Embed Size (px)
Citation preview

Annu. Rev. Public Health. 1989. 10:163-80Copyright © 1989 by Annual Reviews Inc. All rights reserved
STUDIES OF DOCTOR-PATIENTINTERACTION
Debra L. Roter
Department of Health Policy and Management, Johns Hopkins School of Hygiene andPublic Health, Baltimore, Maryland 21205
Judith A. Hall
Department of Psychology, Northeastern University, Boston, Massachusetts 02115
INTRODUCTION
Discussion between doctors and patients has long been regarded as the vehicleby which much of the curing and caring of medicine is conveyed. Sometimesregarded as the art or heart of medicine, its importance was well noted inantiquity and is recognized in modem times. However, it is only since themid-1960s that the actual dynamics of the therapeutic dialogue have beenobserved in any systematic manner and that an attempt to recast this aspect ofmedicine as science has been made. The evolution of methodological andtechnological sophistication has made observation and analysis of the medicalvisit easier over the years, and, indeed, the number of empirical studies ofdoctor-patient communication doubled between 1982 and 1987 to over 60(47).
Several reviews of this body of work have been undertaken (28, 39, 51,55,57), but a resulting synthesis has been lacking; this is a difficult body of workto review. The predominantly exploratory nature of this research, which islargely of the kind in which everything gets correlated with everything else(24), contributes to an overwhelming number of results with which to con-tend. The results appear so confusing that Inui & Carter (28), in reviewingthis literature, characterized the findings as a "Rorschach test" for readers inwhich overall interpretations are as apt to reveal something about the reader asabout the results themselves.
We have elected, therefore, to supplement a selective review of the litera-
l630163 -7525/89/0510-0163502.00
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.
164 ROTER & HALL
ture with results of a meta-analysis of communication studies, in an attempt toachieve a more comprehensive understanding. Meta-analysis involves theapplication of quantitative methods to summarizing a body of research find-ings (20, 33, 43). We highlight patterns of results that may not otherwise obvious and demonstrate that the collective body of research has greater orderand consistency than prior reviews suggest.
We limit this review almost entirely to studies of actual communicationprocesses, thus excluding many studies based solely on patients’ and physi-cians’ reports of events in the medical visit as well as measures of attitudesand expectations. Furthermore, we do not review the growing body ofresearch involving discourse analysis or the analysis of language in its socialcontext (40). This is a rich literature in its own right, but represents a quitedistinct methodological tradition. Rather than do injustice to this literature,we refer the reader to works of Mishler (36), Frankel (15), and West (58).
FRAMEWORKS FOR CODING MEDICAL INTERACTION
Interaction Process Analysis Methods
BALES’ PROCESS ANALYSIS SYSTEM Concerned with group dynamics,Bales (2) developed an analysis scheme for assessing patterns of interaction,communication, and decision-making processes in small groups. Since itsconceptualization, Bales’ scheme has been more widely applied and modifiedthan any other single approach to describing the dynamics of the medicalencounter. The Bales approach focuses on ways in which the process andstructure of communication among persons in a group reflect how theydifferentially participate in problem solving.
According to the theoretical rationale of the Bales method, all interpersonalstatements can be classified as falling into one of two domains, the task andthe socioemotional. Interaction is described in terms of 12 mutually exclusivecategories; six are conceived as affectively neutral and are ascribed to the taskdimension (e.g. gives suggestion or asks for orientation) and six are equallydivided into positive and negative affective categories and are ascribed to thesocioemotional dimension (e.g. agrees or disagrees; shows tension release orshows tension).
Analysis using Bales’ method is based on literal transcripts of the verbalevents of the encounter, which are operationally defined as the smallestdiscriminable speech segment to which the rater can assign classification. Aunit may be as short as a single word or as long as a lengthy sentence;compound sentences are usually divided at the conjunction, and sentenceclauses are scored as separate units when they convey a single item of thoughtor behavior.
Studies of medical encounters in which Bales’ process analysis system was
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.

DOCTOR-PATIENT INTERACTION 165
applied in the late 1960s have become the most often cited studies in the field.In the first study to apply Bales’ system to medical interactions, Davis (10,11) audiotaped the concluding segment of 154 doctor-patient visits at theirfirst encounter, and subsequently recorded the entire follow-up visit for 80 ofthese pairs. Based on a Bales analysis of the audiotape transcripts, Davismanipulated the basic 12 category scores to derive indexes of communicationdifficulty and used factor analysis to reveal underlying dimensions of com-munication. These variables were then correlated with drug compliance.
First visits, probably because they were recorded only in part, were un-related to compliance. However, for revisits, Davis found that patients’ drugcompliance was greatest when patients and physicians engaged in joking andlaughter and when patients sought and received physicians’ suggestions.Noncompliance was more likely when patients and physicians expresseddisagreement.
Furthermore, visits characterized by physicians’ seeking information frompatients without giving them any feedback were more likely to promotenoncompliant behavior than were visits marked by any of the other com-munication patterns identified. Davis termed this type of exchange "nonrecip-rocal informativeness" and concluded that the imbalance in information ex-change during the medical encounter was probably viewed by patients as aphysician failure to meet expectations regarding normal interactive exchange.This failure, Davis suggested, inspired a retaliation through patient failure toadhere to therapeutic recommendations.
In a second study using a slight modification of Bales’ original approach,Freemon, Negrete, Davis & Korsch (16) analyzed transcripts of 285 au-diotapes of pediatric walk-in visits. Patterns of communication in whichphysicians were friendly and approving, informative, and not excessivelyquestioning were positively associated with patient satisfaction and drugcompliance. Again, a finding consistent with Davis’ nonreciprocal in-formativeness was found. Physicians who did not allow their question-askingto dominate the visit, and who provided information to their patients, inspiredthe best results in terms of patient satisfaction and drug compliance.
ROTER’S INTERACTION ANALYSIS SYSTEM In three important ways, Roter(45) modified the Bales approach to studying interaction dynamics in routinemedical encounters. In this system of coding, first of all, identification andclassification of verbal events are coded directly from audiotapes, makingtranscription unnecessary. The unit of analysis remains quite similar toBales’, but now coders unitize speech as they listen to the audiotape.
Second, since coding is done from audiotapes rather than transcripts,assessment of the tonal qualities of interaction is possible. These tonalqualities transmit the emotional context of the visit, as do the words spoken.
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.

166 ROTER & HALL
Coders rate both the patient and physician on global affective dimensions suchas anger, anxiety, dominance, friendliness, and interest.
Finally, categories of interaction are more finely tailored to the substance ofthe medical encounter than in Bales’ system, but generally reflect similargroupings. For instance, categories of information-giving, instructions anddirections, and counseling are substituted for Bales’ original categories ofgiving orientation, suggestion, and opinion.
This system was used to evaluate a health education intervention to increasepatient question-asking during routine medical encounters (45). The interven-tion consisted of encouraging patients to make a list of questions and concernsbefore going into the doctor’s office. Findings revealed that question-askingwas doubled in the experimental group but that this increase was achieved atsome emotional cost. Increased question-asking was associated with reducedpatient sympathy and greater patient anger and anxiety during the encounter.It was also associated with reduced provider sympathy and increased provideranger and matter-of-factness. Moreover, experimental patients were lesssatisfied with their physician at an exit interview.
Nevertheless, over the subsequent six months, experimental patients had asignificantly better rate of appointment-keeping than the control group. Thisincreased rate of appointment-keeping suggests that the task-focused behaviorengaged in within the visit (e.g. question-asking) generalized to task-focusedbehavior subsequent to the visit, in the form of appointment-keeping com-pliance. Further, it was notable that patient satisfaction with the medicalencounter was independent of the patient’s commitment to task-focusedbehavior.
THE VERBAL RESPONSE MODE An alternative approach to Bales’ ProcessAnalysis and its derivatives, based on reference to linguistic theories, wasintroduced by Stiles (48, 49). The Verbal Response Mode (VRM) is a systemin which segments of language, defined grammatically to be equivalent to onepsychological unit of experience, form a taxonomy that implies a particularinterpersonal intent or microrelationship between communicator and recipi-ent. The taxonomy is based on the assignment of language segments to eightmutually exclusive categories by the source of experience, frame of reference,and focus. The categories include disclosure, questioning, edification,acknowledgment, advisement, interpretation, confirmation, and reflection.
The taxonomic groupings were used to identify communication patternsrelated to patient’satisfaction (41, 49). These studies found that patientsatisfaction was associated with communication patterns characterized byinformation exchange. Satisfaction was enhanced when patients were allowedto relate fully their medical history in the early part of the visit, without beingimpeded by closed-ended questions, and when their physicians ended the visitwith information-giving.
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.

DOCTOR-PATIENT INTERACTION 167
COMPARISONS ACROSS CODING SYSTEMS A comparative study of processanalysis schemes was undertaken by Inui and associates (29). Bales’ originalprocess analysis scheme, Roter’s modification, and the VRM were applied to101 new-patient visits to a general medical clinic for which patient knowl-edge, satisfaction, recall of prescribed medications, and compliance had beenmeasured.
The investigators found that the explanatory power of the three systemsdiffered. For instance, the Bales system explained 19% of the variationbetween patients who took prescribed drugs correctly, compared to 28% forthe Roter system, and none for the VRM. Explanation of variation in knowl-edge was somewhat better for Roter than Bales and the VRM, and satisfactionfavored the Roter and Bales systems. Specific findings were: physicians’giving directions and orientation to a patient negatively predicted knowledge;expressions of tension (verbally or nonverbally through global ratings ofanxiety and assertiveness) were negatively related to satisfaction; and patientbids for clarification and physician anxiety (global ratings) were negativelyrelated to compliance.
Drawbacks associated with all systems were also identified. Although theauthors recommended the use of the Roter method, they noted that none of theinteractional systems is ideally suited for capturing the medical encounter at arelatively holistic level or for providing an accounting of sequence in the visit.
CODING AND ABSTRACTION OF INFORMATION EXCHANGE Though the
influence of Bales and other process analysis systems has been considerable,other approaches to coding interaction have been taken. A common alterna-tive has been a more substantive, content-based identification and coding of aparticular kind of communication within the visit, most often informationexchange.
Information statements are generally counted in these investigations and, tovarying degrees, the quantity of information and its presentation are examinedin relation to recall (1, 6, 8, 27, 30, 32). These investigators, and others,conclude that the minority of patients are given adequate information aboutthe drugs they take or their medical condition. What is worse, patients forget agreat deal of what they are told; in fact, on average most estimates of patientrecall are only about 50% of the facts communicated by the physician.Strategies for improved patient recall resulting from these studies are summa-rized in Table 1.
One methodological issue emerging from this literature is the relative meritof scoring recall in terms of the percentage of facts recalled versus theabsolute amount recalled. At least two studies (30, 46) show that as theamount of information offered increases, the proportion recalled goes down.At the same time, there is a strong positive relation between the amountoffered and the absolute amount recalled. Studies reporting only the pro-
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.

168 ROTER& HALL
Table 1 Strategies for improved patient recall
Summarize information at the close of the visitAsk for feedback from the patient on understandingOrganize information into clear blocksRepeat the most important informationBe specific rather than general in instructionsBe early in presenting information during the visit
portional data may therefore paint a misleading picture of how much informa-tion patients actually come away with. Paradoxically, a group of patientsreceiving the most information and remembering the most in absolute termscould have a lower percentage score than a group receiving less to begin with.
These results also point to other issues deserving further attention. Thesimple counting up of informative statements leaves the applicability, im-portance, and accuracy of those statements unaddressed. Future research mayshow that the tbrm and content of inlbrmative statements are as important astheir sheer number, and that what is remembered matters more for patientoutcomes than how much is remembered.
An early and important pilot study that attempted to move in these direc-tions was conducted by Waitzkin & Stoeckle (56). In that study the number explanations and the "depth" of information given by the physician to thepatient were both quantified. Depth of information was coded in such a wayas to discriminate the more from the less technical explanations and to accountfor explanations that were reworded in nontechnical language. In a laterstudy, Waitzkin (54) used this methodology to analyze over 300 medicalencounters. He found that doctors devoted an average of 1.3 minutes toinformation-giving, providing seven informative explanations per encounter.Most explanations were rated in the mid-range of technicality, and 12% ofthese were reworded in nontechnical language.
Other investigators have also addressed the issue of information exchangeand its meaning for patients. Tuckett and associates (52, 53) put less emphasison how information was conveyed and more on how informative the visit wasfor the patient. They examined what doctors actually said in the consultation,but did so with explicit guidelines for a judgment of the intent of thestatement. A judgment was made for each statement as to what the patient wassupposed to grasp, that is, what the key point was. Three topics, diagnosticsignificance, treatment action for the present, and preventive action for thefuture, were rated separately.
Svarstad (50) made most explicit the assessment of adequate information-giving regarding prescribed drug regimens during the medical visit. Shecoded (a) whether the physician specified the purpose and name of the drug;
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.

DOCTOR-PATIENT INTERACTION 169
(b) how long each drug should be taken, (c) the dosage schedules that shouldbe followed, and (d) how regularly the drugs should be taken. The level instruction thus obtained was examined in relation to patient recall andcompliance. Patients who received adequate instruction were more likely tohave an accurate perception of the treatment plan than others, and were morelikely to conform to the doctor’s recommendations. Svarstad noted that only37% of her sample was adequately informed about their drugs.
Svarstad also considered the motivating strategies that physicians engagedin (both verbal and nonverbal) to enhance patient understanding and com-pliance. These included such things as the approachability of the doctor, theextent to which a rationale was provided for the advice given, and the degreeto which the doctor monitored past compliance. These factors also explained ahigh proportion of patient noncompliance.
Coding of Affect in the Medical Visit
Affect, or feeling, can be rated by observers, though it sometimes requiresseveral judges whose ratings are averaged to achieve acceptable levels ofreliability. The simplest approach is to administer global rating scales tojudges of video or audiotapes (as in the Roter system described above). Onecan also segregate verbal from nonverbal channels of communication.
Verbally expressed affect is studied implicitly in content analysis schemeswhenever they count occurrences of "gives approval," "disagrees," and soforth. The expression of affect is not, therefore, limited to nonverbal com-munication as is sometimes assumed. Indeed, when judges were asked tomake ratings of typed clips of physicians’ speech on rating dimensions such asanxiety and sympathy, they were able to do so with good reliability (22).
Purely nonverbal behavior in medical visits is recognized to be important(17) but has been infrequently studied; particularly rare are studies of thevisible channels of doctor-patient nonverbal communication such as facialbehavior and posture (26, 31). Somewhat more often, the tonal or otherfeatures of vocal communication have been assessed. Ratings of content-masked speech have produced promising results beginning with Milmoe’s(35) study of the association between doctors’ voice quality when talkingabout their alcoholic patients and their success in referring those patients totreatment. Since then, it has been demonstrated that the particular vocalaffects expressed when talking about patients are reflected in clinicians’ talkto the same patients (44), and also that a physician’s voice tone relates various patient effects (22, 46).
The work of DiMatteo and colleagues (13, 14) on physicians’ nonverbalcommunication skills also has important implications for our understanding ofaffective communication. In a testing session, these investigators measurephysicians’ abilities to express emotions through the face and voice and to
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.

170 ROTER & HALL
decode the meanings of nonverbal cues of the face and voice. These skillshave been shown to be related to both patient satisfaction and appointment-keeping compliance. Although it is not yet known exactly how these nonver-bal skills are put to use in the medical visit, it is clear that they play animportant role.
THEORETICAL ISSUES
Conceptual Groupings of Process Variables
In an attempt to summarize the common features of the medical communica-tion literature, we applied methods of meta-analysis (24, 47). Because of thequantitative nature of this type of summary, stronger conclusions can often bedrawn regarding the state of the literature than through traditional literaturereviews (43). These methods included three kinds of analytic activities:exhaustive literature searches; the identification and conceptual grouping ofvariables addressed in the literature; and statistical summary of researchresults.
The literature review, conducted through 1985, included a diligent searchfor published, English-language studies of nonpsychiatric medical encountersfor which there was neutral observation (nonparticipant observers, audiotape,or videotape). We located 60 independent studies that provided quantitativedata on the nature of doctor-patient communication (47), and 41 that relatedthis communication to patient or provider variables external to the visit (24).
Though we described in a preceding section the best-established codingsystems, in fact the literature includes some 28 systems by our count, no oneof which has appeared in more than a handful of studies. These systemsgenerated a very large number of variables. In the meta-analysis, we identi-fied over 200 different communication process variables addressed in thestudies reviewed, To uncover underlying similarities and make this largenumber of variables suitable for statistical analysis, it was necessary to reducethem to conceptually meaningful groupings.
To do this, each of us (D. R. and J. H.) independently sorted the variabledescriptions into groupings of conceptually like behaviors. We then comparedour groupings and negotiated a consensus on six mutually exclusive catego-ries. The categories were: 1. information-giving, which includes all categoriesthat imply the proffering of any material that might increase understanding orknowledge; 2. information-seeking, which includes all requests for informa-tion, clarification, or further understanding; 3. social talk, which includes allvarieties of nonmedical and social conversation; 4. positive talk, whichincludes all exchanges with a positive affective tone or intent; 5. negativetalk, which includes all exchanges with a negative affective tone or intent; and6. partnership-building, which includes exchanges of two kinds, those in
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.
DOCTOR-PATIENT INTERACTION 1’71
which the physician facilitates patient participation and those which reflect thephysician’s role as interpreter and synthesizer. Although one can think of aparallel partnership category applying to patients, variables that might have fitin this category were simply not reported in the studies reviewed. Therefore,this category applies only to physician communication.
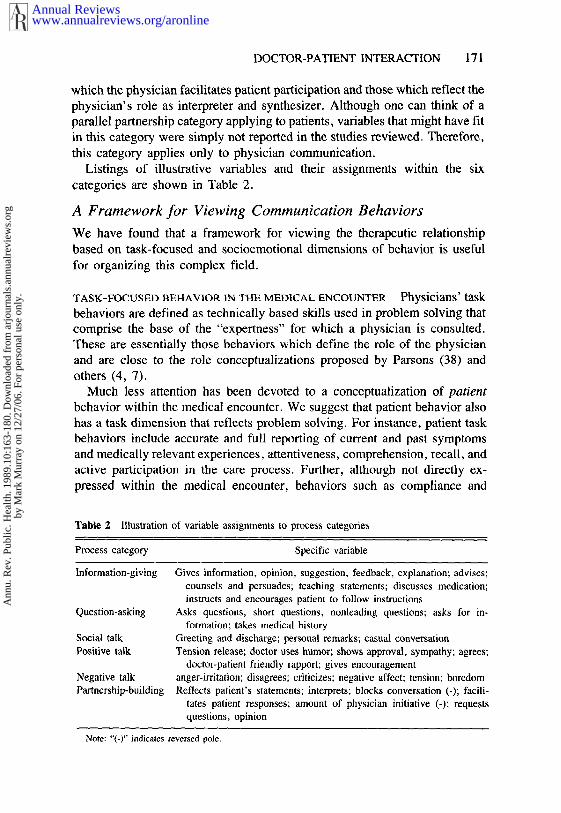
Listings of illustrative variables and their assignments within the six
categories are shown in Table 2.
A Framework for Viewing Communication Behaviors
We have found that a framework for viewing the therapeutic relationshipbased on task-focused and socioemotional dimensions of behavior is usefulfor organizing this complex field.
TASK-FOCUSED BEFIAVIOR IN TFIE MEDICAL ENCOUNTER Physicians’ taskbehaviors are defined as technically based skills used in problem solving thatcomprise the base of the "expertness" for which a physician is consulted.These are essentially those behaviors which define the role of the physicianand are close to the role conceptualizations proposed by Parsons (38) andothers (4, 7).
Much less attention has been devoted to a conceptualization of patientbehavior within the medical encounter. We suggest that patient behavior alsohas a task dimension that reflects problem solving. For instance, patient taskbehaviors include accurate and full reporting of current and past symptomsand medically relevant experiences, attentiveness, comprehension, recall, andactive participation in the care process. Further, although not directly ex-pressed within the medical encounter, behaviors such as compliance and
Table 2 Illustration of variable assignments to process categories
Process category Specific variable
Information -giving
Question-asking
Social talkPositive talk
Negative talkPartnership-building
Gives information, opinion, suggestion, feedback, explanation; advises;counsels and persuades; teaching statements; discusses medication;instructs and encourages patient to follow instructions
Asks questions, short questions, nonleading questions; asks for in-formation; takes medical history
Greeting and discharge; personal remarks; casual conversationTension release; doctor uses humor; shows approval, sympathy; agrees;
doctor-patient friendly rapport; gives encouragementanger-irritation; disagrees; criticizes; negative affect; tension; boredomReflects patient’s statements; interprets; blocks conversation (-); facili-
tates patient responses; amount of physician initiative (-); requestsquestions, opinion
Note: "(-)" indicates reversed pole.
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.

172 ROTER & HALL
utilization of care or services are influenced by the dynamics of the encounterand may also be considered as part of the patient’s task functions.
SOCIOEMOTIONAL BEHAVIOR IN THE MEDICAL ENCOUNTER The socio-
emotional dimension of behavior is more difficult to operationalize than thetask dimension. Although patient behavior has received almost no attention inthis regard, the role of affect in physician behavior has been considered fromseveral viewpoints. Conceptualization of the appropriate expression of physi-cian affect has varied tremendously from Parsons’ (38) view of affectiveneutrality, in which affect is controlled or ignored, to models in whichexpression of affect and task are distinguished as different types of com-munication that are both present during an interaction but are largely in-dependent of one another (7).
Our conceptualization differs from these models, and is premised on thebelief that all face-to-face behavior, even that which is ostensibly neutral,carries affcctive content. This is true for both physicians and patients. Theaffective character of the interaction may be defined on three levels: (a)intrinsic, (b) conveyed, and (c) interpreted. intr insic level comprisesverbal exchanges with explicit socioemotional content such as social con-versation, agreements, criticisms, statements of concern, reassurance,legitimation, partnership, and empathy. The basis of identification for theseexchanges is face validity, that is, the literal content of a communication.
The conveyed level of affect concerns the manner of communication, not itscontent. Voice quality and other nonverbal cues convey affect. Affect is alsoconveyed verbally; aside from a verbal communication’s intrinsic meaning(see above), the innuendo, choice of words, and so forth in the verbal channelcan convey affect (22). Conveyed affect occurs during verbal exchanges thatare intrinsically affective, but also during the performance of task behaviors,e.g. giving information, counseling, and asking questions.
One interesting methodology for assessing vocal affect is to obscure theverbal content from audiotapes by passing them through an electronic band-pass filter (22, 35, 46). This process preserves voice qualities such as pitchcontour and variation, rhythm, and speed. When listening to filtered speech,one perceives voice qualities but not verbal content.
Finally, the interpreted, or attributed, level of affect reflects the totalimpression created in the receivers of a communication. Through attributionor interpretation, communications may gain affective significance that they donot possess either intrinsically or by the manner of expression. Affectiveinterpretations are often consistent with intrinsic and conveyed affect, butthey need not be, as when a patient concludes that the doctor’s socialpleasantries are insincere. The most interesting form of interpretation, fromour point of view, occurs independent of either intrinsic or conveyed corn-
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.
DOCTOR-PATIENT INTERACTION 173
munication. As an example, physicians who give more information may beperceived as interested or friendly simply because they give information andthe patient makes a positive attribution for such behavior (46).
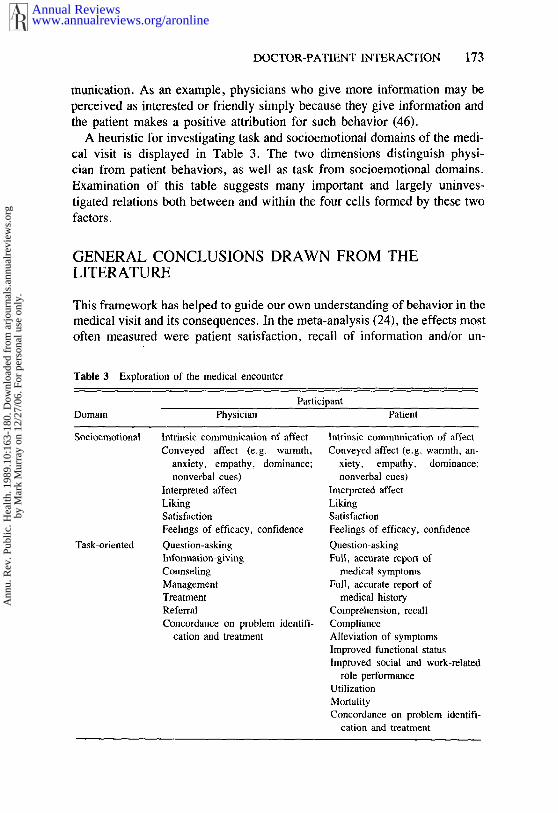
A heuristic for investigating task and socioemotional domains of the medi-cal visit is displayed in Table 3. The two dimensions distinguish physi-cian from patient behaviors, as well as task from socioemotional domains.Examination of this table suggests many important and largely uninves-tigated relations both between and within the four cells formed by these twofactors.
GENERAL CONCLUSIONS DRAWN FROM THELITERATURE
This framework has helped to guide our own understanding of behavior in themedical visit and its consequences. In the recta-analysis (24), the effects mostoften measured were patient satisfaction, recall of information and/or un-
Table 3 Exploration of the medical encounter
ParticipantDomain Physician Patient
Socioemotional
Task-oriented
Intrinsic communication of affect Intrinsic communication of affectConveyed affect (e.g. warmth, Conveyed affect (e.g. warmth, an-
anxiety, empathy, dominance; xiety, empathy, dominance;nonverbal cues) nonverbal cues)
Interpreted affect Interpreted affectLiking LikingSatisfaction SatisfactionFeelings of efficacy, confidence Feelings of efficacy, confidenceQuestion-asking Question-askingInformation-giving Full, accurate report ofCounseling medical symptomsManagement Full, accurate report ofTreatment medical historyReferral Comprehension, recallConcordance on problem identifi- Compliance
cation and treatment Alleviation of symptomsImproved functional statusImproved social and work-related
role performanceUtilizationMortalityConcordance on problem identifi-
cation and treatment
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.

174 ROTER & HALL
derstanding of the medical problem, and patient compliance. Satisfaction wasconsidered a socioemotional outcome; recall and compliance were consideredtask-related outcomes.
Of all the patient variables considered, satisfaction had the most consistentrelation to provider behavior. Satisfaction was best predicted by the amount ofinformation given by providers during the medical encounter. It was alsopositively related to more communication overall, and particularly socialconversation, conversation that could be construed as partnership-building,more immediate and positive nonverbal behavior, and positive talk, and wasnegatively related to negative talk (excluding negative voice quality). Satis-faction was also related to technical and interpersonal competence. Of thevariables considered, only physician question-asking showed no relation tosatisfaction.
Patient compliance was associated with patterns of provider behavior dur-ing the medical encounter, including more information-giving, fewer ques-tions overall (but more questions about compliance in particular), morepositive talk, and less negative talk. Finally, patient recall was best predictedby information-giving, less question-asking, more positive talk, and morepartnership-building.
Comparison of Results Between and Within the Task andSocioemotional Domains
Using our framework, we found the strongest provider-patient relations be-tween corresponding domains of communication. The median absolutecorrelation between physician task behaviors (information-giving andquestion-asking) and patient task behaviors (compliance and recall) was 0.2 the median correlation between physician socioemotional behaviors (positive,social, and negative talk, interpersonal competence, and partnership-building)and patient socioemotional reaction (satisfaction) was 0.26.
For provider-patient correlations between domains, we found an asymmet-rical pattern. The median correlation between physician task behaviors (in-formation-giving, question-asking, and technical competence) and patientsatisfaction was 0.22, but the correlation between physician socioemotionalbehaviors (partnership-building, positive and negative talk) and patient taskbehaviors (compliance and recall) was only 0.10.
Toward a Theory of Reciprocity in the Medical Encounter
We believe than an explanatory mechanism for this pattern of results may beprovided through the broad concept of reciprocity.l Simply put, behaviorsgenerate reciprocal, or like, behaviors. Physician task behaviors and patienttask behaviors reciprocate one another as do physician and patient socioemo-tional behaviors.
We suggest, however, that such reciprocated exchange is not equally
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.
DOCTOR-PATIENT INTERACTION 175
operative between different domains of communication. We believe thatphysicians’ task behaviors carry socioemotional significance for patients andthat because of this one may expect to see correlations between physician taskbehaviors and patient socioemotional behaviors. Task behavior can take onsocioemotional meaning in two ways: through conveyance (voice quality, forexample) and through interpretation, as defined above. As examples, physi-cians who provide more medical information have been found to speak withan interested voice quality (23); or, a physician who is proficient or otherwiseactive in the task domain may be interpreted as interested and caring regard-less of what he or she expresses through specifically socioemotional behaviors(46), because the patient makes a positive inference about the physician’smotivation for engaging in the task behaviors.
This view is consistent with a growing literature demonstrating the efficacyof information-giving for a variety of therapeutic effects, including shortenedhospital stays, decreased use of analgesics, and reduced patient anxiety (12,37). We suggest that the mechanism by which information achieves itstherapeutic effects is through both the informative content per se and throughthe interpreted message of interest and caring. Because of the generalizationof positive affect from the task domain, socioemotional reciprocation by thepatient, expressed in satisfaction or other affective behaviors, can be ex-pected.
In contrast, the weaker relation between physicians’ socioemotional be-haviors and patients’ task behaviors, found in the meta-analysis, can be seenas a lack of reciprocity between these domains. In our view, physicians’socioemotional behaviors do not have ~ufficient task or technical significanceto lead strongly or frequently to reciprocal task-relevant responses in patients;in other words, consistent with the simulation study of Willson & McNamara(59), we believe patients do not typically make task attributions (e.g. com-petence) on the basis of socioemotional behavior. The physician who ispositive socioemotionally may inspire friendliness or liking in the patient, butno, or only weak, task responses such as attending to information, modifyinglifestyle, or adhering to a therapeutic regimen.
CHANGING PATIENT AND PHYSICIAN BEHAVIOR
Descriptions of which aspects of communication are related to positive effectsare not highly meaningful if communication cannot be improved as a result.
Intervention studies attempting to change behavior, particularly physicians’
1The concept of reciprocity is regarded as critically important to the understanding of socialrelations, yet it remains ambiguous, and few theorists pose an operational definition. For a historyof the concept and attendant difficulties in definition, see Gouldner’s extensive discussion (t9).For insight into social psychological elaboration of the concept in terms of equity theory, seeBerkowitz & Walster (5).
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.
176 ROTER & HALL
communication behavior, have been increasing over the past several years,and many of these report positive results (9). In a very simple but effectiveintervention, Bertakis (6) found that training physicians to implement five-minute concluding statement to the visit that included summarization anda request for patient feedback was well accepted by residents and incorporatedinto their visits. The intervention significantly increased patient satisfactionand recall of information.
A more complex study by Goldberg and associates (18) demonstrated thatkey behaviors such as directive question-asking and clarification of the pre-senting complaint, as well as the demonstration of empathy and the reading ofverbal and nonverbal cues, could be taught to residents and that the behaviorscontinued to be practiced at least three months after training was complete.Moreover, the researchers found that given this special training, residentswere better able to detect psychiatric illnesses among their patients.
More recently, Maguire and associates (34) found that similar skills taughtto medical students were still evident in their practice styles some five yearslater when these young doctors were established in their own practice. Theseresearchers were also able to demonstrate that the quality of diagnosticinformation obtained from patients when these skills were used was superiorto that commonly gained by practicing physicians.
Also demonstrating that empathy skills can be effectively taught to physi-cians and that these are incorporated into their practice was a recent Dutchstudy by Bensing & Sluijs (3). After training, the physicians were moreinformative, more empathic, and less directive. However, there was noimpact on the outcome of care. A similar success in training, but failure inimpact, was reported by Putnam and colleagues (42). These investigatorsfound that training of residents was successful in increasing the amount ofexplanation given to patients and the amount of active listening (whichincreased patient giving of information to the doctor); however, these changeswere not related to other patient effects.
Less common than attempts to change physician behavior have been in-terventions to change patient behavior in the medical visit. Two such studiesare noteworthy. The first was described in some detail above (45). A morerecent study by Greenfield and colleagues (21) intervened with patients, againin the waiting room prior to their medical visit, to increase their involvementin care. This was done by having a health educator assist patients in readingtheir medical record and coach them to ask questions and negotiate medicaldecisions with their physicians. The intervention succeeded in changingpatients’ involvement in their care; experimental patients were more verballyactive, more interpersonally engaged, and, though they did not ask signifi-cantly more questions, they made other attempts to control the conversationand elicit information from physicians. Six to eight weeks after the interven-
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.

DOCTOR-PATIENT INTERACTION 177
tion, cxperimcntal group patients reported fewer limitations in physical androle-related activities and preferred a more active role in medical decisionmaking than did members of the control group.
In sum, communication can be effectively changed and these changes domake substantive differences in a variety of outcomes, including the quality ofdiagnosis and treatment, patient recall, satisfaction, and compliance. More-over, it appears that functional outcomes are also affected.
FUTURE DIRECTIONS
The field must contend with a number of fundamental issues for progress tocontinue. The need for guiding theoretical models, current methodologicallimitations, the application of research methods and results to physiciantraining and assessment, and the changing nature of the therapeutic relation-ship are among these important considerations.
Primary among these issues is the lack of theoretical models to guideinvestigators. This deficit has contributed to the largely exploratory nature ofthis work, resulting in a proliferation of findings with little conceptual fram-ing of their meaning.
Methodological limitations are evident in all systems of interactional analy-sis. There has yet to be developed a practical approach to accounting forinteraction sequence. A basic assumption has been that summary profilesbased on frequencies of verbal behaviors engaged in during the encounteradequately reflect the communication process. However, as pointed out bylnui & Carter (28), this is analogous to describing "Hamlet" as a play in whichthe principal characters include ghosts, witches, lords, ladies, officers, sol-diers, sailors, messengers, and attendants---one of whom is already dead, oneof whom dies by drowning, one by poisoned drink, two by poisoned sword,and one by sword and by drink!
The design of research in the field has been quite narrow, and almostentirely cross-sectional. Only two studies followed patient-physician dyadsprospectively, and that was only through two visits. Forty percent of thestudies did not even specify whether the patient and physician were previouslyacquainted. Better specification of the ongoing relationship can be accom-plished through more conscientious reporting by investigators and throughmore creative research designs.
Investigators have some responsibility to make their research methods andfindings accessible to the clinical audience. Seven studies reflect some formof physician intervention, usually medical student or resident training. Moreintervention studies are needed in which teaching methods are evaluated inlight of actual changes in physicians’ communication style and, further,validated against changes in patient outcomes. Those physicians responsible
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.

178 ROTER & HALL
for training in clinical interviewing courses could particularly benefit fromthis area of work by collaborating with researchers to develop analysisschemes pertinent to quality of care assessment.
We believe much greater progress has been made in the measurement ofconventionally defined technical performance quality than in the measure-
ment of interpersonal performance quality. Research on the interpersonaldomain clearly has evaluative as well as descriptive overtones, but thatevaluation tends to embrace the "more is better" principle (or less, dependingon the behavior in question), rather than being based on explicit criteria for
what should and should not be done. Furthermore, less evidence is availablefor establishing such criteria. Much work is needed in this area.
Application of research to patient interventions is also an important andrelatively underdeveloped focus. Studies that employed patient interventionshave found favorable effects. This is clearly an area that needs furtherelaboration and has tremendous potential for health education trials.
One further issue is worthy of consideration: the basic characteristics of theprovider-patient relationship may be undergoing substantial evolution (28).There is considerable evidence that patients are becoming more consumeristin orientation, and particularly the new generation of patients is likely tochallenge physician authority directly within the medical encounter (25).There is likewise evidence that physicians may be accommodating theirpatients with a more egalitarian relationship and tolerance for patientparticipation in decision making. The implications of these changes aretremendous and they must be given full and serious consideration in con-ceptualizing how the patient-physician relationship may be articulated in themedical encounter.
In sum, important strides have been made in the understanding of doctor-patient relations but challenges remain. The most significant of these chal-lenges is to push forward our conceptual and methodological imagination toapproach the field in new and even more meaningful ways.
Literature Cited
1. Bain, D. J. G. 1976. Doctor-patientcommunication in general practice con-sultations. Med. Ed. 10:125-31
2. Bales, R. F. 1950. Interaction ProcessAnalysis. Cambridge, Mass.: Addison-Wesley
3. Bensing, J. M., Sluijs, E. M. 1985.Evaluation of an interview trainingcourse for general practitioners. Soc.Sci. Med. 20:737-44
4. Ben-Sira, Z. 1980. Affective and instru-mental components in the physician-patient relationship: An additional di-
mension of interaction theory. J. HealthSoc. Behav. 21:170
5. Berkowitz, L., Walster, E., ed. 1976.Equity Theory: Toward a GeneralTheory of Social Interaction. Adv. Exp.Soc. Psychol. Vol. 9. New York: Aca-demic
6. Bertakis, K. 1977. The communicationof information from physician to patient:A method for increasing patient reten-tion and satisfaction. J. Fam. Pract.5:217-22
7. Bloom, S. 1963. The Doctor and His
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.
DOCTOR-PATIENT INTERACTION 179
Patient: A Sociological Interpretation.New York: Russell Sage
8. Bradshaw, P., et al. 1975. Recall ofmedical advice. Br. J. Soc. Clin. Psy-chol. 14:55-62
9. Carroll, J. G., Monroe, J. 1979. Teach-ing medical interviewing: A critique ofeducational research and practice. J.Med. Educ. 54:498-500
10. Davis, M. 1969. Variations in patients’compliance with doctors’ advice: Anempirical analysis of patterns of com-munication. Am. J. Public Health58:274-88
11. Davis, M. 1971. Variation in patients’compliance with doctors’ orders: Medi-cal practice and doctor-patient interac-tion. Psychiatry Med. 2:31-54
12. Devine, E. C., Cook, T. D. 1983. Ameta-analytic analysis of effects of psy-choeducational interventions on lengthof post-surgical hospital stay. NursingRes. 32:267-74
13. DiMatteo, M. R., Hays, R. D., Prince,L. M. 1986. Relationship of physicians’nonverbal communication skill to patientsatisfaction, appointment noncompli-ance, and physician workload. HealthPsychol. 5:581-94
14. DiMatteo, M. R., Taranta, A., Fried-man, H. S., Prince, L. M. 1980. Pre-dicting patient satisfaction from physi-cians’ nonverbal communication skills.Med. Care 18:376-87
15. Frankel, R. M. 1983. Talking in inter-views. In Interaction Competence, ed.G. Psathas. New York: Irvington
16. Freemon, B., Negrete, V., Davis, M.,Korsch, B. 1971. Gaps in doctor patientcommunication. Pediatric Res. 5:298-311
17. Friedman, H. S. 1982. Nonverbal com-munication in medical interaction. InInterpersonal Issues in Health Care,ed. H. S. Friedman, M. R. DiMatteo.New York: Academic
18. Goldberg, D. P., Steele, J. J., Smith,C., Spivey, L. 1980. Training familydoctors to recognize psychiatric illnesswith increased accuracy. Lancet 2:521-23
19. Gouldner, A. W. 1960. The norm ofreciprocity: A preliminary statement.Am. SocioL Rev. 25:161-79
20. Green, 13. F., Hall, J. A. 1984. Quan-titative methods for literature reviews.Annu. Rev. Psychol. 35:37-53
21. Greenfield, S., Kaplan, S., Ware, J. E.1985. Expanding patient involvement incare. Ann. Int. Med. 102:520-28
22. Hall, J. A., Roter, D. R., Rand, C. S.1981. Communication of affect between
patient and physician. J. Health Soc.Behav. 22:18-30
23. Hall, J. A., Roter, D~ L., Katz, N. R.1987. Task versus socioemotional be-haviors in physicians. Med. Care 25:399-412
24. Hall, J. A., Roter, D. R., Katz, N. R.1988. Meta-analysis of correlates of pro-vider behavior in medical encounters.Med. Care 26:657-75
25. Haug, M. R., Levin, B. 1981. Prac-titioner or patient--who’s in charge? J.Health Soc. Behav. 22:212-29
26. Hooper, E. M., Comstock, L. M.,Goodwin, J. M., Goodwin, J. S. 1982.Patient characteristics that influencephysician behavior. Med. Care 20:630-38
27. Hulka, B., et al. 1975. Medication useand misuse: Physician-patient discrepan-cies. J. Chronic Dis. 28:7-21
28. Inui, T. S., Carter, W. B. 1985. Prob-lems and prospects for health servicesresearch on provider-patient com-munication. Med. Care 23:521-38
29. Inui, T. S., Carter, W. B., Kukull, W.A., Haigh, V. H. 1982. Outcome-baseddoctor-patient interaction analysis: 1.Comparison of techniques. Med. Care20:535-49
30. Joyce, C., Richard, B., Caple, G., Ma-son, M., Reynolds, E., Mathews, J.1969. Quantitative study of doctor-patient communication. Q. J. Med.38:183-94
31. Larsen, K. M., Smith, C. K. 1981. As-sessment of nonverbal communication inthe patient-physician interview. J. Fami-ly Pract. 12:481-88
32. Ley, P. 1977. Psychological studies ofdoctor-patient communication. In Con-tributions to Medical Psychology, ed. S.Rochman, Vol. 1. Oxford: Pergamon
33. Louis, T. A., Fineberg, H. V., Mostel-ler, F. 1985. Findings for public healthfrom meta-analysis. Annu. Rev. PublicHealth 6:1-20
34. Maguire, P., Fairburn, S., Fletcher, C.1986. Consultation skills of young doc-tors: I. Benefits of feedback training ininterviewing as students persist. Br.Med. J. 292:1573-76
35. Milmoe, S., Rosenthal, R., Blanc, H.T., Chafetz, M. E., Wolf, 1. 1967. Thedoctor’s voice: Postdictor of successfulreferral of alcoholic patients. J. Abnor-mal Psychol. 72:78-84
36. Mishler, E. G. 1984. The Discourse ofMedicine. Norwood, NJ: Ablex
37. Mumford, E., Schlesinger, H., Glass,G. 1989-. The effects of psychologicalintervention on recovery from surgery
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.

180 ROTER & HALL
and heart attacks: An analysis of theliterature. Am. J. Public Health 72:141-51
38. Parsons, T. 1951. The Social System.Glencoe, I11.: Free Press
39. Pendleton, D. 1983. Doctor-patientcommunication: A review. In Doctor-patient Communication, ed. D. Pendle-ton, J. Hasler, pp. 5-53. New York:Academic
40. Potter, J., Wetherell, M. 1987. Dis-course and Social Psychology: BeyondAttitudes and Behavior. Beverly Hills:Sage
41. Putnam, S., Stiles, W., Jacob, M.,James, S. 1985. Patient exposition andphysician explanation in initial medicalinterviews and outcomes of clinicalvisits. Med. Care 23:74--83
42. Putnam, S. M., Stiles, W. B., Jacob, C.M,, James, S. A, 1988. Teaching themedical interview: An interventionstudy. J. General Int. Med. 3:38-47
43. Rosenthal, R. 1984. Meta-Analytic Pro-cedures for Social Research. BeverlyHills: Sage
44. Rosenthal, R., Blanck, P. D., Vannicel-li, M. 1984. Speaking to and aboutpatients: Predicting therapists’ tone ofvoice. J. Consult. Clin. Psychol.52:679-86
45. Roter, D. L. 1977. Patient participationin the patient-provider interaction.Health Educ. Monogr. 5:281-315
46. Roter, D. L., Hall, J. A., Katz, N. R.1987. Relations of physicians’ task andsocioemotional behaviors to analoguepatients’ satisfaction, recall, and im-pressions. Med. Care 25:437-51
47. Roter, D. L., Hall, J. A., Katz, N. 1~.1988. Doctor-patient communication: Adescriptive summary of the literature.Patient Educ. Counsel. 12:99-119
48. Stiles, W., Putnam, S., James, S.,Wolf, M. 1979. Dimensions of patientand physician roles in medical screeninginterviews. Soc. Sci. Med. 13A:335-41
49. Stiles, W., Putnam, S., Wolf, M.,James, S. 1979. Interaction exchange
structure and patient satisfaction withmedical interviews. Med. Care 17:667-81
50. Svarstad, B. 1976. Physician-patientcommunication and patient conformitywith medical advice. In Growth of Bu-reaucratic Medicine, ed. D. Mechanic.New York: Wiley
51. Tuckett, D., Williams, A. 1984. Ap-proaches to the measurement of explana-tion and information-giving in medicalconsultations: A review of empiricalstudies. Soc. Sci. Med. 7:571-80
52. Tuckett, D. A., Boulton, M., Olson, M.1985. A new approach to the measure-ment of patients’ understanding of whatthey are told in medical consultations. J.Health Soc. Behav. 26:27-38
53. Tuckett, D., Boultun, M., Olson, C.,Williams, A. 1985. Meetings BetweenExperts: An Approach to Sharing Ideasin Medical Consultations. London:Tavistock
54. Waitzkin, H. 1985. Information givingin medical care. J. Health Soc. Behav.26:81-101
55. Waitzkin, H. 1984. Doctor-patient com-munication: Clinical implications of so-cial scientific research. J. Am. Med.Assoc. 252:2441-46
56. Waitzkin, H., Stoeckle, J. 1972. Thecommunication of information about ill-ness: Clinical, sociological and method-ological considerations. Adv. Psy-chosom. Med. 8:180~215
57. Wasserman, R. C., lnui, T. S. 1983.Systematic analysis of clinician-patientinteractions: A critique of recent ap-proaches with suggestions for future re-search. Med. Care 21:279-85
58. West, C. 1984. Routine Complications:Troubles with Talk Between Doctors andPatients. Bloomington: Indiana Univ.Press
59. Willson, P., McNamara, J. R. 1982.How perceptions of a simulated physi-cian-patient interaction influence in-tended satisfaction and compliance. Soc.Sci. Med. 16:1699-1704.
www.annualreviews.org/aronlineAnnual Reviews
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.
Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.

Ann
u. R
ev. P
ublic
. Hea
lth. 1
989.
10:1
63-1
80. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by M
ark
Mur
ray
on 1
2/27
/06.
For
per
sona
l use
onl
y.






![[d], [o] If one doctor doctors another doctor does the doctor who doctors the doctor doctor the doctor the way the doctor he is doctoring doctors? Or](https://img.pdfslide.us/doc/110x75/56649e995503460f94b9c732/d-o-if-one-doctor-doctors-another-doctor-does-the-doctor-who-doctors-the.jpg)





















