB 8 HYP,B <1.07 52 M - N 5 HYP 1-18 61 M - LBBB 6 B 2 79 37M - N 9 HYP 2-310 53M + LVH 8 HYP <1-011 64 F - N 5 HYP 8-312 65 F - N 8 HYP 5-913 49M - N 8 HYP <1.014 35 F - N 7 HYP,B 3-215 54M - N 11 HYP 1-616 66 F - N 12 B 8-617 62M - N 9 HYP <1-018 58M - N 10 HYP 1-719 41 F - N 12 HYP,DXT 4-320 60 F + N 5 HYP <1-021 56M - N 4 HYP 4-622 65 M + RBBB 6 B 4-023 64 F - N 10 HYP 4-724 42M - N 5 HYP <1-025 68M + LBBB 10 DXT 12-126 58 F - N 5 HYP 14-027 28 M + LVH 5 HYP 37-028 50 F - N Pre-op B 39-029 65 M - N 6 DXT,HYP 18-730 70 F + LVH Pre-op - 40-231 46M - N Pre-op - 41-132 72M - N 7 Nil 70-533 53M - N 14 HYP 22-434 64 F + N 12 HYP,B 15-8
B, bromocriptine; DXT, radiotherapy; HYP, hypophysectomy; N, normal; LBBB, left bundle branch block; RBBB, right bundle branchblock; LVH, left ventricular hypertrophy.
on July 19, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.3.185 on 1 S
eptember 1989. D
ownloaded from

Cardiac dysfunction in acromegaly
Blood was withdrawn for the measurement ofserum concentration of growth hormone, thyroidfunction tests, serum creatine kinase concentration,random blood glucose, and for liver function tests,including y-glutamyl transpeptidase.
ELECTROCARDIOGRAPHYA standard 12 lead electrocardiogram was performedon each patient and evidence of old myocardialinfarction, left ventricular hypertrophy, or conduc-tion abnormalities was sought. Patients then under-went a maximal, symptom limited, graded treadmillexercise test with a modified Chung protocol; thebipolar electrocardiographic leads CM5 and CC5were monitored during the test."7 Horizontal ordownsloping ST segment depression of > 1 mm at80 ms from the J point was regarded as evidence ofischaemia.
AMBULATORY ELECTROCARDIOGRAPHICMONITORINGTwenty four hour electrocardiographic monitoring(Oxford Medilog) was performed to detect rhythmdisturbances and the tapes were analysed with aReynolds Medical Pathfinder and visual supervision.
SYSTOLIC TIME INTERVALSWe measured systolic time intervals on a multi-channel Cambridge recorder at a paper speed of100 mm/s from simultaneous recordings of the elec-trocardiogram, carotid pulse tracing, and phono-cardiogram. We recorded high frequency phono-cardiograms with a piezoelectric microphonepositioned on the precordium to display optimallythe aortic component of the second heart sound.Carotid pulse tracings were obtained with a handheld funnel pick up that was air coupled to a crystaltransducer. The electrocardiographic lead showingthe earliest onset of the QRS complex was used formeasurements. A mean of three values for pre-ejec-tion period, left ventricular ejection time, and hencethe ratio were derived according to the methoddescribed by Weissler and Garrand.'8
THALLIUM-201 SCINTIGRAPHYAt symptom limited peak exercise a bolus of74 MBqthallium-201 was injected through an indwellingforearm venous cannula and exercise was continuedfor a further minute. Scintigrams were obtained inthe anterior, left anterior oblique, and lateral viewsand scanning was repeated 4-6 hours later with acardiac gamma camera (Elscint 215M) equippedwith a low energy, all-purpose collimator with anenergy window of 20% around the 80 keV photo-peak ofthallium-201. The scintigrams were reported"blind" by two trained observers without knowledge
187of the patient's clinical or laboratory findings. Aftersubtraction for background a region of interest wasplaced around the left ventricle and a semiquan-titative program was used to obtain counts from fivedifferent segments of the left ventricle. Segmentalperfusion abnormalities were classified as fixed orreversible according to previously establishedcriteria."'
Ischaemic heart disease was considered to bepresent if any of the following was present: (a)documented myocardial infarction; (b) angina pec-toris with ST/T wave abnormalities on a resting 12lead electrocardiogram; (c) presence of > 1 mmhorizontal or downsloping ST segment depression80 ms after the J point on exercise testing associatedwith the demonstration of a fixed or reversibleperfusion defect on thallium-201 scintigraphy; (d)reversible perfusion defect on thallium scintigraphyeven in the absence of significant ST segmentdepression on exercise testing.
ECHOCARDIOGRAPHYWe attempted to get a cross sectional echocardiogramin all patients with a Diasonics V-3400R real time,phased array imaging system coupled to a 2-5 MHztransducer. Scans were obtained in the standardviews in order to examine the aortic and mitralvalves. We then obtained a derivedM mode record-ing of the left ventricle at a paper speed of 25 mm/s,having adjusted the transducer to obtain optimalrecordings of both the interventricular septum andleft ventricular posterior wall. The M mode scan atthe level of the chordae tendineae was used tomeasure left ventricular end diastolic and end sys-tolic dimensions, and the thickness of the interven-tricular septal wall and left ventricular posterior wall.Mean values from three cardiac cycles were used forcalculation. From these values we calculated leftventricular mass using the formula of Devereux andReichek.Y
Analysis of the echocardiograms was carried outwithout knowledge of the clinical or laboratoryfindings.
RADIONUCLIDE VENTRICULOGRAPHYEquilibrium radionuclide ventriculography was per-formed at rest with individuals in the supine position,after in vivo labelling ofred blood cells with stannouspyrophosphate (Pyrolite) and 740 MBq of tech-netium-99m. Imaging was performed with a mobilegamma camera (Elscint Model 215M) in the leftanterior oblique (best septal) projection. Electrocar-diographic gating was used to collect and organise thedata into a series of32 frames for each cardiac cycle inorder to obtain a high resolution left ventriculartime-activity curve.
on July 19, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.3.185 on 1 S
eptember 1989. D
ownloaded from

188Cardiac cycles falling outside a pre-selected range
of acceptable cycle lengths were automaticallyexcluded from analysis by setting an RR triggeringtolerance of 5%; this prevented distortion of thetime-activity curve by variation in cycle length. Byexcluding long or short cycles, the portion of thetime-activity curve describing diastolic events wasaccurately preserved. Five million counts werecollected and the data were stored in a 64 x 64matrix on a dedicated computer. After nine pointsmoothing and time correction, left ventricularregions ofinterest were drawn by a computer derivedcounts based method. A second derivative edgedefining algorithm based on a Fourier and amplitudemodel was used to identify the left ventricularcontour in each of the 32 frames.' After backgroundsubtraction a high resolution time-activity curve wasdifferentiated and from the curve the point of peakfilling rate was identified. Exercise radionuclidestudies were performed in supine patients and volun-teers usingmethods described in detail elsewhere.2'-6
Global left ventricular systolic function was asses-sed by the ejection fraction, ejection rate, and ejectiontime. Peak filling rate, time to peak filling rate, earlyfilling rate, and first one third filling fraction wereused to describe left ventricular diastolic func-1ion112142A-26Each investigation was reported blindly by trained
observers without knowledge of the patient's clinicalor laboratory findings or the results ofthe other tests.The study was approved by the hospital ethics
committee and patients and volunteers gave writteninformed consent before participating. We used twotailed unpaired Student's t tests and linear regressionanalysis for statistical analysis.
Results
We studied 34 patients (21 men and 13 women, meanage 56 years (range 28-72)) with past or presentacromegaly. In seven plasma concentrations ofgrowth hormone were raised at the time of study.Other pituitary function was normal at the time ofstudy; however, seven were receiving steroidreplacement and three thyroxine replacementtherapy. Liver function tests were normal in allpatients. None had evidence of diabetes mellitus.Table 1 sunmarses the cardiovascular state of thepatients. Hypertension was present in nine (26%),none had electrocardiographic evidence of oldmyocardial infarction, and in only three (9%) wereRomhilt and Estes's electrocardiographic criteria'7for left ventricular hypertrophy fulfilled. All patientswere in sinus rhythm at the time ofstudy. There wereconduction abnormalities on the resting electrocar-diogram in four (12%). A total of 14 had evidence of
Rodrigues, Caruana, Lahiri, Nabarro, Jacobs, Rafteryhypertension or ischaemic heart disease or both. Onepatient (case 23) who had an inconclusive exercisetest and who did not undergo thallium scintigraphyor a wall motion study was excluded from analysis.
EXERCISE TESTINGOnly one patient stopped exercising because ofanginal pain. Fatigue was the end point in 17 andbreathlessness in 15. Five achieved the target heartrate and stopped because offatigue. Five had positiveST segment criteria for ischaemia but all ofthese hadnormal exercise and redistribution thallium-201scans and normal wall motion on radionuclide ven-triculography.
AMBULATORY ELECTROCARDIOGRAPHICMONITORINGArrhythmias were detected in 14 patients. The mostcommon finding was asymptomatic isolated ven-tricular extrasystoles. One of these patients (case 27)had prolonged asymptomatic episodes of ventricularbigeminy. In another patient runs of ventriculartachycardia were recorded, which were producingsymptoms of palpitation and dizziness (case 8). Thispatient had left bundle branch block on the restingelectrocardiogram, abnormal wall motion on radio-nuclide ventriculography, and a reversible perfusiondefect on thallium scintigraphy; it was thereforededuced that he had ischaemic heart disease. Twopatients (cases 13 and 25) had sinus pauses and in oneof these (case 13) asymptomatic pauses of up to 44seconds were recorded at night.
SYSTOLIC TIME INTERVALSAccording to the normal range (025-0-41) definedby Martins et al8 systolic time intervals were abnor-mal at rest in only three (9%); all had other evidenceofischaemic heart disease with dilated left ventricles.Systolic time intervals were only abnormal whenthere were other recognisable cardiac abnormalities.
THALLIUM-201 SCINTIGRAPHYExercise and redistribution thallium-201 imagingwas performed in 28 patients. There were fixedperfusion defects suggestive of myocardial scarringin four and reversible perfusion abnormalities werepresent in a further four patients (table 2).
ECHOCARDIOGRAPHYCross sectional and M mode echocardiography wasattempted in all patients, but adequate scans forcalculation of left ventricular mass could be obtainedin only 25. In the remaining nine patients onlyqualitative assessment of the echocardiograms waspossible. Valve abnormality was detected in only onepatient (case 12), whose echocardiogram indicated
on July 19, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.3.185 on 1 S
eptember 1989. D
ownloaded from

Cardiac dysfunction in acromegalythe presence of a thickened, sclerotic aortic valvewith mild stenosis. Left ventricular hypertrophy(wall thickness > 11 mm) was detected in 12 (48%).In one patient (case 30) concentric left ventricularhypertrophy was associated with systolic anteriormotion of the anterior mitral leaflet and calcificationof the posterior mitral annulus but there were no
other features to suggest hypertrophic cardio-myopathy. In another patient there was early systolicclosure of the aortic valve (case 34).There was no significant correlation between left
ventricular wall thickness and peak filling rate (r =
0 1,p = NSforseptalthickness; andr = 0 3,p = NSfor posterior free wall thickness). The left ventricularcavity was dilated in five patients and of these twohad other evidence of ischaemic heart disease. Theremaining three had no evidence of hypertension or
ischaemic heart disease. Increased left ventricularmass was detected in 17 (68%) of the patients by thecriteria (>200 g) of Mather et al.' No significantcorrelation was detected between the left ventricularmass and peak filling rate (r = - 0.3, p = NS).
189
RADIONUCLIDE VENTRICULOGRAPHYNineteen patients had no recognisable cause of heartdisease. None was receiving any cardioactive medica-tion at the time of study. The results of radionuclideventriculography in these patients were analysed indetail and compared with the results from 22 age
matched controls (table 3). None of these patientsdeveloped abnormalities of regional wall motion on
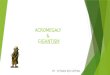
exercise. Resting systolic function was similar in boththe controls and the patients, but peak filling rates at
rest were significantly depressed in the patients (p <
0 005) despite comparable resting heart rates (fig 1).Mean exercise ejection fraction and ejection rate inthe two groups were similar, but ejection time andtime to peak filling rate were longer in the patients(p < 005 and p < 0-02 respectively). The sig-nificantly higher exercise heart rate in the controlsthan the patients (p < 0 01) could account for thisresult. The diastolic indices remained abnormal on
exercise in the patients. The change in mean ejectionfraction on exercise was + 4-1(8-4)% in the controlgroup and + 2-7 (10-0)% in the patients (p = NS).
Table 2 Results of exercise testing, echocardiography, thallium scintigraphy, and nuclear angiography
ExercisePatient No time (min) GXT result GXTsymptoms Thallium scan RNA WMA LV mass (g)
1 7-4 - SOB N 0 1552 13-7 + SOB N 0 2273 18-0 - F N 0 1994 8-8 + THR/F N 0 2915 8-4 - SOB N 0 2436 6-3 - SOB N 0 2147 17-9 - THR/F N/D N/D 1858 9 7 I/C SOB/VE R + -
9 13-4 - THR/F R 0 -10 9.9 + SOB N 0 19311 8-1 - F N 0 -12 N/D N/D N/D N 0 13913 18-8 - THR/F N 0 -14 14-0 - F N/D N/D 22815 15-7 - F N 0 33316 14-0 + SOB N 0 20717 17-9 - F N 0 25818 18-0 - F N 0 28719 12-3 - SOB N 0 26120 15-0 - F N/D 0 26121 10-8 - F N 0 -22 2-9 - SOB Fx + -23 2-1 I/C SOB N/D N/D -24 20-0 - THR/F N/D 0 23225 5-8 I/C F Fx + 59126 12-2 - F N 0 16727 13-2 - SOB N 0 24928 17-5 - SOB N/D 0 22929 8-4 - AP R + -30 1.0 I/C SOB R 0 18631 19-6 - F Fx 0 35332 4-1 - SOB Fx 0 36133 18-7 + F N 0 16034 9-5 I/C SOB N 0 -
WMA, wall motion abnormality; THR, target heart rate; SOB, shortness of breath; F, fatigue; I/C, inconclusive; R, reversible defect; Fx,fixed defect; N/D, not done; GXT, graded treadmill exercise test; AP, angina pectoris; N, normal angiography; VE, ventricularextrasystoles; RNA, radionuclide angiography.
on July 19, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.3.185 on 1 S
eptember 1989. D
ownloaded from

190RADIONUCLIDE VENTRICULOGRAPHY INHYPERTENSIVE ACROMEGALIC PATIENTSThe results of radionuclide ventriculography in thenine hypertensive acromegalic patients were com-pared with those in normal age matched normoten-sive controls and with 14 age matched patients withessential hypertension (table 4). Five of the hyper-tensive acromegalic patients were receiving f block-
Table 3 Results (mean (SD)) of radionuclideangiography in the 19 normotensive acromegalic patients andthe 22 age matched controls
Normotensiveand Controk v
Controls aromegalic acromegalics
Rest variables:Ejection fraction(%) 61(7) 61(10) NSEjection rate (EDV/s) 1-8 (0 3) 2-0 (0.5) NSEjection time (ms) 350 (41) 330 (57) NSPeak filling rate (EDV/s) 2-9 (0-4) 2-4(0 7) <0-005Early filling rate (EDV/s) 1-3 (0-4) 11 (0 5) NSTime to peak filling rate
(ms) 161(56) 193 (67) NSFirst one third filling
fraction 0-5 (0 2) 0 4 (0 2) NSHeart rate (bpm) 69 (10) 72 (9) NS
Exercise variables:Ejection fraction (%) 64 (9) 63 (9) NSEjection rate (EDV/s) 2-8 (0 7) 2-4 (0 4) NSEjection time (ms) 230 (46) 260 (30) < 0 05Peak filling rate (EDV/s) 5-7 (1-2) 4 9 (1-7) NSEarly filling rate (EDV/s) 2-7 (0-9) 2 5 (1-1) NSTime to peak filling rate
(ms) 121 (32) 155 (53) <0-02First one third filling
fraction 04(02) 03(01) NSHeart rate (bpm) 140(24) 121(16) <0-01
EDV, end diastolic volume.
Rodrigues, Caruana, Lahiri, Nabarro, Jacobs, Rafteryers and one was on calcium antagonists at the time ofstudy.
Resting ejection fraction was similar in the threegroups, as were resting ejection rate and ejectiontime. Mean (SD) resting peak filling rate in thenormal subjects was 2-9 (0 4) EDV/s. The essential
Controls
Acromegalic patients
T T Mean( SD)
Fig 1 Peak filling rate at rest and on exercise innormotensive patients with acromegaly and in age matchedcontrols. ED V, end diastolic volumes.'
Table 4 Results (mean (SD)) of radionuclide angiography in hypertensive acromegalic patients, patients with essentialhypertension, and age-matched controls
Controls EHT AHT(n = 14) (n = 14) (n = 9) CvEHT CvAHT EHTvAHT
Rest variables:Ejection fraction (%) 60 (6) 57 (8) 63 (9) NS NS NSEjection rate (EDV/s) 1-8 (03) 1-9 (0-3) 2-0 (0-6) NS NS NSEjection time (ms) 343 (46) 337 (54) 350 (77) NS NS NSPeak filling rate (EDV/s) 2-9 (0-4) 2-7 (0 8) 1-8 (0-5) NS <0-001 <0-01Early filling rate (EDV/s) 1-4 (0-5) 0-2 (0-2) 0-9 (04) <0-001 <0-02 <0-001Time to peak filling rate (ms) 152 (53) 168 (41) 237 (87) NS <0-01 <005First one third filling fraction 0-46 (0-25) 0-28 (0-17) 0-33 (0-17) <0-05 NS NSHeart rate (bpm) 70 (11) 82 (16) 62 (12) <0-05 NS <0-01Systolic blood pressure (mm Hg) 138 (16) 155 (21) 155 (25) NS NS NSDiastolic blood pressure (mm Hg) 85 (10) 102 (4) 94 (10) <0-001 NS NSAge (yr) 54 (8) 52 (8) 56 (15) NS NS NS
Exercise variables:Ejection fraction (°/) 64 (9) 63 (8) 58 (14) NS NS NSEjection rate (EDV/s) 2-6 (0-5) 2-7 (0-7) 2-0 (0-5) NS <0-05 <0-05Ejection time (ms) 246 (43) 234 (40) 290 (80) NS NS <0-05Peak filling rate (EDV/s) 5-3 (1-3) 5-0 (1-1) 3-3 (1-0) NS <0-005 <0005Early filling rate (EDV/s) 2-6 (0-9) 2-2 (1-2) 1-4 (0-7) NS <0-01 NSTime to peak filling rate (ms) 124 (34) 114 (34) 203 (59) NS <0-002 <0-001First one third filling fraction 0-41 (0-16) 0-44 (0-23) 0-2 (0-12) NS <0_001 <0-02Heart rate (bpm) 131 (21) 129 (19) 98 (19) NS <0.005 <0005
EHT, essential hypertensives; AHT, hypertensive acromegalic patients; C, controls; EDV, end diastolic volume.
on July 19, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.3.185 on 1 S
eptember 1989. D
ownloaded from

Cardiac dysfunction in acromegaly
[]ControlsPatients with essential hypertPat with c and
^
.
.-161
pc.O.005
I-,
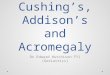
Fig 2 Peakfilling rate at rest and on exercishypertensive patients with acromegaly and incontrols and patients with essential hypertensidiastolic volumes.
hypertension group had a slightly lowrate (2.7(0.8) EDV/s, p = NS) but insive acromegalic patients the peak filsignificantly depressed (1-8(0.5) EDV/(fig 2). A similar abnormality was seen ifilling rate. The first one third fillingabnormal in the patients with essentialbut not in those with acromegaly andThe early filling rate was lower in bothgroups than in the controls.
COMPARISON BETWEEN ACTIVE ANDTREATED ACROMEGALYOfthe acromegalic patients studied, se'(> 10 mU/l) serum concentrations ofmone at the time ofstudy. The results oventriculography in this group were aresults from 13 patients whose gro'concentrations were well within the(< 10 mU/l) at the time of the study. ]
difference in either systolic or diastolicdetected between these groups althougfilling rate was slightly lower in patiendisease (2 0(0 9) EDV/s) than in tre(2.2(0.8) EDV/s) p = NS).
Discusion
Cardiac hypertrophy, "cardiomyopatigestive cardiac failure have been descril
191as one third of patients with acromegaly' but thepathophysiology ofcardiac dysfunction in this condi-
tension tion remains unclear.79 In this study there wasteogjon evidence of hypertension in 26% of patients, which
accords with other reported series, as did thefrequency of ischaemic heart disease.6`9 Cardiac
05 dysfunction in acromegaly has been attributed tothese known causes of heart disease.9 No previousstudy, however, has excluded coronary artery disease
Mean C SD) and hypertension from the study population. Wehave attempted to do this using a combination ofelectrocardiography, exercise testing, and stressthallium-201 scintigraphy.Using electrocardiography alone, we detected left
ventricular hypertrophy by Romhilt and Estes's* criteria' in only three (9%) of our patients. ButI electrocardiography has limitations for detecting
ventricular hypertrophy in these patients, becauseacromegaly results in a considerable alteration in the
* shape ofthe chest wall with an increase in anteropos-terior diameter and hence greater than normal elec-
w in trical insulation of the heart from surface electrodes.age-matched When it is technically feasible, echocardiographyion. EDV, end overcomes these difficulties and in this study there
was evidence of left ventricular hypertrophy in 48%and an increased left ventricular mass in 68%.
rer peak filling Similar results were reported by others.'the hyperten- In five (15%) the exercise test was positive by STlling rate was segment criteria but in all of them thallium-201is, p < 0-001) scintigraphy was normal. A previous study from ourin time to peak department showed that positive exercise tests ing fraction was patients with left ventricular hypertrophy are inac-hypertension curate predictors of coronary artery disease unlesshypertension. thallium-201 scintigraphy is also abnormal.3' Quan-hypertensive titative thallium-201 imaging is well established and
has been shown to be a highly sensitive technique fordetecting underlying coronary artery disease.9 31Harris et al have also reported false positive exercisetests in patients with left ventricular hypertrophy
Yen had raised and angiographically normal coronary arteries.32r growth hor- Because angina or wall motion abnormalities did notf radionuclide develop in any of these acromegalic patients duringompared with exercise radionuclide angiography, these positivewth hormone exercise test results in conjunction with negativenormal range thallium-201 scans make it unlikely that obstructiveNo significant disease was present in the large coronary arteries.function was Cardiovascular morbidity is more common inh resting peak acromegaly.Y While cardiac failure may be responsi-its with active ble for this, some workers reported an increased:ated patients incidence of arrhythmias in these patients.5 In our
series, 14 of the 34 patients had arrhythmias. Onepatient had several episodes of symptomatic ven-tricular tachycardia, but this patient undoubtedlyhad ischaemic heart disease and this was probably
hy", and con- the cause of the arrhythmia. Thirteen patients hadbed in asmany frequent ventricular extrasystoles and in one patient
on July 19, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.3.185 on 1 S
eptember 1989. D
ownloaded from

192
there were long periods of asymptomatic ventricularbigeminy. Arrhythmia was also more in patients withleft ventricular hypertrophy and strain in thepresence of normal coronary arteries," a finding thatmay also be applicable to acromegalic patients.
Others have used systolic time intervals to studypatients with acromegaly, with conflicting results.Jonas et al studied 10 patients and showed anabnormally high PEP/LVET (pre-ejection phase/left ventricular ejection time) ratio in six7-but fivepatients had hypertension, one had thyrotoxicosis,and one had diabetes mellitus. Furthermore, coro-nary heart disease was excluded by history andphysical examination alone, without exercise testingor thallium-201 scintigraphy. Because it is wellrecognised that an increased PEP/LVET ratio mayoccur in patients with congestive cardiac failure,hypertension, and various myocardial diseases, thedemonstration of an abnormality in this group ofpatients does not necessarily imply that impairedsystolic function was caused by acromegaly. Martinset al studied 16 patients and found an abnormallyhigh PEP/LVET in three with concomitant angina orhypertension.8 Only one other patient, in whomcoronary artery disease and hypertension had beenexcluded, showed abnormal systolic time intervals.Similarly, four of the 23 patients studied by Matheret al had high PEP/LVET ratios.'8 In three of these,causes other than acromegaly were clearly impli-cated. Our findings accord with those of Martins etal8 and Mather et al8 because an abnormal PEP/LVET ratio was only detected in patients with co-existing coronary heart disease. Systolic timeintervals, however, are not as sensitive or specificas radionuclide angiography for assessing cardiacfunction34 and it is therefore unlikely that subtlesubclinical cardiac dysfunction would be detected bythis method.Most workers used echocardiography for assessing
left ventricular function.83s 3' This technique isinsensitive because of the assumptions necessary tocalculate ejection fraction.'7 Furthermore, any errorsin measuring wall thickness and cavity size areexaggerated when these values are used to derivevolumes. It is now generally accepted that radio-nuclide angiography is a more accurate method ofassessing left ventricular function. In two previousstudies, patients with acromegaly were investigatedby radionuclide angiography," and in neither wascardiac dysfunction shown unless coexisting hyper-tension or ischaemic heart disease was present. Onlyleft ventricular ejection fraction (systolic function)was measured, however. Our results accord withthese studies in that we were unable to detect anyabnormality of systolic function in acromegalicpatients who had no evidence of other cardiacdisease.
Rodrigues, Caruana, Lahiri, Nabarro, Jacobs, RafteryLeft ventricular diastolic function has not
previously been studied in acromegaly. Severalworkers have suggested that diastolic filling is moresensitive than ejection fraction for assessing earlyimpairment ofcardiac function, not only in ischaemicheart disease'°0 but also in other conditions such ashypertrophic cardiomyopathy" and hypertension.'4In our study there was a highly significant differencein resting peak filling rate between controls andpatients with acromegaly. The diastolic peak fillingrate was reduced and the time to peak filling rate wasprolonged, indicating impaired diastolic relaxation.Diastolic indices remained abnormal on exercise.This abnormality of diastolic filling was apparenteven in those acromegalic patients in whom hyper-tension and ischaemic heart disease were excluded.
Altered diastolic relaxation may be caused byabnormalities in the active energy-dependent relaxa-tion process as is the case in patients with acutemyocardial ischaemia,"'l2 or by an increase in thevisco-elastic properties of the left ventricle as occursafter myocardial infarction.3839 While the increasedleft ventricular mass seen in acromegaly may reducecompliance, this factor is unlikely to be solely respon-sible for our findings, because there was no correla-tion between diastolic filling variables and left ven-tricular wall thickness or left ventricular mass. Lieand Grossman showed mononuclear cell infiltrate ormyocarditis in up to 59% of cases of acromegaly.'Hejmancik et al also reported increased interstitialfibrosis in acromegaly.3 It is not known whether thefinding of an inflammatory reaction relates to theactivity of the acromegaly with fibrosis representing"healing" once the condition is treated. Although wefound no difference in diastolic dysfunction betweenactive and treated acromegaly, the reduced peakfilling rate detected in our study may well reflectthese histological abnormalities, which would beexpected to increase ventricular stiffness and reducecompliance. Our study therefore adds clinical sup-port to the necropsy evidence for a specific heartmuscle disease in acromegaly.
Furthermore, acromegalic patients with coexistenthypertension showed greater depression of diastolicfunction than age and blood pressure matchedpatients with essential hypertension, suggesting thathypertension may be less well tolerated when thereare underlying acromegalic changes in the myocar-dium; this factor may contribute to the increasedfrequency of clinical cardiac disease in acromegaly.Some of the hypertensive acromegalic patients in ourstudy, however, were receiving f blockers and abnor-malities of peak filling rate may have been exag-gerated by the negative chronotropic properties ofthese agents. Early therapeutic intervention withaddition of calcium antagonists may improve thediastolic abnormalities detected.'5 I
on July 19, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.3.185 on 1 S
eptember 1989. D
ownloaded from

Cardiac dysfunction in acromegaly 193We found evidence of subclinical cardiac dysfunc-
tion in acromegaly in the absence of other knowncauses ofheart disease and our findings are consistentwith the histological abnormalities previously shownin the hearts of patients with acromegaly.
We thank Mrs Gill Clarke and Mr David Hinge fortheir invaluable assistance with the technical andstatistical aspects of this study and Dr R Himsworthand Dr R Clayton (Endocrinology Department,Northwick Park Hospital) for allowing us to studytheir patients.
References
1 Pepine CJ, Aloia J. Heart muscle disease in acromegaly.Am JMed 1970;48:530-4.
2 Courville CB, Mason VR. The heart in acromegaly.Arch Intern Med 1938;61:704-13.
3 Hejmancik MR, Bradfield JY, Hermann GR.Acromegaly and the heart; a clinical and pathologicstudy. Ann Intern Med 1951;34:1445-56.
4 McGuffin WL, Sherman BM, Roth J, et al. Acromegalyand cardiovascular disorders. A prospective study.Ann Intern Med 1974;81: 11-8.
5 Rossi L, Thiene G, Caregaro L, Giordano R, Lauro S.Dysrhythmias and sudden death in acromegalic heartdisease. A clinicopathologic study. Chest 1977;72:495-8.
6 Lie JT, Grossman SJ. Pathology of the heart inacromegaly: anatomic findings in 27 autopsiedpatients. Am Heart J 1980;100:41-52.
7 Jonas EA, Aloia JF, Lane FJ. Evidence of subclinicalheart muscle dysfunction in acromegaly. Chest 1975;67:190-4.
8 Martins JB, Kerber RE, Sherman BM, Marcus ML,Ehrhardt JC. Cardiac size and function inacromegaly. Circulation 1977;56:863-9.
9 O'Keefe JC, Grant SJ, Wiseman JC, et al. Acromegalyand the heart-echocardiographic and nuclear imagingstudies. Aust NZ JMed 1982;12:603-7.
10 Bonow RO, Bacharach SL, Green MV, et al. Impairedleft ventricular diastolic filling in patients with coro-nary artery disease: assessment with radionuclidecineangiography. Circulation 1981;64:315-23.
11 Rodrigues EA, Lahiri A, Raftery EB. An objective non-invasive method for detecting early diastolic dysfunc-tion in patients with coronary artery disease [Abs-tract]. Br Heart J 1986;55:511.
12 Rodrigues EA, Lahiri A, Raftery EB. Improvement indiastolic dysfunction in ischaemic heart disease aftertreatment with calcium antagonists [Abstract]. ClinSci 1986;70(suppl 13):6.
13 Qureshi S, Wagner HN, Alderson PO, et al. Evaluationof left ventricular function in normal persons andpatients with heart disease. J Nucl Med 1978;19:135-41.
14 Inouye I, Massie B, Loge D, et al. Abnormal leftventricular filling; an early finding in mild tomoderate hypertension. Am J Cardiol 1984;53:120-6.
15 Bonow RO, Rosing DR, Bacharach SL, et al. Effects ofverapamil on left ventricular systolic function and
diastolic filling in patients with hypertrophic car-diomyopathy. Circulation 1981;64:787-96.
16 Magorien DJ, Shaffer P, Bush C, et al. Haemodynamiccorrelates for timing intervals, ejection rate and fillingrate derived from the radionuclide angiographicvolume curve. Am J Cardiol 1984;53:567-71.
17 Rodrigues EA, Lahiri A, Hughes LO, Kohli RS,Whittington JR, Raftery EB. Anti-anginal efficacy ofcarvedilol, a beta-blocker with vasodilating activity.Am J Cardiol 1986;58:916-21.
18 Weissler AM, Garrand CL. Systolic time intervals incardiac disease. Mod Concepts Cardiovasc Dis1971;40:1-8.
19 O'Hara MJ, Lahiri A, Whittington JR, Crawley JCW,Raftery EB. Detection of high risk coronary arterydisease by thallium imaging. Br Heart J 1985;53:616-23.
20 Lahiri A, Zanelli GD, O'Hara MJ, et al. Simultaneousmeasurement ofleft ventricular function and myocar-dial perfusion during a single exercise test: dualisotope imaging with gold-195m and thallium-201.Eur Heart J 1986;7:493-500.
21 Lahiri A, O'Hara MJ, Bowles MJ, Crawley JCW,Raftery EB. Influence of left ventricular function andseverity of coronary artery disease on exerciseinduced pulmonary thallium-201 uptake. Int J Car-diol 1984;5:475-90.
22 Devereux RB, Reichek N. Echocardiographic deter-mination of left ventricular mass in man: anatomicvalidation of the method. Circulation 1977;55:613-8.
23 Adam WE, Tarkowska A, Bitter F, Stauch M, GeffersH. Equilibrium (gated) radionuclide ventriculo-graphy. Cardiovasc Radiol 1979;2:161-73.
24 Rodrigues EA, Lahiri A, Raftery EB. Improvement inleft ventricular diastolic function in patients withstable angina after chronic treatment with verapamiland nicardipine. Eur Heart J 1987;8:624-9.
25 Lahiri A, Rodrigues EA, Al-Khawaja IM, Raftery EB.Effects of a new vasodilating beta-blocking drug(Carvedilol) on left ventricular function in stableangina pectoris. Am J Cardiol 1987;59:769-77.
26 Hains ADB, Al-Khawaja I, Hinge DA, Lahiri A,Raftery EB. Radionuclide left ventricular ejectionfraction: a comparison of three methods. Br Heart J1987;57:242-6.
27 Romhilt DW, Estes EH. A point-score system for theECG diagnosis of left ventricular hypertrophy. AmHeart J 1968;75:752-8.
28 Mather HM, Boyd MJ, Jenkins JS. Heart size andfunction in acromegaly. Br Heart J 1979;41:697-701.
29 Wright AD, HillDM, Lowy C, FraserTR. Mortality inacromegaly. QJ Med (new series) 1970;39:1-16.
30 Heber ME, Caruana MP, Brigden G, Clarke G, LahiriA, Raftery EB. Diagnosis of chest pain in hyper-tensive patients [Abstract]. Clin Sci 1987;72(suppl16):8P.
31 Lahiri A. Myocardial perfusion scintigraphy with singlephoton radionuclides. Current Opinion Cardiol 1986;1:926-32.
32 Harris CN, Aronow WS, Parker DP, Kaplan MA.Treadmill stress test in left ventricular hypertrophy.Chest 1973;63:353-7.
33 McLenachan JM, Hendeson E, Dargie HJ. Arrhyth-
on July 19, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.3.185 on 1 S
eptember 1989. D
ownloaded from

194 Rodrigues, Caruana, Lahiri, Nabarro, Jacobs, Rafterymias in the presence of left ventricular hypertrophyand strain and normal coronary arteries [Abstract].Clin Sci 1986;71(suppl 15):56P.
34 Braunwald E, Rose J, Sonnenblick EH. Mechanisms ofcontraction of the normal and failing heart 2nd ed.Boston: Little Brown, 1976.
35 Smalhridge RC, Rajfer S, Davia J, Schaaf M.Acromegaly and the heart. An echocardiographicstudy. Am JMed 1979;66:22-7.
36 Savage DD, Henry WL, Eastmen RC, Borer JS,Gorden P. Echocardiographic assessment of cardiacanatomy and function in acromegalic patients. Am JMed 1979;67:823-9.
37 Feigenbaum H. Echocardiography. 2nd ed. Philadel-phia: Lea and Febiger, 1979.
38 Diamond G, Forrester JS. Effect of coronary arterydisease and acute myocardial infarction on left ven-tricular compliance in man. Circulation 1972;45:11-9.
39 Rodrigues EA, Lahiri A, Hinge DA, Raftery EB. Leftventricular diastolic function in patients with chronicstable angina: comparison with normal subjects. AmJNomnvas Cardiol 1988;244-54.
40 Hughes LO, Lahiri A. Improvement in indices ofmyocardial ischaemia in a case of hypertrophic obs-tructive cardiomyopathy treated with verapamil. NuclMed Commun 1987;8:177-82.
on July 19, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.3.185 on 1 S
eptember 1989. D
ownloaded from