-
8/13/2019 Overt and Subclinical Hypothyroidism
1/18
THER PY IN PR CTICE Drugs 2012; 72 1) ; 17-330012.6667/12/
X)01.0017/S66.5S/0
2012 Adis Data information BV. Aii rights r e se rved .
Overt and Subclinical ypothyroidismWho to Treat and How
eepak Khandelwal an d Nikhil Tandon
Department of Endocrinology and Metabolism, All India Institute
of Medical Sciences, New Delhi, India
Contents
Abstract 171. Introduction 182. Epidemiology and Aetioiogy
19
2.1 Prevaience ot Overt and Subclinicai Hypothyroidism 192.2
Natural History of Subciinicai Hypothyroidism 192.3 Causes 19
3. Ciinicai Features and Diagnosis 194. Who to Treat 20
4.1 Overt Hypothyroidism 204.2 Subciinicai Hypothyroidism with
Thyroid-Stimuiating Hormone TSH) >10miU/L 21
4.3 Subciinicai Hypothyroidism with TSH
-
8/13/2019 Overt and Subclinical Hypothyroidism
2/18
18 Khandelwal Tando
concentration in the presence of normal serum free thyroxine
(T4) a
triiodothyronine (T3) concentrations. Subclinical hypothyroidism
may pgress to overt hypothyroidism in. approxima tely 2-5 cases
annually. patients with overt hypothyroidism and subclinical
hypothyroidism wTSH >10mIU/L should be treated. There is
consensus on the need to trsubclinical hypothyroidism of any
magnitude in pregn ant wom en and w omwho are contemplating
pregnancy, to decrease the risk of pregnancy coplications and
impaired cognitive development of the offspring. Howevcontroversy
remains regarding treatm ent of non-pregn ant a dult patients
wsubclinical hypothyroidism and serum TSH values 85 years. Other
pituitary hormones should be evuated in patients with central
hypothyroidism, especially assessment of thypothalam
ic-pituitary-adrenal axis, since hypocortisolism, if present, neeto
be rectified prior to initiating thyroid hormone replacement.
Levothyroxine (LT4) monotherapy remains the current standard
fmanagement of primary, as well as central, hypothyroidism.
Treatment cbe started with the full calculated dose for most young
patients. Howevtreatme nt should be initiated at a low dose in
elderly patien ts, patients w
coronary artery disease and patients with long-standing severe
hypothroidism. In primary hypothyroidism, treatment is monitored
with seruTSH, with a target of 0.5-2.0mlU/L. In patients with
central hypothyroism, treatment is tailored according to free or
total T4 levels, which shouldmaintained in the upper half of the
normal range for age. In patients wpersistently elevated TSH
despite an apparently adequate replacement doof LT4, poor
compliance, malabsorption and the presence of drug intertions
should be checked. O ver-replacement is comm on in clinical
practice ais associated with increased risk of atrial fibrillation
and osteoporosis, ahence should be avoided.
. I n t roduc t ion inadequate thyrotropin-releasing horm one
(Trelease from the hypothalamus (tertiary h
Hy poth yroid ism is a con dition in which the thyroid ism ). In
clinical practice it is no t thyroid gland is unable to make
adequate am ounts possible to discrim inate between secondaryof
thyroid hormo ne to meet the requirements of tertiary hypothy
roidism, which are conseqperip heral tissues. In prim ary hypothy
roidism , often referred to as 'centra l hypo thyroidicharacterized
by failure of the thyroid g land itself Primary hypothyroidism is
the aetiology ina fall in serum con centra tions of thyroid ho rm
one proxim ately 99 of cases of hypothyroidcauses an increased
secretion and elevation of serum Th e term subc hnica l hy po thy
roi dis m is u
thyroid-stimulating horm one (TSH) conce ntra- define that grade
of primary hypothyro idtions. Dec reased thyro idal secretion of
thyro id which there is an elevated TS H con cen traho rm on e can
also be caused by insufficient sti the presence of norm al serum
free thyroxin
-
8/13/2019 Overt and Subclinical Hypothyroidism
3/18
Overt and Subclinical Hypothyroidism 19
nnually.' ] The term myxoedema is now usually
eserved for cases of overt hypothyroidism thatre severe or
complicated, or both.'^'
In this review, we predominantly discuss andnform regarding
issues pertaining to primary hy-othyroidism in young healthy
adults. Wheneverecessary, distinctive aspects of the
pathogenesis,linical profile and management of primary
hy-othyroidism in other special populations and ofentral
hypothyroidism is discussed separately.
2 Epidemiology a nd Aetioiogy
2.1 Prevalence of O vert an d SubclinicalHypothyroidism
Primary hypothyroidism, which is widely pre-alent worldwide, is
more common in womenhan men and increases in incidence with
age,specially after the onset of middle age. The pre-alence of
spontaneous overt hypothyroidism isetween 1 and 2% and ten times
more commonn women than in men, while approximately 8%f women and
3% of men have subcUnical hy-othyroidism.'^1 Community studies of
elderlyeople have found a higher prevalence of hy-oth yroid ism:
app roxim ately 10% of the subjectsged >60 years had serum TSH
values above theormal
2.2 Natural History of Subclinical
HypothyroidismIn a follow-up study of the Whickham Sur-
vey,f'*l a population-based study in northernEngland, women who
had both high serum TSHand anti-thyroid antibody concentrations
devel-oped overt hypothyroidism at an annual rate of4.3%, com pared
with 2.6% and 2 .1% in womenwho had only high serum TSH
concentrations oronly elevated anti-thyroid antibody
concentra-tions, respectively. Subsequent studies have alsoreported
that subjects with higher baseline serumTSH values and/or elevated
anti-thyroid anti-bodies have a higher propensity to progress
toovert h ' ^ ^ l
2.3 Causes
The causes of hypothyroidism are sum marizedin table I.
3 Ciinicai Features and Diagnosis
Symptoms are generally related to the durationand severity of
hypothyroidism, and the rapiditywith which hypothyroidism occurs.
Presenting signs,symptoms and laboratory findings of
hypothyroid-ism are summarized in table II. The clinical
mani-festations of hypothyroidism are characterized by
able I Causes of hypothyroidismii
rimary hypothyroidism Central hypothyroidismoss of functional
thyroid tissueHashimoto s thyroiditisSurgical removal of the
thyroidRadioiodine ablation, external irradiation of the
thyroidSilent and postpartum thyroiditisCytokine-induced
thyroiditisInvasive fibrous thyroiditisThyroid infiltration
(amyloidosis, haemochromatosis,sarcoidosis, scleroderma,
cystinosis, primary thyroid lymphoma)Thyroid dysgenesis
unctional defects in thyroid hormone biosynthesis and
releaseIodine deficiency and iodine excess
Thyroid hormone biosynthetic defectDrugs: antithyroid agents,
lithium, amiodaron e, tyrosine kinase inhibitors (e.g.sunitinib),
ethionamide, sulphonamides, goitrogenic chemicals, thalidomide
Pituitary or hypothalamic neoplasmsTrauma (surgery, head
injury)RadiationIschaemic necrosis (postpartum
pituitaryinfarction/Sheehan s syndrome, sev ere shock,diabetes
meilitUs)Vascular (haemorrhage, aneurysm of internal
carotidartery)Infections (abscess, tuberculosis,
syphilis,toxoplasmosis)Infiltrative disorders (sarcoidosis,
histiocytosis,haemochromatosis)Lymphocytic hypophysitisDrugs
(bexarotene)Set point diseases (infants born to mothers w ith
poorly
-
8/13/2019 Overt and Subclinical Hypothyroidism
4/18
20
Table II Presenting symptoms,
Symptoms
signs and laboratory findings of hypothyroidism'^ ''^'
Signs
handelwal Tan
Laboratory/radiological findings
ExhaustionSomnolenceSlow cognitionEm otional labilityIntolerance
to coldConstipationDepressionWeight gainMyalgiaMuscle crampsCalf
stiffness
Growth failurePubertal delaySexual dys
functionMenorrhagiaMenstrual irregularityImpaired
fertilityParesthesiaHearing impairmentHoarseness of voice
Coarsening of facial featuresPuffiness below the eyesDry, thin
and pale skinCoarseness or loss of
hairMacroglossiaGoitreHypothermiaBradycardiaDiastolic
hypertensionSlow relaxation of tendon reflexesPleural effusion
Pericardial effusionAscitesNon-pitting oedema of lower
legAtaxiaGalactorrhoeaSleep-disordered breathing
HyponatraemiaHypercholesterolaemiaAnaemiaElevated serum creatine
kinaseHyperprolactinaemiaHyperhomocysteihaemiaElevated serum
carcino-embryonic antigen Epiphyseal dysgenesisDelayed bone
agePituitary gland enlargement
either slowing of body functions or consequent
to accumulation of glucosaminoglycans in thetissues. No single
symptom/sign is a very sensitiveor specific indicator of the
presence of hypothy-roidism. However, presence of multiple
symp-toms, particularly if recent in onset, increases thelikelihood
of hypothyroidism.t'^1 There are certainsymptoms or signs (e.g.
presence of a goitre orshort stature in children) that should
alwaysprompt a thyroid function test to rule out
possiblehypothyroidism.I'^l
As me ntione d in section 1, prim ary hyp othy -roidism is the
aetiology in mo re tha n 99 cases ofhypothyroidism, thereby making
serum TSHme asure me nt the best single test for the exclusionor
detection of hypothyroidism in most clinicalsettings. Raised serum
TSH concentrations iden-tify primary hypothyroidism irrespective of
thecause or severity. If the TSH level is high, furthermeasurement
of the serum free T4 should becarried out. A low serum free T4 in
conjunctionwith an elevated serum TSH level establishes a
diagnosis of overt hypothyroidism, while in sub-clinical
hypothyroidism the serum free T4 con-
t ti i b d fi iti l H
elevated o r inappropriately norm al in the pres
of low serum T4 values. In patients suspectehaving central
hypothyroidism, measuremenfree T4 is the test of choice. Measuring
total Talso acceptable, provided there are no alterain binding
proteins.
Once the diagnosis of prima ry hypothy roiis made, additional
imaging or serological teis unnecessary if the thyroid gland is
normaexamination.[' '*1 Measurement of anti-thyperoxidase (TPO )
antibodies is a valuable adin the evaluation of patients with
subclinhypothyroidism because it predicts a higher of developing
overt hypothyroidism. In patwith central hypothyroidism,
measuremenother pituitary hormones and imaging ofsellar-suprasellar
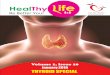
are a is required. La bor aevaluation of a patient with suspected
hyporoidism is summarized in figure 1.
4 Who to Treat
4.1 Overt Hypothyroidism
P i i h h h idi h
-
8/13/2019 Overt and Subclinical Hypothyroidism
5/18
vert and Subclinical H ypothyroidism 21
o confirm the results with a second sample. ^^ In-ividuals with
some conditions, e.g. recovery phasef thyroiditis or drug-induced
hypothyroidism mayeed temporary thyroxine replacement to
ensureuthyroidism until recovery is complete.
4,2 Subclinical Hypothyroidism withThyroid-Stimulating Hormone
TSH) >10mlU/L
In the last few years, there have been severalublications
regarding subclinical hypothyroid-
sm and its clinical relevance that have provokedebate about its
screening and treatment. Becausef the difficulties in interpreting
data from manyifferent sources, in 2002 the American Associa-on of
Clinical Endocrinologists (AACE), The USndocrine Society and the
American Thyroid As-ociation (ATA) convened a panel to propose
evi-ence-based guidelines on diagnosis, screening an d
treatment of subclinical hypothyroidism. The panelfound good
evidence that subclinical hypothy-roidism is associated with
progression to overt hy-pothyroidism, and fair evidence that serum
TSHlevels >10mIU/L are associated with elevations intotal and
low-density lipoprotein cholesterol levels.However, there was
insufficient evidence regardingan association between subclinical
hypothyroidismand adverse cardiac events, cardiac
dysfunction,neuropsychiatrie symptoms or systemic symptomsof
hypothyroidism .t
The Panel recommended that patients with anelevated serum TSH
level have the test repeated,along with a serum free T4 (FT4)
measurement,within 2-12 weeks. When repeat studies
confirmsubclinical hypothyroidism, further evaluation isrequired,
including clinical assessment of signsand symptoms of
hypothyroidism, ascertainmentof previous treatment for
hyperthyroidism (e.g.
Signs and symptoms suggestive of hypothyroidism
Serum TSH
Low Normal
Serum Fr4
High
Low suspicion ofhypothyroidism
Strong suspicionof hypotfiyroidism
Low Normal
Central hypothyroidism
No further test
Evaluate for causesof suppressed TSH
Serum FT4
Low Normal
Serum FT4Overt primary
hypothyroidismSubclinical
hypothyroidism
MRI sellaEvaluation of otherpituitary hormones
Low Normal
Check anti-TPOantibody
-
8/13/2019 Overt and Subclinical Hypothyroidism
6/18
22 Khandelwal Tando
radiotherapy, partial thyroidectomy), presence of
thyromegaly and family history of thyroid disease.In addition,
these patients should be screened forhyperlipidaemia. The Consensus
Expert Panel rec-ommended that treatment was reasonable forpatients
with TSH levels >10mIU/L, as thesepatients also have a higher
rate of progression toovert hypothyroidism.''* Most other
guidelinesand expert views also recommend treatment ofsubclinical
hypothyroid patients with TSH levels
Primary hypothyroidism |
4.3 Sub clinicai Hyp othyroidism with TSH
-
8/13/2019 Overt and Subclinical Hypothyroidism
7/18
Overt and Subclinical H ypothyroidism
nd 30 g of this is prod uce d daily in he althy
dults, 80% arising from the 5'-deiodination ofT4 in periphera l
tissues and 20% secreted d irectlyrom the thyroid.P"^' Thyroid
hormone prepara-ions available for treatment of hypothyroidismre
levothyroxine sodium (L-thyroxine [LT4]),iothyronine sodium
(L-triiodothyronine [LT3])
and desiccated thyroid.
5.1 Levoth yrox ine Sodium L-thyrox ine, LT4)
LT4 is synthetically produced but identical to
T4 secreted by the thyroid. LT4 is the preferreddrug because its
administration closely mimicsglandular secretion and its conversion
to T3 isappropriately regulated by tissues, maintainingts steady
and a deq uate supply.^'' Its long half-life
of 7 days allows single daily dose administrationand results in
only small fluctua tions in serumconcentrations between the daily
doses. Omissionof a single day's dose has little clinical
relevanceand the patient may safely take an omitted tablet
he following day. Moreover, titration of dose iseasy, because of
availability of multiple tabletstrengths. LT4 is primarily absorbed
in the jeju-num, and absorption is greater in the fasting80%) than
in the fed state (60%).P^l Non-specific
absorption of LT4 by dietary fibre has beenshown to decrease the
bioavailability of LT4,necessitating a h igher dose in patients
with a highntake of dietary fibre. Serum T4 concentrations
peak 2-4 hours after an oral dose and remainabove normal for
approximately 6 hours inpatients receiving daily replacement
therapy.'^^1The LT4 content of tablets is standardized
byhigh-pressure liquid chromatography and, theUS FDA currently
requires all LT4 preparationso contain 95-105% of the stated
amount.^^'
Generic and brand-name LT4 preparat ions aremostly
bioequivalent, but altered bioavailabilityhas been reported due to
changes in the formula-tion of preparations. Hence, it is not
advisable toalter the bran d during long-term ' ^'
5.2 Liothyronine Sodium L-triiodothyronine,LT3)
is available in tablet strengths of 5 |ag, 25 ng and
50 |ig. It requires m ultiple daily ad m inistratio n inview of
its short half-life of ~ day. Another dis-advantage is that serum
T3 concentration risesto supranormal values of up to 250-600% in
theabsorption phase, during which many patientsrep ort ad verse
effects, especially palpitations.f^^'In a recent randomized,
double-blind crossovertrial, it was shown that substitution of LT3
forLT4 at equivalent doses (relative to the pituitary)reduced body
weight and caused favourablechanges in lipid profile without
appreciable ad-verse effects. However, this study involved a
verylimited number of subjects and, also, both LT4and LT3 were used
thrice-daily in this study,which limits its clinical utility.
^"1LT3 may be usefulprior to treatment of thyroid cancer with
radio-active iodine ('^'I), as patients can be withdrawnfrom LT3
for shorter periods of time than LT4. Itmay be used when a rapid
effect is desired (e.g.perioperatively or in myxedema coma).
Further-more, its use can be considered in rare cases of
LT4 maldigestion or malabsorption as well as inpatients with
documentation of inhibition of T4to T3 conversion.'-"' O therwise,
it is not intendedas sole maintenance therapy in treatment of
hypo-thyroidism.
5.3 C om b in at io n LT4/LT3 Therapy
Combination LT4 and LT3 treatment hasbeen tried in an effort to
more closely mimic the
thyroid secretion pattern of T4 and T 3. How ever,there is no
currently available preparation con-taining LT4 and LT3 in a
combination that ade-quately reproduces the relative quantities of
thesehormones produced by the human thyroid. Fur-thermore, no
preparation produces a sustainedrelease of thyroid hormones in a
pattern similarto that of the human thyroid.'^^' Having been
dis-regarded as a therapeutic approach to the treat-ment of
hypothyroidism since the 1970s, interestin combination LT4/LT3
therapy was re-ignitedby a randomized, double-blind crossover trial
of31 patients published by Bunevicius et al.'^^l in
-
8/13/2019 Overt and Subclinical Hypothyroidism
8/18
24 Khandelwal Tando
with LT4 alone. However, a majority of patientsin the study had
been treated previously forthyroid cancer and were receiving
relatively highdoses of LT4, which could have confounded theresults
of the study. However, subsequent ran-domized controlled studies
have failed to show abeneficial effect of combined LT4/LT3
therapyon measures of well-being, health and mentalfunctioning,
with some even reporting harm-ful effects.'^'* A me ta-an alys is
of 11 ran dom izedcontrolled trials involving 1216 participants
of
LT4/LT3 combination versus LT4 monotherapyfor treatment of
clinical hypothyroidism foundno difference in any clinical or
biochemical para-meter compared with LT4 monotherapy.'^^'
TheExecutive Committee of the British Thyroid As-sociation stated
in 2007' ^' tha t combined LT 4/LT 3cannot be recommended because
of a lack of ben-efit and a small num ber of undesirable and
harmfuleffects seen with combination treatment.
5.4 Desiccated ThyroidDesiccated thyroid contains both T4 and
T3
extracted from the thyroid gland of animals. Itcontains
excessive amounts of T3 relative to T4,is not a pure preparation of
thyroid hormonesand ha s issues relate d to stability.'^* W hile it
wasthe mainstay of therapy in hypothyroidism untilthe 1970s, there
is currently no evidence support-ing its use in the treatment of
hypothyroidism.
6 initiating LT Therapy
The goal of treatme nt is to restore the individualto a
euthyroid state, with resolution of signs andsymp toms. The
rapidity with which the euthyroidstate should be attained is
dictated by severalfactors, notably, the age of patient, the
durationand severity of hypothyroidism and the presenceof other
co-morbid conditions, specifically car-diac disease. LT4 is
recommended to be taken as
a single daily dose on an empty stomach at least30 minutes
before breakfast.'^''^ A recent ran-domized double blind crossover
trial has sug
snacks before bedtime, allowing a gap ofhours between the last
meal and LT4. This not be practicable in other cultures or
fordividuals who have a habit of late dinner bedtime snack. LT4
should be taken at leasthours apart from drugs that are known to
ifere with its absorption (table 111).'^^^
Most patients who are aged
-
8/13/2019 Overt and Subclinical Hypothyroidism
9/18
vert and Subclinical Hj^pothyroidism 25
T4 requirements are greatly dependent on the
ndividual 's lean body mass, rather than actualotal body
weight.'"^"^ The LT4 dose is generallyigher in patients with
previous thyroidectomyhan in those with autoimmune thyroiditis,
inhich there may be some residual functioning
hyroid tissue. In the absence of any functioninghyroid tissue,
the complete daily replacement dosen women and men ranges from
100|xg to 150|agn d betwe en 125 ^g a nd 200 |xg, respe
ctively.''^'re-treatment serum TSH predicts, to a certainxtent, the
daily maintenance dose of LT4 inatients with primary
hypothyroidism. Patients
with subclinical hypothyroidism, because of theminimal extent of
the thyroid hormone defi-iency, may be controlled with total daily
dosagesf LT4 as low as 25-50 |xg.
7 Monitoring
After initiation of thyroid hormone therapy,ymptom s and signs
of hypothyroidism should bessessed at each follow-up visit. LT4
effectivelyelieves the manifestations of thyroid hormoneeficiency
in most patients; this can be expectedeveral weeks to months after
initiation of ther-.py. Resolution of symptoms and signs usuallyags
behind biochemical normalization. The ear-iest clinical response to
thyroxine replacement issually diuresis and weight loss due to
mobiliza-ion of interstitial fiuid as glycosaminoglycansre
degraded. Weight loss is predominantly due
o fluid loss, and even in obese patients is unlikelyo exceed 5
kg, especially if pre-treatment TSHalues were modestly elevated.'
'^' A decrease inat with thyroxine therapy, if any, is usually
mini-
mal and occurs late in the course of treatment.Reduction in
puffiness and an increase in pulseate and pulse pressure are also
early responsesfter treatm ent.' '" Fea tures such as appetite,
con-tipation, hoarseness of voice, cold intolerance andatigue
recover later, while symptoms and signselated to the skin,
appendages and nervous sys-em are the last to resolve.''^
After initiating ther apy , -the dose sho uld be
to re-set after introducing or modifying LT4 ther-
apy. Serum TSH should be maintained in thelower half of normal
range (0.5-2.0 mlU/L).'^''-''^)In the event that serurn TSH is
either elevat.ed orsuppressed, there will be a need for a modest
in-crease or decrease in dose, respectively. The doseshould ideally
not be increased or decreased bymore than 12.5 or 25 \ig and serum
TSH againme asured after 2 m onth s to assess ade qua cy ofthe
dose. Because of the long half-life of LT4,small dosage adjustments
may even be performedby adding or withdrawing a tablet once or
twice aweek. A minor deviation from the targeted TSHvalue should
not immediately prom pt dose adjust-ment; instead, a repeat TSH
measurement can beperformed after 2-3 months before deciding ona
dose change. Once the patient attains a bio-chemical euthyroid
state, serum TSH should nextbe measured after 6 months. This is
required be-cause, at initiation of therapy, due to the
hypo-thyroid state, the administered LT4 may be stillbe metabolized
slowly and appear adequate for
the patient 's requirements. Once euthyroidism isrestored,
thyroxine metabolism m ay increase andthe same dose be rendered
sub-optimal. Once astable LT4 dose is achieved, monitoring needs
tobe carried out annually. While this strategy worksfor most
patients with hypothyroidism, patientswith post-ablative
hypothyroidism may continueto have a decline in thyroid reserve
over the yea rs,necessitating semi-annual or even annual dosechange
s until the effect of the '^ 'I plate aus . Some-
times, a similar evolution of declining thyroidreserve over a
period of time m ay also be ob servedin patients with Graves'
disease who have had asub-total thyroidectomy.
Some experts also estimate serum T4 (total orfree) to monitor
therapy. If this is being done,care should be taken that the blood
sampleshould be collected prior to receiving the day'sdose of LT4.
Invariably, if the serum TSH levelsare in the mid to low normal
range, serum T4levels will be in the mid to high nor m al ra nge.
Fo robvious reasons, the main role of serum T4 iswhen monitoring
thyroxine replacement in a pa-
-
8/13/2019 Overt and Subclinical Hypothyroidism
10/18
26 Khandelwal Tando
8 Persistentiy Eievated TS Despite
Thyroid Hormone RepiacementAn important cause of persistently
elevated
TS H despite adequa te replacement dose of LT4 isnon-compliance
of the patient. In fact, thesepatients can have an elevated TSH
with high-normal or elevated FT4, as they may not takeLT4 for days
and then take several pills a fewdays before their testing. No
change in the LT4dose is needed in this situation; rather,
emphasisshould be placed on com pliance with therapy andthe thyroid
function test repeated in 3-4 weeks.It sometimes helps to ask the
patient to take aweek's supply of medicine in a separate
pill-box,which will allow easy ascertainment of misseddoses. Any
extra pills left in the container canactually all be taken on the
last day of the week,to ensure that the patient receives his or her
weeklydose. Because of the long half-hfe of 7 days, someauthors
propose that LT4 can be given onceweekly in poo rly co mp liant
patients. A crossover
trial of 12 patie nts show ed tha t a single weeklydose achieved
fairly good therapeutic results.'' '^1Weekly dosing or end-of-week
catch-up dosing,while sub-optimal, remains an acceptable
alter-native for habitual non-com pliers. Weekly dosingshould not
be given in patients who have cor-onary artery disease.
Other causes of persistently elevated TSH de-spite an apparently
adequate dose of LT4, includemalabsorption and interference by
drugs (table
III). It is worth excluding coeliac disease in suchcases, as it
may coexist in patients with hypo-thyroidism because of its
autoimmune nature.Interference to the laboratory assay as a result
ofheterophil antibodies in a patient's serum also canlead to
artificial elevation in TSH.
9 Treatment in Spe ciai Circumstanc es
9.1 Primary Hypothyroidism In SpeciaiCircumstances9 1 1
Pregnancy
Patient Aiready on R epiacement Becoming
nancy and fetal development. Untreated
hypothyroidism during pregnancy is found associated with
increased risk of maternal htension, pre-eclampsia, postpartum
haemorranaemia, fetal death, low birth weight and na ta l r es pir
ato ry distress. '*''-'*^] In a la ndobservational study, Haddow et
al'^'^i also fthat women with overt or subchnical hyproidism
deliver babies with an average intelligquotient (IQ) score 7 points
below the mean children born to healthy women and thyrotreated
women. If hypothyroidism has beeagnosed before pregnancy, the
preconcepLT4 dose should be modified to reach a level not higher
than 2.5mIU/L before plapregnancy.''*^'
During pregnancy, the LT4 requirement icreased by 25-50% in most
hypothyroid wowhich becomes evident early in the first trster.f *
The increased requirement is probab lyto a combination of factors:
rapid rise in thyine-binding globuhn (TBG) levels resulting the
physiological rise in estrogen, increasedtribution volume of
thyroid hormones, andcreased placental transport and metabolism
.maternal T4. The LT4 dose should be increby 30-50% by 4-6 weeks
gestation. As therelarge individual variability in dose
requiremdose adjustment requires testing serum TSHtotal T4 (FT4
according to some authors) atular intervals, such as every 4-6
weeks. It isommended that serum TSH be maintaine
trimester-specific normal ranges (
-
8/13/2019 Overt and Subclinical Hypothyroidism
11/18
vert and Subclinical H ypothyroidism 27
with iron or calcium. A time gap of 4-6 hours
etween LT4 and these supplements should bemaintained.
Hypothyroidism De tecte d for the First Time duringPregnancyWhen
hypothyroidism is detected for the first
ime during pregnancy, the test should be repeated.Unless the
result is expected within 24 hours,reatment must be started before
confirmation tovoid loss of time. LT4 dosage should be titratedo
rapidly reach, and thereafter maintain, serum
TSH concentrations to trimester-specific normalTSH ranges.
Factors determining the appropriate
ose for initiation of therapy are time of gesta-ion, and the
aetiology and severity of the disease.n view of increased
requirements, the full replace-
me nt dose of LT 4 in pregna ncy is 2.0-2.4 [ig/kgodyweight/day.
Therapy may be initiated by giv-ng, for the first few days, a LT4
dose corre-pond ing to two to three times the estimated
finaleplacement daily dose, to rapidly normalize the
xtra-thyroidal thyroxine pool. Thyroid functionests shou ld be
re-m easure d within 30- 40 '' ^
Subciinical Hypothyroidism and PregnancySubclinical
hypothyroidism has been shown to
be associated with an adverse outcome for bothhe mother and the
offspring. LT4 treatment has
been shown to improve obstetrical outcome buthas not been proved
to modify long-term neuro-ogical development in the offspring.
However,
given that the potential benefits outweigh the
potential risks, LT4 replacement is recomm endedn all pregnant
women with subclinical hypo-hyroidism.'"*^ It is no t clearly
defined whe the r
LT4 treatment should be continued postpartumn women in whom
diagnosis of subclinical hypo-hyroidism was made during pregnancy.
In our
opinion, treatment should be continued in thesewomen if serum
TSH is >10mIU/L or in the pre-ence of hypothyroid symptoms,
goitre or anti-
TPO antibodies, as advised for other adults withsubclinical
hypothyroidism. Also, women who areplanning a subsequent pregnancy
should continueon LT4 replacement. In all other women, LT4
9 7 Coronary Artery Disease
Initiation of LT4 replacement therapy in patientswith coronary
heart disease should be carried outcautiously to avoid exacerbating
angina pectoris,or precipitating acute myocardial
infarction,ventricular arrhythmias or congestive heart fai-lure.'^1
Alth oug h tre atm ent of hyp othy roidismwith LT4 will improve
myocardial function andreduce peripheral vascular resistance, it
will in-crease the need for oxygen in the myocardium.In patients
with an already compromised myo-
cardial blood supply due to coronary athero-sclerosis, LT4
treatment may provoke anginalsymp toms. In a study of 1503
hypothyro id subjects(average age 71 years), 2% developed new
onsetangina during LT4 therapy. In patients with pre-existing
angina, after LT4 treatment, symptomsimproved in 38%, remained
unchange d in 46% andworsened in 16%.'^' Patients with pre-existing
an-gina should ideally undergo cardiac evaluation forcorrectable
lesions of the coronary arteries and betreated appropriately prior
to initiating LT4 ther-apy. LT4 in such individuals should be
started at adose of 25 ng/day or even less and it should be
in-creased no faster than at 4-weekly intervals. If an-gina is
precipitated while increasing the LT4 dose,it should be reduced to
the highest dose toleratedby the patient and a further attempt made
to in-crease the dose again only after another 4 weeks.
9 1 3 lderly
In many cases, hypothyroidism in elderly patients
is characterized by a paucity of specific signs andsymptoms. The
symptoms may be subtle and in-clude hoarseness, deafness,
confusion, dementia,ataxia, depression, dry skin or hair loss.'^^'
A n orm alstarting dosage of LT4 in an elderly subjectis aro un d 1
(ig/kg/day, which is m aintain ed for4 -6 weeks. ^1 If heart
disease is suspected, a lowerstarting dose, as mentioned in section
9.1.2 isappropriate. Dosage adjustments are guided bythe response
in TSH and the clinical state, withemphasis on possible cardiac
adverse effects.Limited evidence suggests that treatment of
sub-clinical hypothyroidism with serum TSH of up to
-
8/13/2019 Overt and Subclinical Hypothyroidism
12/18
28 Khandelwal Tand
Table IV Ciinicai characteristics, screening and evaluation
of
congenitai hypothyroidism' I^^ ^^'CausesThyroid
dysgenesisThyroid dyshormonogenesisHypothalamic-pltuitary
abnormaiityTransient hypothyroidism (maternal antithyroid
medication, maternaiblocking antibodies, iodine deficiency or
excess)
Symptoms and signsUnexplained postmaturity, poor feeding,
hypothermia, iethargy,proionged jaundice, abdominai distension,
umbilicai fiernia, iargetongue, hoarse cry, m ottied dry skin,
iarge posterior fontanei,deiayed skeietai maturation
Screening methodsPrimary TSH with backup T4 measurementPrimary
T4 with backup TSH measurementCombined primary TSH pius T4
measurements (ideai method)
if screening positive or hypothyroidism suspected laterDetailed
history and examinationRepeat serum TSH and either totai T4 or
FT4Additional work up in confirmed cases (shouid not iead to deiay
intreatment); thyroid radionuciide scintigraphy, thyroid
sonographyand serum thyrogiobuiin
a Frequency; ; 3000 to ; 4000 iive births.
FT4=free T4; T4=thyroxine; TSH=thyroid-stimulating hormone.
in adverse effects and is instead found to beassociated with
prolonged life
9 4 Congenital ypothyroidism
Clinical characteristics, screening and evalua-tion of
congenital hypothyroidism is summ arizedin table IV. The overall
goals of treatment incongenital hypothyroidism are to assure
normalgrowth and development and cognitive outcomesimilar to
genetic potential by restoring serum T4concentration rapidly to the
normal range fol-lowed by continued clinical and biochemical
eu-thyroidism. The aim of treatment is to keep theserum T4 (total
or free) concentration in the up-per half of the normal range
adjusted for age. Ofnote, most commercial laboratories do not
pro-vide age-adjusted normal ranges in their reports.In the first
postnatal year, serum T4 should be10-16 i^g/dL an d serum FT 4 sh
ould be 1.4 2.3
ng/dL. The serum TSH concentration should be
-
8/13/2019 Overt and Subclinical Hypothyroidism
13/18
vert and Subclinical H ypothyroidism 29
piphysis are other radiological manifestations of
ypothyroidism in children.The recommended dose of LT4 for each
age
roup is as follows:'^'3-12 m onth s: 6-10 |ig/kg/day1-3 years :
4 -6 fxg/kg/day3-10 years: 3-5 ng/kg/day10-16 years: 2-4 ng/kg/d
ay.Treatment should be individualized because
he absorption of LT4 and m etabolism vary am ongndividuals.
Serum FT4 and TSH concentrations
hould be monitored periodically, preferably at- to 6-month
intervals. Available data indicatehat risk of progression from
subclinical to overtypothyroidism is less common in children
anddolescents, and the recovery of thyroid functions more
frequent.'^^' In one recent multicentretudy from Italy, 88% of
subclinical hypo thyro idhildren normalized their TSH over a period
of
years.'*^^ Also, persistent subclinical hypothy-oidism in
children is not associated with altera-ion in growth, maturation,
body mass index andognitive functions, even after several
years.'*"*' Inact, there is a view that subclinical hypothy-oidism
in children may b e just a norm al variation,ather than a sign of a
failing thyroid gland.'^^' In
match ed case -control stud y of type 1 diabetichildren,
subclinical hyp othyroidism was associated
with significantly increased risk of symptomaticypoglycaemia as
compared with matched eu-hyroid controls, which became compa rable
after months of LT4 replacement.^**'
9 1 6 Adren al Insufficiency
In the event there is co-existence of thyroidormone deficiency
and glucocorticoid deficiency,t is important to replace
glucocorticoids beforetarting LT 4. This is because LT 4 therapy
may leado an increased metabolism and, thereby, an in-reased demand
of cortisol, potentially increasinghe likelihood of precipitating
an adrenal crisis.
9 1 7 D ifferentiated tiyroid Cancer
Patients who have had a thyroidectomy forifferentiated thyroid
cancer, with or without
Table V American Thyroid Association and E uropean Thyroid
As-
sociation recommendations for thyroid-stimulating hormone
(mlU/L)targets in patients with differentiated thyroid cancer ^
^
Patient category Recommendation
ATA ETA
High and intermediate risk (initialtherapy)
Persistent disease
High-risk disease free (follow-up)
Low risk (initial therapy)
Low-risk disease free (follow-up)
0.1-0.5
-
8/13/2019 Overt and Subclinical Hypothyroidism
14/18
30 Khandelwal Tand
ease of treatmen t with LT 4, which is the s tanda rd
treatment even in central hypothyroidism.[^' 'Serum TS H level
is not helpful in cases of centra lhypothyroidism. Instead, the
chnician shouldevaluate serum FT 4, adjusting the LT4 dosage tokeep
the serum FT4 in the upper half of the nor-mal range for age.^^^l
Monitoring total T4 is alsoacceptable, provided there are no
alterations inbinding proteins.
The possible presence of secondary adrenalinsufficiency should
be kept in mind and pituitary-
adrenal function should be assessed, usually byan
adrenocorticotropic hormone (ACTH) stimula-tion test. If present,
secondary adrenal insufficiencyshould be treated before starting
LT4 replace-ment. Treatment of other pituitary hormone
de-ficiencies might affect dosing of LT4. Growthhormone deficiency
may mask central hypothy-roidism, an d this might beco me evident
only afterreplacement of growth hormone.'^^^ Concomitantestrogen
replacement in women also significantlyincreases LT 4 dose
requireme nt due to an increasein TB G I i
rarity of this emergency, very few random
studies have looked at the treatment and outM ost experts
recommend use of intravenous(loading doses va rying from 200 to 500
|alowed by m aintenan ce doses of 50-100 |ig duntil oral intake and
bowel motility are adeqafter which patients can be switched to
oraplacement. Advice regarding use of concomintravenou s LT3 is
inconsistent, with som e exrecommending that it has no utility,'^'
' othervising that it should be used only in compatients,t''*i and
a few suggesting that it shouadministered in all patients with
myxoecom a.I ' ' '' Argu men ts in favour of the intraveroute are
risk of aspiration and the uncertof absorption with the nasogastric
rHowever, in one previous'^^l and one recenstudy, outcomes did not
differ between patwho received LT4 via a nasogastric tubethose who
received it intravenously. The ularger do ses of L T4 (>500
ng/day) is assocwith higher mortality and therefore
isrecommended.'^^'
9.3 Myxoedema Com a
Myxoedema coma represents a decompensatedstate of severe
untreated hypothyroidism. In general,it occurs in elderly
individuals with long-s tandinghypothyroidism and usually during
winter months.Major chnical hallmarks of myxoedema coma arealtered
men tal status, defective therm orgulationand a precipitating event
or illness, in addition tobiochemical hypothyroidism.'^^-^^l
Diagnosis re-quires a high index of suspicion, and failure
torecognize and treat it in a timely manner can befatal. Given a
reason able index of suspicion, treat-ment should begin immediately
while awaitinglaboratory results. The three-pronged approachto
treatment comprises (i) supportive measures,with particular
emphasis on haemodynamic sup-port, including use of steroids; (ii)
thyroid hor-
mone replacement; and (iii) concomitant man-agement of
coexisting problems, most importantlyinfections Controversy
surrounds thyroid hor-
10 Adverse Effects
LT4 is a drug recognized to have a natoxic to therapeutic ratio
with significant cal consequences of excessive treatment. Chunder-
or over-replacement is common in clpractice and data indicate that
over-treatoccu rs in ab ou t 20% of LT 4-tre ated patients.'Adverse
effects of over-replacement includrisk of bone loss, especially in
postmenop
^''-^''] and increased risk of atrial fibA syndrome of
hyperadrenergic
soon after LT4 treatment has been descrwhich could be
attributable to anaemia in cases.'^' ' Transient scalp hair loss
can also place during the first few weeks of LT4 repment.'^^ Rare
cases of allergic reactions havereported, which were almost always
seconda
dye or other inactive constituents.t'^^ Ch ang ia different
brand or tablet with a differentgenerally overcame the problem Two
other
-
8/13/2019 Overt and Subclinical Hypothyroidism
15/18
vert and Subclinical H ypothyroidism 31
11 Conclusions
Hypothyroidism is a common disorder, read-ly diagnosed with
laboratory investigations. Allatients with overt hypothyroidism and
sub-linical hypothyroidism with TSH >10mIU/Lhould be treated, as
should all pregnant women
with any degree of subclinical hypothyroidism.However, treatment
of non-pregnant patientswith subclinical hypothyroidism and serum
TSH
alues up to lOmlU/L remains controversial, withmost expert
groups recommending LT4 therapy
nly in the presence of symptoms, goitre, positiventi-TPO
antibodies or infertility. LT4 remains theurrent standard for
treatment and combined
LT4/LT3 is not recommended. Adequacy of treat-ment is monitored
using serum TSH in primary
nd serum FT4 in secondary hypothyroidism.Special considerations
are needed in pregnantwomen, children, elderly patients and
patientswith cardiac disease. Un der- or over-treatm ent is
ommon in clinical practice and should be avoided.
Acknowledgements
No sources of funding were used to conduct this study orrepare
this manuscript. The authors have no conflicts of in-erest that are
directly relevant to the content of this article.
References1. Wiersitiga WM. Hypothyroidism and myxedema coma.
In:
Jameson JL, DeGroot LJ, editors. Endocrinology adultand
pdiatrie. 6th rev. ed. Philadelphia (PA): Saunders,
2010: 1607-222. Brent GA, Larsen PR, Davies TF. Hyopthyroidism
andthyroiditis. In: Kronenberg HM, Melmed S, Polonsky KS,et al.,
editors. Williams textbook of endocrinology. 11threv. ed.
Philadelphia (PA): Saunders, 2008: 377-410
3. Biondi B, Cooper DS. The clinical significance of
subclinicalthyroid dysfunction. Endocr Rev 2008 Feb; 29 (1):
76-131
4. Vanderpump MP, Tunbridge WM, French JM, et al. Theincidence
of thyroid disorders in the commu nity: a twenty-year follow-up of
the Whickham Survey. Clin Endocrinol(Oxf) 1995 Jul; 43 (1 ):
55-68
5. Roberts CG, Ladenson PW. Hypothyroidism. Lancet 2004Mar 6;
363 (9411): 793-803
6. Vanderpump MP, Tunbridge WM. Epidemiology and pre-vention of
clinical and subclinical hypothyroidism. Thyr-oid 2002Oct; 12 (10):
839-47
8. Huber G, Staub JJ, Meier C, et al. Prospective study of
thespontaneous course of subclinical hypothyroidism: prog-nostic
value of thyrotropin, thyroid reserve, and thyroidantibodies. J
Clin Endocrinol M etab 2 2 Jul; 87 (7): 3221-6
9. Diez JJ, Iglesias P. Spontaneous subclinical hypothyroidismin
patients older than 55 years: an analysis of natural courseand risk
factors for the development of overt thyroid failure.J Clin E
ndocrinol Me tab 2004 Oct; 89 (10): 4890-7
10. Braverman LE, Utiger R D. Introduction to hyp
othyroidism.In: Braverman LE, Utiger RD, editors. Werner and
In-gabar's the thyroid: a fundamental and clinical text.
Phila-delphia (PA): Lippincott Williams & Wilkins, 2005:
697-9
11. Singer PA. Primary hyp othyroidism due to other causes.
In:Braverman LE, Utiger RD, editors. Werner and Ingabar'sthe
thyroid: a fundamental and clinical text. Philadelphia(PA):
Lippincott Williams & Wilkins, 2005: 745-53
12. Wiersinga WM. Adult hypothyroidism. South Dartmouth(MA):
Endocrine Education Inc. [online]. Available fromURL:
http://www.thyroidmanager.org/chapter9/0-frame.htm [Accessed 2011 A
ug 8]
13. Canaris GJ, Steiner JF, Ridgway EC. Do traditional symp-toms
of hypothyroidism correlate with biochemical dis-ease? J Gen Intern
Med 1997 Sep; 12 (9): 544-50
14. Hueston WJ. Treatment of hypothyroidism. Am Fam Phy-sician
200 Nov 15; 64 (10): 1717-24
15. Vaidya B, Pearce SH. Management of hypothyroidism inadults.
BMJ 2008 Aug 2; 337: 284-9
16. Surks MI, Ortiz E, Daniels GH, et al. Subclinical
thyroiddisease: scientific review and guidelines for diagnosis
andmanagem ent. JA MA 2004 Jan 14; 291 (2): 228-38
17. Gharib H, Tuttle RM, Baskin HJ, et al. Subelinical
thyroiddysfunction: a joint statement on managem ent from
theAmerican Association of Clinical Endocrinologists, theAmerican
Thyroid A ssociation, and the End ocrine Society.J Clin En docrinol
Metab 2005 Jan; 90 (1): 581-7
18. Jones DD , May K E, Geraci SA. Subclinical thyroid diseaseAm
J Med 2010 Jun; 123 (6): 502-4
19. Papi G, Uberti ED, Betterle C, et al. Subclinical
hypothy-roidism. Curr Opin Endocrinol Diabetes Obes 2007 Jun;
14(3): 197-208
20. McDermott MT, Ridgway EC. Subclinical hypothyroidismis mild
thyroid failure and should be treated. J Clin En-docrinol Metab
2001 Oct; 86 (10): 4585-90
21. Fatourechi V. Subclinical hypothyroidism: how should it
bemanaged? Treat Endocrinol 2002; I (4): 211-6
22. Chu JW, Crapo LM. The treatment of subclinical hypo-
thyroidism is seldom necessary. J Clin End ocrinol M etab
2001 Oct; 86 (10): 4591-923. Gussekloo J, van Exel E, de Craen
AJ, et al. Thyroid status
disability and cognitive function, and survival in old ageJAM A
2004 Dec 1; 292 (21): 2591-9
24. Woeber KA. Treatment of hypothyroidism. In: BravermanLE,
Utiger RD, editors. Werner and Ingabar's the thyroid:
a fundamental and clinical text. Philadelphia (PA): Lip-pincott
Williams & Wilkins, 2005: 864-925. Fish LH, Schwartz HL,
Cavanaugh J, et al. Replacement
-
8/13/2019 Overt and Subclinical Hypothyroidism
16/18
Khandelwal Tan
26 . Mandel SJ, Brent GA , Larsen PR. Levothyroxine therapy
inpatients with thyroid disease. Ann Intern Med 1993 Sep 15;119
(6): 492-502
27. US Department of Health and Human Services, US FDA.Sample
letter [online]. Available from URL:
http://www.fda.gov/downloads/Dr^gs/DrugSafety/PostmarketDrugSafetylnformationforPatientsandProviders/UCM
161272.pdf[Accessed 2011 Au g 8]
28. American Thyroid Association; Endocrine Society; Amer-ican
Association of Clinical Endocrinologists. Joint state-ment on the
U.S. Food and Drug Administration's deci-sion regarding
bioequivalence of levothyroxine sodium.Thyroid 2004 Jul; 14 (7):
486
29. Wiersinga WM. Thyroid hormone replacement therapy.
Horm Res 2001; 56 Sup pl. 1: 74-8130. Celi FS, Zemskova M,
Linderman JD, et al. Metaboliceffects of liothyronine therapy in
hypothyroidism: a ran-domized, dou ble-blind, crossover trial of
liothyronine ver-sus levothyroxine. J Clin Endocrinol Metab. Epub
2011Aug 24
31. Clarke N, Kabadi UM. Optimizing treatment of
hypothyr-oidism. Treat Endocrinol 2004; 3 (4): 217-21
32. Arm our Thyroid (USP) and combined
thyroxine/tri-iodothyronine as thyroid hormone replacement: a
state-ment from the British Thyroid Association ExecutiveCommittee,
November 2 7 [onhne]. Available from UR
L:http://www.british-thyroid-association.org/Guidehnes/Do
cs/Armour_nov_07.pdf [Accessed 2011 Aug 8]33. Bunevicius R,
Kazana vicius G, Zalinkevicius R, et al. Effectsof thyroxine as
compared with thyroxine plus triiodothyr-onine in patients with hyp
othyroidism. N Engl J Med 1999Feb 11; 340 (6 ): 424-9
34. Escobar-Morreale HF, Botella-Carretero JI, Escobar delRey F,
et al. Review: treatment of hypothyroidism withcombinations of
levothyroxine plus liothyronine. J ClinEndocrinol Metab 2005 Aug;
90 (8): 4946-54
35. Grozinsky-Glasberg S, Fraser A , Nahsho ni E, et
al.Thyroxine-triiodothyronine combination therapy versusthyroxine
monotherapy for clinical hypothyroidism: meta-analysis of
randomized controlled trials. J Clin EndocrinolMetab 2006 Jul; 91
(7): 2592-9
36. Rees-Jones RW, Larsen PR. Triiodothyronine and thyrox-ine
content of desiccated thyroid tablets. Metabolism 1977 .No v; 26
(11): 1213-8
37. Bolk N, Visser TJ, Nijman J, et al. Effects of evening
vsmorning levothyroxine intake: a randomized double-blindcrossover
trial. Arch Intern M ed 2010 Dec 13; 170 (22):1996-2003
38. Liwanpo L, Hershman JM. Conditions and drugs interfer-ing
with thyroxine absorption. Best Pract Res Clin En-docrinol Me tab
2009 Dec; 23 (6): 781-92
39. John-Kalarickal J, Pearlman G, Carlson HE. New medica-tions
which decrease levothyroxine absorption. Thyroid
2007 A ug; 17 (8): 763-540. Santini F, Pinchera A , Marsili A,
et al. Lean body mass is a
major determinant of levothyroxine dosage in the treat-
42. McDermott MT. In the clinic: hypothyroidism. AnnMed 2009 Dec
1; 151 (11):ITC61
43. Grebe SK, Cooke RR, Ford HC, et al. Treatment ofthyroidism
with once weekly thyroxine. J Clin EndMetab 1997 Mar; 82 (3):
870-5
44. Davis LE, Leveno KJ, Cunningham FG. Hypothyrcomplicating
pregnancy. Obstet Gynecol 1988 Jul;108-12
45. Wasserstrum N, Anania CA. Perinatal consequenmaternal
hypothyroidism in early pregnancy aadequate replacement. Clin
Endocrinol (Oxf) 1995 (4): 353-8
46 . Haddow JE, Palomaki GE, Allan WC, et al. Mthyroid
deficiency during pregnancy and subseque
ropsychological development of the child. N Engl 1999 Aug 19;
341 (8): 549-5547 . Abalovich M, Amino N , Barbour LA, et al. Manag
em
thyroid dysfunction during pregnancy and postpartEndocrine
Society Clinical Practice Guideline. J Cdocrinol Metab 2007 Aug; 92
(8 Supp l.): S1-47
48. Alexander EK, Marqusee E, Lawrence J, et al. Timimagnitude
of increases in levothyroxine requirduring pregnancy in women with
hypothyroidism. J Med 2004 Jul 15; 351 (3): 241-9
49. Fitzpatrick DL, Russell MA. Diagnosis and managemthyroid
disease in pregnancy. Obstet Gynecol ClinAm 2010 Jun; 37 (2):
173-93
50. Aronow WS. The heart and thyroid disease. Clin GMed 1995 May
; 11 (2): 219-29
51. Keating FR , Parkin TW , Selby JB, et al. Treatmen t
odisease associated with myxedema. Prog Cardiova1961 Jan; 3:
364-81
52. Sawin CT. Thyroid dysfunction in older persons. AdvMed 1992;
37: 223-48
53. Laurberg P, Andersen S, Blow Pedersen I, et al. thyroidism
in the elderly: pathophysiology, diagnotreatment. Drugs Aging 2005;
22 (1): 23-38
54. Gussekloo J, van Exel E, de Craen AJ, et al. Thyroidtion,
activities of daily living and survival in extreage: the 'Leiden
85-plus Study'. Ned Tijdschr Ge2006 Jan 14; 150 (2): 90-6
55. Rastogi MV, LaFranchi SH. Congenital hypothyroOrphanetJ Rare
Dis 2010 Jun 10; 5: 17
56. American Academy of Pediatrics, Rose SR; SectiEndocrinology
and Committee on Genetics, AmThyroid Association, Brown RS; Public
Health Cotee, Lawson Wilkins Pdiatrie Endocrine Society, Update of
newborn screening and therapy for conhypothyroidism. Pediatrics
2006 Jun; 11.7 (6): 2290-
57. Vliet GV. Hypothyroidism in infants and childrengenital
hypothyroidism. In: Braverman LE, Utigeeditors. Werner and
Ingabar's the thyroid: a fundamand clinical text. Philadelphia
(PA): Lippincott Willi
Wilkins, 2005: 1033-4158. Working Group on Neonatal Screening of
the Eur
Society for Paediatric Endocrinology. Revised guid
-
8/13/2019 Overt and Subclinical Hypothyroidism
17/18
Overt and Subclinical H ypothyroidism
RD , editors. Werner and Ingabar's the thyroid: a funda-
mental and clinical text. Philadelphia (PA): LippincottWilliams
Wilkins, 2005: 1041-760. Counts D, Varma SK. Hypothyroidism in
children. Pediatr
Rev 2009 Jul; 30 (7): 251-861. Setian N. Hypothyroidism in
children: diagnosis and treat-
. men t. J Pediatr (Rio J) 2007 Nov; 83 (5 Supp l): S209-1662.
Moore DC. Natural course of 'subclinical' hypothyroidism
in childhood and adolescence. Arch Pediatr Adolesc Med1996 Mar;
150 (3): 293-7
63. Wasniewska M, Salerno M, Cassio A, et al.
Prospectiveevaluation of the natural course of idiopathic
subclinicalhypothyroidism in childhood and adolescence. Eur J
En-docrinol 2009 Mar; 160 (3): 417-21
64. Cerbone M, Bravaccio C, Capalbo D, et al. Linear growthand
intellectual outcome in children with long-term idio-pathic
subclinical hypothyroidism. Eur J Endocrinol 2011Apr; 64 (4):
591-7
65. Kaplowitz PB. Subclinical hypothyroidism in children:normal
variation or sign of a failing thyroid gland? Int JPediatr
Endocrinol 2010; 281453 [online]. Available fromURL:
http://www.ijpeonline.eom/content/2010/l/281453[Accessed 2011 Aug
8]
66. Mohn A, Di Michle S, Di Luzio R, et al. The effect
ofsubclinical hypothyroidism on metabolic control in chil-dren and
adolescents with type diabetes mellitus. DiabetMed 2002 Jan; 19(1):
70-3
67. McGriff NJ , Csako G, Go urgiotis L, et al. Effects of
thyroidhormone suppression therapy on adverse clinical outcomesin
thyroid cancer. A nn Med 2002; 34 (7-8): 554-64
68. Cooper DS, Doherty GM, Haugen BR, et al., on behalf
ofAmerican Thyroid Association (ATA) Guidelines Taskforceon Thyroid
Nodules and Differentiated Thyroid Cancer.Revised American Thyroid
Association management guide-lines for patients with thyroid
nodules and differentiatedthyroid cancer. Thyroid 2009 Nov; 19
(11): 1167-214
69. Pacini F, Schlumberger M, Dralle H, et al., on behalf
ofEuropean Thy roid Cancer Taskforce. European consensusfor the
manag emen t of patients with differentiated thyroidcarcinoma of
the follicular epithelium. Eur J Endocrinol
2006 Jun; 154 (6): 787-80370. Martino E, Pinchera A. Central h
ypothyroidism. In:Braverman LE, Utiger RD, editors. Werner and
Ingabar'sthe thyroid: a fundamental and clinical text.
Philadelphia(PA): Lippinc ott Williams Wilkins, 2005: 754-68
71. Yamada M, Mori M. Mechanisms related to the patho-physiology
and management of central hypothyroidism.Nat Clin Pract Endocrinol
M etab 2008 Dec; 4(12 ): 683-94
72. Lania A, Persani L, Beck-Peccoz P. Central hypothyroid-ism.
Pituitary 2008; 11 (2): 181-6
73. Porretti S, Giavoli C, Ronchi C, et al. Recom binant hum
anGH replacement therapy and thyroid function in a largegroup of
adult GH-deficient patients: when does L-T(4)
therapy become mandatory? J Clin E ndocrinol M etab 2002May; 87
(5): 2042-574. Arafah BM. Increased need for thyroxine in women
with
76. Fliers E, Wiersinga WM. Myxedema coma. Rev Endocr
Metab Disord 2003 May; 4 (2): 137-4177. Kwaku MP, Burman KD.
Myxedema coma. J Intensive
Care Med 2007 Jul-Aug; 22 (4): 224-3178. Ringel MD. Management
of hypothyroidism and hyper-
thyroidism in the intensive care unit. Crit Care Clin 2001Jan;
17(1): 59-74
79. Wartofsky L. Myxedema coma. Endocrinol Metab ClinNorth Am
2006 Dec; 35 (4): 687-98
80. Arlot S, Debussche X, Lalau JD, et al. Myxoedema
coma:response of thyroid hormones with oral and
intravenoushigh-dose L-thyroxine treatment. Intensive Care Med1991;
17(1): 16-8
81. Dutta P, Bhansali A, Masoodi SR, et al. Predictors of
out-
come in myxoedema coma: a study from a tertiary carecentre. Crit
Care 2008; 12 (1): Rl
82. Yam amoto T, Fukuya ma J, Fujiyoshi A. Factors
associatedwith mortality of myxedema coma: report of eight casesand
literature survey. Thyroid 1999 Dec; 9 (12): 1167-74
83. Parle JV, Franklyn JA, Cross KW, et al. Thyroxine
pre-scription in the community: serum thyroid stimulatinghormone
level assays as an indicator of undertreatment orovertreatment. Br
J Gen Pract 1993 Mar; 43 (368): 107-9
84. Ross DS, Daniels GH , Gouveia D. The use and limitationof a
chemiluminescent thyro tropin assay as a single thyroidfunction
test in an out-patient endocrine clinic. J Clin Endocrinol Me tab
1990 Sep; 71 (3): 764-9
85. Canaris GJ, Manowitz NR, Mayor G, et al. The Coloradothyroid
disease prevalence study. Arch Intern Med 2000Feb 28; 160 (4):
526-34
86. Uzzan B, Campos J, Cucherat M, et al. Effects on bonemass of
long term treatment with thyroid horm ones: a metaanalysis. J Clin
Endocrinol M etab 996 Dec; 81(12): 4278-89
87. Faber J, Galloe AM. Changes in bone mass during pro-longed
subclinical hyperthyroidism due to L-thyroxinetreatment: a m
eta-analysis. Eur J Endocrinol 994 Apr; 130(4): 350-6
88. Sawin CT, Geller A, Wolf PA, et al. Low serum
thyrotropinconc entratio ns as a risk factor for atrial
fibrillation in oldepersons. N Engl J Med 1994 Nov 10; 331 (19):
1249-52
89. Shakir KM , Turton D, Aprill BS, et al. Anemia: a cause
ointolerance to thyroxine sodium. Mayo Clin Proc 2000Feb; 75 (2):
189-92
90. Shibata H, Hayakawa H, Hirukawa M, et al. Hypersensitivity
caused by synthetic thyroid hormones in a hy-pothyroid patient with
Hashimoto's thyroiditis. Arch Intern Med 1986 Aug; 146 (8):
1624-5
91. Rovet JF, Daneman D, Bailey JD. Psychologic and
psychoeducational consequences of thyroxine therapy for
juvenileacquired hypothyroidism. J Pediatr 1993 Apr; 122 (4):
543-9
92. Van Dop C, Conte FA, Koch TK, et al. Pseudotumor cere-bri
associated with initiation of levothyroxine therapy forjuvenile
hypothyroidism. N Engl J Med 1983 May 5; 308
(18): 1076-80
C d Nikhil T d f d
-
8/13/2019 Overt and Subclinical Hypothyroidism
18/18
Copyright of Drugs is the property of ADIS International Limited
and its content may not be copied or emailed
to multiple sites or posted to a listserv without the copyright
holder's express written permission. However,
users may print, download, or email articles for individual
use.










![Review Article Screening for Maternal Thyroid Dysfunction ...downloads.hindawi.com/journals/jtr/2013/851326.pdf · subclinical hypothyroidism(SH) [ ]. Because of the clear associations](https://img.pdfslide.us/doc/110x75/5f021d227e708231d402a39e/review-article-screening-for-maternal-thyroid-dysfunction-subclinical-hypothyroidismsh.jpg)