Embed Size (px)
Citation preview

Thorax 1991;46:117-121
Structure of a human pulmonary acinus
N Berend, A C Rynell, H E Ward
AbstractThe structure of the human pulmonaryacinus has been described infrequently.The aim ofthe study was to determine thebranching pattern of respiratory bron-chioles and alveolar ducts in a humanacinus from the peripheral part of thelung, where space constraints may haveaffected airway branching patterns. Thelungs were obtained from an 18 year oldvictim of a motor vehicle accident andfixed in inflation under a pressure of25 cm H20. A block was cut from thelower edge of the right lower lobe andembedded in plastic. Serial sections werecut and the branching pattern of airwayssubtended by a terminal bronchiole werefollowed. The acinus was bounded on twosides by pleura and on the remainingsides by connective tissue septa. The ter-minal bronchiole divided into two res-piratory bronchioles, each of which gaverise to four systems of alveolar ducts.Between successive systems of alveolarducts the respiratory bronchioles con-tinued as single airways, becoming pro-gressively more alveolated towards theperiphery but not subtending furtherbranches of respiratory bronchioles. Theduct systems became less complex to-wards the periphery, near to the edge ofthe lung. The total volume of the acinuswas similar to that found in previousstudies. This branching pattern has notbeen described previously in a humanacinus.
Department ofThoracic Medicine,Royal North ShoreHospital, St Leonards,New South Wales 2065,AustraliaN Berend (alsoDepartment of Medicine,University of Sydney)A C Rynell,H E WardReprint requests to: DrBerendAccepted 12 December 1990
The structure of the human pulmonary acinus,defined functionally as the largest lung unit inwhich all airways participate in gas exchange,'has seldom been described. The results of suchstudies have yielded a picture of acinar struc-ture of considerable variability, both in size andin the number of generations of branches.2`8 Inpart, this variability may be a reflection ofmethodological differences in the variousstudies, but true heterogeneity of acinargeometry is also possible. This was highlightedin a recent study by Haefeli-Bleuer andWeibel,9 in which a seven to eight fold dif-ference in acinar volume was documentedwithin one lobe of a lung. In general, however,the terminal bronchiole has been observed tosubtend several generations of respiratorybronchioles, which in turn subtend severalgenerations of alveolar ducts.
In this study we sectioned an acinus from a
subpleural location serially, finding an acinarstructure not previously described in a humanlung.
MethodsThe right lung of an 18 year old man who haddied of head injuries was obtained at necropsy.A chest radiograph obtained before death wasnormal. The lung was weighed and inflatedwith air to a transpulmonary pressure of 25 cmH20 and the lung volume was obtained bywater displacement. The lung was then fixed ininflation via the bronchus at a constant trans-pulmonary pressure of 25 cm H20 with 10%buffered formalin for 72 hours. The lungvolume was then remeasured.
Multiple blocks were cut from various partsof the lung. The acinus described in this paperwas selected from the lower edge of the rightlower lobe posterolaterally in the costophrenicangle and was bounded on two sides and thedistal end by pleura. The block of tissue wasdehydrated in graded ethanol at room tem-perature. Infiltration and embedding wereachieved by means of an LKB 2218-500 His-toresin embedding kit. The tissue was preinfil-trated in 1:1 99% ethanol:infiltration solutionfor 12 hours to ensure complete penetration.The tissue was then transferred to pure infiltra-tion solution and kept at 4CC for one week, thesolution being changed three times. Duringthis period the tissue was also intermittentlysubjected to vacuum to remove air. The tissuewas then embedded in 20 x 20 x 20mmpolyethylene mould for polymerisation and theblock was kept on ice and under refrigeration.Holes were drilled through the block at eachcorner to enable accurate stacking of sectionsfor reconstruction.
After completion of polymerisation serial 5gm sections were cut with a D profile tungstencarbide steel knife. Sections were stained with0 5% toluidine blue in 1% borax. Every fifthsection was used for the reconstruction,additional sections being viewed where it wasdifficult-to decide on branching patterns.
Sections were photographed and the ter-minal bronchioles, respiratory bronchioles,and alveolar ducts identified, labelled, andtraced. The outlines were then retraced on adigitising tablet and the airways reconstructedby means of a three dimensional reconstructionprogram (PC-3D Multidimensional Comput-ing, Durham, North Carolina, USA).
All dimensions were corrected by twoshrinkage factors. Shrinkage during fixationwas calculated from the known volumes beforeand after fixation of the whole lung. Shrinkage
117
on 28 July 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.46.2.117 on 1 February 1991. D
ownloaded from

Berend, Rynell, Ward
SERIALSECTIONS
DISTAL TIPOF BLOCK
Figure I Configuration of the tissue block cutfrom the lower edge of the right lowerlobe. Note that less than 1 mm could not be sectioned at the distal tip of the-block.
during processing was calculated by comparingthe area of the block face (photographed atknown magnification and then digitised) withthe area of the final section (projected at knownmagnification on to an electronic digitisingtablet).
ResultsThe weight of the right lung was 346 g and theair inflated volume 3701 ml. Volume shrinkageduring fixation was 19% and area shrinkageduring processing 4-6%. Serial sections werecut to within less than 1 mm of the pleural edge
Intervals along respiratory bronchioles between origins ofalveolar duct systems
Left RightInterval (Psm) hemiacinus hemiacinus
Terminal bronchiole 410 430bifurcation to 1st ductsystem
1st to 2nd duct system 870 6302nd to 3rd duct system 730 Overlap3rd to 4th duct system 320 650
at the distal extreme of the block of tissue(fig 1). Possibly therefore some distal brancheswere lost.
Reconstruction was facilitated by theenclosure of the acinus by two pleural surfacesand two connective tissue septa, producing across section the shape of a parallelogram(fig 2). The cross sectional area at this level was45-6 mm2. The total length of the acinus was3 82 mm without the missing tip. This is longerthan the sum of the distances between thebranches (table) because some of the firstalveolar ducts recurved to be proximal to thebifurcation of the terminal bronchiole.The terminal bronchiole before bifurcation
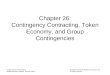
showed some areas of flattened epithelium.The terminal bronchiole (fig 2) leading into theacinus divided into two respiratory bron-chioles. The branch point is shown in figure 3.All subsequent branches were alveolar ducts-that is, at each branch point there was onedaughter respiratory bronchiole, other bran-ches being alveolar ducts. The whole branch-ing system of the acinus is shown schematicallyin figure 4. The first alveolar duct branches inthe right hemiacinus (that is, the part of theacinus supplied by the right respiratory bron-chiole) are shown in figure 5 and had theirorigin 430 Mm below the bifurcation of theterminal bronchiole. This was a combined
Figure 2 Shape of theacinus in cross section,approximaiely that of aparallelogram bounded bytwo pleural surfaces andtwo connective tissue septa.The terminal bronchioleleading into the acinus isindicated. P-pleura;CTS connective tissuesepta; TB-terminalbronchiole.
118
on 28 July 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.46.2.117 on 1 February 1991. D
ownloaded from

Structure of a human pulmonary acinus
TB
RB A RB
LEFT
HEMIACINUS
Figure 3 The terminal bronchiole about to divide into two respiratory bronchioles.
origin of three alveolar ducts, each of whichsubsequently gave rise to further ducts (fig 4).The respiratory bronchiole then continued as asingle airway (fig 6) until, 630 ,um below theprevious system of alveolar ducts, a secondsystem arose. Over the same length of res-piratory bronchiole giving rise to the secondsystem a third system originated (fig 7), andthis can be followed schematically in figure 4.After a further interval of 650 ,um a final systemoriginated, consisting of only two alveolarducts with the respiratory bronchiole termin-ating in a fully alveolated state (fig 8).A similar pattern was seen in the left
hemiacinus (the portion of the acinus suppliedby the left respiratory bronchiole). Again, therespiratory bronchiole continued as a singleairway between duct systems with the distancesbetween systems shown in the table. A finalsingle duct arose 320 jim below the third systemand the respiratory bronchiole simply becamefully alveolated and terminated. Possibly,
Figure 5 First branches (alveolar ducts) arisingfrom the respiratory bronchiolesupplying the right hemiacinus. RB-respiratory bronchiole; AD-alveolar ducts.
/
<
RIGHT
HEMIACINUS
Figure 4 Schematic representation of the overallstructure of the acinus. Length and directions of branches)iot to scale. Ternzinal bronchiole; -respiratorybronchiole; -alveolar duct.
however, final branches in both the left and theright hemiacinus close to the pleural surfacewere missed because ofour inability to cut rightup to the extreme end of the acinus.Although the respiratory bronchioles sub-
tended approximately equal numbers ofalveolar ducts (51 for the right and 58 for theleft), the alveolar duct systems were asym-metric with different numbers of branches ateach level. The alveolar duct systems becameprogressively less complex towards the peri-phery as the acinus narrowed approaching theedge of the lung.The total volume of the acinus was estimated
to be 153 mm3 with a small additional volumeclose to the edge of the lung.
DiscussionAn initial problem in this study was obtainingan appropriate lung free of trauma or disease.Although it was not known whether theaccident victim had been a smoker, his youngage precluded the possibility of a major degreeof smoking induced lung disease. The normalchest radiograph before death and the normallung weight reassured us that there was no lungtrauma or pulmonary oedema.There were several reasons for reconstruct-
ing an acinus from the periphery of the lung.Here were found connective tissue septa be-tween the acini, which facilitated reconstruc-tion because there were fewer interdigitationswith neighbouring acini. We thought that itwould be of interest to look at an acinus thathad developed in a part of the lung where space
119
on 28 July 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.46.2.117 on 1 February 1991. D
ownloaded from

Berend, Rynell, Ward
Figure 6 Respiratory bronchiole between first and second alveolar duct systems.RB-respiratory bronchiole.
Figure 7 Second and third duct systems (DS) arising from opposite sides of therespiratory bronchiole (RB).
Figure 8 Respiratory bronchiole supplying the right hemiacinus terminating in afualveolated state-that is, becoming an alveolar duct.
was constrained because this may have affecteddevelopment of-airway branching.Two major technical difficulties were en-
countered. Firstly, paraffin embedded blocksyielded sections with variable shrinkage anddistortion, which made accurate stacking ofsections impossible. We therefore decided toembed the tissue blocks in plastic. This, how-ever, proved to be technically very difficult.After considerable trial and error we developeda method that produced good tissue penetra-tion of the embedding medium and a block freeof air bubbles. Unfortunately, the tissue wasvery close to the edge ofthe block and thereforesections could not be cut right up to theextreme distal end ofthe acinus. The amount oftissue lost was less than 1 mm but further distal
>W<J branches may have been missed.The second major problem was related to the
determination of the branching patterns of thealveolar ducts. Sections 25 gm apart werephotographed and enlarged and these wereinitially examined to detect alveolar ducts aris-ing from the respiratory bronchioles. Each ofthese ducts was then followed by examiningsuccessive photographs moving either proxi-mally or distally, as appropriate. The sameprocess was followed for each generation ofalveolar ducts and this proved to be verydifficult and time consuming. On occasion we
\- had to refer to additional sections under themicroscope within the 25 pm intervals between
§ photographs to be certain of the branchingpatterns. Visualisation ofthe three dimensionalreconstruction was of value only for small partsof the acinus as the whole structure is toocomplex, a problem also encountered byMercer and Crapo,'0 who performed a threedimensional reconstruction of a rat acinus.An unexpected finding that facilitated this
work was the enclosure of the acinus by thepleural surfaces and connective tissue septa. Inthe human lung there are usually interlobularsepta, though these are often incomplete, andrarely interacinar septa.91' In the acinus des-cribed in this paper the only interacinar inter-digitations were on the proximal boundary, thelateral and distal boundaries being defined bythe pleura and connective tissue septa. Theareas of flattened epithelium seen in the ter-minal bronchiole may be rudimentary alveolior diverticula and these have also been des-cribed by von Hayek," Schreider and Raabe,7and Hansen et al.8The branching* patterns in this acinus
appeared to differ fundamentally from acinidescribed previously in- the human lung.
^ Previous studies have documented a system ofj several generations of respiratory bronchioles,
which in turn subtend several generations ofalveolar ducts.37" According to conventional
* terminology the respiratory bronchiole follow-ing the origins of each new cluster of ductsshould be regarded as a new generation. In ouracinus, however, all clusters of ducts arose asside branches with clear continuation of therespiratory bronchiole as a single airway (figs 5-7). Previous studies have identified a total of
flly nine to twelve generations of intra-acinar air-ways, the branching pattern being mainly
120
on 28 July 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.46.2.117 on 1 February 1991. D
ownloaded from

Structure of a human pulmonary acinus
(irregularly) dichotomous with some tricho-tomous and quadrivial divisions. In theirrecent study Haefeli-Bleuer and Weibel,9 usinga silicone rubber cast of an acinus, considereddivisions to be mainly dichotomous with poly-chotomous branches really being dichotomousbranches in close proximity. Although poly-chotomous branches appeared common in thepresent study we could not always be certainthat these were not dichotomous branches inclose succession. Following each cluster ofalveolar ducts, which usually arose from amultiple origin, the respiratory bronchiole con-tinued as a single airway and finally became aduct. Because of the wedge shape of the edge ofthe lung and the pleural boundaries the alveolarduct systems became smaller and less complextowards the periphery of the acinus. The totalacinar volume (153 mm3) was within the rangepreviously described (50-450 mm3).9 An intra-acinar duct to duct communication and bron-chiole-duct communication were identified butothers are likely to have been missed. Suchcommunications would be much more obviouswith an acinar cast than with a reconstructiontechnique. No interacinar pathways forcollateral ventilation were identified.The difference between this acinus and others
described in the human lung may be related todifferences of position within the lung fromwhich the acinus was derived. The acinusdescribed in the lungs of a child by Boyden,3however, was derived from a location similar tothat of ours but had the standard acinar struc-ture described by others.
1 Rodriguez M, Ber S, Farre A, Weibel ER. Pulmonaryacinus: geometry and morphometry of the peripheralairway system in rat and rabbit. Am J Anat 1987;180:143-55.
2 Pump KK. Morphology of the acinus ofthe human lung. DisChest 1969;56:126-34.
3 Boyden EA. The structure of the pulmonary acinus in a childof six years and eight months. Am J Anat 1971;132:275-300.
4 Hansen JE, Ampaya EP. Human air space shapes, sizes,areas and volumes. J Appl Physiol 1975;38:990-5.
5 Parker H, Horsfield K, Cumming G. Morphometry of distalairways in the human lung. J Appl Physiol 1971;31:386-91.
6 Horsfield K, Cumming G. Morphology of the bronchial treein man. J Appi Physiol 1968;24:373-83.
7 Schreider JP, Raabe OG. Structure ofthe human respiratoryacinus. Am JAnat 1981;162:221-32.
8 Hansen JE, Ampaya EP, Bryant GH, Navin JJ. Branchingpattern of airways and air spaces of a single humanterminal bronchiole. J Appl Physiol 1975;38:983-9.
9 Haefeli-Bleuer B, Weibel ER. Morphometry of the humanpulmonary acinus. Anat Record 1988;220:401-14.
10 Mercer RR, Crapo JD. Three dimensional reconstruction ofthe rat acinus. J Appl Physiol 1987;63:785-94.
11 Von Hayek H. The human lung. New York: Hefner, 1960:172-3.
121
on 28 July 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.46.2.117 on 1 February 1991. D
ownloaded from