Embed Size (px)
Citation preview

Thorax (1975), 30, 113.
Isolated chylopericardium due to mediastinallymphangiomatous hamartoma
R. E. JENNER and HLA 00
Departments of Surgery and Pathology, King's College Hospital, London SE5
Jenner, R. E. and Oo, H. (1975). Thorax, 30, 113-117. Isolated chlopericardium due tomediastinal lymphangiomatous hamartoma. Isolated chylopericardium is a rare cause
of pericardial effusion. Intrapericardial chyle was first noticed by Hasebroek (1888) atnecropsy. Twenty years ago Groves and Effler (1954) first reported a clinical case ofisolated chylopericardium. The present case is similar to theirs in several respects, andis the nineteenth case to be reported. To our knowledge this is the first British reportof an isolated chylopericardium and is the fourth case of isolated chylopericardium dueto a mediastinal lymphangiomatous hamartoma to be successfully treated.
CASE REPORT
A 30-year-old housewife was admitted for investiga-tion of an apparent enlargement of the heart in July,1973. She had been perfectly well until three monthsprior to admission when she became anorectic andnauseated following a minor fall one week pre-viously. Her symptoms were associated with a fullfeeling in the epigastrium and these symptoms lasteda week. She then became weak and experiencedpalpitations and breathlessness on mild exertion. Shewas investigated by her family doctor for infectioushepatitis as three members of the family had con-tracted this within the preceding six months. Bariummeal and liver function tests were normal, but a chestradiograph showed an enlarged cardiac outline. It wasknown that in 1967 her chest film was normal. Therewas no past history of rheumatic fever, tuberculosisor chest trauma, nor had she ever suffered any seriousrespiratory illness. Her general health was good andshe had undergone a normal pregnancy 18 monthsearlier. She was on no drugs and knew of noallergies.On examination she appeared a fit woman with no
anaemia nor dyspnoea at rest. Physical examinationwas non-contributory.
INVESTIGATIONS The blood picture, blood chemistry,and urinalysis were all normal. ESR 3 mm/hr. Pro-thrombin time normal. The Paul Bunnel test wasnegative. No autoantibodies were detected and LEcells were negative. The chest radiograph showed anapparent enlargement of the heart with normal lungfields (Fig. 1). The electrocardiogram was normalapart from low-voltage complexes. Serum electro-Green S-McCormack Food Ltd.
phoresis was normal. A right heart catheter revealednormal pressures and the right atrial angiogramconfirmed a pericardial effusion.Because she had become asymptomatic and was
apyrexial she was discharged home for out-patientfollow-up. A presumptive diagnosis of viral peri-carditis was made as there was nothing to suggesta bacterial or malignant aetiology. Shortly after dis-charge the results of viral studies showed a high titreto Coxsackie B virus 1/256 apparently supportingthe diagnosis. The effusion, however, did not diminish.It was aspirated one month after discharge and500 ml of milky fluid was removed. Chemical analysiswas as follows: Total lipids 1,840 mg/ 100 ml,cholesterol 128 mg/ 100 ml, triglyceride content1,637 mg/100 ml. The fluid was sterile and the whitecount 5,000 mm'. Lipoprotein electrophoresis showedthat the fluid consisted mainly of chylomicrons. Noacid-fast bacilli or cholesterol crystals were seen. Thisanalysis showed that the fluid was chyle and notcholesterol pericarditis. Three days later the patientbecame acutely distressed and extremely dyspnoeicwith tetany. Although the cause of her symptomswas thought to be due to an anxiety state and nottamponade, a further aspiration of 300 ml of chyleby the sub-xyphoid route was performed. The patientwas readmitted for surgery.
In September, 1973, a left posterolateral thoraco-tomy was made through the sixth intercostal space.In order to demonstrate the thoracic duct and anycommunication between it and the pericardial cavityconfectioner's green dye' in a fatty meal was ad-ministered five hours preoperatively. Thoracotomyrevealed a large lax immobile pericardial sac withdilated lymphatic channels coursing over it. The leftlung was free and there were no adhesions over the
113
on 25 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.30.1.113 on 1 February 1975. D
ownloaded from

R. E. Jenner and H. Oo
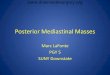
FIG. 1. Chest radiograph taken when the patient was first seen,demonstrating an apparent enlargement of the cardiac silhouette.Note that there is nothing to suggest a mediastinal tumour.
pericardium. Lying above the heart in the anteriormediastinum was a purple-grey sheet of tissue extend-ing to cover the left phrenic nerve.
PROCEDURE The pericardium was opened anterior tothe phrenic nerve and 800 ml of unstained milkychyle was aspirated. The heart, epicardial fat, andserous pericardium were normal. Biopsies were takenfrom the pericardium and the tissue in the anteriorsuperior mediastinum; a frozen section from thelatter was reported as benign. The thoracic duct was
located in its normal position and found to bethickened but also unstained by the dye. Five milli-litres of patent blue dye was injected around thethoracic duct to detect any communication betweenit and the pericardial cavity. Again no fistulouschannels were demonstrated. The thoracic duct was
ligated where it entered the posterior mediastinumand an anterior pericardiectomy was performed. Thewound was closed in layers after inserting an inter-costal pleural drain. This was removed on the thirdpostoperative day having drained only a small quantityof blood. There were no postoperative complicationsand the patient was discharged home after twoweeks. A postoperative lymphangiogram showed thata single thoracic duct had been ligated opposite the
eleventh thoracic vertebra (Fig. 2). She was wellwhen she was seen at a six months follow-up clinic,and her chest film showed a normal sized heart.Histology of the excised tissues showed a lymph-angiomatous hamartoma (Fig. 3) and a slightlythickened pericardium with dilated lymphatics.
DISCUSSION
Isolated chylopericardium is very rare. Moreoften it is associated with chyle in the pleuralcavities. Yater (1935), in a review of 100 casesof chylothorax, found three patients who had aconcomitant chylopericardium. The aetiology maybe (1) any neoplastic or inflammatory processinvolving the thoracic duct, (2) trauma by ruptureor following open-heart surgery, (3) lymph-angiectasis (a developmental abnormality inwhich there is a lymphatic communication be-tween the thoracic duct and pericardium), andfinally, (4) idiopathic. In practice lymphangiectasisand lymphangiomatous hamartomas account forthe majority of reported isolated chyloperi-cardiums. Mediastinal lymphangiomas areextremely rare. Herlitzka and Gale (1958), in a
114
on 25 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.30.1.113 on 1 February 1975. D
ownloaded from

Isolated chylopericardium due to mediastinal lymphangiomatous hamartoma
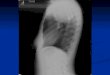
FIG. 2. Postoperative lymphangiogram showing theefJects of ligation of the thoracic duct low in themediastinum.
review of 174 mediastinal tumours and cyststreated surgically, found no case of lymph-angioma, and again Nelson, Shefts, and Bowers(1957) encountered only one case of hygroma ina series of 141 mediastinal tumours and cysts.Over 40 cases have now been reported. The mostcommon site for these mediastinal tumours is inthe anterior mediastinum, and there is no evidence
available to suggest that lymphangiomas mayundergo malignant transformation. The prognosisfor these tumours is good. The aetiology oflymphangiomas is unknown. They may arise fromlymphatic tissue normally present in the area, orthey may grow from mesodermal 'rests' whichproduce imperfect lymphoid channels. All re-ported cases of chylopericardium due to lymph-angiomatous hamartomas have occurred inyoung people or infants (suggesting a congenitaldefect), and all in females. A cystic hygroma isa variety of lymphangioma that develops inrelation to the lymph sacs of the jugular and iliacregions and possesses considerable growthpotential. The tumour in our case had the usualhistological characteristics of a lymphangiomatoushamartoma; the only difference between this anda cystic hygroma is in the number and size of thecystic spaces. The effect of chyle in the peri-cardium is essentially a mechanical one in whichthe cardiac output is reduced due to diminishedfilling of the right side of the heart. It is knownthat chylopericardium may be present for manyyears before the patient presents. Cardiac tam-ponade has been noted in about half the reportedcases. Although tamponade did not occur in ourcase, her symptoms were typical. If there is noexternal loss of chyle, nutritional disturbancesand inanition do not follow. In the case reportedby Miller, Pruett, and Long (1959) there was densepleural and mediastinal fibrosis due to the irritantproperties of the chyle.
It has always intrigued writers, in isolatedchylopericardium, as to why the chyle shouldcollect solely in the pericardial sac. One ex-planation is that it forms along communicationsbetween the pericardium and the thoracic duct.Although these are not described anatomically, itis probable that such communications do arise asa result of faulty embryological development. Theanatomy of the thoracic duct has been extensivelystudied, and several variations are known to exist(Meade, Head, and Moen, 1950). Lymphatics havevalves that permit a unidirectional flow into thesuperior mediastinum. Best and Taylor (1966)found that on ligating the thoracic duct high inthe mediastinum of the dog the pressure rose to15 cm of water. In our case it is possible thatchyle refluxed from the thoracic duct into thepericardial sac along dilated channels. Alterna-tively, the chyle could have flowed into thepericardial sac from the tumour into which thethoracic duct flowed. It is more difficult toaccount for those cases where there is no tumouror obstruction. Bartel and Neute (1964) suggested
115
on 25 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.30.1.113 on 1 February 1975. D
ownloaded from

R. E. Jenner and H. Oo
S.<., a, ,,;TilM~'
*T, *
-:-4.*"'qk
~ ~ ~ 4
144
44
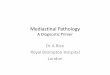
FIG. 3. A typical section of the tumour showing numerous irregular cystic spaces of varyingsizes lined by a layer of flattened endothelial cells. Focal lymphoid aggregates are present in theintervening fibrocollagenous walls (H and E X45).
that such cases may be due to an abnormal per-meability of the lymphatics. Although it wouldseem that obstruction of the thoracic duct wouldbe the common factor in chylopericardium, manycases of thoracic duct obstruction are unassociatedwith the accumulation of chyle, and it is knownthat the thoracic duct can be ligated in thesuperior mediastinum without causing chyloperi-cardium. Blalock, Cunningham, and Robinson(1936) produced chylopericardium and chylo-thorax experimentally in dogs by ligating thesuperior vena cava above the azygos vein, but notif the thoracic duct had been ligated at a pre-vious thoracotomy. These authors were unableto produce chylopericardium in dogs by tying themain right and left lymphatic ducts, indicatingthat there are a number of other lymphatics whichempty into the superior vena cava or its branches.The pathology may be missed because it is
difficult to obtain a good examination of thewhole pericardium from a standard right or leftthoracotomy. The patient of Groves and Effler(1954) illustrates this and also another important
operative detail. In their first operation through aleft thoracotomy the lax and distended peri-cardium was simply drained and a 4 cm windowwas made to create a fistula into the left hemi-thorax. Three months later the massive pericardialeffusion had recurred. A right thoracotomy wasthen performed which revealed a lymphangioma-tous hamartoma which was not evident before.A large portion of this tumour was excised andmore importantly the thoracic duct was ligatedlow in the chest.Once milky fluid has been aspirated from the
pericardium the diagnosis of chylopericardiumshould be easy. The only differential diagnosis toconsider is cholesterol pericarditis. Cholesterolpericarditis has been associated with hypertension,tuberculosis, carcinoma, mitral stenosis, atrialseptal defect, and arthritis (Brawley, Vasko, andMorrow, 1966). Apart from cardiac catheteriza-tion or diagnostic ultrasound, further preoperativeinvestigations should include a lymphangiogram,although this may not be helpful in a positiveway, as in the case reports by Hudspeth and
116
on 25 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.30.1.113 on 1 February 1975. D
ownloaded from

Isolated chylopericardium due to mediastinal lymphangiomatous hamartoma
Miller (1966) and Puig-Massana, Murtra, andCalbet (1972). Both their cases had normal pre-operative lymphangiograms, although it was clearthere must have been an abnormal communicationbetween the thoracic duct and the pericardium.Definite proof that such a communication existscan be shown by giving the patient a lipophilicdye in fat, for example, Sudan III in corn oil,and recovering the dye later by pericardialaspiration and ether extraction. More simply, anisotopically labelled fat ("'I-labelled triolein) canbe given orally followed by a cardiac scan. Boththese tests have been shown to be reliable. In ourcase a mixture of green S dye and butter ad-ministered preoperatively failed to demonstratethe thoracic lymphatic system. Peroperativedemonstration of fistulous lymphatic tracts is bestperformed by injection of dye directly into thethoracic duct if this is possible.The surgical objectives in this condition are to
relieve the raised intrapericardial pressure andprevent recurrent accumulation of chyle, andalso to search for a possible cause for the con-dition. Uniformly good results have come frompericardial fenestration and ligation of thethoracic duct low in the mediastinum. Besides per-mitting decompression, pericardial fenestrationshould also prevent the possible late onset ofconstrictive pericarditis. However, of the twoprocedures, ligation of the thoracic duct wouldappear to be the most important. The only twopostoperative deaths reported have occurred whenthe thoracic duct was not ligated.
We thank Mr. A. M. Macarthur and Dr. D. A.Chamberlain for their permission and help inreporting this case.
REFERENCES
Bartel, J. and Neute, E. (1964). Das isoliertechyloperikard. Cardiologia, 45, 251.
Best, C. H. and Taylor, N. B. (1966). The physio-logical basis of medical practices. In A Text inApplied Physiology, 8th edition, p. 508. Williamsand Wilkins, Baltimore.
Blalock, A., Cunningham, R. S., and Robinson, C. S.(1936). Experimental production of chylothoraxby occlusion of the superior vena cava. Annalsof Surgery, 104, 359.
Brawley, R. K., Vasko, J. S., and Morrow, A. G.(1966). Cholesterol pericarditis. AmericanJournal of Medicine, 41, 235.
Groves, L. K. and Effier, D. B. (1954). Primarychylopericardium. New England Journal ofMedicine, 250, 520.
Hasebroek, G. (1888). Analyse einer chylosen peri-cardialen Flissigkeit (chylopericardium). Zeit-schrift fur Physiologische Chemie, 12, 289.
Herlitzka, A. and Gale, J. W. (1958). Tumors andcysts of mediastinum; survey of 174 media-stinal tumors treated surgically during past 18years at the University of Wisconsin Hospitals.Archives of Surgery, 76, 697.
Hudspeth, A. S. and Miller, H. S. (1966). Isolated(primary) chylopericardium. Journal of Thoracicand Cardiovascular Surgery, 51, 528.
Meade, R. H. Jr., Head, J. R., and Moen, C. W.(1950). The management of chylothorax. Journalof Thoracic Surgery, 19, 709.
Miller, S. U., Pruett, H. J., and Long, A. (1959). Fatalchylopericardium caused by hamartomatouslymphangiomatosis. American Journal ofMedicine, 26, 951.
Nelson, T. G., Shefts, L. M., and Bowers, W. F.(1957). Mediastinal tumors; analysis of 141 cases.Diseases of the Chest, 32, 123.
Puig-Massana, M., Murtra, M., and Calbet, J. M.(1972). Idiopathic massive chylopericardium.British Heart Journal, 34, 431.
Yater, W. M. (1935). Non-traumatic chylothorax andchylopericardium; review and report of a casedue to carcinomatous thromboangiitis obliteransof the thoracic duct and upper great veins.Annals of Internal Medicine, 9, 600.
Requests for reprints to: R. E. Jenner, FRCS,Department of Surgery, King's College Hospital,Denmark Hill, London SE5.
117
on 25 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.30.1.113 on 1 February 1975. D
ownloaded from