Embed Size (px)
Citation preview

Student Self-Perception of Eating Habits in Relation to Peers and Reported Dietary IntakeA. Secker1 & S. Down
1Heart Niagara Inc., Niagara Falls, Canada
ABSTRACT
Data were gathered from 906 fourth to sixth grade students from across the Regional Municipality of Niagara. Student nutrition questionnaires, as well as in-class measurements of height and weight, were collected. Through multiple choice questions, students provided detailed information about the types and frequency of foods they consumed the day before. Students were also asked to rate how they perceive their eating habits to compare to their peers. This study aims to identify if student self-perception of eating ! habits in relation to their peers matches reported dietary ! ! intake. The results of this study will help to inform ! ! ! future health interventions at the elementary ! ! school level in order to reduce childhood obesity and its complications.
Figure 1: The dynamic influences of nutritional literacy, perception, and diet on one another.
Nutrition Literacy Perception Diet
Intervention
According to the World Health Organization body mass index (BMI) classification, approximately one third of Canadian children aged 5-17 would be considered overweight or obese (Roberts, Shields, de Groh, Aziz, & Gilbert, 2012). That childhood weight issues tend to continue on through adulthood (Magarey, Daniels, Boulton, & Cockington, 2003) speaks to the need to promote early intervention at the elementary school level.
Two main factors related to BMI include level of physical activity and dietary intake. Healthy eating is related to several factors, such as available food sources, choices in food consumption, nutrition literacy, and self-perception of eating habits.
Regarding the concept of self-perception and health, Schermel et al. (2014) examined the perceived health and diet status of adult Canadians in comparison to their actual health status. Through the use of two surveys completed by 6,665 (baseline) and 5,494 people across Canada, the authors found that, “the majority of Canadians (71.0%) rated both their diet and health similarly” and that 33.6% of Canadians “perceived their health to be very good . . . while very few (3.2%) perceived their health to be very poor” (p. 7). According to the authors, Canadians appear to “perceive their diets and health to be better than they actually are,” citing a discrepancy between participantsʼ self-reported weight status and diet and the Canadian Community Health Survey which indicates that “approximately 59% of Canadians are overweight or obese” and that 50% of Canadian adults do not meet the minimum daily recommendation of fruit and vegetable consumption (Statistics Canada, 2005). Schermel et al. suggest that, “problematically, consumers who are satisfied with their diets may have lower motivation to change their diets compared to those who are less satisfied” (p.7). One aspect of this proposed study is to identify whether children may also have misperceptions about the healthfulness of their food consumption in relation to their peers. If so, their motivation to make changes to a healthier diet may also be affected and interventions may be necessary (See Figure 1).
BACKGROUND
This study would seek to identify if student self-perception of their eating habits in relation to their peers matches their dietary intake in order to inform future health interventions at the elementary school level. BMI classification as a potential factor would also be explored.
OBJECTIVE
METHODS
Participants in this proposed descriptive study are 906 students from fourth to sixth grade at 34 elementary schools from across the Regional Municipality of Niagara. Data were collected from the students throughout the 2013-2014 school year as part of Heart Niagaraʼs Healthy Heart Schools Program. Although schools were chosen from throughout the region, participation was influenced by program funding grants and the interest of school administration. Of the 34 elementary schools, 15 are identified as schools in low-income neighbourhoods (Niagara Prosperity Initiative, 2006) and 21 of the schools are located in Niagara Falls. Additionally, 7 of the participating schools are part of the Niagara Catholic District School Board with the remainder being under the jurisdiction of the District School Board of Niagara.
PARTICIPANTS
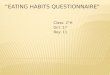
Data were gathered through the use of a multiple choice student questionnaire booklet that was designed by Heart Niagara in partnership with The Hospital for Sick Children in Toronto. The questionnaire has a total of 116 questions on topics of family history, personal health, tobacco use, nutrition, attitudes towards food, and physical activity habits. Questionnaires are sent to participating schools upon booking the Healthy Heart Schools Program and the studentsʼ home room teacher distributes the questionnaires. Students are given one to three weeks to complete the booklet at home, from their perspective, with parent or guardian assistance. This study will use data from the 21 questions on nutrition which ask the student to recall how often, and of what kinds, of foods they consumed in the last 24 hours as well as one question on their perception of their eating habits in comparison to their peers (See Figure 2).
Dietary assessment tools, such as the 24-hour recall and food frequency questionnaires, have been successfully used with children as young as, or younger than, the participants for this proposed study (St John et al., 2008). These tools are generally restricted to group comparisons due to the individual variations that can occur in day-to-day dietary choices (Feldman et al., 1993). A short parent-proxy eating and physical activity questionnaire similar to the one in use for this proposed study was found to have an acceptable level of relative validity in comparison with an interviewer-administered 24-hour food recall assessment (Bennett, de Silva-Sanigorski, Nichols, Bell, & Swinburn, 2009).
DATA COLLECTION
Student responses to the 24-hour dietary recall portion of the 2013-2014 Grade 5 assessment booklet will be scored using an adapted version of the revised Canadian Healthy Eating Index (Woodruff & Hanning, 2010). Tertile cut-offs will be used to reflect “above average”, “average”, or “below average” healthy eating for that 24-hour period. Student responses to the self-perceived eating habits in relation to peers question will be collapsed to provide three levels: healthier than peers, about the same as peers, or less healthy than peers. BMI will be grouped according to the sex and age-controlled percentile rankings listed by the Centre for Disease Control: “normal weight” is at or below the 85th percentile; “overweight” is between the 85th to 95th percentile; obese is at or above the 95th percentile (Ogden & Flegal, 2010).
PROCEDURE
Figure 2: Applicable pages from the student questionnaire
Chi-square analysis will be used to determine any significant associations between dietary intake and self-perception of eating habits within each BMI classification. Chi-square analysis will also be used to determine if there are any significant differences between dietary intake and self-perception of eating habits between BMI classifications (See Table 1).
STATISTICAL ANALYSES
Normal Weight Overweight Obese
Dietary Intake RankSelf-Perception Self-Perception Self-Perception
Dietary Intake Rank <Healthy Same >Healthy <Healthy Same >Healthy <Healthy Same >Healthy
Below AverageAverage
Above Average
Table 1: Example Results Table
LIMITATIONS
This study will rely on parents to assist their children in completing the questionnaire. As such, potential limitations in this form of data collection include reporting errors if the parent was not present for all of the studentʼs meals or if the parent or child cannot remember what the child consumed. Additionally, self-reporting can lead to social desirability bias, influenced by a fear of being negatively evaluated (Bennett et al., 2009 & Garriguet, 2008). Another limitation of this study is that students are asked to report their food intake for a single day. A snapshot of one 24 hour period may not be representative of a studentʼs typical eating habits.
ACKNOWLEDGEMENTS
Heart Niagara has funded the creation of this poster and subsequent research paper. Data were collected through Heart Niagaraʼs grade 5 Healthy Heart Schools Program which is funded in part by the Niagara Prosperity Initiative and the Niagara Falls Hydro Foundation. The authors also wish to acknowledge assistance from The Hospital for Sick Children for consultation regarding the student questionnaire and the creation of this poster.
REFERENCES
Bennett, C-A, de Silva-Sanigorski, A. M., Nichols, M., Bell, A. C., & Swinburn, B. A. (2009). ! Assessing the intake of obesity-related foods and beverages in young children: ! Comparison of a simple population survey with 24 hr-recall. International Journal of ! Behavioral Nutrition and Physical Activity, 6(71).Garriguet, D. (2008). Under-reporting of energy intake in the Canadian community health ! survey. Health Reports, 19(4), 37-45.
Lytle, L. A., Nichaman, M. Z., Obarzanek, E., Glovsky, E., Montgomery, D., Nicklas, T., Zive, M., & Feldman, H. (1993). Validation of 24-hour recalls assisted by food records in third-grade children. Journal of the American Dietetic Association, 93(12), 1431–1436.
Niagara Prosperity Initiative. (2006). Neighbourhood mapping tool. Retrieved from! http://maps.niagararegion.ca/prosperityinitiative/
Ogden, C. L. & Flegal, K. M. (2010). Changes in terminology for childhood overweight and obesity (Report No. 25).
Roberts, K.C., Shields, M., de Groh, M., Aziz, A., & Gilbert, J-A. (2012). Overweight and ! obesity in children and adolescents: Results from the 2009 to 2011 Canadian Health ! Measures Survey. Statistics Canada Catalogue no. 82003XPE. Ottawa, Ontario. Health ! Reports, Vol. 23, no. 3, September 2012.
Schermel, A., Mendoza, J., Henson, S., Dukeshire, S., Pasut, L., Emrich, T., Lou, W., Qi, Y., & LʼAbbe, M. (2014). Canadiansʼ perceptions of food, diet, and health – A national survey. PLOS ONE, 1(9), 1-8.
St John, M., Durant, M., Campagna, P. D., Rehman, L. A., Thompson, A. M., Wadsworth, L. A., & Murphy, R. J. L. (2008). Overweight Nova Scotia children and youth. Canadian Journal of Public Health, 99(4), 301–306.
Woodruff, S. J. & Hanning, R.M. (2010). Development and implications of a revised Canadian ! Healthy Eating Index (HEIC-2009). Public Health Nutrition, 13(6), 820–825.